State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part II: Synthetic Polymers-Based Biomaterials

 , and
, and
Abstract
:1. Natural versus Synthetic Polymers
2. Manufacturing Processes of Synthetic Matrices for Oral Soft Tissue Augmentation
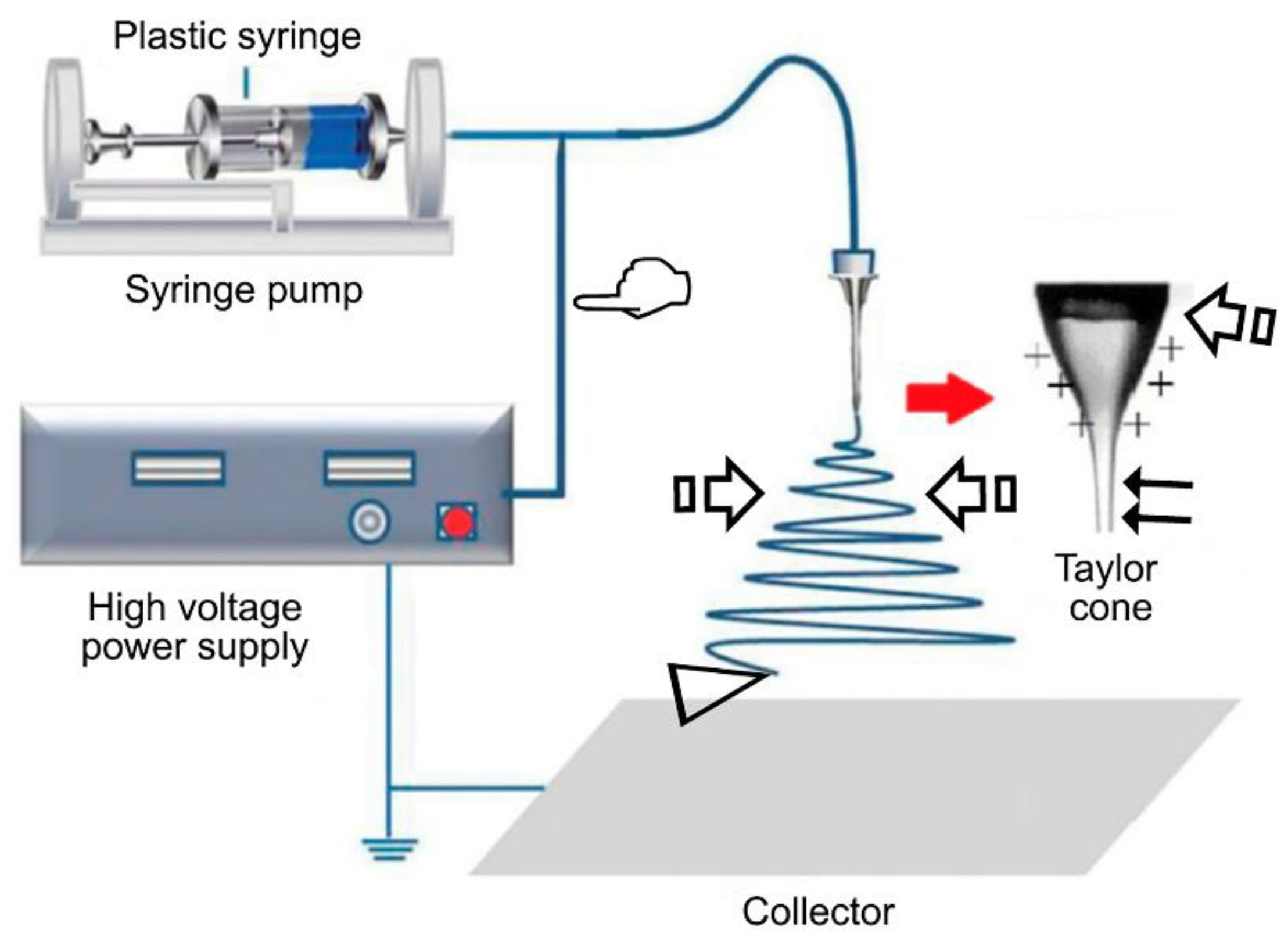
2.1. Electrospinning
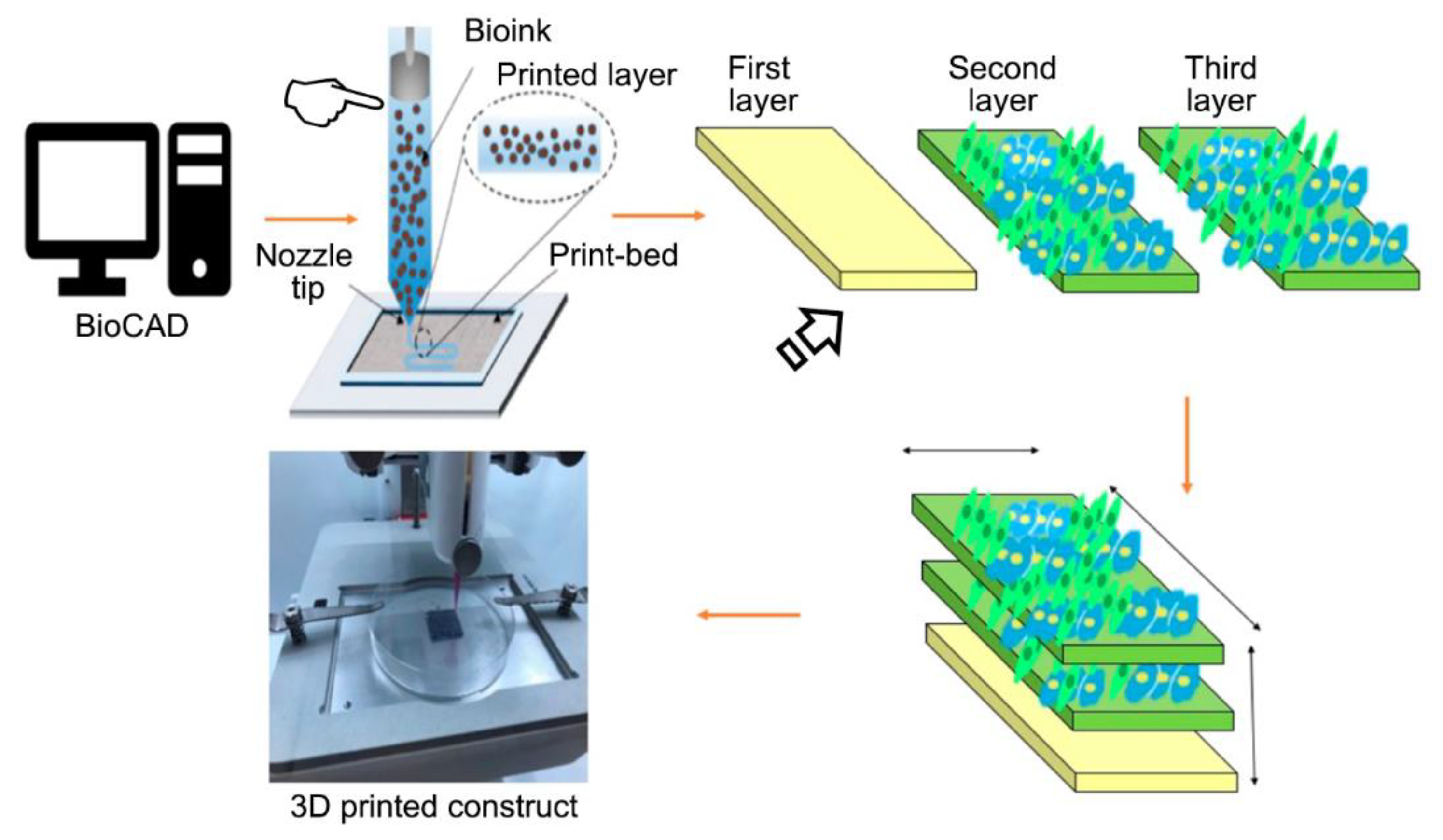
2.2. 3D Printing
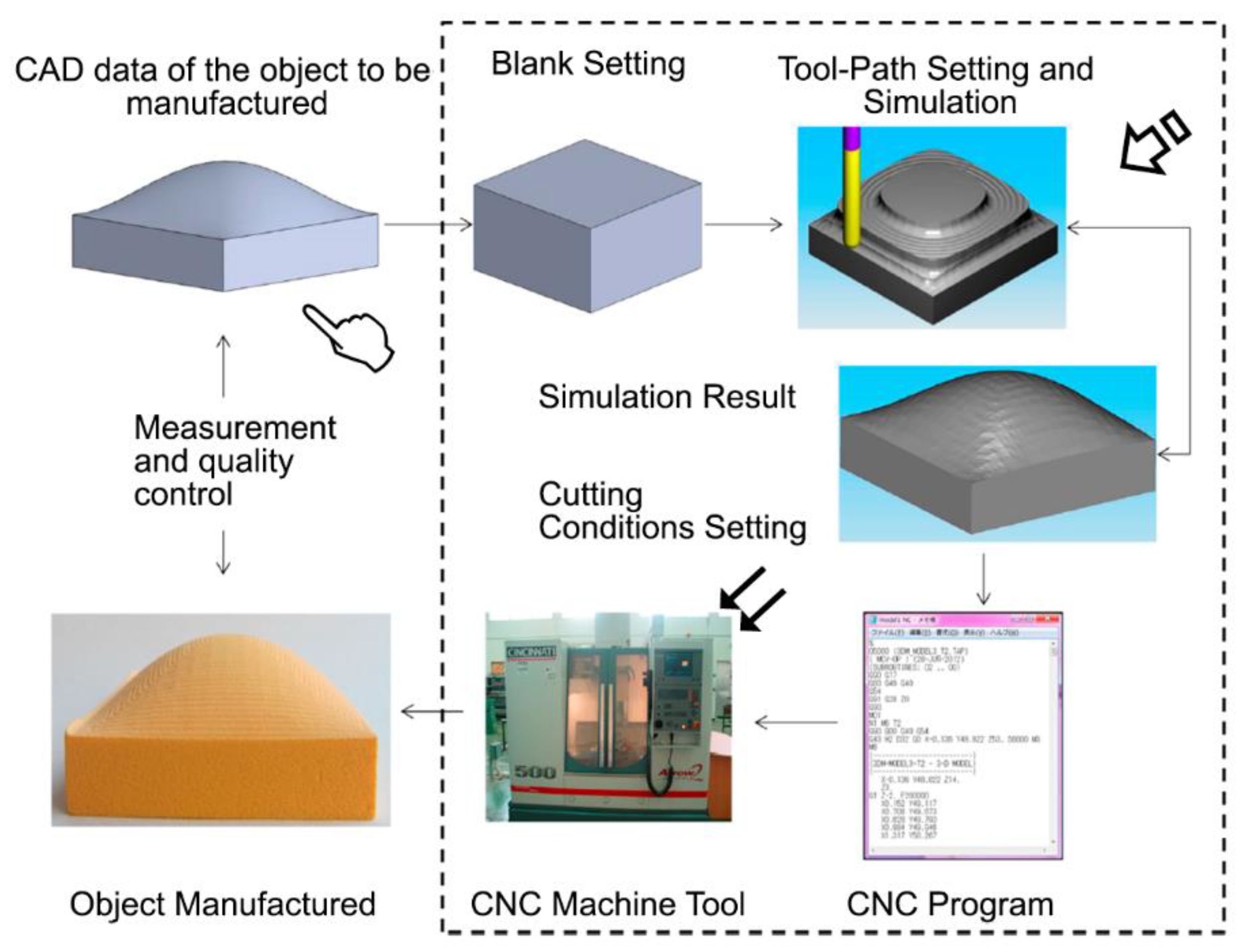
2.3. CAD/CAM
3. New Trends in Synthetic Polymeric Blends for Oral Tissue Engineering
3.1. Resorbable versus Non-Resorbable Matrices
3.2. Loading of Matrix Scaffolds Strategies to Stimulate the Formation of Capillary-Like Networks In Vivo Recruitment of Osteoblasts
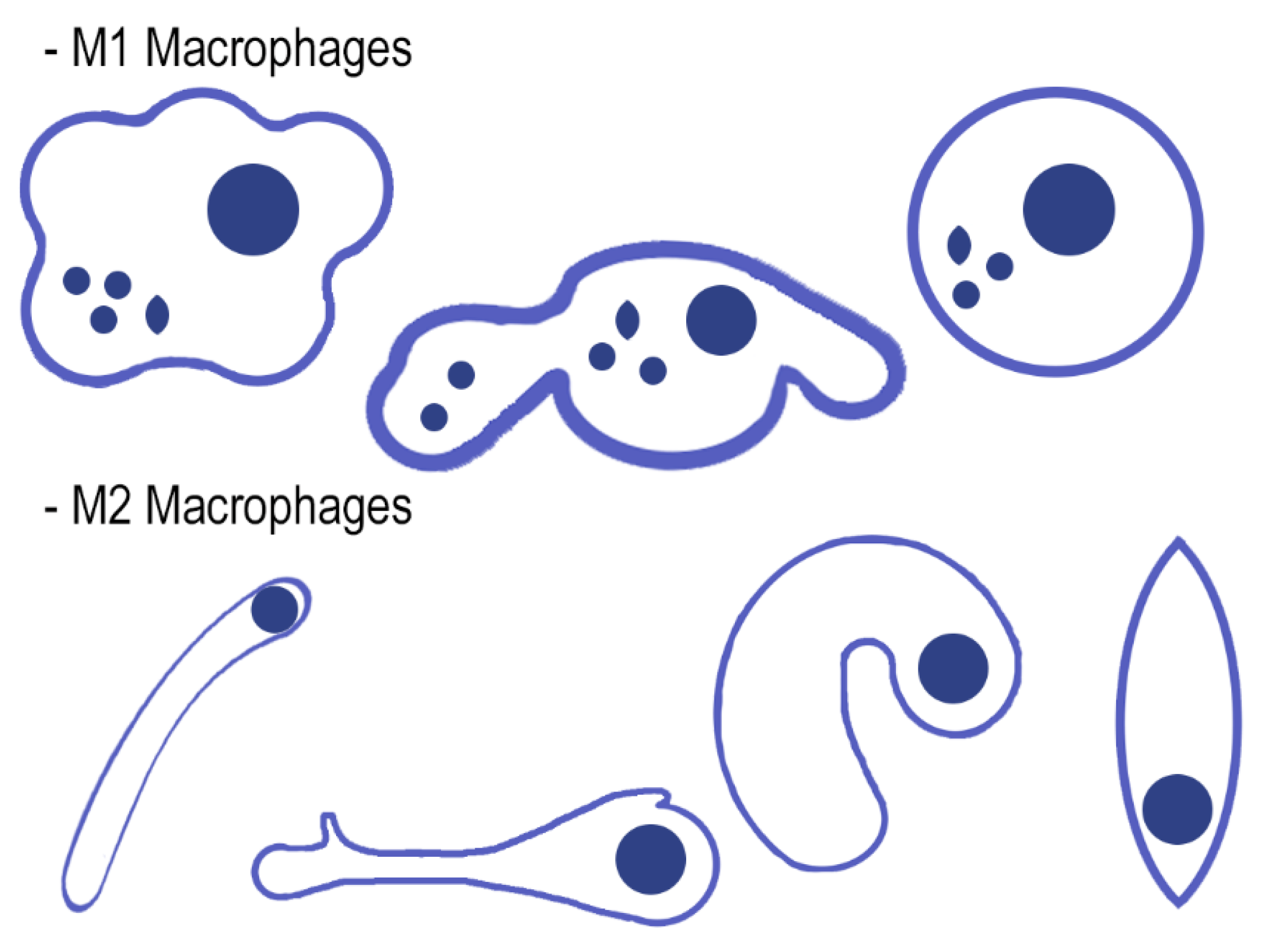
3.3. The Intertwined Concepts of Tissue Engineering and the Innate Immune Response Related with Angiogenesis Macrophages Functional Polarization (M1/M2)
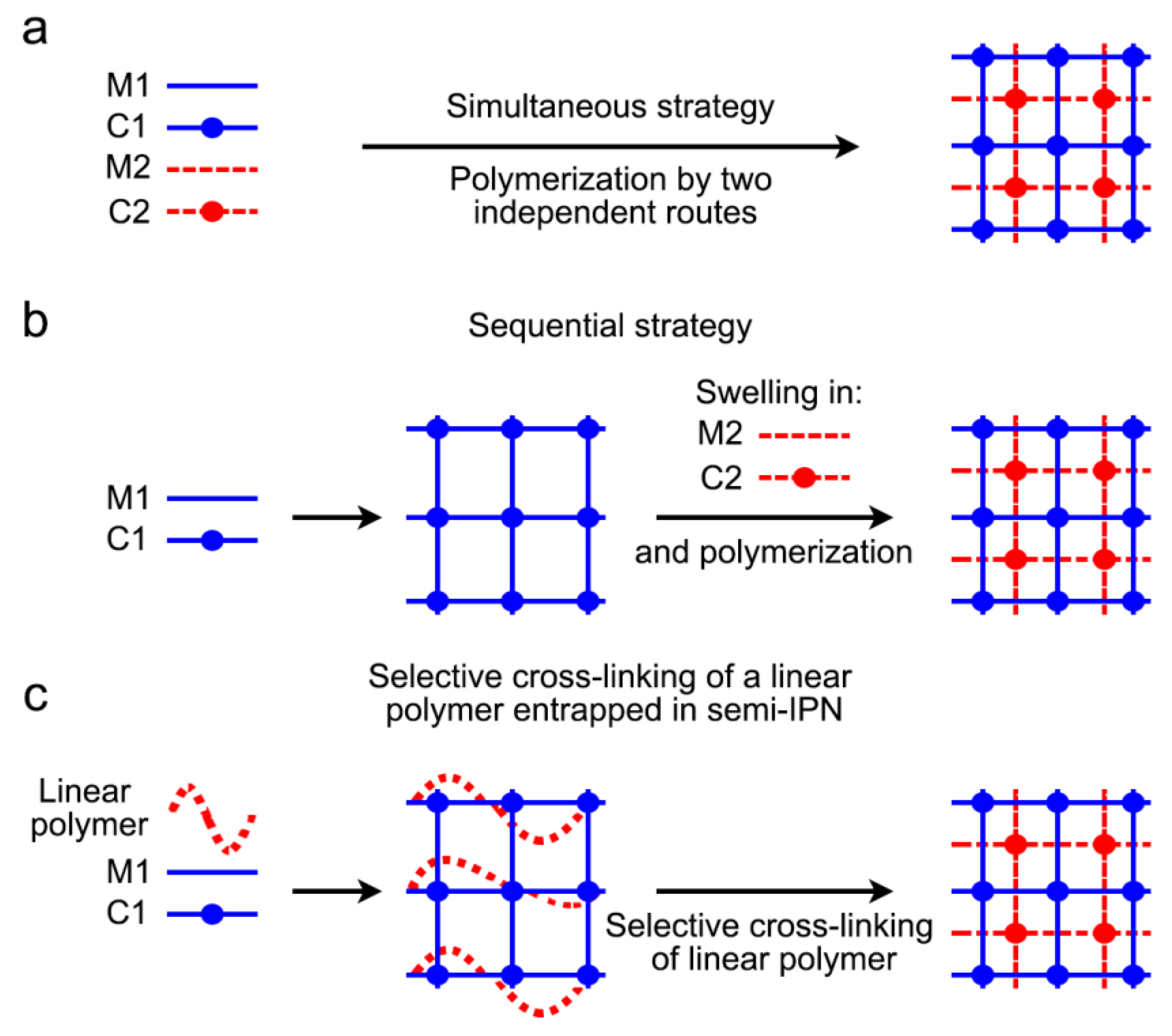
4. Hydrogels, Promising Breakthrough Technology for Soft Tissue Surgery. Mechanically Enhanced Semi-Interpenetrating Polymer Network (IPN) Hydrogel
5. Protocol of Research on Matrices for Soft Tissue Augmentation
5.1. Description of the Matrix and Sample Preparation
5.2. Cell Culture Fibroblasts, Osteoblasts, Endothelial Cells, Keratinocytes, and Cell Morphology
5.3. Cell Viability and Cytotoxicity (LIVE/DEAD® Assay)
5.4. Animal Experimentation
5.4.1. Mouse Experimental Design
5.4.2. Dog Experimental Design
6. Trends for Future
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BMP | Bone morphogenetic protein |
| CAD | Computer-aided design |
| CAM | Computer-aided manufacturing |
| DMEM | Dulbecco’s modified Eagle’s medium |
| DNA | Deoxyribonucleic acid |
| DSC | Differential calorimetry |
| ECM | Extracellular matrix |
| FCS | Fetal calf serum |
| FTIR | Fourier transform infrared |
| H&E | Hematoxylin and eosin |
| HGF | Human gingival fibroblasts |
| HOB | Human osteoblast-like |
| HOK | Human oral keratinocytes |
| HUVEC | Human umbilical vein endothelial cells |
| IFN-γ | Interferon gamma |
| IL | Interleukin |
| IPN | Interpenetrating polymer network |
| LDH | Lactate dehydrogenase |
| MMP | Metalloproteinase |
| MNGC | Multinucleated giant cell |
| Nm | Nanostructured membranes silica loaded |
| (Zn-Nm) | Nanostructured membranes silica loaded doped with Zinc |
| (Dox-Nm) | Nanostructured membranes silica loaded doped with Doxycycline |
| NPs | Nanoparticles |
| PCL | Polycaprolactone or poly(ε-caprolactone) |
| PGA | Poly(glycolic acid) |
| pHEMA-co-MAA | 2-hydroxyethyl methacrylate-co-methacrylic acid |
| PLA | Poly(lactic acid), polylactic acid or polylactide |
| PLGA | Poly(lactic-co-glycolic) acid |
| ROI | Region of interest |
| SEM | Scanning electron microscopy |
| TB | Toluidine blue |
| TGF-β | Transforming growth factor beta |
| TNF-α | Tumoral necrosis factor alpha |
| VEGF | Vascular endothelial growth factor |
References
- Zafar, M.S.; Khurshid, Z.; Almas, K. Oral tissue engineering progress and challenges. Tissue Eng. Regen. Med. 2015, 12, 387–397. [Google Scholar] [CrossRef]
- Dhandayuthapani, B.; Yoshida, Y.; Maekawa, T.; Kumar, D.S. Polymeric Scaffolds in Tissue Engineering Application: A Review. Int. J. Polym. Sci. 2011, 2011, e290602. [Google Scholar] [CrossRef]
- Sheikh, Z.; Najeeb, S.; Khurshid, Z.; Verma, V.; Rashid, H.; Glogauer, M. Biodegradable Materials for Bone Repair and Tissue Engineering Applications. Materials 2015, 8, 5744–5794. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.; Farre Guasch, E.; Sándor, G.; Gibbs, S.; Jager, D.; Forouzanfar, T. Soft Tissue Augmentation Techniques and Materials Used in the Oral Cavity. Implant. Dent. 2016, 25, 1. [Google Scholar] [CrossRef]
- Bhardwaj, N.; Chouhan, D.; Mandal, B.B. Tissue Engineered Skin and Wound Healing: Current Strategies and Future Directions. Curr. Pharm. Des. 2017, 23, 3455–3482. [Google Scholar] [CrossRef]
- Tavelli, L.; McGuire, M.K.; Zucchelli, G.; Rasperini, G.; Feinberg, S.E.; Wang, H.-L.; Giannobile, W.V. Extracellular matrix-based scaffolding technologies for periodontal and peri-implant soft tissue regeneration. J. Periodontol. 2020, 91, 17–25. [Google Scholar] [CrossRef]
- Siddique, N.; Raza, H.; Ahmed, S.; Khurshid, Z.; Zafar, M.S. Gene Therapy: A Paradigm Shift in Dentistry. Genes 2016, 7, 98. [Google Scholar] [CrossRef]
- Carter, S.-S.D.; Costa, P.F.; Vaquette, C.; Ivanovski, S.; Hutmacher, D.W.; Malda, J. Additive Biomanufacturing: An Advanced Approach for Periodontal Tissue Regeneration. Ann. Biomed. Eng. 2017, 45, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Osorio, R.; Cabello, I.; Medina-Castillo, A.L.; Osorio, E.; Toledano, M. Zinc-modified nanopolymers improve the quality of resin-dentin bonded interfaces. Clin. Oral Investig. 2016, 20, 2411–2420. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.; Toledano-Osorio, M.; Osorio, R.; Carrasco-Carmona, Á.; Gutiérrez-Pérez, J.-L.; Gutiérrez-Corrales, A.; Serrera-Figallo, M.-A.; Lynch, C.D.; Torres-Lagares, D. Doxycycline and Zinc Loaded Silica-Nanofibrous Polymers as Biomaterials for Bone Regeneration. Polymers 2020, 12, 1201. [Google Scholar] [CrossRef]
- Toledano, M.; Gutierrez-Pérez, J.L.; Gutierrez-Corrales, A.; Serrera-Figallo, M.A.; Toledano-Osorio, M.; Rosales-Leal, J.I.; Aguilar, M.; Osorio, R.; Torres-Lagares, D. Novel non-resorbable polymeric-nanostructured scaffolds for guided bone regeneration. Clin. Oral Investig. 2019, 24, 2037–2049. [Google Scholar] [CrossRef]
- Bottino, M.C.; Thomas, V.; Schmidt, G.; Vohra, Y.K.; Chu, T.-M.G.; Kowolik, M.J.; Janowski, G.M. Recent advances in the development of GTR/GBR membranes for periodontal regeneration—A materials perspective. Dent. Mater. 2012, 28, 703–721. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.S.; Chen, S.-S.; Li, C.-W.; Nguyen, N.C.; Nguyen, H.T. A comprehensive review: Electrospinning technique for fabrication and surface modification of membranes for water treatment application. RSC Adv. 2016, 6, 85495–85514. [Google Scholar] [CrossRef]
- Jun, I.; Han, H.-S.; Edwards, J.R.; Jeon, H. Electrospun Fibrous Scaffolds for Tissue Engineering: Viewpoints on Architecture and Fabrication. Int. J. Mol. Sci. 2018, 19, 745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asmatulu, R.; Khan, W.S. Chapter 2—Historical background of the electrospinning process. In Synthesis and Applications of Electrospun Nanofibers; Micro and Nano Technologies; Asmatulu, R., Khan, W.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 17–39. ISBN 978-0-12-813914-1. [Google Scholar]
- Reneker, D.H.; Chun, I. Nanometre diameter fibres of polymer, produced by electrospinning. Nanotechnology 1996, 7, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Anu Bhushani, J.; Anandharamakrishnan, C. Electrospinning and electrospraying techniques: Potential food based applications. Trends Food Sci. Tech. 2014, 38, 21–33. [Google Scholar] [CrossRef]
- Wang, J.; Windbergs, M. Functional electrospun fibers for the treatment of human skin wounds. Eur. J. Pharm. Biopharm. 2017, 119, 283–299. [Google Scholar] [CrossRef]
- Zong, H.; Xia, X.; Liang, Y.; Dai, S.; Alsaedi, A.; Hayat, T.; Kong, F.; Pan, J.H. Designing function-oriented artificial nanomaterials and membranes via electrospinning and electrospraying techniques. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 92, 1075–1091. [Google Scholar] [CrossRef]
- Chen, K.; Chou, W.; Liu, L.; Cui, Y.; Xue, P.; Jia, M. Electrochemical Sensors Fabricated by Electrospinning Technology: An Overview. Sensors 2019, 19, 3676. [Google Scholar] [CrossRef]
- Haider, A.; Haider, S.; Kang, I.-K. A comprehensive review summarizing the effect of electrospinning parameters and potential applications of nanofibers in biomedical and biotechnology. Arab. J. Chem. 2015, 11, 1165–1188. [Google Scholar] [CrossRef]
- Sun, B.; Long, Y.Z.; Zhang, H.D.; Li, M.M.; Duvail, J.L.; Jiang, X.Y.; Yin, H.L. Advances in three-dimensional nanofibrous macrostructures via electrospinning. Prog. Polym. Sci. 2014, 39, 862–890. [Google Scholar] [CrossRef]
- Berton, F.; Porrelli, D.; Di Lenarda, R.; Turco, G. A Critical Review on the Production of Electrospun Nanofibres for Guided Bone Regeneration in Oral Surgery. Nanomaterials 2019, 10, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurmann, N.; Sperling, L.-E.; Pranke, P. Electrospun and Electrosprayed Scaffolds for Tissue Engineering. Adv. Exp. Med. Biol. 2018, 1078, 79–100. [Google Scholar] [PubMed]
- Chen, D.W.-C.; Liu, S.-J. Electrospun Nanofibrous Scaffolds for Soft Tissue Regeneration. In Biomaterials for Implants and Scaffolds; Springer Series in Biomaterials Science and Engineering; Li, Q., Mai, Y.-W., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 271–301. ISBN 978-3-662-53574-5. [Google Scholar]
- Manoukian, O.S.; Matta, R.; Letendre, J.; Collins, P.; Mazzocca, A.D.; Kumbar, S.G. Electrospun Nanofiber Scaffolds and Their Hydrogel Composites for the Engineering and Regeneration of Soft Tissues. Methods Mol. Biol. 2017, 1570, 261–278. [Google Scholar]
- Mohammadzadehmoghadam, S.; Dong, Y.; Barbhuiya, S.; Guo, L.; Liu, D.; Umer, R.; Qi, X.; Tang, Y. Electrospinning: Current Status and Future Trends. In Nano-Size Polymers: Preparation, Properties, Applications; Fakirov, S., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 89–154. ISBN 978-3-319-39715-3. [Google Scholar]
- Chandra, P.K.; Soker, S.; Atala, A. Chapter 1—Tissue engineering: Current status and future perspectives. In Principles of Tissue Engineering, 5th ed.; Lanza, R., Langer, R., Vacanti, J.P., Atala, A., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 1–35. ISBN 978-0-12-818422-6. [Google Scholar]
- Tebyetekerwa, M.; Ramakrishna, S. What Is Next for Electrospinning? Matter 2020, 2, 279–283. [Google Scholar] [CrossRef] [Green Version]
- Raveendran, N.; Meinert, C.; Ipe, D.; Ivanovski, S. Optimization of 3D bioprinting of periodontal ligament cells. Dent. Mater. 2019, 35, 1683–1694. [Google Scholar] [CrossRef]
- Derby, B. Printing and Prototyping of Tissues and Scaffolds. Science 2012, 338, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Okabe, K.; Yamada, Y.; Ito, K.; Kohgo, T.; Yoshimi, R.; Ueda, M. Injectable soft-tissue augmentation by tissue engineering and regenerative medicine with human mesenchymal stromal cells, platelet-rich plasma and hyaluronic acid scaffolds. Cytotherapy 2009, 11, 307–316. [Google Scholar] [CrossRef]
- Janmohammadi, M.; Nourbakhsh, M.S. Recent advances on 3D printing in hard and soft tissue engineering. Int. J. Polym. Mater. Pol. Biomater. 2020, 69, 449–466. [Google Scholar] [CrossRef]
- Rimann, M.; Bono, E.; Annaheim, H.; Bleisch, M.; Graf-Hausner, U. Standardized 3D Bioprinting of Soft Tissue Models with Human Primary Cells. J. Lab. Autom. 2016, 21, 496–509. [Google Scholar] [CrossRef] [Green Version]
- Pati, F.; Ha, D.-H.; Jang, J.; Han, H.H.; Rhie, J.-W.; Cho, D.-W. Biomimetic 3D tissue printing for soft tissue regeneration. Biomaterials 2015, 62, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Hafezi, F.; Shorter, S.; Tabriz, A.G.; Hurt, A.; Elmes, V.; Boateng, J.; Douroumis, D. Bioprinting and Preliminary Testing of Highly Reproducible Novel Bioink for Potential Skin Regeneration. Pharmaceutics 2020, 12, 550. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.; Blokzijl, M.M.; Levato, R.; Visser, C.W.; Castilho, M.; Hennink, W.E.; Vermonden, T.; Malda, J. Assessing bioink shape fidelity to aid material development in 3D bioprinting. Biofabrication 2017, 10, 014102. [Google Scholar] [CrossRef] [PubMed]
- Loai, S.; Kingston, B.R.; Wang, Z.; Philpott, D.N.; Tao, M.; Cheng, H.-L.M. Clinical Perspectives on 3D Bioprinting Paradigms for Regenerative Medicine. Regen. Med. Front. 2019, 1, e190004. [Google Scholar]
- Leigh, S.J.; Bradley, R.J.; Purssell, C.P.; Billson, D.R.; Hutchins, D.A. A Simple, Low-Cost Conductive Composite Material for 3D Printing of Electronic Sensors. PLoS ONE 2012, 7, e49365. [Google Scholar] [CrossRef]
- Stratton, S.; Manoukian, O.S.; Patel, R.; Wentworth, A.; Rudraiah, S.; Kumbar, S.G. Polymeric 3D printed structures for soft-tissue engineering. J. Appl. Polym. Sci. 2018, 135, 45569. [Google Scholar] [CrossRef] [Green Version]
- Nikolova, M.P.; Chavali, M.S. Recent advances in biomaterials for 3D scaffolds: A review. Bioact. Mater. 2019, 4, 271–292. [Google Scholar] [CrossRef]
- Fischer, B.; Schulz, A.; Gepp, M.; Neubauer, J.; Gentile, L.; Zimmermann, H. 3D printing of hydrogels in a temperature controlled environment with high spatial resolution. Curr. Dir. Biomed. Eng. 2016, 2. [Google Scholar] [CrossRef]
- Li, J.; Wu, C.; Chu, P.K.; Gelinsky, M. 3D printing of hydrogels: Rational design strategies and emerging biomedical applications. Mater. Sci. Eng. R Rep. 2020, 140, 100543. [Google Scholar] [CrossRef]
- Abboud, M.; Orentlicher, G. Computer-Aided Manufacturing in Medicine. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2012, 20, 19–36. [Google Scholar] [CrossRef]
- Alghazzawi, T.F. Advancements in CAD/CAM technology: Options for practical implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Galhano, G.Á.P.; Pellizzer, E.P.; Mazaro, J.V.Q. Optical Impression Systems for CAD-CAM Restorations. J. Craniofac. Surg. 2012, 23, e575. [Google Scholar] [CrossRef]
- Ullah, A.S.; Harib, K.H. Tutorials for Integrating CAD/CAM in Engineering Curricula. Educ. Sci. 2018, 8, 151. [Google Scholar] [CrossRef] [Green Version]
- Davidowitz, G.; Kotick, P.G. The Use of CAD/CAM in Dentistry. Dent. Clin. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Tayebi, L. Applications of Biomedical Engineering in Dentistry; Springer: Cham, Switzerland, 2019; ISBN 978-3-030-21583-5. [Google Scholar]
- Mortadi, N.; Eggbeer, D.; Lewis, J.; Williams, R. CAD/CAM/AM applications in the manufacture of dental appliances. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 727–733. [Google Scholar] [CrossRef]
- Susic, I.; Travar, M.; Susic, M. The application of CAD / CAM technology in Dentistry. IOP Conf. Ser. Mater. Sci. Eng. 2017, 200, 012020. [Google Scholar] [CrossRef] [Green Version]
- Boitelle, P.; Mawussi, B.; Tapie, L.; Fromentin, O. A systematic review of CAD/CAM fit restoration evaluations. J. Oral Rehabil. 2014, 41, 853–874. [Google Scholar] [CrossRef]
- Barenghi, L.; Barenghi, A.; Cadeo, C.; Di Blasio, A. Innovation by Computer-Aided Design/Computer-Aided Manufacturing Technology: A Look at Infection Prevention in Dental Settings. Biomed. Res. Int. 2019, 2019, 6092018. [Google Scholar] [CrossRef]
- Yen, H.H.; Stathopoulou, P.G. CAD/CAM and 3D-Printing Applications for Alveolar Ridge Augmentation. Curr. Oral Health Rep. 2018, 5, 127–132. [Google Scholar] [CrossRef]
- Pietruski, J.K.; Skurska, A.; Bernaczyk, A.; Milewski, R.; Pietruska, M.J.; Gehrke, P.; Pietruska, M.D. Evaluation of concordance between CAD/CAM and clinical positions of abutment shoulder against mucosal margin: An observational study. BMC Oral Health 2018, 18, 73. [Google Scholar] [CrossRef] [Green Version]
- Lops, D.; Bressan, E.; Parpaiola, A.; Sbricoli, L.; Cecchinato, D.; Romeo, E. Soft tissues stability of cad-cam and stock abutments in anterior regions: 2-year prospective multicentric cohort study. Clin. Oral Implant. Res. 2015, 26, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Naveau, A.; Rignon-Bret, C.; Wulfman, C. Zirconia abutments in the anterior region: A systematic review of mechanical and esthetic outcomes. J. Prosthet. Dent. 2019, 121, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P. Use of CAD/CAM Healing Abutment Immediately After Dental Implant Placement for the Non-Esthetic Zone: A Guided Soft Tissue Healing Technique. J. Oral Implantol. 2016, 42, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Zopf, D.A.; Mitsak, A.G.; Flanagan, C.L.; Wheeler, M.; Green, G.E.; Hollister, S.J. Computer Aided–Designed, 3-Dimensionally Printed Porous Tissue Bioscaffolds for Craniofacial Soft Tissue Reconstruction. Otolaryngol. Head Neck Surg. 2014, 152, 57–62. [Google Scholar] [CrossRef]
- Wang, J.; Wang, L.; Zhou, Z.; Lai, H.; Xu, P.; Liao, L.; Wei, J. Biodegradable Polymer Membranes Applied in Guided Bone/Tissue Regeneration: A Review. Polymers 2016, 8, 115. [Google Scholar] [CrossRef]
- Toledano, M.; Toledano-Osorio, M.; Carrasco-Carmona, Á.; Vallecillo, C.; Lynch, C.D.; Osorio, M.T.; Osorio, R. State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part I: Natural Polymers-based Biomaterials. Polymers 2020, in press. [Google Scholar]
- Pabst, A.M.; Happe, A.; Callaway, A.; Ziebart, T.; Stratul, S.I.; Ackermann, M.; Konerding, M.A.; Willershausen, B.; Kasaj, A. In vitro and in vivo characterization of porcine acellular dermal matrix for gingival augmentation procedures. J. Periodont. Res. 2014, 49, 371–381. [Google Scholar] [CrossRef]
- Osorio, R.; Carrasco-Carmona, Á.; Toledano, M.; Osorio, E.; Medina-Castillo, A.L.; Iskandar, L.; Marques, A.; Deb, S.; Toledano-Osorio, M. Ex vivo investigations on bioinspired electrospun membranes as potential biomaterials for bone regeneration. J. Dent. 2020, 98. [Google Scholar] [CrossRef]
- Shahabipour, F.; Ashammakhi, N.; Oskuee, R.K.; Bonakdar, S.; Hoffman, T.; Shokrgozar, M.A.; Khademhosseini, A. Key components of engineering vascularized 3-dimensional bioprinted bone constructs. Transl. Res. 2019, 216, 57–76. [Google Scholar] [CrossRef]
- Li, H.; Chang, J. Bioactive silicate materials stimulate angiogenesis in fibroblast and endothelial cell co-culture system through paracrine effect. Acta Biomater. 2013, 9, 6981–6991. [Google Scholar] [CrossRef]
- Rather, H.A.; Jhala, D.; Vasita, R. Dual functional approaches for osteogenesis coupled angiogenesis in bone tissue engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 103, 109761. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Zhou, Y.; Shao, J.; Chen, Z.; Song, B.; Chang, J.; Wu, C.; Xiao, Y. Stimulation of osteogenesis and angiogenesis of hBMSCs by delivering Si ions and functional drug from mesoporous silica nanospheres. Acta Biomater. 2015, 21, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Zahm, A.M.; Bucaro, M.A.; Srinivas, V.; Shapiro, I.M.; Adams, C.S. Oxygen tension regulates preosteocyte maturation and mineralization. Bone 2008, 43, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, C.M.; Schlegel, K.A.; Gammel, L.; Moest, T. Gingiva thickening with a porcine collagen matrix in a preclinical dog model: Histological outcomes. J. Clin. Periodontol. 2019, 46, 1273–1281. [Google Scholar] [CrossRef]
- Maggiano, I.S.; Maggiano, C.M.; Clement, J.G.; Thomas, C.D.L.; Carter, Y.; Cooper, D.M.L. Three-dimensional reconstruction of Haversian systems in human cortical bone using synchrotron radiation-based micro-CT: Morphology and quantification of branching and transverse connections across age. J. Anat. 2016, 228, 719–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Li, J.; Cheng, M.; Wang, Q.; Yeung, K.W.K.; Chu, P.K.; Zhang, X. Zinc-Modified Sulfonated Polyetheretherketone Surface with Immunomodulatory Function for Guiding Cell Fate and Bone Regeneration. Adv. Sci. 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Osorio, R.; Yamauti, M.; Osorio, E.; Ruiz-Requena, M.E.; Pashley, D.H.; Tay, F.R.; Toledano, M. Zinc reduces collagen degradation in demineralized human dentin explants. J. Dent. 2011, 39, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Muthukuru, M.; Sun, J. Doxycycline Counteracts Bone Morphogenic Protein 2–Induced Osteogenic Mediators. J. Periodontol. 2013, 84, 656–665. [Google Scholar] [CrossRef]
- Almazin, S.M.; Dziak, R.; Andreana, S.; Ciancio, S.G. The Effect of Doxycycline Hyclate, Chlorhexidine Gluconate, and Minocycline Hydrochloride on Osteoblastic Proliferation and Differentiation In Vitro. J. Periodontol. 2009, 80, 999–1005. [Google Scholar] [CrossRef]
- Park, J.-B. Effects of Doxycycline, Minocycline, and Tetracycline on Cell Proliferation, Differentiation, and Protein Expression in Osteoprecursor Cells. J. Craniofac. Surg. 2011, 22, 1839–1842. [Google Scholar] [CrossRef]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface characteristics of dental implants: A review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Bosshardt, D.D. OsteoMacs: Key players around bone biomaterials. Biomaterials 2016, 82, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, M.; Pettersson, J.; Johansson, A.; Thorén, M.M. Titanium release in peri-implantitis. J. Oral Rehabil. 2019, 46, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.-H.; Rastogi, R.; Shelke, J.; Amiji, M.M. Modulation of Macrophage Functional Polarity towards Anti-Inflammatory Phenotype with Plasmid DNA Delivery in CD44 Targeting Hyaluronic Acid Nanoparticles. Sci. Rep. 2015, 5, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Wuescher, L.M.; Worth, R.; Yildirim-Ayan, E. Mechano-Immunomodulation: Mechanoresponsive Changes in Macrophage Activity and Polarization. Ann. Biomed. Eng. 2019, 47, 2213–2231. [Google Scholar] [CrossRef] [PubMed]
- Buchacher, T.; Ohradanova-Repic, A.; Stockinger, H.; Fischer, M.B.; Weber, V. M2 Polarization of Human Macrophages Favors Survival of the Intracellular Pathogen Chlamydia pneumoniae. PLoS ONE 2015, 10, e0143593. [Google Scholar] [CrossRef] [Green Version]
- Garg, K.; Pullen, N.A.; Oskeritzian, C.A.; Ryan, J.J.; Bowlin, G.L. Macrophage functional polarization (M1/M2) in response to varying fiber and pore dimensions of electrospun scaffolds. Biomaterials 2013, 34, 4439–4451. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.; Toledano-Osorio, M.; Navarro-Hortal, M.D.; Varela-López, A.; Osorio, R.; Quiles, J.L. Novel Polymeric Nanocarriers Reduced Zinc and Doxycycline Toxicity in the Nematode Caenorhabditis elegans. Antioxidants 2019, 8, 550. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.-F.; Chen, Y.-J.; Zhang, J.-X.; Shen, L.; Wang, R.; Zhou, J.-S.; Hu, J.-G.; Lü, H.-Z. Adoptive transfer of M2 macrophages promotes locomotor recovery in adult rats after spinal cord injury. Brain Behav. Immun. 2015, 45, 157–170. [Google Scholar] [CrossRef]
- Mariani, E.; Lisignoli, G.; Borzì, R.M.; Pulsatelli, L. Biomaterials: Foreign Bodies or Tuners for the Immune Response? Int. J. Mol. Sci. 2019, 20, 636. [Google Scholar] [CrossRef] [Green Version]
- Madden, L.R.; Mortisen, D.J.; Sussman, E.M.; Dupras, S.K.; Fugate, J.A.; Cuy, J.L.; Hauch, K.D.; Laflamme, M.A.; Murry, C.E.; Ratner, B.D. Proangiogenic scaffolds as functional templates for cardiac tissue engineering. Proc. Natl. Acad. Sci. USA 2010, 107, 15211–15216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morón-Calvente, V.; Romero-Pinedo, S.; Toribio-Castelló, S.; Plaza-Díaz, J.; Abadía-Molina, A.C.; Rojas-Barros, D.I.; Beug, S.T.; LaCasse, E.C.; MacKenzie, A.; Korneluk, R.; et al. Inhibitor of apoptosis proteins, NAIP, cIAP1 and cIAP2 expression during macrophage differentiation and M1/M2 polarization. PLoS ONE 2018, 13, e0193643. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Luo, J.; Zhang, Y.; Li, Z.; Chen, F.; Song, W.; Zhang, Y. The unique regulation of implant surface nanostructure on macrophages M1 polarization. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 106, 110221. [Google Scholar] [CrossRef] [PubMed]
- McWhorter, F.Y.; Wang, T.; Nguyen, P.; Chung, T.; Liu, W.F. Modulation of macrophage phenotype by cell shape. Proc. Natl. Acad. Sci. USA 2013, 110, 17253–17258. [Google Scholar] [CrossRef] [Green Version]
- Korzinskas, T.; Jung, O.; Smeets, R.; Stojanovic, S.; Najman, S.; Glenske, K.; Hahn, M.; Wenisch, S.; Schnettler, R.; Barbeck, M. In Vivo Analysis of the Biocompatibility and Macrophage Response of a Non-Resorbable PTFE Membrane for Guided Bone Regeneration. Int. J. Mol. Sci. 2018, 19, 2952. [Google Scholar] [CrossRef] [Green Version]
- Dragan, E.S. Design and applications of interpenetrating polymer network hydrogels. A review. Chem. Eng. J. 2014, 243, 572–590. [Google Scholar] [CrossRef]
- Tamay, D.G.; Dursun Usal, T.; Alagoz, A.S.; Yucel, D.; Hasirci, N.; Hasirci, V. 3D and 4D Printing of Polymers for Tissue Engineering Applications. Front. Bioeng. Biotechnol. 2019, 7. [Google Scholar] [CrossRef]
- Gong, J.P.; Katsuyama, Y.; Kurokawa, T.; Osada, Y. Double-Network Hydrogels with Extremely High Mechanical Strength. Adv. Mater. 2003, 15, 1155–1158. [Google Scholar] [CrossRef]
- Haque, M.A.; Kurokawa, T.; Gong, J.P. Super tough double network hydrogels and their application as biomaterials. Polymer 2012, 53, 1805–1822. [Google Scholar] [CrossRef]
- Li, Z.; Shen, J.; Ma, H.; Lu, X.; Shi, M.; Li, N.; Ye, M. Preparation and characterization of pH- and temperature-responsive nanocomposite double network hydrogels. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 1951–1957. [Google Scholar] [CrossRef]
- Ning, C.Q.; Mehta, J.; El-Ghannam, A. Effects of silica on the bioactivity of calcium phosphate composites in vitro. J. Mater. Sci. Mater. Med. 2005, 16, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Hämmerle, C.H.F.; Cochran, D.L.; Jones, A.A.; Görlach, C.; Uebersax, L.; Mathes, S.; Graf-Hausner, U.; Jung, R.E. Soft tissue volume augmentation by the use of collagen-based matrices in the dog mandible—A histological analysis. J. Clin. Periodontol. 2011, 38, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Benner, M.; Fienitz, T.; Happe, A.; Kreppel, M.; Nickenig, H.-J.; Zöller, J.E. Biodegradation pattern and tissue integration of native and cross-linked porcine collagen soft tissue augmentation matrices—An experimental study in the rat. Head Face Med. 2014, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrantino, L.; Bosshardt, D.; Nevins, M.; Santoro, G.; Simion, M.; Kim, D. Tissue Integration of a Volume-Stable Collagen Matrix in an Experimental Soft Tissue Augmentation Model. Int. J. Periodontics Restor. Dent. 2016, 36, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.; Nguyen, K.; Miller, M.; Tandon, R.; Signorino, F. Evaluation of the Safety and Efficacy of Soft Tissue Augmentation with a Compressive-Resistant Collagen Matrix in a Non-Human Primate Model. J. Oral Maxillofac. Surg. 2018, 77. [Google Scholar] [CrossRef]
- Seo, G.-Y.; Thoma, D.S.; Jung, U.-W.; Lee, J.-S. Increasing the tissue thickness at implant sites using guided bone regeneration and an additional collagen matrix: Histologic observations in beagle dogs. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.W.; Kim, S.; Waller, T.; Cha, J.-K.; Cho, S.-W.; Jung, U.-W.; Thoma, D.S. Soft tissue substitutes to increase gingival thickness: Histologic and volumetric analyses in dogs. J. Clin. Periodontol. 2019, 46, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Caballé-Serrano, J.; Zhang, S.; Ferrantino, L.; Simion, M.; Chappuis, V.; Bosshardt, D.D. Tissue Response to a Porous Collagen Matrix Used for Soft Tissue Augmentation. Materials 2019, 12, 3721. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, C.M.; Matta, R.E.; Moest, T.; Humann, J.; Gammel, L.; Neukam, F.W.; Schlegel, K.A. Soft tissue volume alterations after connective tissue grafting at teeth: The subepithelial autologous connective tissue graft versus a porcine collagen matrix—A pre-clinical volumetric analysis. J. Clin. Periodontol. 2016, 43, 609–617. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ART. | Animals | Sample and Treatment Modalities | Surgeries | Sacrifice | Histological and Histometric Assessment. |
|---|---|---|---|---|---|
| Thoma et al. (2011) [97] | Six male large hound type dogs Age: >2 years Weight: 60–70 kg | 36 samples (six samples per animal; two samples per group)
| All mandibular P2, P4, and the distal roots of M1 were extracted on both sides of the mandible and the buccal plate of the extraction sites was removed. After a healing period of 2 months, full-thickness mucoperiosteal flaps were elevated to receive the treatment. | At 28 days (n = 3) and 84 days (n = 3) following soft tissue augmentation surgery, euthanasia was performed on all animals. | Qualitative analysis with a stereoscope: old bone, newly formed bone, non-mineralized bone, collagen matrix, vascularization of the matrix, tissue integration, and inflammatory reaction. Computer-assisted histomorphometric measurements: augmented ridge width in four different levels 1.5, 3.5, 5.5, and 7.5 mm below the crest, including measurements of native bone, newly formed bone, and non-mineralized tissue. |
| Pabst et al. (2014) [62] | Six female euthymic nude mice Age: 6–8 weeks Weight: 26–28 g | 12 samples (two samples per animal) Treatment: Porcine-derived collagen matrix (Mucoderm, Botiss Dental, Berlin, Germany) | Two matrices were implanted subcutaneously right and left alongside the dorsal midline of each mouse. | After 21 days (n = 6), the mice were sacrificed. | Analysis with a stereoscope: Three microobjects were obtained from each sample for each of the different stains
|
| Rothamel et al. (2014) [98] | Forty albino rats of the Wistar strain Age: 3 +/− 0.5 months Weight: 350 +/− 21 g | 160 samples (four samples per animal: one per group)
| A skin incision was made paramedian along the vertebral column followed by the separation of four unconnected subcutaneous pouches. The membranes were randomly allocated in the resulting 160 pouches. | At 1 (n = 5), 2 (n = 5), 4 (n = 5), 8 (n = 5), and 12 (n = 5) weeks, animals were sacrificed. | Histomorphometricanalysis: For image acquisition, a color CCD camera was mounted on a binocular light microscope. Digital images were evaluated using an imaging program to evaluate:
|
| Ferrantino et al. (2016) [99] | Six mature beagle dogs Weight: 11.6–14.5 kg | Split-mouth study; 12 samples (2 samples per animal; one per group) Test group: VCMX (Fibro-Gide® prototype, Geistlich Pharma AG, Wolhusen, Switzerland) Control group: no treatment | The study was divided into three phases: surgical extraction of six maxillary premolars per animal, surgical matrix placement with full thickness flap and either a VCMX in contact with the bone or the flap repositioned without the use of a biomaterial (sham group), and evaluation prior to sacrifice. | At incremental time points, including day 0 (n = 1) and 4 (n = 1), 7 (n = 1), 15 (n = 1), 30 (n = 1), and 90 (n = 1) days after matrix placement, the canines were sacrificed. | Prior to microscopic examination, the samples were cut into slices and stained with different stains (hematoxylin/eosin, basic fuchsin, and toluidine blue; double stained with toluidine blue and basic fuchsin). Microscopy examination: tissue integration process, cell and blood vessel invasion, and new collagen formation. |
| Herford et al. (2018) [100] | Six skeletally mature male nonhuman primates (Rhesus macaques) | This study also performs a combination part with bone guided regeneration (BGR)
| Surgery 1: Tooth extraction and creation of a bony defect. Surgery 2: Soft tissue augmentation procedures with partial-thickness flaps. Surgery 3: Implant placement. | No sacrifice. One month post-implant placement, the soft tissue surrounding the implant was biopsied. | Soft Tissue Analysis (In Vivo): Periodontal probing, shear modulus elasticity, and volumetric analysis. Soft Tissue Analysis (In Vitro): Qualitative analysis with a stereoscope: Vascularization of the matrix, collagen matrix evaluation, inflammation, and tissue integration. Histomorphometric assessment: Images were captured via digital camera and light microscope; the images were evaluated using analysis software. |
| Seo et al. (2019) [101] | Four male beagle dogs Age: 18–24 months Weight: approx. 15 kg | Split-mouth study; 24 samples (6 samples per animal; 3 sample per side)
| A standardized bony defect was surgically created bilaterally. R.O.G procedures were performed. In the test group, an additional collagen matrix was applied over the collagen membrane; subsequently, a periosteal releasing incision was made to allow advancement of the mucoperiosteal flap. | At 8 weeks of healing, all animals were euthanized. | Microcomputed tomography analysis: The scanned dataset was processed in DICOM format and reconstructed with three-dimensional software in order to measure thickness of the soft-tissue layer. Microscopy examination: Using an image analysis software. Outcomes measured in the region of interest (ROI); thickness of the soft-tissue layer, thicknesses of the membrane complex including the dense connective tissue above the membrane, the membrane, and the dense connective tissue below the membrane, proportions of new bone formation, remaining bone material and connective tissue. |
| Song et al. (2019) [102] | Six beagle dogs Age: 12–15 months Weight: 10–15 kg | Split-mouth study; 12 samples (2 per animal)
| Tunnel technique was made on an attached gingiva underneath the mesiolabial side of the first incisor area to distolabial side of the third incisor area. | At 12 weeks after the operation, the animals were sacrificed. | Microscopy examination: Analyzed with a computer software. Parameters measured: Horizontal thickness (mean thickness of total soft tissue, mean thickness of total connective tissue, and mean thickness of dense connective tissue) and number of rete pegs (rete pegs underneath the keratinized epithelium and rete pegs underneath the sulcular epithelium and junctional epithelium). Volumetric analysis: Dental impressions at all five time points were obtained and digitized using a dental scanner. The resulting STL files were subsequently analyzed using software. |
| Caballé-Serrano et al. (2019) [103] | Six beagle dogs Weight 11.6–14.5 kg | Split-mouth study; 12 samples (2 samples per animal; one per group) Test group: VCMX (Fibro-Gide® prototype, Geistlich Pharma AG, Wolhusen, Switzerland) Control group: No treatment | Six maxillary premolars were atraumatically extracted to create two edentulous spaces in each dog. After 90 days, a full thickness flap was elevated, and either a VCMX in contact with the bone was placed, or the flap was repositioned without the use of a biomaterial (sham group). | At incremental time points, including day 0 (n = 1), 4 (n = 1), 7 (n = 1), 15 (n = 1), 30 (n = 1); and 90 (n = 1) days after matrix placement, the canines were sacrificed. | Scanning Electron Microscopy examination MAC387 Immunohistochemistry: To visualize cells that belong to the inflammatory linage derived from hematopoietic stem cells such as granulocytes, monocytes, and macrophages. PCNA Immunohistochemistry: To visualize cells that were in a proliferative phase. Quantitative Analysis CD86 Immunohistochemistry TGM2 Immunohistochemistry: To stain blood vessels. |
| Schmitt et al. (2019) [69] | Eight healthy female beagle dogs Age: 12–18 months | Randomized split-mouth study: 16 samples (2 samples per animal; one per group) Test group: Natural porcine 3D collagen matrix (CM, mucoderm®, Botiss Biomaterials GmbH) Control group: SCTG (control group) from the palate. | The two treatments (CM and SCTG) were allocated to either the right or left upper canine by simple randomization. The tunnel technique was performed in an extent that the soft tissue graft could be inserted stable without the need of any further fixation. | After 10 months, the animals were sacrificed. | Histomorphometrically measured connective tissue thickness (CTT) in mm. Descriptive histological analyses, Immunohistochemical analyses, and Immunohistological quantification:
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toledano, M.; Toledano-Osorio, M.; Carrasco-Carmona, Á.; Vallecillo, C.; Toledano, R.; Medina-Castillo, A.L.; Osorio, R. State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part II: Synthetic Polymers-Based Biomaterials. Polymers 2020, 12, 1845. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081845
Toledano M, Toledano-Osorio M, Carrasco-Carmona Á, Vallecillo C, Toledano R, Medina-Castillo AL, Osorio R. State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part II: Synthetic Polymers-Based Biomaterials. Polymers. 2020; 12(8):1845. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081845
Chicago/Turabian StyleToledano, Manuel, Manuel Toledano-Osorio, Álvaro Carrasco-Carmona, Cristina Vallecillo, Raquel Toledano, Antonio Luis Medina-Castillo, and Raquel Osorio. 2020. "State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part II: Synthetic Polymers-Based Biomaterials" Polymers 12, no. 8: 1845. https://0-doi-org.brum.beds.ac.uk/10.3390/polym12081845