
Preoperative Magnetic Resonance Image and Computerized Tomography Findings Predictive of Facial Nerve Invasion in Patients with Parotid Cancer without Preoperative Facial Weakness—A Retrospective Observational Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
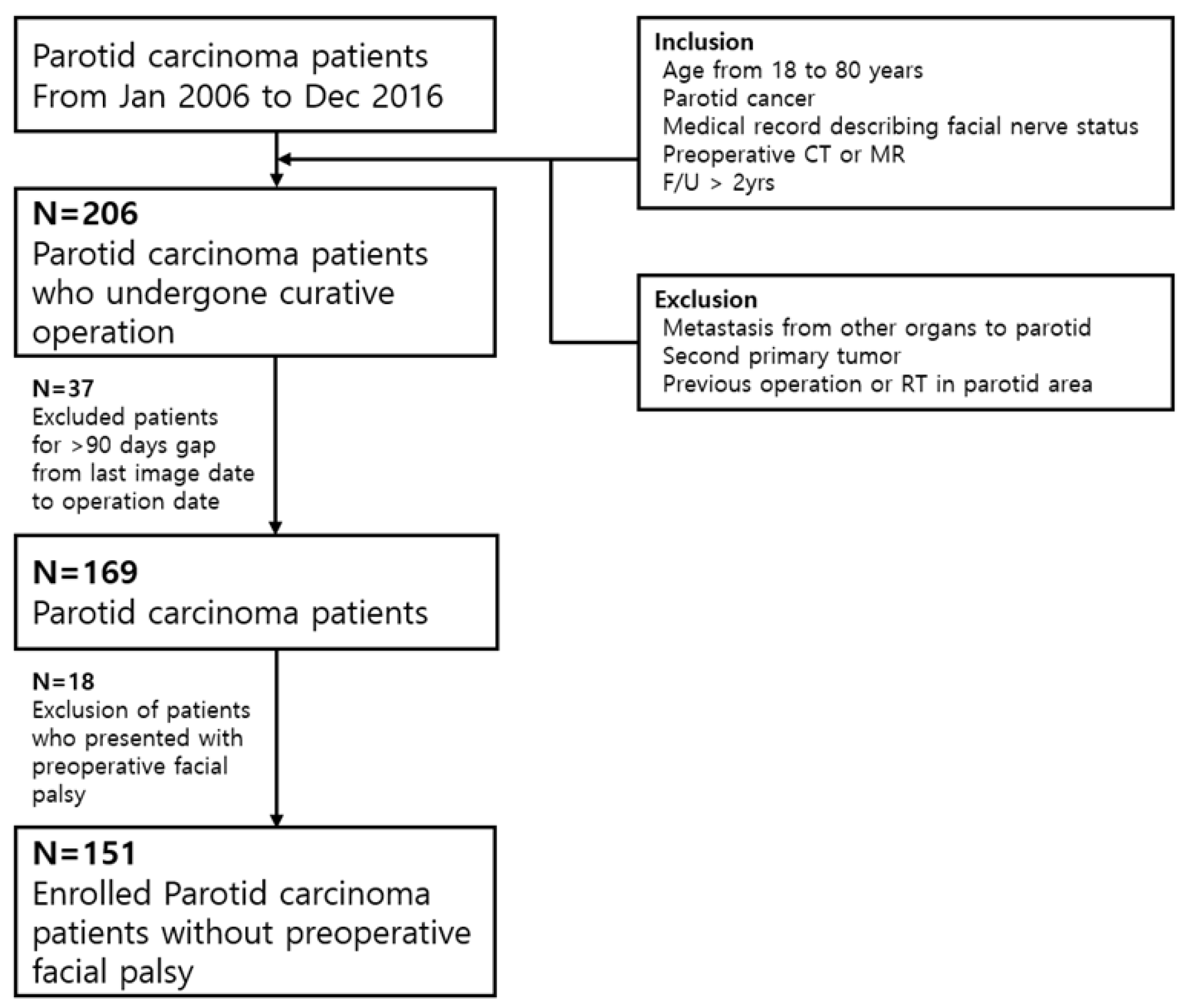
2.1. Study Patients
2.2. Variables
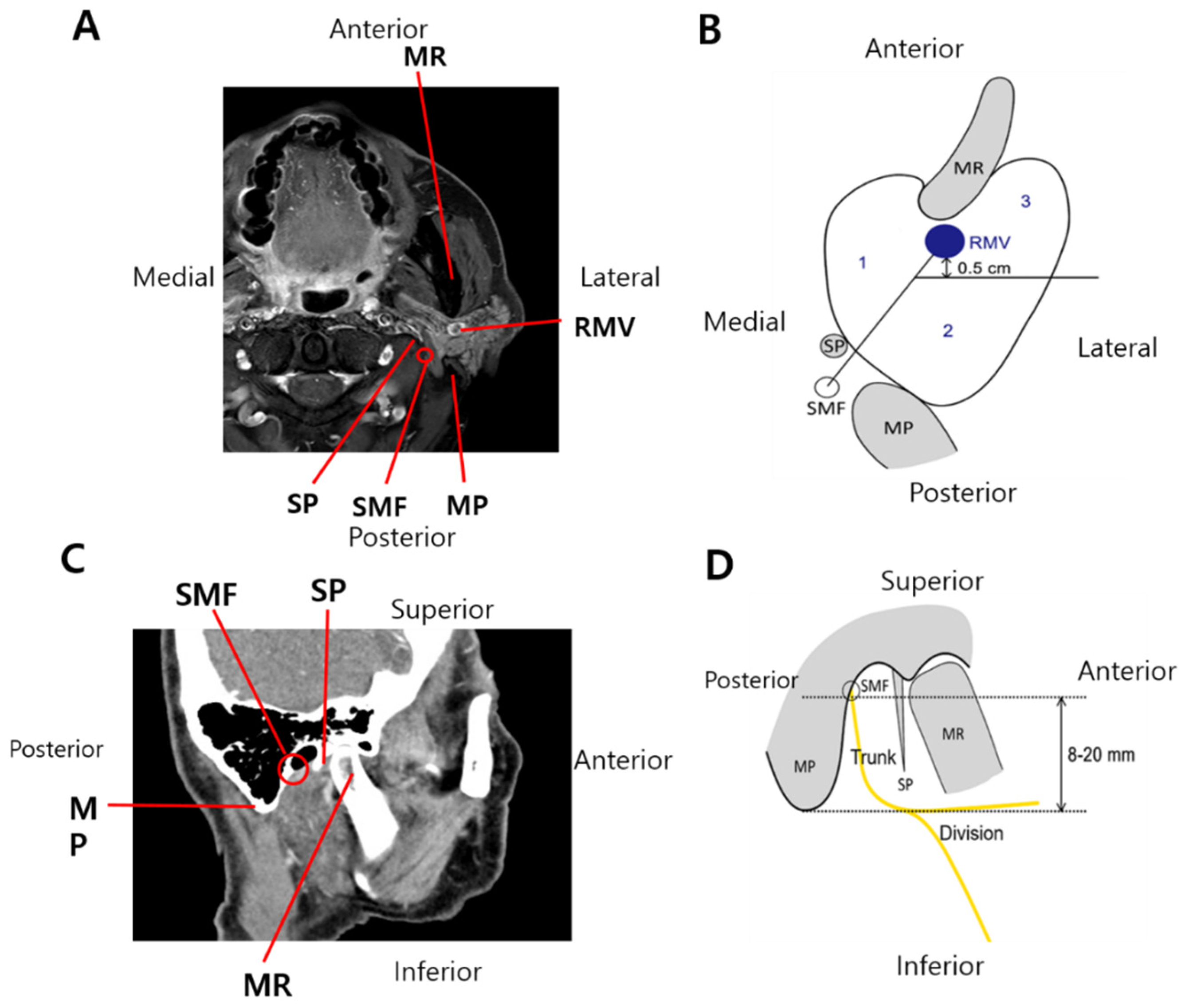
2.2.1. Radiological Variables
2.2.2. Clinical and Pathological Variables
2.3. Magnetic Resonance Imaging
2.4. Computerized Tomography
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Patients with or without FNI
3.2. Clinicopathological and Radiological Factors Predicting FNI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carvalho, A.L.; Nishimoto, I.N.; Califano, J.A.; Kowalski, L.P. Trends in incidence and prognosis for head and neck cancer in the United States: A site-specific analysis of the SEER database. Int. J. Cancer 2005, 114, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.R.; Katabi, N.; Zhung, J.; Wolden, S.L.; Zelefsky, M.J.; Kraus, D.H.; Shah, J.P.; Wong, R.J.; Ghossein, R.A.; Lee, N.Y. Clinical and pathologic prognostic features in acinic cell carcinoma of the parotid gland. Cancer 2009, 115, 2128–2137. [Google Scholar] [CrossRef] [PubMed]
- Pohar, S.; Gay, H.; Rosenbaum, P.; Klish, D.; Bogart, J.; Sagerman, R.; Hsu, J.; Kellman, R. Malignant parotid tumors: Presentation, clinical/pathologic prognostic factors, and treatment outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Patel, N.S.; Modest, M.C.; Moore, E.J.; Janus, J.R.; Olsen, K.D. Occult temporal bone facial nerve involvement by parotid malignancies with perineural spread. Otolaryngol.–Head Neck Surg. 2015, 153, 385–391. [Google Scholar] [CrossRef]
- Nellis, J.C.; Ishii, M.; Byrne, P.J.; Boahene, K.D.; Dey, J.K.; Ishii, L.E. Association among facial paralysis, depression, and quality of life in facial plastic surgery patients. JAMA Fac. Plast. Surg. 2017, 19, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Han, S.J.; Park, S.H. Functional Outcomes of Immediate Facial Nerve Repair After Radical Parotidectomy. J. Neurol. Surg. Part B Skull Base 2016, 77, A046. [Google Scholar] [CrossRef]
- Huyett, P.; Duvvuri, U.; Ferris, R.L.; Johnson, J.T.; Schaitkin, B.M.; Kim, S. Perineural Invasion in Parotid Gland Malignancies. Otolaryngol. Head Neck Surg. 2018, 158, 1035–1041. [Google Scholar] [CrossRef]
- Grazioli, L.; Olivetti, L.; Matricardi, L.; Zanetti, U.; Burlini, D.; Negrini, S.; Fugazzola, C.; Chiesa, A. Comparison of ultrasonography, computerized tomography, and magnetic resonance in the study of parotid masses. Radiol. Med. 1993, 86, 268–280. [Google Scholar]
- Imaizumi, A.; Kuribayashi, A.; Okochi, K.; Ishii, J.; Sumi, Y.; Yoshino, N.; Kurabayashi, T. Differentiation between superficial and deep lobe parotid tumors by magnetic resonance imaging: Usefulness of the parotid duct criterion. Acta Radiol. 2009, 50, 806–811. [Google Scholar] [CrossRef]
- Poletti, A.M.; Imparato, S.; Signorelli, G.C.; Cugini, G.; Colombo, G. The multiplanar analysis of the retromandibular vein in surgical planning for parotid gland tumors. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1587–1593. [Google Scholar] [CrossRef]
- Badger, D.; Aygun, N. Imaging of perineural spread in head and neck cancer. Radiol. Clin. 2017, 55, 139–149. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Sootweg, P.J. (Eds.) Tumours of the salivary glands. In World Health Organization Classification of Head and Neck Tumours, 4th ed.; IARC Press: Lyon, France, 2017; Volume 9, pp. 159–202. [Google Scholar]
- Dulguerov, P.; Marchal, F.; Lehmann, W. Postparotidectomy facial nerve paralysis: Possible etiologic factors and results with routine facial nerve monitoring. Laryngoscope 1999, 109, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Preis, M.; Soudry, E.; Bachar, G.; Shufel, H.; Feinmesser, R.; Shpitzer, T. Predicting facial nerve invasion by parotid gland carcinoma and outcome of facial reanimation. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 107. [Google Scholar] [CrossRef] [PubMed]
- Bendet, E.; Talmi, Y.P.; Kronenberg, J. Preoperative electroneurography (ENoG) in parotid surgery: Assessment of facial nerve outcome and involvement by tumor—a preliminary study. Head Neck J. Sci. Spec. Head Neck 1998, 20, 124–131. [Google Scholar] [CrossRef]
- Rouchy, R.C.; Attye, A.; Medici, M.; Renard, F.; Kastler, A.; Grand, S.; Tropres, I.; Righini, C.A.; Krainik, A. Facial nerve tractography: A new tool for the detection of perineural spread in parotid cancers. Eur. Radiol. 2018, 28, 3861–3871. [Google Scholar] [CrossRef]
- Divi, V.; Fatt, M.A.; Mukherji, S.K.; Bradford, C.R.; Chepeha, D.B.; Wolf, G.T.; Teknos, T.N. Use of cross-sectional imaging in predicting facial nerve sacrifice during surgery for parotid neoplasms. ORL 2004, 66, 262–266. [Google Scholar] [CrossRef]
- Fujii, H.; Fujita, A.; Kanazawa, H.; Sung, E.; Sakai, O.; Sugimoto, H. Localization of parotid gland tumors in relation to the intraparotid facial nerve on 3D double-echo steady-state with water excitation sequence. Am. J. Neuroradiol. 2019, 40, 1037–1042. [Google Scholar] [CrossRef]
- de Ru, J.A.; van Benthem, P.P.G.; Hordijk, G.-J. The location of parotid gland tumors in relation to the facial nerve on magnetic resonance images and computed tomography scans. J. Oral Maxillofac. Surg. 2002, 60, 992–994. [Google Scholar] [CrossRef]
- Kurabayashi, T.; Ida, M.; Ohbayashi, N.; Ishii, J.; Sasaki, T. Criteria for differentiating superficial from deep lobe tumours of the parotid gland by computed tomography. Dentomaxillofac. Radiol. 1993, 22, 81–85. [Google Scholar] [CrossRef]
- Kim, J.; Yang, H.; Lee, S.; Kim, H.; Shin, D.; Cho, Y.; Cho, H.H. Effectiveness of anatomic criteria for predicting parotid tumour location. Clin. Otolaryngol. 2016, 41, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Domenick, N.A.; Johnson, J.T. Parotid tumor size predicts proximity to the facial nerve. Laryngoscope 2011, 121, 2366–2370. [Google Scholar] [CrossRef]
- Zbären, P.; Triantafyllou, A.; Devaney, K.O.; Vander Poorten, V.; Hellquist, H.; Rinaldo, A.; Ferlito, A. Preoperative diagnostic of parotid gland neoplasms: Fine-needle aspiration cytology or core needle biopsy? Eur. Arch. Otorhinolaryngol. 2018, 275, 2609–2613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaillard, C.; Perie, S.; Susini, B.; St Guily, J.L. Facial nerve dysfunction after parotidectomy: The role of local factors. Laryngoscope 2005, 115, 287–291. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 151) | FNI (+) (n = 30) | FNI (−) (n = 121) | p-Value |
|---|---|---|---|---|
| Clinical factors | ||||
| Age (years), median (range) | 55 (19–80) | 56 (19–80) | 55 (19–78) | 0.630 |
| Gender, male/female | 73/78 (48.3/51.7) | 21/9 (70.0/30.0) | 52/69 (43.0/57.0) | 0.008 |
| Smoking history > 10 pack-years | 32 (21.2) | 6 (20.0) | 26 (21.5) | 0.858 |
| Alcohol intake ≥ 1 drink/day | 60 (39.7) | 9 (30.0) | 51 (42.1) | 0.224 |
| Charlson’s comorbidity index score ≥ 1 | 25 (16.6) | 5 (16.7) | 20 (16.5) | 0.986 |
| Histologic grade, low/intermediate/high | 81/30/36 (53.6/19.9/23.8) | 10/6/13 (33.3/20.0/43.3) | 71/24/23 (58.7/19.8/19.0) | 0.012 |
| Pathological tumor size (mm), mean (SD) | 24.1 (10.3) | 31.2 (9.6) | 22.4 (9.8) | 0.000 |
| cT category, T3–4 | 15 (10.0) | 8 (26.7) | 7 (5.8) | 0.001 |
| cN category, N1–3 | 24 (15.9) | 10 (33.3) | 14 (11.6) | 0.004 |
| Lymphovascular invasion | 21 (13.9) | 7 (23.0) | 14 (11.6) | 0.096 |
| ECS (+) | 56 (37.1) | 18 (60.0) | 38 (31.4) | 0.004 |
| Resection margin involvement | 26 (17.2) | 11 (36.7) | 15 (12.4) | 0.002 |
| Follow-up duration, median (range) | 62 (24–120) | 62 (24–118) | 61 (24–120) | 0.767 |
| Treatment | ||||
| Surgery alone | 71 (47.0) | 3 (10.0) | 68 (56.2) | 0.000 |
| Surgery plus RT | 72 (47.7) | 26 (86.7) | 46 (38.0) | |
| Surgery plus CCRT | 8 (5.3) | 1 (3.3) | 7 (5.8) | |
| Last status | ||||
| NED | 126 (83.4) | 18 (60.0) | 108 (89.3) | 0.003 |
| DOD/DOC | 14/6 (9.3/4.0) | 7/3 (23.3/10.0) | 7/3 (5.8/2.5) | |
| AD | 4 (2.6) | 2 (6.7) | 2 (1.7) | |
| Recurrence, any site | 27 (17.9) | 9 (30.0) | 18 (14.9) | 0.053 |
| Variable | Total (n = 151) | FNI (+) (n = 30) | FNI (−) (n = 121) | p-Value |
|---|---|---|---|---|
| Level (location) of invasion division/trunk/both | 24/4/2 (80.0/13.3/6.7) | |||
| Margin, well-defined/spiculated/ill-defined | 59/80/12 (39.1/53.0/7.9) | 4/24/2 (13.3/80.0/6.7) | 55/56/10 (45.4/46.2/8.3) | 0.003 |
| Tumor size (mm), mean (SD) | 25.0 (9.5) | 30.6 (7.5) | 24.1 (9.5) | 0.001 |
| Presence in area 3 | 122 (80.8) | 29 (96.7) | 93 (76.9) | 0.014 |
| Tumor present at the main trunk course | 34 (22.5) | 10 (33.3) | 24 (19.8) | 0.113 |
| RMV involvement, none/obliteration/displacement | 114/27/9 (75.5/17.9/6.0) | 18/9/2 (60.0/30.0/6.7) | 96/18/7 (79.3/14.9/5.8) | 0.023 |
| SMF involvement (yes vs. no) | 11 (7.3) | 3 (10.0) | 8 (6.6) | 0.523 |
| Distance from the SMF to the upper tumor margin (mm), mean (SD) | 13.7 (11.4) | 10.2 (9.5) | 14.5 (11.7) | 0.060 |
| Positive impression of FNI by radiologists | 59 (39.1) | 21 (70.0) | 38 (31.4) | 0.000 |
| Variable | FNI | |
|---|---|---|
| OR (95% CI) | p-Value a | |
| Margin, spiculated vs. ill–defined | 4.35 (1.31–14.41) | 0.016 |
| Tumor size, 2.2 cm | 6.02 (1.63–22.24) | 0.007 |
| Presence in area 3 | 8.98 (1.08–74.87) | 0.042 |
| High histological grade | 3.65 (1.26–10.61) | 0.017 |
| RMV involvement (obliteration) | ||
| RMV obliteration | 1.54 (0.53–4.48) | 0.426 |
| RMV displacement | 0.84 (0.13–5.41) | 0.851 |
| Positive impression of FNI by radiologists | 3.55 (1.35–12.7) | 0.012 |
| Variable | AUC | SE | 95% CI | p-Value |
|---|---|---|---|---|
| Impression by radiologists | 0.693 | 0.058 | 0.613–0.765 | <0.001 |
| Predictive variables | ||||
| Tumor size, margin, and presence in area 3 | 0.787 | 0.052 | 0.713–0.849 | <0.001 |
| Three factors + histological grade | 0.839 | 0.047 | 0.770–0.893 | <0.001 |
| Difference between areas | ||||
| Three factors vs. radiologist | 0.094 | 0.062 | −0.028–0.216 | 0.129 |
| Four factors vs. radiologist | 0.146 | 0.061 | 0.027–0.265 | 0.017 |
| Variable | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|---|---|---|---|---|
| Impression by radiologists | 70.00 | 68.60 | 35.59 | 90.22 | 68.87 |
| Predictive variables | |||||
| Size, margin, and presence in area 3 | 76.67 | 72.73 | 41.07 | 92.63 | 73.51 |
| Three factors + histological grade | 83.33 | 69.42 | 40.32 | 94.38 | 72.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, W.K.; Lee, M.K.; Choi, Y.J.; Lee, Y.S.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Preoperative Magnetic Resonance Image and Computerized Tomography Findings Predictive of Facial Nerve Invasion in Patients with Parotid Cancer without Preoperative Facial Weakness—A Retrospective Observational Study. Cancers 2022, 14, 1086. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041086
Cho WK, Lee MK, Choi YJ, Lee YS, Choi S-H, Nam SY, Kim SY. Preoperative Magnetic Resonance Image and Computerized Tomography Findings Predictive of Facial Nerve Invasion in Patients with Parotid Cancer without Preoperative Facial Weakness—A Retrospective Observational Study. Cancers. 2022; 14(4):1086. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041086
Chicago/Turabian StyleCho, Won Ki, Min Kyoung Lee, Young Jun Choi, Yoon Se Lee, Seung-Ho Choi, Soon Yuhl Nam, and Sang Yoon Kim. 2022. "Preoperative Magnetic Resonance Image and Computerized Tomography Findings Predictive of Facial Nerve Invasion in Patients with Parotid Cancer without Preoperative Facial Weakness—A Retrospective Observational Study" Cancers 14, no. 4: 1086. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041086