
A Global Evaluation of the Performance Indicators of Colorectal Cancer Screening with Fecal Immunochemical Tests and Colonoscopy: A Systematic Review and Meta-Analysis

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics and Quality Assessment
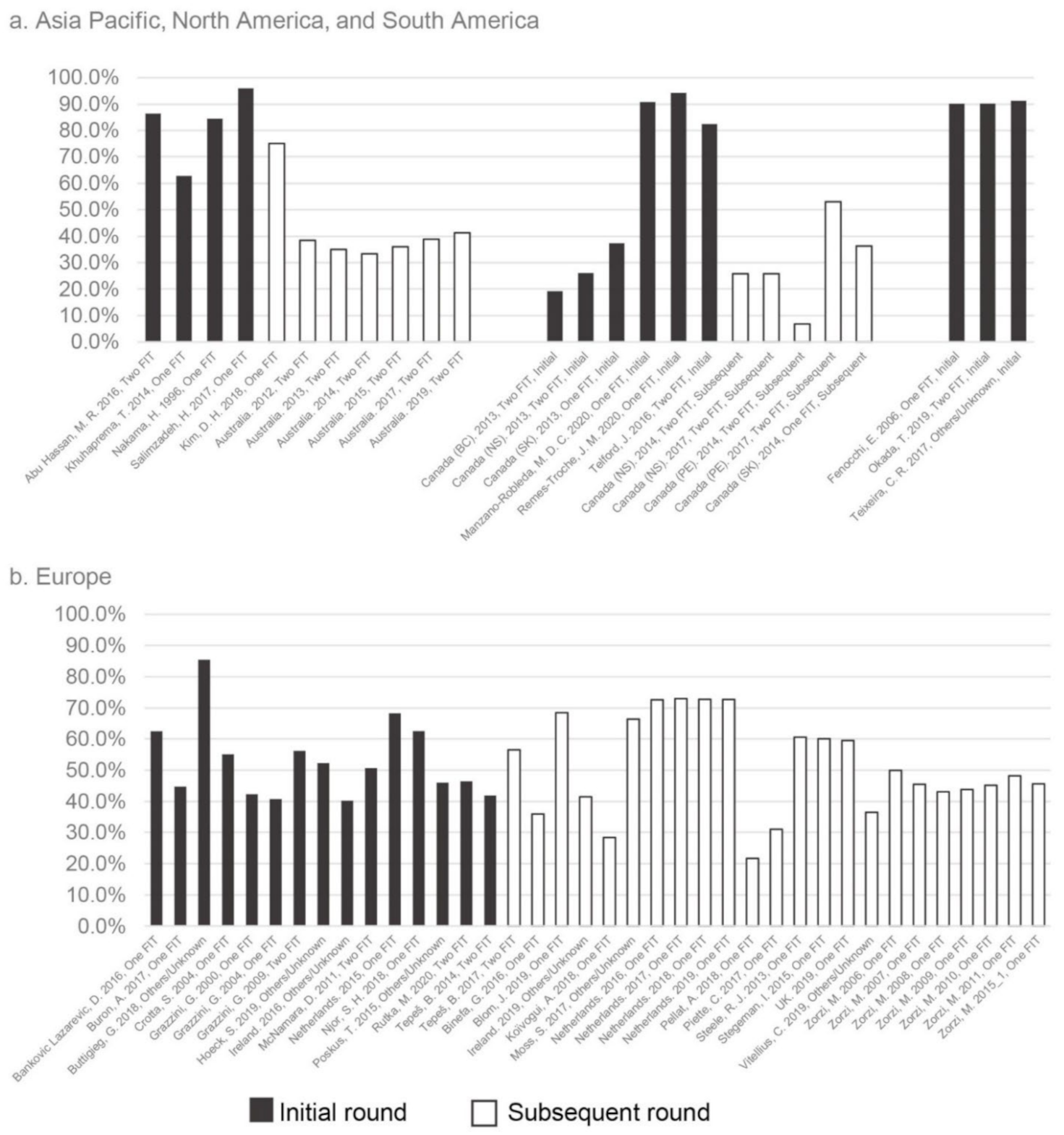
3.2. Participation Rate
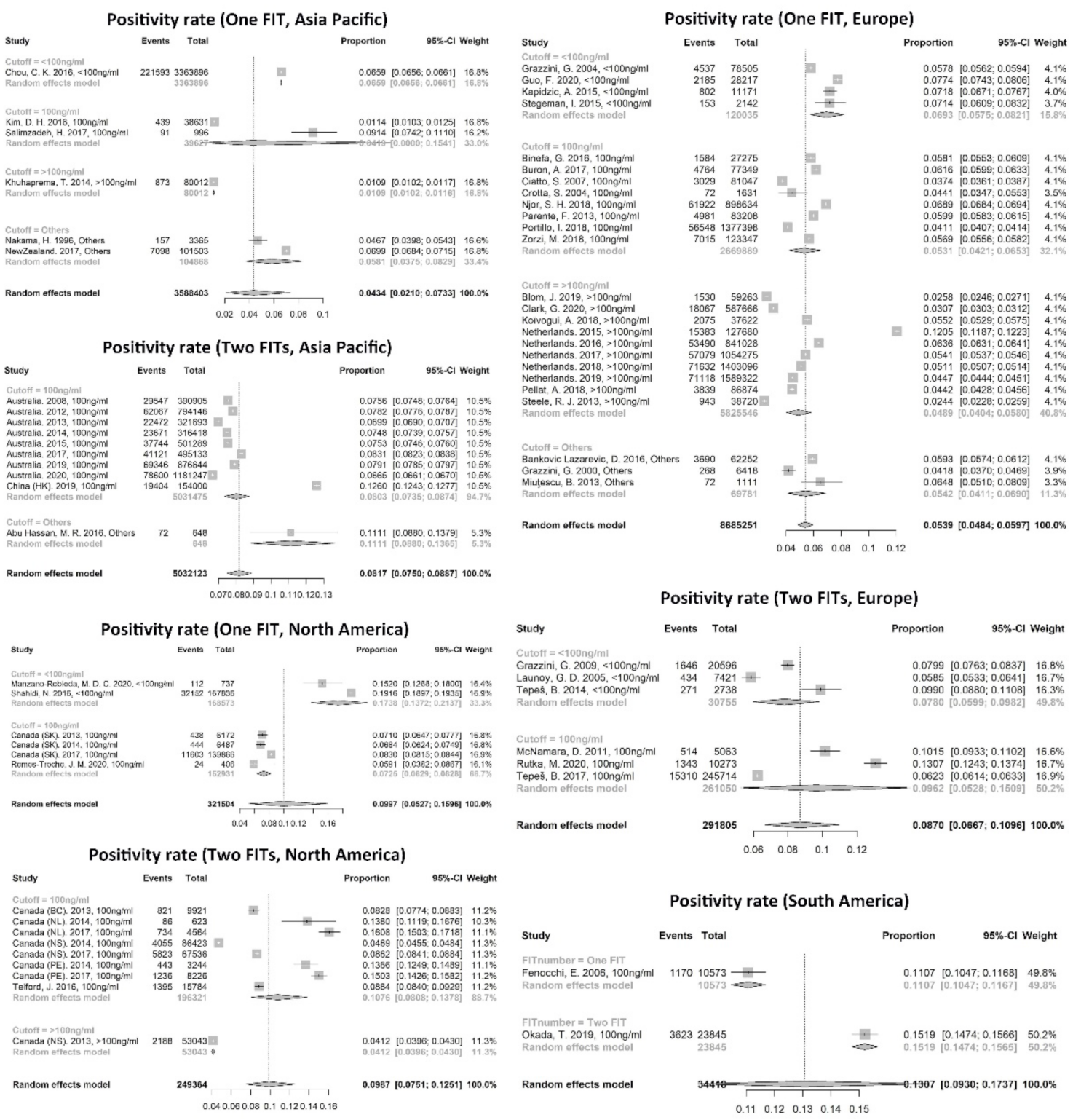
3.3. FIT Invalid Rate and Positivity Rate
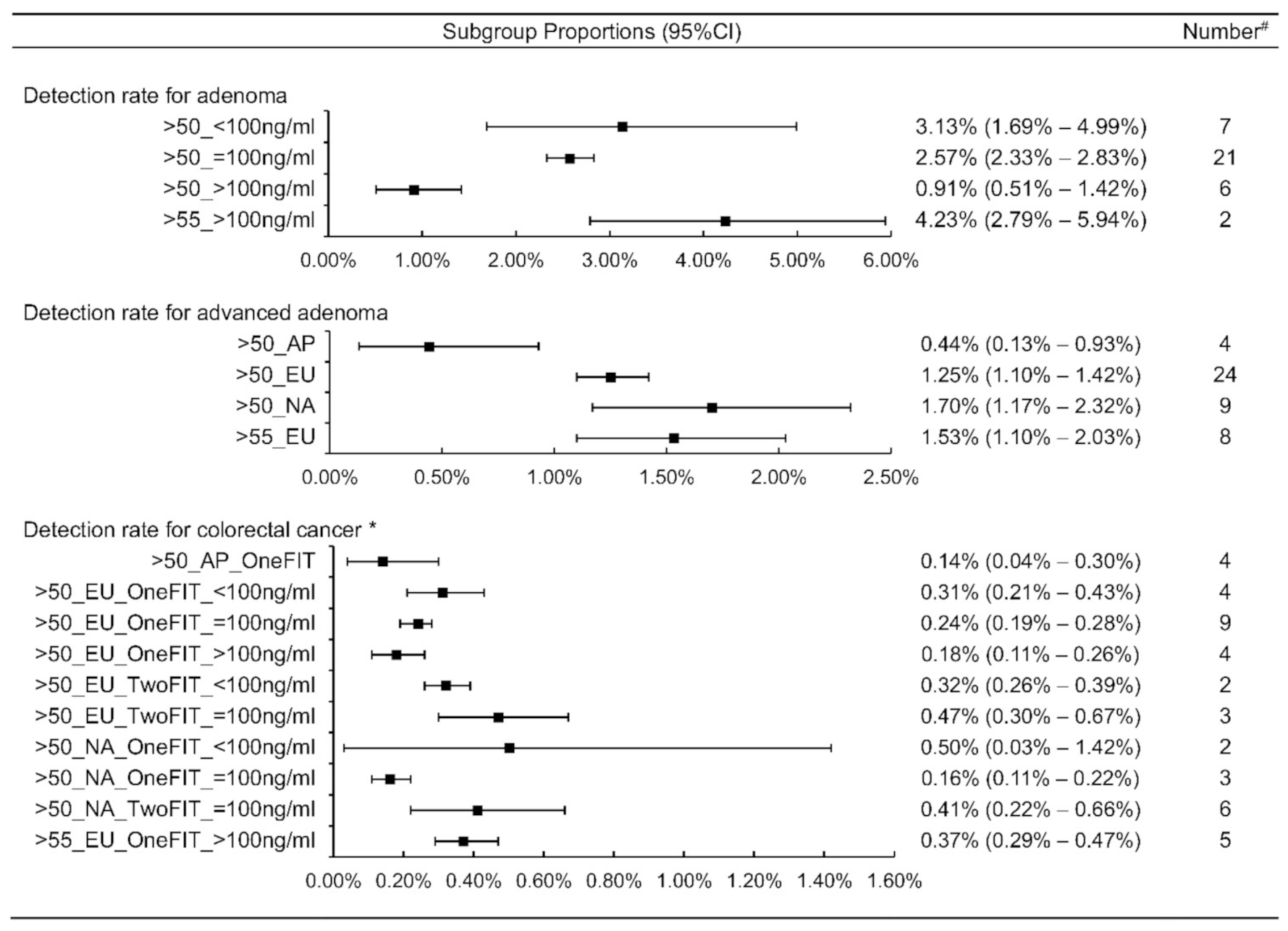
3.4. Detection Rate and PPV
3.5. Indicators Related to Colonoscopy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. Colorectal Cancer, December 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf (accessed on 17 January 2022).
- Hewitson, P.; Glasziou, P.; Watson, E.; Towler, B.; Irwig, L. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (Hemoccult): An update. Am. J. Gastroenterol. 2008, 103, 1541–1549. [Google Scholar] [CrossRef]
- Zorzi, M.; Fedeli, U.; Schievano, E.; Bovo, E.; Guzzinati, S.; Baracco, S.; Fedato, C.; Saugo, M.; Tos, A.P.D. Impact on colorectal cancer mortality of screening programmes based on the faecal immunochemical test. Gut 2015, 64, 784–790. [Google Scholar] [CrossRef]
- Stern, C. Flexible sigmoidoscopy versus fecal occult blood testing for colorectal cancer screening in asymptomatic individuals. Clin. J. Oncol. Nurs. 2014, 18, 471–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [Green Version]
- Mousavinezhad, M.; Majdzadeh, R.; Sari, A.A.; Delavari, A.; Mohtasham, F. The effectiveness of FOBT vs. FIT: A meta-analysis on colorectal cancer screening test. Med. J. Islam. Repub. Iran 2016, 30, 366. [Google Scholar]
- Lauby-Secretan, B.; Vilahur, N.; Bianchini, F.; Guha, N.; Straif, K. The IARC perspective on colorectal cancer screening. N. Engl. J. Med. 2018, 378, 1734–1740. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). Colorectal cancer screening. In IARC Handbook of Cancer Prevention; IARC: Lyon, France, 2019; Volume 17, pp. 1–300. [Google Scholar]
- Canadian Partnership against Cancer. Quality Determinants and Indicators for Measuring Colorectal Cancer Screening Program Performance in Canada; Canadian Partnership against Cancer: Toronto, ON, Canada, 2012. [Google Scholar]
- Lee, S.J.; Boscardin, W.J.; Stijacic-Cenzer, I.; Conell-Price, J.; O’Brien, S.; Walter, L.C. Time lag to benefit after screening for breast and colorectal cancer: Meta-analysis of survival data from the United States, Sweden, United Kingdom, and Denmark. BMJ 2013, 346, e8441. [Google Scholar] [CrossRef] [Green Version]
- Wools, A.; Dapper, E.A.; de Leeuw, J.R.J. Colorectal cancer screening participation: A systematic review. Eur. J. Public Health 2016, 26, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Liles, E.G.; Bent, S.; Levin, T.R.; Corley, D.A. Accuracy of fecal immunochemical tests for colorectal cancer: Systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Niedermaier, T.; Weigl, K.; Hoffmeister, M.; Brenner, H. Diagnostic performance of flexible sigmoidoscopy combined with fecal immunochemical test in colorectal cancer screening: Meta-analysis and modeling. Eur. J. Epidemiol. 2017, 32, 481–493. [Google Scholar] [CrossRef]
- Senore, C.; Basu, P.; Anttila, A.; Ponti, A.; Tomatis, M.; Vale, D.B.; Ronco, G.; Soerjomataram, I.; Primic-Žakelj, M.; Riggi, E.; et al. Performance of colorectal cancer screening in the European Union Member States: Data from the second European screening report. Gut 2018, 68, 1232–1244. [Google Scholar] [CrossRef] [PubMed]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Navarro, M.; Nicolas, A.; Ferrandez, A.; Lanas, A. Colorectal cancer population screening programs worldwide in 2016: An update. World J. Gastroenterol. 2017, 23, 3632–3642. [Google Scholar] [CrossRef] [PubMed]
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C. Cancer Screening in Report on the Implementation of the Council Recommendation on Cancer Screening; Screening Group, International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Wieten, E.; de Klerk, C.M.; van der Steen, A.; Ramakers, C.R.; Kuipers, E.J.; Hansen, B.E.; Lansdorp-Vogelaar, I.; Bossuyt, P.M.; Dekker, E.; Spaander, M.C.W. Equivalent accuracy of 2 quantitative fecal immunochemical tests in detecting advanced neoplasia in an organized colorectal cancer screening program. Gastroenterology 2018, 155, 1392–1399. [Google Scholar] [CrossRef] [Green Version]
- Segnan, N.; Patnick, J.; Von Karsa, L. European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- Rex, D.K.; Schoenfeld, P.S.; Cohen, J.; Pike, I.M.; Adler, D.G.; Fennerty, B.M.; Lieb, J.G.; Park, W.G.; Rizk, M.K.; Sawhney, M.S.; et al. Quality indicators for colonoscopy. Am. J. Gastroenterol. 2015, 110, 72–90. [Google Scholar] [CrossRef] [PubMed]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I 2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminski, M.F.; Robertson, D.J.; Senore, C.; Rex, D.K. Optimizing the quality of colorectal cancer screening worldwide. Gastroenterology 2020, 158, 404–417. [Google Scholar] [CrossRef]
- Peng, L.; Balavarca, Y.; Niedermaier, T.; Weigl, K.; Hoffmeister, M.; Brenner, H. Risk-adapted cutoffs in colorectal cancer screening by fecal immunochemical tests. Am. J. Gastroenterol. 2020, 115, 1110–1116. [Google Scholar] [CrossRef]
- Wilén, H.R.; Blom, J.; Höijer, J.; Hultcrantz, R. Fecal immunochemical test in colorectal cancer screening: Colonoscopy findings by different cut-off levels. J. Gastroenterol. Hepatol. 2019, 34, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; Kubik, M.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1965–1977. [Google Scholar]
- Von Karsa, L.; Patnick, J.; Segnan, N.; Atkin, W.; Halloran, S.; Lansdorp-Vogelaar, I.; Malila, N.; Minozzi, S.; Moss, S.; Quirke, P.; et al. European guidelines for quality assurance in colorectal cancer screening and diagnosis: Overview and introduction to the full supplement publication. Endoscopy 2013, 45, 51–59. [Google Scholar] [PubMed] [Green Version]
- Robertson, D.J.; Lee, J.K.; Boland, C.R.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Lieberman, D.; Levin, T.R.; Rex, D.K. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: A consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2017, 152, 1217–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, N.N.; Sutradhar, R.; Forbes, S.S.; Paszat, L.F.; Saskin, R.; Rabeneck, L. Analysis of administrative data finds endoscopist quality measures associated with postcolonoscopy colorectal cancer. Gastroenterology 2011, 140, 65–72. [Google Scholar] [CrossRef]
- Kaminski, M.F.; Thomas-Gibson, S.; Bugajski, M.; Bretthauer, M.; Rees, C.J.; Dekker, E.; Hoff, G.; Jover, R.; Suchanek, S.; Ferlitsch, M.; et al. Performance measures for lower gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) quality improvement initiative. Endoscopy 2017, 49, 378–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binefa, G.; Garcia, M.; Milà, N.; Fernández, E.; Rodríguez-Moranta, F.; Gonzalo, N.; Benito, L.; Clopés, A.; Guardiola, J.; Moreno, V. Colorectal cancer screening programme in Spain: Results of key performance indicators after five rounds (2000–2012). Sci. Rep. 2016, 6, 19532. [Google Scholar] [CrossRef] [PubMed]
- Hassan, C.; Rossi, P.G.; Camilloni, L.; Rex, D.K.; Jimenez-Cendales, B.; Ferroni, E.; Borgia, P.; Zullo, A.; Guasticchi, G.; HTA Group. Meta-analysis: Adherence to colorectal cancer screening and the detection rate for advanced neoplasia, according to the type of screening test. Aliment. Pharmacol. Ther. 2012, 36, 929–940. [Google Scholar] [CrossRef]
- National Health Service (NHS). Report of the Independent Review of Adult Screening Programmes in England; NHS: London, UK, 2019. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance Indicators | Studies | Number | Range | Estimates (95%CI) | I2 |
|---|---|---|---|---|---|
| Participation rate | 69 | 73,047,226 | (6.80%, 95.98%) | 54.00% (49.28–58.69%) | 100.0% |
| Invalid rate | 28 | 10,695,371 | (0.09%, 5.30%) | 1.08% (0.87–1.31%) | 99.9% |
| Positive rate | 74 | 24,374,662 | (1.09%, 30.01%) | 7.28% (6.81–7.76%) | 99.9% |
| Adenoma detection rate | 49 | 17,613,793 | (0.23%, 7.73%) | 2.26% (2.00–2.53%) | 99.9% |
| Advanced adenoma detection rate | 47 | 20,943,205 | (0.09%, 3.69%) | 1.26% (1.10–1.44%) | 99.9% |
| CRC detection rate | 61 | 23,584,358 | (0.00%, 1.16%) | 0.28% (0.25–0.31%) | 99.5% |
| PPV for adenoma | 52 | 823,533 | (11.11%, 72.68%) | 44.79% (41.8–47.79%) | 99.9% |
| PPV for advanced adenoma | 49 | 920,387 | (6.67%, 48.36%) | 27.13% (24.39–29.97%) | 99.9% |
| PPV for CRC | 61 | 973,245 | (0.0%, 15.07%) | 5.48% (4.96–6.02%) | 99.1% |
| Colonoscopy compliance rate | 69 | 1,310,390 | (31.42%, 96.01%) | 7/69 studies >90%, 30/69 studies > 80% | |
| Bowel preparation (adequate) | 14 | 202,936 | (65.20%, 97.30%) | 13/14 studies > 85% | |
| Colonoscopy completion rate | 40 | 798,029 | (73.16%, 100.00%) | 21/40 studies > 95%, 30/40 studies > 90% | |
| Colonoscopy complication rate | 27 | 811,334 | (0.00%, 1.23%) | 18/27 studies < 0.5% | |
| Performance Indicators | Meta-Regression | Significant Covariates a | Adjusted R2 | |||||
|---|---|---|---|---|---|---|---|---|
| Type | Continents | FIT Number | FIT Cutoff Value b | Age Group | Screening Round | |||
| Participation rate | Uni | √ | √ | √ | √ | √ | √ | - |
| Multi | Article: ref Report: −0.168 *** | AP: ref Euro: −0.221 *** NA: −0.104 ** SA: 0.266 *** | One: ref Two: −0.135 *** | - | >50 yrs: ref >55 yrs: 0.322 *** | Initial: ref Subsequent: −0.099 *** | 86.98% | |
| Invalid rate | Uni | - | √ | √ | √ | - | - | - |
| Multi | - | Euro: ref NA: 0.048 ** | One: ref Two: 0.032 *** | <100 ng/mL: ref >100 ng/mL: 0.048 ** | - | - | 54.63% | |
| Positive rate | Uni | √ | √ | √ | √ | √ | √ | - |
| Multi | - | AP: ref Euro: 0.04 ** NA: 0.082 *** SA: 0.139 *** | One: ref Two: 0.048 *** | <100 ng/mL: ref 100 ng/mL: −0.037 ** >100 ng/mL: −0.083 *** | - | - | 21.25% | |
| FIT adenoma detection rate | Uni | √ | √ | √ | √ | √ | - | - |
| Multi | - | - | - | <100 ng/mL: ref >100 ng/mL: −0.062 *** | >50 yrs: ref >55 yrs: 0.063 *** | - | 41.13% | |
| FIT advanced adenoma detection rate | Uni | - | √ | √ | √ | √ | √ | - |
| Multi | - | AP: ref Euro: 0.053 *** NA: 0.062 *** SA: 0.044 * | - | - | >50 yrs: ref >55 yrs: 0.029 *** | - | 50.46% | |
| FIT CRC detection rate | Uni | - | √ | √ | √ | √ | √ | - |
| Multi | - | AP: ref Euro: 0.013 *** NA: 0.012 * SA: 0.054 *** | One: ref Two: 0.013 *** | <100 ng/mL: ref >100 ng/mL: −0.009 * | >50 yrs: ref >55 yrs: 0.015 *** | - | 56.11% | |
| PPV for adenoma | Uni | √ | √ | - | - | √ | √ | - |
| Multi | - | - | - | - | >50 yrs: ref >55 yrs: 0.112 * | - | 25.56% | |
| PPV for advanced adenoma | Uni | - | √ | √ | √ | √ | - | - |
| Multi | - | AP: ref Euro: 0.130 *** NA: 0.090 * | - | <100 ng/mL: ref 100 ng/mL: 0.087 ** >100 ng/mL: 0.088 ** | - | - | 63.85% | |
| PPV for CRC | Uni | - | √ | - | √ | √ | - | - |
| Multi | - | AP: ref SA: 0.011 * | - | - | - | - | 54.83% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, H.; Lin, J.; Xu, Z.; Chen, X.; Wang, H.H.X.; Huang, L.; Huang, J.; Zheng, Z.; Wong, M.C.S. A Global Evaluation of the Performance Indicators of Colorectal Cancer Screening with Fecal Immunochemical Tests and Colonoscopy: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 1073. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041073
Ding H, Lin J, Xu Z, Chen X, Wang HHX, Huang L, Huang J, Zheng Z, Wong MCS. A Global Evaluation of the Performance Indicators of Colorectal Cancer Screening with Fecal Immunochemical Tests and Colonoscopy: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(4):1073. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041073
Chicago/Turabian StyleDing, Hanyue, Jiaye Lin, Zijun Xu, Xiao Chen, Harry H. X. Wang, Liwen Huang, Junjie Huang, Zhijie Zheng, and Martin C. S. Wong. 2022. "A Global Evaluation of the Performance Indicators of Colorectal Cancer Screening with Fecal Immunochemical Tests and Colonoscopy: A Systematic Review and Meta-Analysis" Cancers 14, no. 4: 1073. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041073