
Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners

 ,
, 
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Training
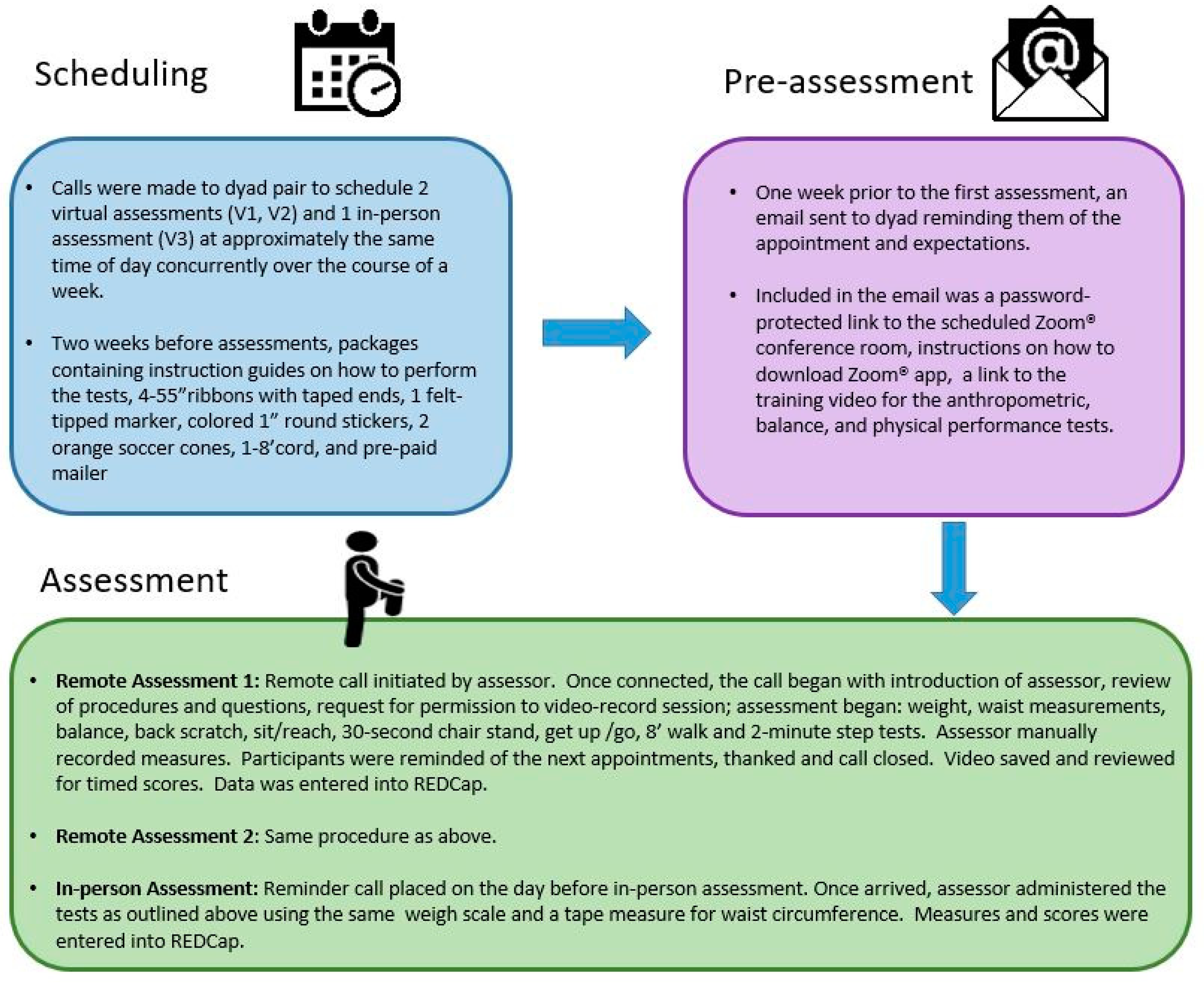
2.4. Procedures
2.5. Anthropometric Measures
2.6. Physical Performance Measures
2.7. Data Analysis
2.8. Sample Size Considerations
3. Results
3.1. Demographics and Characteristics
3.2. Validity and Reliability Results—Overall Sample
3.3. Validity and Reliability Results—Survivors and Partners
3.4. Validity and Reliability Results—Balance
3.5. Feasibility Benchmarks
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denlinger, C.S.; Sanft, T.; Moslehi, J.J.; Overholser, L.; Armenian, S.; Baker, K.S.; Broderick, G.; Demark-Wahnefried, W.; Friedman, D.L.; Goldman, M.; et al. NCCN Guidelines Insights: Survivorship, Version 2.2020. J. Natl. Compr. Cancer Netw. 2020, 18, 1016–1023. [Google Scholar] [CrossRef]
- Gan, T.; Cheng, H.-L.; Tse, M.M.Y. Feasibility, acceptability, and effects of behavior change interventions for improving multiple dietary behaviors among cancer survivors: A systematic review. Support. Care Cancer 2021, 30, 2877–2889. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Ogawa, E.F.; Harris, R.; Dufour, A.B.; Morey, M.C.; Bean, J. Reliability of virtual physical performance assessments in veterans during the COVID-19 pandemic. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100146. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.; Lipps, C.; Guidarelli, C.; Herrera-Fuentes, P. Converting Physical Function Testing to the Remote Setting: Adapting Our Research Protocol During COVID-19. Innov. Aging 2020, 4, 936–937. [Google Scholar] [CrossRef]
- Blair, C.K.; Harding, E.; Herman, C.; Boyce, T.; Demark-Wahnefried, W.; Davis, S.; Kinney, A.Y.; Pankratz, V.S. Remote Assessment of Functional Mobility and Strength in Older Cancer Survivors: Protocol for a Validity and Reliability Study. JMIR Res. Protoc. 2020, 9, e20834. [Google Scholar] [CrossRef]
- Bierer, B.; White, S.; Barnes, J.; Gelinas, L. Ethical Challenges in Clinical Research During the COVID-19 Pandemic. J. Bioethical Inq. 2020, 17, 717–722. [Google Scholar] [CrossRef]
- Doherty, G.J.; Goksu, M.; De Paula, B.H.R. Rethinking cancer clinical trials for COVID-19 and beyond. Nat. Cancer 2020, 1, 568–572. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19): Information for NIH Applicants and Recipients of NIH Funding; National Institute of Health, US Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-20-087.html (accessed on 23 September 2021).
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wu-han, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekhlyudov, L.; Duijts, S.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.; Smith, K.C.; Tevaarwerk, A.; Yu, X.; et al. Addressing the needs of cancer survivors during the COVID-19 pandemic. J. Cancer Surviv. 2020, 14, 601–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabhan, C.; Choueiri, T.K.; Mato, A.R. Rethinking Clinical Trials Reform During the COVID-19 Pandemic. JAMA Oncol. 2020, 6, 1327. [Google Scholar] [CrossRef]
- Marra, D.E.; Hamlet, K.M.; Bauer, R.M.; Bowers, D. Validity of teleneuropsychology for older adults in response to COVID-19: A systematic and critical review. Clin. Neuropsychol. 2020, 34, 1411–1452. [Google Scholar] [CrossRef]
- Chipps, J.; Brysiewicz, P.; Mars, M. A Systematic Review of the Effectiveness of Videoconference-Based Tele-Education for Medical and Nursing Education. Worldviews Evid.-Based Nurs. 2012, 9, 78–87. [Google Scholar] [CrossRef]
- Rush, K.L.; Hatt, L.; Janke, R.; Burton, L.; Ferrier, M.; Tetrault, M. The efficacy of telehealth delivered educational approaches for patients with chronic diseases: A systematic review. Patient Educ. Couns. 2018, 101, 1310–1321. [Google Scholar] [CrossRef] [Green Version]
- Matcham, F.; Pietro, C.B.D.S.; Bulgari, V.; de Girolamo, G.; Dobson, R.; Eriksson, H.; Folarin, A.A.; Haro, J.M.; Kerz, M.; Lamers, F.; et al. Remote assessment of disease and relapse in major depressive disorder (RADAR-MDD): A multi-centre prospective cohort study protocol. BMC Psychiatry 2019, 19, 72. [Google Scholar] [CrossRef] [Green Version]
- Bove, R.; Garcha, P.; Bevan, C.J.; Crabtree-Hartman, E.; Green, A.J.; Gelfand, J.M. Clinic to in-home telemedicine reduces barriers to care for patients with MS or other neuroimmunologic conditions. Neurol.-Neuroimmunol. Neuroinflamm. 2018, 5, e505. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.J.E.; Dabbs, A.D.; Hergenroeder, A.L.; Vendetti, M.L.; Jones, K.B.; Willey, B.M.; Morrell, M.R.; Imes, C.C. Considerations for assessing physical function and physical activity in clinical trials during the COVID-19 pandemic. Contemp. Clin. Trials 2021, 105, 106407. [Google Scholar] [CrossRef]
- Mallow, J.A.; Petitte, T.; Narsavage, G.; Barnes, E.; Theeke, E.; Mallow, B.K.; Theeke, L.A. The Use of Video Conferencing for Persons with Chronic Conditions: A Systematic Review. E-Health Telecommun. Syst. Netw. 2016, 5, 39–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidoo, N.; Nguyen, V.T.; Ravaud, P.; Young, B.; Amiel, P.; Schanté, D.; Clarke, M.; Boutron, I. The research burden of randomized controlled trial participation: A systematic thematic synthesis of qualitative evidence. BMC Med. 2020, 18, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, D.; Asghar, A.; Kenworthy-Heinige, T.; Johnson, M.R.; Willis, C.; Kantorowicz, A.S.; Condon, D.L.; Huang, G.D. Increasing access to clinical research using an innovative mobile recruit-ment approach: The (MoRe) concept. Contemp. Clin. Trials Commun. 2020, 19, 100623. [Google Scholar] [CrossRef] [PubMed]
- Pekmezi, D.W.; Crane, T.E.; Oster, R.A.; Rogers, L.Q.; Hoenemeyer, T.; Farrell, D.; Cole, W.W.; Wolin, K.; Badr, H.; Demark-Wahnefried, W. Rationale and Methods for a Randomized Controlled Trial of a Dyadic, Web-Based, Weight Loss Intervention among Cancer Survivors and Partners: The DUET Study. Nutrition 2021, 13, 3472. [Google Scholar] [CrossRef] [PubMed]
- CDC Calls on Americans to Wear Masks to Prevent COVID-19 Spread; Centers for Disease Control and Prevention, Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.cdc.gov/media/releases/2020/p0714-americans-to-wear-masks.html (accessed on 15 October 2021).
- Lohman, T.J.; Roache, A.F.; Martorell, R. Anthropometric Standardization Reference Manual. Med. Sci. Sports Exerc. 1992, 24, 952. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.C.; Rikli, R.E. Measuring functional. J. Funct. Aging 2002, 7, 24–30. Available online: https://www.medicina.univr.it/documenti/OccorrenzaIns/matdid/matdid182478.pdf (accessed on 10 December 2021).
- Podsiadlo, D.; Richardson, S. The timed “up and go”: A test of basic functional mobility for frail elderly persons. J. Am. Gerontol. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- The Four-Stage Balance Test Assessment; Centers for Disease Control and Prevention, Department of Health and Human Services: Washington, DC, USA, 2017. Available online: https://www.cdc.gov/steadi/pdf/4-Stage_Balance_Test-print.pdf (accessed on 2 October 2021).
- Bland, M.J.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Rosner, B. Fundamentals of Biostatistics, 8th ed.; Cengage Learning: Boston, MA, USA, 2016. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Naaman, R.; Parrett, A.; Bashawri, D.; Campo, I.; Fleming, K.; Nichols, B.; Burleigh, E.; Murtagh, J.; Reid, J.; Gerasimidis, K. Assessment of Dietary Intake Using Food Photography and Video Recording in Free-Living Young Adults: A Comparative Study. J. Acad. Nutr. Diet. 2021, 121, 749–761.e1. [Google Scholar] [CrossRef] [PubMed]
- Batalik, L.; Winnige, P.; Dosbaba, F.; Vlazna, D.; Janikova, A. Home-Based Aerobic and Resistance Exercise Interventions in Cancer Patients and Survivors: A Systematic Review. Cancers 2021, 13, 1915. [Google Scholar] [CrossRef] [PubMed]
- Ibeggazene, S.; Turner, R.; Rosario, D.; Bourke, L. Remote interventions to improve exercise behaviour in sedentary people living with and beyond cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.M.; Boisvert, C.; Li, F.; Lyons, K.S.; Beer, T.M.; Mitri, Z.; Meyers, G.; Eckstrom, E.; Campbell, K.L. Delivering exercise medicine to cancer survivors: Has COVID-19 shifted the landscape for how and who can be reached with supervised group exercise? Support. Care Cancer 2021, 30, 1903–1906. [Google Scholar] [CrossRef]
- Paschal, K.; Oswald, A.; Siegmund, R.; Siegmund, S.; Threlkeld, J. Test-retest reliability of the physical performance test for persons with Parkinson disease. J. Geriatr. Phys. Ther. 2006, 29, 82–86. [Google Scholar] [CrossRef]
- Dahl, A.K.; Hassing, L.B.; Fransson, E.; Pedersen, N.L. Agreement between self-reported and measured height, weight and body mass index in old age—A longitudinal study with 20 years of follow-up. Age Ageing 2010, 39, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Kuczmarski, M.F.; Kuczmarski, R.J.; Najjar, M. Effects of age on validity of self-reported height, weight, and body mass index: Findings from the Third National Health and Nutrition Examination Survey, 1988–1994. J. Am. Diet Assoc. 2001, 101, 28–34. [Google Scholar] [CrossRef]
- Villanueva, E.V. The validity of self-reported weight in US adults: A population based cross-sectional study. BMC Public Health 2001, 1, 11. [Google Scholar] [CrossRef] [Green Version]
- Sahyoun, N.R.; Maynard, L.M.; Zhang, X.L.; Serdula, M.K. Factors associated with errors in self-reported height and weight in older adults. J. Nutr. Health Aging 2008, 12, 108–115. [Google Scholar] [CrossRef]
- Khunti, K.; Taub, N.; Webb, D.; Srinivasan, B.; Stockman, J.; Griffin, S.J.; Simmons, R.; Davies, M. Validity of self-assessed waist circumference in a multi-ethnic UK population. Diabet. Med. 2011, 29, 404–409. [Google Scholar] [CrossRef]
- Ghosh-Dastidar, M.; Nicosia, N.; Datar, A. A novel approach to anthropometric assessment for geographically dispersed samples: A pilot study. Prev. Med. Rep. 2020, 19, 101125. [Google Scholar] [CrossRef] [PubMed]
- Sobhiyeh, S.; Kennedy, S.; Dunkel, A.; Dechenaud, M.E.; Weston, J.A.; Shepherd, J.; Wolenski, P.; Heymsfield, S.B. Digital anthropometry for body circumference measurements: Toward the development of universal three-dimensional optical system analysis software. Obes. Sci. Pr. 2021, 7, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Sawers, A.; Hafner, B.J. Characterizing Practice Effects in Performance-Based Tests Administered to Users of Unilateral Lower Limb Prostheses: A Preliminary Study. PMR 2020, 13, 969–978. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 Measure | COVID-19 Modification |
|---|---|
| Weight assessed in light clothing, without shoes, on a calibrated scale set on a hard surface observed in-person by assessor. Weight is measured twice, averaged, and recorded. | Modification for virtual assessments 1 and 2: participant’s scale is used; camera is positioned so assessor can see scale face. Participant is asked to “zero out” the scale prior to stepping on it. Modification for in-person assessment: assessor weighs the participants on the same scale as used in V1, V2. |
| Waist circumference assessed by assessor using a non-stretch tape measure, at level of umbilicus and upon exhale. | Modification for virtual assessments 1 and 2: Camera is place on floor angled up to capture midsection of participant and partner or placed on table/chair facing both so mid-section is in frame. Assessor instructs partner to place the taped end of the ribbon on the umbilicus; holding taped end in place, partner wraps the ribbon snugly around the waist (shirt lifted) placing ribbon parallel to the ground. Participant is asked to rotate in front of the camera to assure the ribbon is flat against the skin and parallel to the ground. Once proper technique is confirmed by the assessor, participant is asked to inhale, and, upon exhale, partner marks the point where the ribbon overlaps. The test is repeated and both ribbons are mailed back to assessor to be measured. |
| Original Measure (All of Which Have Proven Reliability and Validity) | Adaptations of the Reference Test to Permit Virtual Assessments |
|---|---|
| Sit-and-reach: a test of flexibility [28]. | The camera is placed on floor at a 90-degree angle with direct view of seated participant with bent and extended legs in frame; assessor guides participant and partner in measuring distance and participant through procedure. |
| 30 s chair stand: a test of lower body strength [28]. | The camera is placed on floor angled to see participant in both seated and standing positions or held by partner; assessor instructs participant to place the chair against a wall to prevent it from moving during test and guides the participant and partner through test procedure. |
| Back scratch: a test of lower body strength [28]. | The camera is placed on table or counter, angled to see participant’s back and observe the partner’s measurements, as well as which side is being measured, using standard vinyl tape measure included in study supplies package. Assessor guides participant and partner on test protocol. |
| 8’ Get-up-and-go (TUG): a test of lower body strength [29] | The camera is placed on floor to observe partner measure 8’ distance using 8’ cord included in study materials (along with color stickers and orange cones to serve as “markers”). Camera is positioned on floor or held by partner so that seated participant and orange cone marking 8’ end point are in frame. Assessor gives signal to “go” after ensuring participant is correct starting position. Timed score is recorded after viewing time stamp on video recording. |
| Timed 8’ Walk: a test to assess gait [28]. | Assessor instructs partner to move cone out horizontally from previous test and place the other cone adjacent for mark “finish line’ with space wide enough for passage. The camera is placed on floor at a distance that captures the chair and the orange cones that signify the “finish line”. Time is stopped as soon as participant breaks the plane of the “finish line”. Timed score is recorded after viewing time stamp on video recording. |
| 2 min step test: a test to assess endurance [28]. | The camera is placed on floor angled towards wall to ensure proper measurement and sticker placement, i.e., a sticker is placed on the wall that corresponds to the measured midpoint between the trochanter and patella, and then the distance between that midpoint to the floor below (see script). The camera is then angled so that a full view of participant (head-to-toe) is in frame. Assessor instructs participant not to talk during test, to draw-up knee to the height of the sticker with each step, and to rest as needed. Partner is instructed to spot as needed, Score on completed steps is recorded. |
| Measure | Virtual 1 (V1) Mean (SD) | Virtual 2 (V2) Mean (SD) | ICC (95% CI) (V1 vs. V2) * | Mean Difference (V1–V2) | Limits of Agreement (V1–V2) | p-Value |
|---|---|---|---|---|---|---|
| Weight (kg) [n = 71] | 86.2 (21.0) | 87.4 (18.8) | 0.93 (0.89, 0.96) | −1.2 (7.5) | −15.9, 13.5 | 0.18 |
| Waist Circumference (cm) [n = 73] | 107.9 (14.9) | 107.4 (15.1) | 0.98 (0.97, 0.99) | 0.5 (2.8) | −4.9, 6.0 | 0.11 |
| 30 s Chair stand (reps) [n = 74] | 10.7 (3.0) | 12.0 (3.5) | 0.80 (0.69, 0.87) | −1.3 (2.1) | −5.4, 2.9 | <0.001 |
| 8’ Get Up/Go (sec to 10th) [n = 74] | 7.8 (2.1) | 7.4 (1.6) | 0.74 (0.62, 0.83) | 0.5 (1.4) | −2.3, 3.2 | 0.006 |
| 8’ Walk (sec to 10th) [n = 74] | 2.2 (0.5) | 2.2 (0.4) | 0.47 (0.27, 0.63) | 0.0 (0.5) | −0.9, 1.0 | 0.64 |
| Sit & Reach (cm) [n = 73] | −0.7 (3.5) | −0.3 (3.2) | 0.86 (0.78, 0.91) | −0.4 (1.8) | −4.0, 3.1 | 0.047 |
| Back scratch (cm) [n = 72] | −3.5 (3.4) | −3.4 (3.4) | 0.90 (0.84, 0.93) | −0.0 (1.5) | −3.0, 3.0 | 0.96 |
| 2-min step test (# steps) [n = 74] | 77.3 (23.3) | 82.4 (22.8) | 0.87 (0.80, 0.92) | −5.1 (11.8) | −28.1, 18.0 | <0.001 |
| Measure | (V1 + V2)/2 Mean (SD) | In-Person Mean (SD) | ICC and 95% CI (Average Virtual vs. In-Person) * | Mean Difference (Average Virtual vs. In-Person) | Limits of Agreement (Average Virtual vs. In-Person) | p-Value |
|---|---|---|---|---|---|---|
| Weight (kg) [n = 71] | 86.8 (19.5) | 87.2 (18.6) | 0.98 (0.97, 0.99) | −0.4 (3.9) | −8.0, 7.3 | 0.43 |
| Waist Circumference (cm) [n = 73] | 107.7 (14.9) | 103.6 (15.5) | 0.96 (0.93, 0.97) | 4.1 (4.6) | −4.9, 13.0 | <0.001 |
| 30 s Chair stand (reps) [n = 74] | 11.3 (3.1) | 12.1 (3.3) | 0.86 (0.79, 0.92) | −0.7 (1.7) | −4.0, 2.5 | <0.001 |
| 8’ Get Up/Go (sec to 10th) [n = 74] | 7.6 (1.7) | 7.5 (1.4) | 0.80 (0.70, 0.87) | 0.1 (1.0) | −1.9, 2.1 | 0.32 |
| 8’ Walk (sec to 10th) [n = 74] | 2.2 (0.4) | 2.2(0.4) | 0.65 (0.49, 0.76) | 0.0 (0.3) | −0.6, 0.7 | 0.35 |
| Sit & Reach (cm) [n = 73] | −0.5 (3.2) | −0.0 (3.2) | 0.89 (0.82, 0.93) | −0.5 (1.5) | −3.5, 2.5 | 0.009 |
| Back scratch (cm) [n = 72] | −3.5 (3.3) | −3.1 (3.2) | 0.95 (0.92, 0.97) | −0.4 (1.0) | −2.4, 1.6 | 0.003 |
| 2-min step test (# steps) [n = 74] | 79.8 (22.3) | 85.3 (25.9) | 0.84 (0.76, 0.90) | −5.5 (13.9) | −32.8, 21.9 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoenemeyer, T.W.; Cole, W.W.; Oster, R.A.; Pekmezi, D.W.; Pye, A.; Demark-Wahnefried, W. Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners. Cancers 2022, 14, 1075. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041075
Hoenemeyer TW, Cole WW, Oster RA, Pekmezi DW, Pye A, Demark-Wahnefried W. Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners. Cancers. 2022; 14(4):1075. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041075
Chicago/Turabian StyleHoenemeyer, Teri W., William W. Cole, Robert A. Oster, Dorothy W. Pekmezi, Andrea Pye, and Wendy Demark-Wahnefried. 2022. "Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners" Cancers 14, no. 4: 1075. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041075