
Completion of FLOT Therapy, Regardless of Tumor Regression, Significantly Improves Overall Survival in Patients with Esophageal Adenocarcinoma


 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Selection, Study Design, and Inclusion Criteria
2.2. Statistical Analysis
2.3. Statement of Ethics
3. Results
3.1. Clinical Data
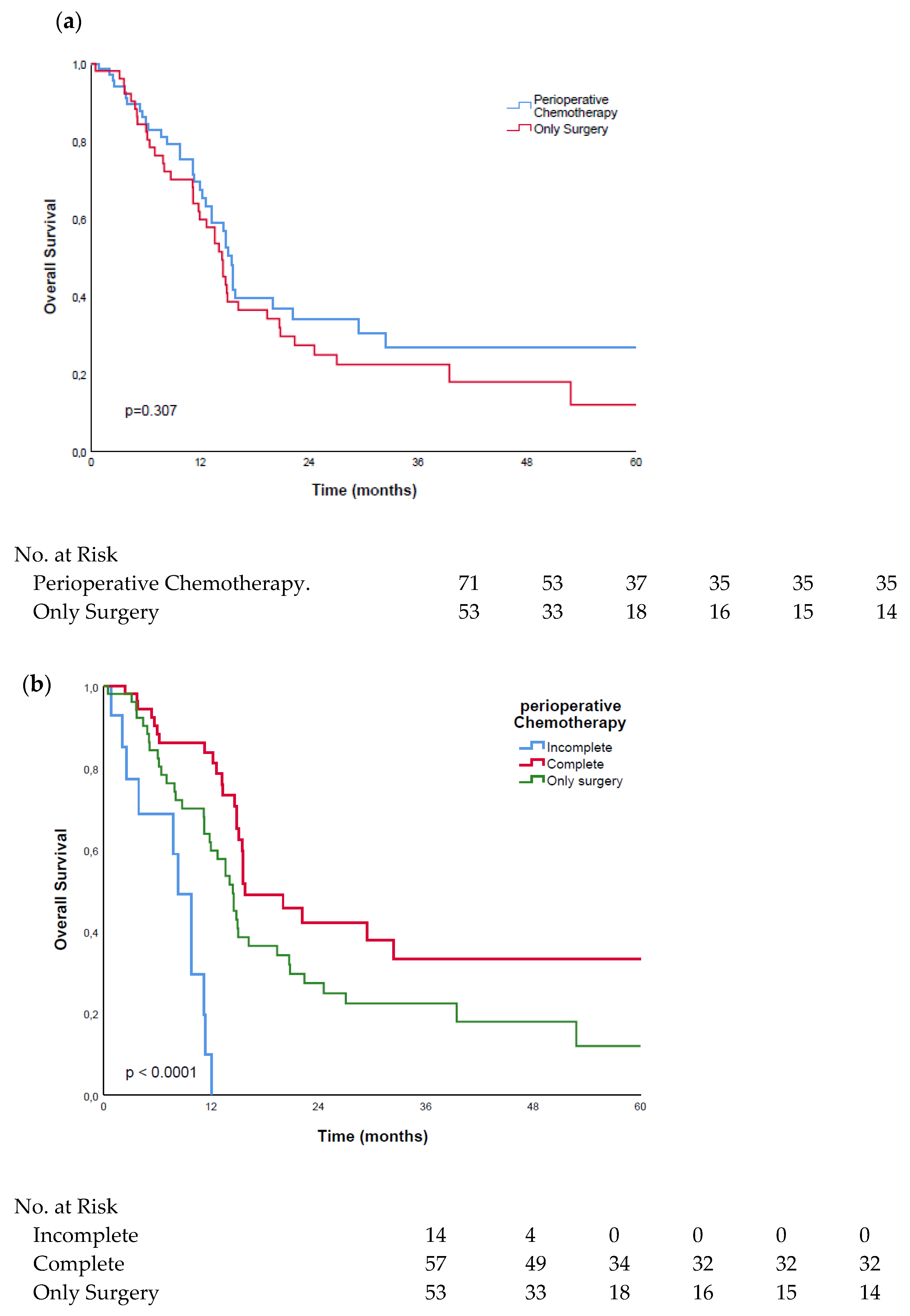
3.2. Surgery Alone vs. FLOT
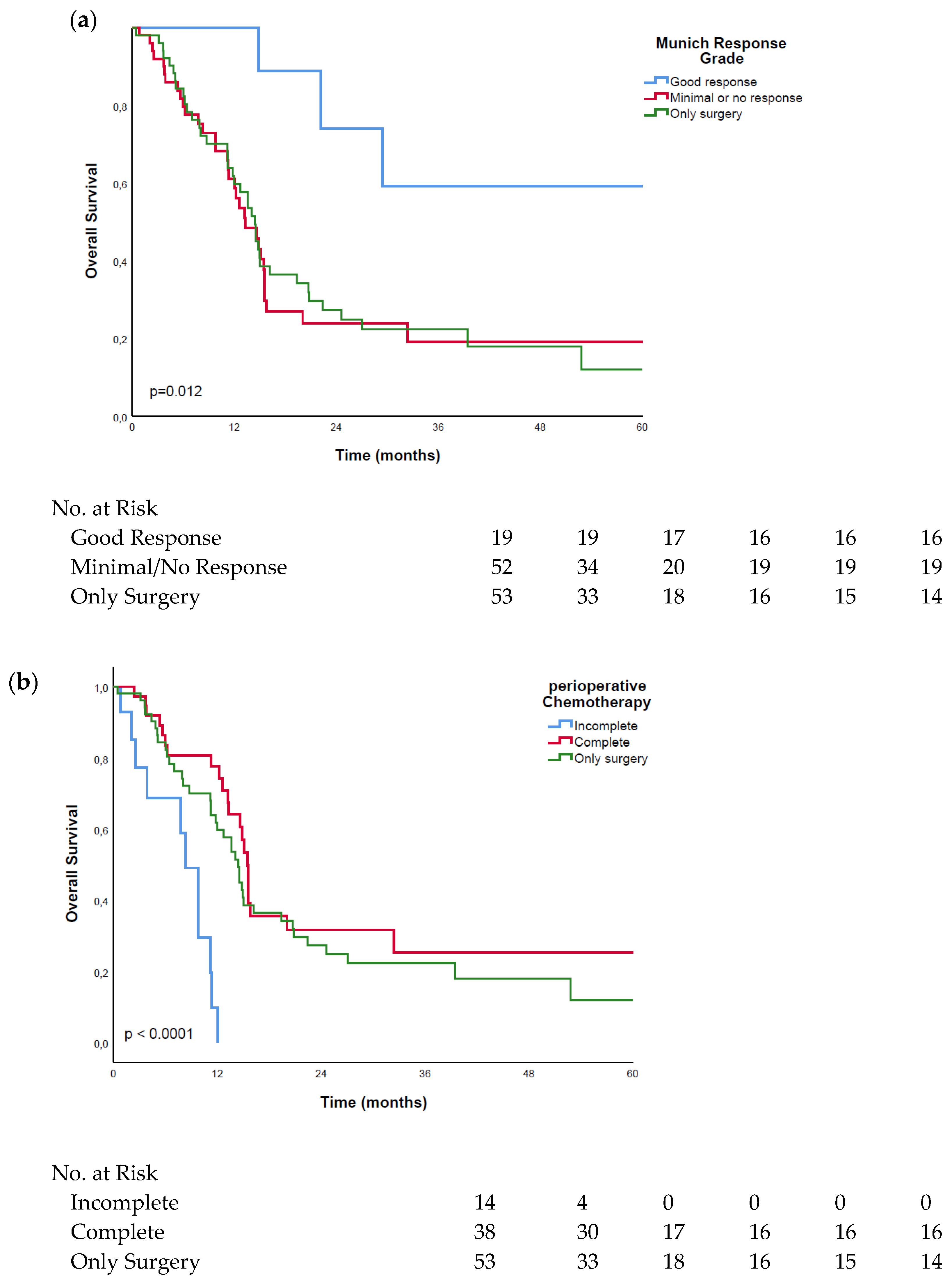
3.3. Good Response vs. Minimal or No Response
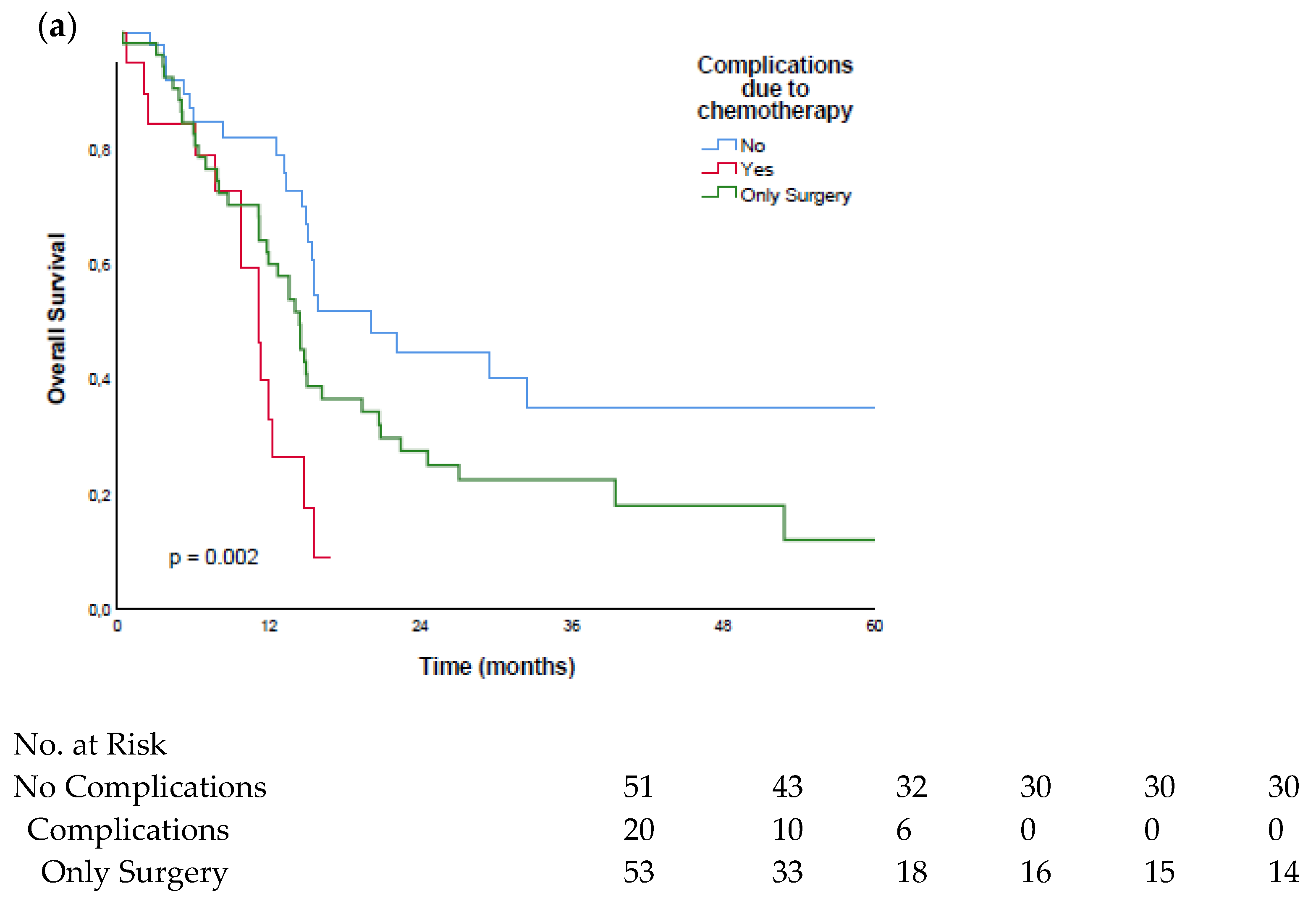
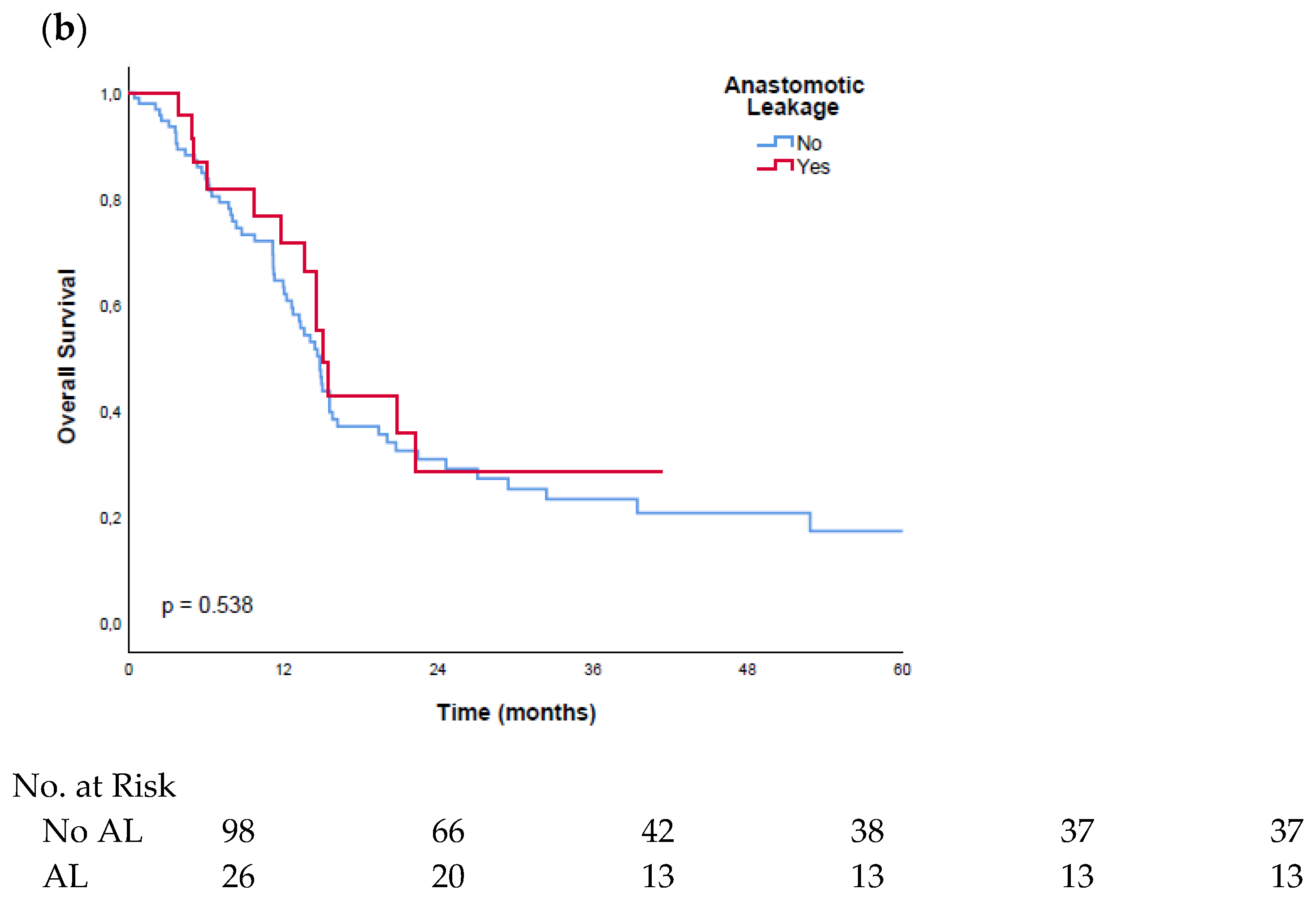
3.4. Surgical Complications vs. Chemotherapy Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Short, M.W.; Burgers, K.G.; Fry, V.T. Esophageal Cancer. Am. Fam. Physician 2017, 95, 22–28. [Google Scholar] [PubMed]
- Pennathur, A.; Gibson, M.K.; Jobe, B.A.; Luketich, J.D. Oesophageal Carcinoma. Lancet Lond. Engl. 2013, 381, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Lepage, C.; Rachet, B.; Jooste, V.; Faivre, J.; Coleman, M.P. Continuing Rapid Increase in Esophageal Adenocarcinoma in England and Wales. Am. J. Gastroenterol. 2008, 103, 2694–2699. [Google Scholar] [CrossRef]
- Rubenstein, J.H.; Taylor, J.B. Meta-Analysis: The Association of Oesophageal Adenocarcinoma with Symptoms of Gastro-Oesophageal Reflux. Aliment. Pharmacol. Ther. 2010, 32, 1222–1227. [Google Scholar] [CrossRef]
- Turati, F.; Tramacere, I.; La Vecchia, C.; Negri, E. A Meta-Analysis of Body Mass Index and Esophageal and Gastric Cardia Adenocarcinoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 609–617. [Google Scholar] [CrossRef]
- Tramacere, I.; La Vecchia, C.; Negri, E. Tobacco Smoking and Esophageal and Gastric Cardia Adenocarcinoma: A Meta-Analysis. Epidemiol. Camb. Mass 2011, 22, 344–349. [Google Scholar] [CrossRef]
- Allum, W.H.; Stenning, S.P.; Bancewicz, J.; Clark, P.I.; Langley, R.E. Long-Term Results of a Randomized Trial of Surgery with or without Preoperative Chemotherapy in Esophageal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5062–5067. [Google Scholar] [CrossRef]
- Kelsen, D.P.; Ginsberg, R.; Pajak, T.F.; Sheahan, D.G.; Gunderson, L.; Mortimer, J.; Estes, N.; Haller, D.G.; Ajani, J.; Kocha, W.; et al. Chemotherapy Followed by Surgery Compared with Surgery Alone for Localized Esophageal Cancer. N. Engl. J. Med. 1998, 339, 1979–1984. [Google Scholar] [CrossRef] [Green Version]
- Bolger, J.C.; Donohoe, C.L.; Lowery, M.; Reynolds, J.V. Advances in the Curative Management of Oesophageal Cancer. Br. J. Cancer 2021. [Google Scholar] [CrossRef]
- Glatz, T.; Verst, R.; Kuvendjiska, J.; Bronsert, P.; Becker, H.; Hoeppner, J.; Kulemann, B. Pattern of Recurrence and Patient Survival after Perioperative Chemotherapy with 5-FU, Leucovorin, Oxaliplatin and Docetaxel (FLOT) for Locally Advanced Esophagogastric Adenocarcinoma in Patients Treated Outside Clinical Trials. J. Clin. Med. 2020, 9, 2654. [Google Scholar] [CrossRef]
- Burmeister, B.H.; Thomas, J.M.; Burmeister, E.A.; Walpole, E.T.; Harvey, J.A.; Thomson, D.B.; Barbour, A.P.; Gotley, D.C.; Smithers, B.M. Is Concurrent Radiation Therapy Required in Patients Receiving Preoperative Chemotherapy for Adenocarcinoma of the Oesophagus? A Randomised Phase II Trial. Eur. J. Cancer 2011, 47, 354–360. [Google Scholar] [CrossRef]
- Hoeppner, J.; Lordick, F.; Brunner, T.; Glatz, T.; Bronsert, P.; Röthling, N.; Schmoor, C.; Lorenz, D.; Ell, C.; Hopt, U.T.; et al. ESOPEC: Prospective Randomized Controlled Multicenter Phase III Trial Comparing Perioperative Chemotherapy (FLOT Protocol) to Neoadjuvant Chemoradiation (CROSS Protocol) in Patients with Adenocarcinoma of the Esophagus (NCT02509286). BMC Cancer 2016, 16, 503. [Google Scholar] [CrossRef] [Green Version]
- Hoeppner, J.; Zirlik, K.; Brunner, T.; Bronsert, P.; Kulemann, B.; Sick, O.; Marjanovic, G.; Hopt, U.T.; Makowiec, F. Multimodal Treatment of Locally Advanced Esophageal Adenocarcinoma: Which Regimen Should We Choose? Outcome Analysis of Perioperative Chemotherapy versus Neoadjuvant Chemoradiation in 105 Patients. J. Surg. Oncol. 2014, 109, 287–293. [Google Scholar] [CrossRef]
- van Hagen, P.; Hulshof, M.C.C.M.; van Lanschot, J.J.B.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; Richel, D.J.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Preoperative Chemoradiotherapy for Esophageal or Junctional Cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.H.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ychou, M.; Boige, V.; Pignon, J.-P.; Conroy, T.; Bouché, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.-M.; Saint-Aubert, B.; et al. Perioperative Chemotherapy Compared with Surgery Alone for Resectable Gastroesophageal Adenocarcinoma: An FNCLCC and FFCD Multicenter Phase III Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.-G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative Chemotherapy with Fluorouracil plus Leucovorin, Oxaliplatin, and Docetaxel versus Fluorouracil or Capecitabine plus Cisplatin and Epirubicin for Locally Advanced, Resectable Gastric or Gastro-Oesophageal Junction Adenocarcinoma (FLOT4): A Randomised, Phase 2/3 Trial. Lancet Lond. Engl. 2019, 393, 1948–1957. [Google Scholar] [CrossRef]
- Becker, K.; Mueller, J.D.; Schulmacher, C.; Ott, K.; Fink, U.; Busch, R.; Böttcher, K.; Siewert, J.R.; Höfler, H. Histomorphology and Grading of Regression in Gastric Carcinoma Treated with Neoadjuvant Chemotherapy. Cancer 2003, 98, 1521–1530. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Jing, S.-W.; Qin, J.-J.; Liu, Q.; Zhai, C.; Wu, Y.-J.; Cheng, Y.-J.; Czito, B.G.; Wang, J. Comparison of Neoadjuvant Chemoradiotherapy and Neoadjuvant Chemotherapy for Esophageal Cancer: A Meta-Analysis. Future Oncol. Lond. Engl. 2019, 15, 2413–2422. [Google Scholar] [CrossRef]
- Dolan, J.P.; Kaur, T.; Diggs, B.S.; Luna, R.A.; Sheppard, B.C.; Schipper, P.H.; Tieu, B.H.; Bakis, G.; Vaccaro, G.M.; Holland, J.M.; et al. Significant Understaging Is Seen in Clinically Staged T2N0 Esophageal Cancer Patients Undergoing Esophagectomy. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2016, 29, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Kidane, B.; Korst, R.J.; Weksler, B.; Farrell, A.; Darling, G.E.; Martin, L.W.; Reddy, R.; Sarkaria, I.S. Neoadjuvant Therapy Vs Upfront Surgery for Clinical T2N0 Esophageal Cancer: A Systematic Review. Ann. Thorac. Surg. 2019, 108, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Mota, F.C.; Cecconello, I.; Takeda, F.R.; Tustumi, F.; Sallum, R.A.A.; Bernardo, W.M. Neoadjuvant Therapy or Upfront Surgery? A Systematic Review and Meta-Analysis of T2N0 Esophageal Cancer Treatment Options. Int. J. Surg. Lond. Engl. 2018, 54, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Hölscher, A.H.; Bollschweiler, E.; Bogoevski, D.; Schmidt, H.; Semrau, R.; Izbicki, J.R. Prognostic Impact of Neoadjuvant Chemoradiation in CT3 Oesophageal Cancer—A Propensity Score Matched Analysis. Eur. J. Cancer Oxf. Engl. 2014, 50, 2950–2957. [Google Scholar] [CrossRef] [PubMed]
- Schneider, P.M.; Baldus, S.E.; Metzger, R.; Kocher, M.; Bongartz, R.; Bollschweiler, E.; Schaefer, H.; Thiele, J.; Dienes, H.P.; Mueller, R.P.; et al. Histomorphologic Tumor Regression and Lymph Node Metastases Determine Prognosis Following Neoadjuvant Radiochemotherapy for Esophageal Cancer: Implications for Response Classification. Ann. Surg. 2005, 242, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Yibulayin, W.; Abulizi, S.; Lv, H.; Sun, W. Minimally Invasive Oesophagectomy versus Open Esophagectomy for Resectable Esophageal Cancer: A Meta-Analysis. World J. Surg. Oncol. 2016, 14, 304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagens, E.R.C.; Reijntjes, M.A.; Anderegg, M.C.J.; Eshuis, W.J.; van Berge Henegouwen, M.I.; Gisbertz, S.S. Risk Factors and Consequences of Anastomotic Leakage After Esophagectomy for Cancer. Ann. Thorac. Surg. 2021, 112, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Cho, B.C.; Takahashi, M.; Okada, M.; Lin, C.-Y.; Chin, K.; Kadowaki, S.; Ahn, M.-J.; Hamamoto, Y.; Doki, Y.; et al. Nivolumab versus Chemotherapy in Patients with Advanced Oesophageal Squamous Cell Carcinoma Refractory or Intolerant to Previous Chemotherapy (ATTRACTION-3): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Kojima, T.; Shah, M.A.; Muro, K.; Francois, E.; Adenis, A.; Hsu, C.-H.; Doi, T.; Moriwaki, T.; Kim, S.-B.; Lee, S.-H.; et al. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables. | All | Surgery Only | Perioperative CTx | p Value * | Perioperative CTx: Good Response | p Value * | Perioperative CTx: Minimal/No Response | p Value * |
|---|---|---|---|---|---|---|---|---|
| Patients | 124 (100%) | 53 (42.7%) | 71 (57.3%) | 19 (26.8%) | 52 (73.2%) | |||
| Age (years) | ||||||||
| ≤60 | 42 (33.9%) | 13 (24.5%) | 29 (40.8%) | 0.058 | 7 (36.8%) | 0.304 | 22 (42.3%) | 0.053 |
| >60 | 82 (66.1%) | 40 (75.5%) | 42 (59.2%) | 12 (63.2%) | 30 (57.7%) | |||
| Sex | ||||||||
| Male | 102 (82.3%) | 44 (83.0%) | 58 (81.7%) | 0.848 | 16 (84.2%) | 0.905 | 42 (80.8%) | 0.765 |
| Female | 22 (17.7%) | 9 (17.0%) | 13 (18.3%) | 3 (15.8%) | 10 (19.2%) | |||
| T category | ||||||||
| ypT0 | 5 (4.0%) | 0 (0.0%) | 5 (7.0%) | 0.020 | 5 (26.3%) | <0.0001 | 0 (0.0%) | 0.136 |
| yp/pT1 | 8 (6.5%) | 0 (0.0%) | 8 (11.3%) | 4 (21.1%) | 4 (7.7%) | |||
| yp/pT2 | 21 (16.9%) | 9 (17.0%) | 12 (16.9%) | 6 (31.6%) | 6 (11.5%) | |||
| yp/pT3 | 75 (60.5%) | 38 (71.7%) | 37 (52.1%) | 4 (21.1%) | 33 (63.5%) | |||
| yp/pT4 | 15 (12.1%) | 6 (11.3%) | 9 (12.7%) | 0 (0.0%) | 9 (17.3%) | |||
| N category | ||||||||
| yp/pN0 | 29 (23.4%) | 5 (9.4%) | 24 (33.8%) | 0.002 | 12 (63.2%) | <0.0001 | 12 (23.1%) | 0.011 |
| yp/pN1 | 37 (29.8%) | 22 (41.5%) | 15 (21.1%) | 6 (31.6%) | 9 (17.3%) | |||
| yp/pN2 | 27 (21.8%) | 9 (17.0%) | 18 (25.4%) | 1 (5.3%) | 17 (32.7%) | |||
| yp/pN3 | 31 (25.0%) | 17 (32.1%) | 14 (19.7%) | 0 (0.0%) | 14 (26.9%) | |||
| R category | ||||||||
| 0 | 109 (87.9%) | 46 (86.8%) | 63 (88.7%) | 0.743 | 19 (100.0%) | 0.095 | 44 (84.6%) | 0.750 |
| 1 | 15 (12.1%) | 7 (13.2%) | 8 (11.3%) | 0 (0.0%) | 8 (15.4%) | |||
| AEG | ||||||||
| I | 47 (37.9%) | 23 (43.4%) | 24 (33.8%) | 0.285 | 7 (36.8%) | 0.689 | 17 (32.7%) | 0.252 |
| II | 71 (57.3%) | 29 (54.7%) | 42 (59.2%) | 11 (57.9%) | 31 (59.6%) | |||
| III | 6 (4.8%) | 1 (1.9%) | 5 (7.0%) | 1 (5.3%) | 4 (7.7%) | |||
| ASA | ||||||||
| 1 | 1 (0.8%) | 1 (1.9%) | 0 (0.0%) | 0.081 | 0 (0.0%) | 0.315 | 0 (0.0%) | 0.201 |
| 2 | 26 (21.0%) | 11 (20.8%) | 15 (21.1%) | 4 (21.1%) | 11 (21.2%) | |||
| 3 | 79 (63.7%) | 29 (54.7%) | 50 (70.4%) | 14 (73.7%) | 36 (69.2%) | |||
| 4 | 18 (14.5%) | 12 (22.6%) | 6 (8.5%) | 1 (5.3%) | 5 (9.6%) | |||
| Clavien–Dindo | ||||||||
| 0 | 25 (20.2%) | 2 (3.8%) | 23 (32.4%) | <0.0001 | 7 (36.8%) | 0.009 | 16 (30.8%) | <0.0001 |
| 1 | 5 (4.0%) | 1 (1.9%) | 4 (5.6%) | 0 (0.0%) | 4 (7.7%) | |||
| 2 | 32 (25.8%) | 10 (18.9%) | 22 (31.0%) | 4 (21.1%) | 18 (34.6%) | |||
| 3 | 24 (19.4%) | 16 (30.2%) | 8 (11.3%) | 3 (15.8%) | 5 (9.6%) | |||
| 4 | 36 (29.0%) | 22 (41.5%) | 14 (19.7%) | 5 (13.9%) | 9 (17.3%) | |||
| 5 | 2 (1.6%) | 2 (3.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Type of surgery | ||||||||
| Open | 82 (66.1%) | 39 (73.6%) | 43 (60.6%) | 0.100 | 8 (42.1%) | 0.010 | 35 (67.3%) | 0.408 |
| Laparoscopic | 33 (26.6%) | 9 (17.0%) | 24 (33.8%) | 10 (52.6%) | 14 (26.9%) | |||
| Hybrid | 9 (7.3%) | 5 (9.4%) | 4 (5.6%) | 1 (5.3%) | 3 (5.8%) | |||
| Anastomotic leak | ||||||||
| No | 98 (79.0%) | 42 (79.2%) | 56 (78.9%) | 0.960 | 13 (68.4%) | 0.341 | 43 (82.7%) | 0.653 |
| Yes | 26 (21.0%) | 11 (20.8%) | 15 (21.1%) | 6 (31.6%) | 9 (17.3%) |
| Type of Complication | Complications during CTx * | Cause for Discontinuitation of CTx * |
|---|---|---|
| n = 20 of 71 (28.2%) | n = 14 of 71 (19.7%) | |
| Weight loss | 2 (7.7%) | 0 (0.0%) |
| Nausea and vomiting | 4 (15.4%) | 2 (12.5%) |
| Polyneuropathy | 4 (15.4%) | 2 (12.5%) |
| Pneumonitis | 3 (11.5%) | 3 (18.8%) |
| Fatigue | 4 (15.4%) | 3 (18.8%) |
| Diarrhea | 3 (11.5%) | 2 (12.5%) |
| Edema of lips and neck | 1 (3.8%) | 1 (6.3%) |
| Hand foot syndrome | 1 (3.8%) | 1 (6.3%) |
| Loss of hair | 2 (7.7%) | 0 (0.0%) |
| Cardiac symptoms | 2 (7.7%) | 2 (12.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stüben, B.-O.; Stuhlfelder, J.; Kemper, M.; Tachezy, M.; Ghadban, T.; Izbicki, J.R.; Bokemeyer, C.; Sinn, M.; Karstens, K.-F.; Reeh, M. Completion of FLOT Therapy, Regardless of Tumor Regression, Significantly Improves Overall Survival in Patients with Esophageal Adenocarcinoma. Cancers 2022, 14, 1084. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041084
Stüben B-O, Stuhlfelder J, Kemper M, Tachezy M, Ghadban T, Izbicki JR, Bokemeyer C, Sinn M, Karstens K-F, Reeh M. Completion of FLOT Therapy, Regardless of Tumor Regression, Significantly Improves Overall Survival in Patients with Esophageal Adenocarcinoma. Cancers. 2022; 14(4):1084. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041084
Chicago/Turabian StyleStüben, Björn-Ole, Jakob Stuhlfelder, Marius Kemper, Michael Tachezy, Tarik Ghadban, Jakob Robert Izbicki, Carsten Bokemeyer, Marianne Sinn, Karl-Frederick Karstens, and Matthias Reeh. 2022. "Completion of FLOT Therapy, Regardless of Tumor Regression, Significantly Improves Overall Survival in Patients with Esophageal Adenocarcinoma" Cancers 14, no. 4: 1084. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041084