The Importance of Stromal Endometriosis in Thoracic Endometriosis

 ,
,
Abstract
:1. Endometriosis
2. Thoracic Endometriosis Syndrome
2.1. Epidemiology
2.2. Symptoms and Diagnosis
2.3. Correlation of TE with Pelvic Endometriosis
2.4. Histological and Immunohistochemical Characterization of TE
2.5. Pathogenesis of TE
3. Materials and Methods
4. Results
5. Discussion
- The coelomic metaplasia theory suggests that endometriosis arises by metaplasia of coelomic epithelial cells. However, this theory cannot explain why the majority of thoracic endometriosis occurs on the right side of the lung in females. Additionally, TE has never been observed in male pneumothorax [48]. Furthermore, no one has up to date demonstrated how one cell type, the coelomic epithelial cell, can differentiate into two distinct cell types, endometrial epithelial and stromal cells, which must happen in an always highly identical manner at many different sites in the body as diverse as the pelvis up to the brain [49]. Recently, we have casted some doubts on the metaplasia hypothesis [49], but as of yet no one has presented convincing data showing metaplasia of peritoneal cells into endometrial epithelial and stromal cells neither in vivo nor in vitro;
- The stem/progenitor cell theory is mainly advocated by the groups of Gargett [6] and Taylor [50]. They suggest that stem/progenitor cells from the endometrium or bone marrow are responsible for the formation of ectopic endometrial implants. Firstly, the terminology of the cells is somehow diffuse; in the case of pluripotent stem cells, we again have the same problem as with the metaplasia hypothesis, the stem cell must differentiate into two distinct cell types, endometrial epithelial and stromal cells, and this must happen in an identical manner at many different sites in the body [49]. Although a model was presented recently [51], however, no transformation of stem cells into endometrial epithelial and stromal cells has ever been shown to occur at the sites of ectopic endometrial implants. Secondly, in the case of progenitor cells, these cells are already committed to the endometrial lineage, and thus endometrial stromal and epithelial cells can be distinguished. This is not in contradiction to the hypothesis of Sampson, but only an extension. Recently, it was suggested that stem cells might also be the cause of TE [32] and one of the arguments in favor of stem cells was the difference in histologic features between eutopic endometrial tissue and ectopic implants. However, besides the fact that ectopic endometrial implants nearly always have an overtly endometrial phenotype [1], we have recently shown that ectopic endometrial implants are highly similar to eutopic endometrium and have not lost their distinct epithelial characteristics [52].
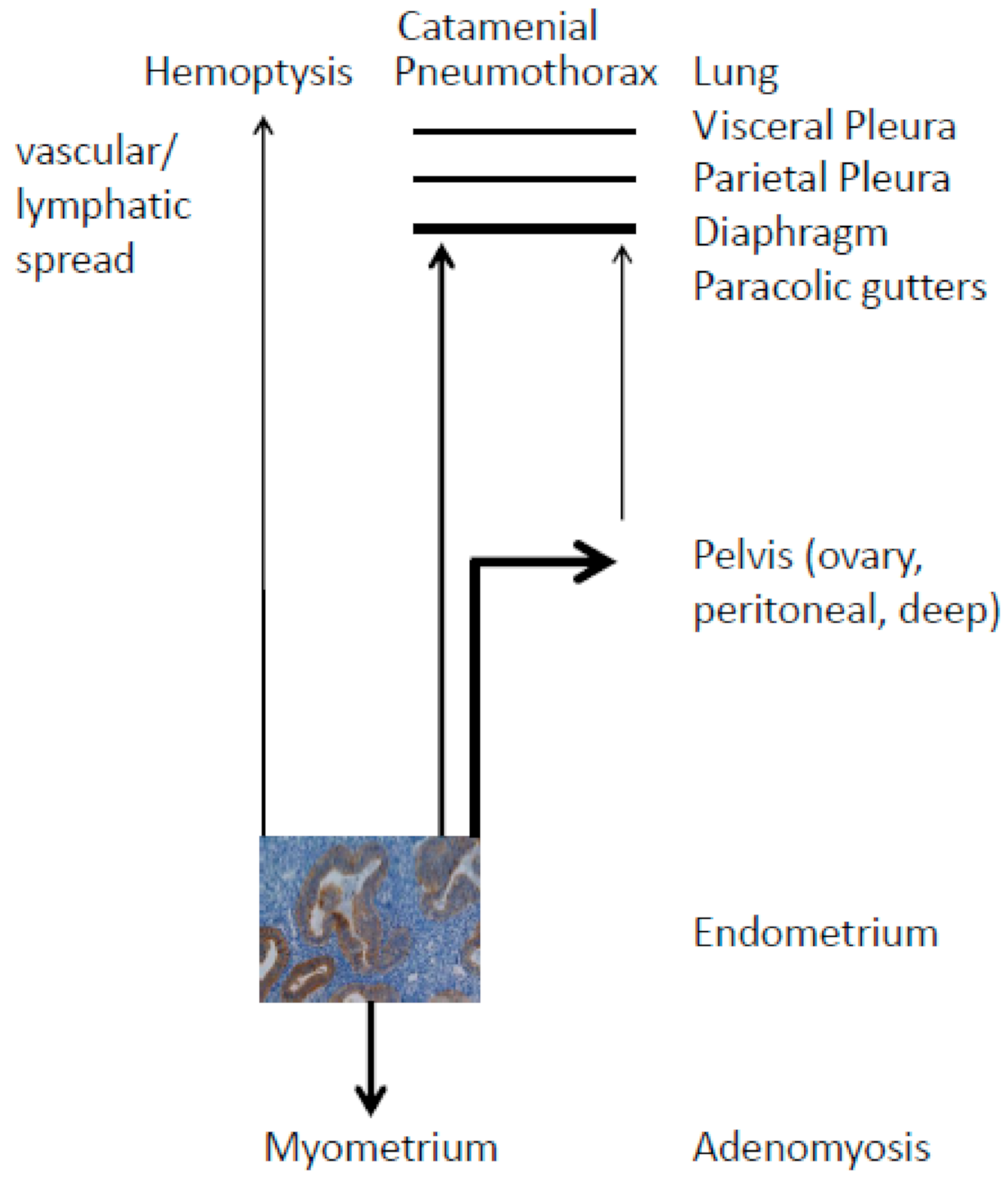
- The hypothesis of retrograde menstruation is the most probable theory to explain the phenomenon of pelvic and thoracic endometriosis. The implantation hypothesis of Sampson [3] is based upon: (a) endometrial tissue breakdown, primarily by menstruation, and (b) migration of endometrial cells through either the fallopian tube and pelvis, primarily by retrograde menstruation, or vascular or lymphatic spread, that results in: (c) invasion and implantation at pelvic or extra-pelvic sites (Figure 1) [53].
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clement, P.B. The pathology of endometriosis: A survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv. Anat. Pathol. 2007, 14, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.W. Fibrogenesis resulting from cyclic bleeding: The Holy Grail of the natural history of ectopic endometrium. Hum. Reprod. 2018, 33, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [Google Scholar] [CrossRef]
- Meyer, R. Zur Frage der heterotopen Epithelwucherung, insbesondere des Peritonealepithels und in die Ovarien. Virch. Arch. Pathol. Anat. Phys. 1924, 250, 595–610. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Wattiez, A.; Gomel, V.; Martin, D.C. Pathogenesis of endometriosis: The genetic/epigenetic theory. Fertil. Steril. 2019, 111, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Gargett, C.E.; Schwab, K.E.; Brosens, J.J.; Puttemans, P.; Benagiano, G.; Brosens, I. Potential role of endometrial stem/progenitor cells in the pathogenesis of early-onset endometriosis. Mol. Hum. Reprod. 2014, 20, 591–598. [Google Scholar] [CrossRef] [Green Version]
- Leyendecker, G.; Kunz, G.; Herbertz, M.; Beil, D.; Huppert, P.; Mall, G.; Kissler, S.; Noe, M.; Wildt, L. Uterine peristaltic activity and the development of endometriosis. Ann. N. Y. Acad. Sci. 2004, 1034, 338–355. [Google Scholar] [CrossRef]
- Signorile, P.G.; Baldi, F.; Bussani, R.; Viceconte, R.; Bulzomi, P.; D’Armiento, M.; D’Avino, A.; Baldi, A. Embryologic origin of endometriosis: Analysis of 101 human female foetuses. J. Cell Physiol. 2012, 227, 1653–1656. [Google Scholar] [CrossRef]
- Brosens, I.; Gargett, C.E.; Guo, S.W.; Puttemans, P.; Gordts, S.; Brosens, J.J.; Benagiano, G. Origins and progression of adolescent endometriosis. Reprod. Sci. 2016, 23, 1282–1288. [Google Scholar] [CrossRef] [Green Version]
- Bulun, S.E.; Yilmaz, B.D.; Sison, C.; Miyazaki, K.; Bernardi, L.; Liu, S.; Kohlmeier, A.; Yin, P.; Milad, M.; Wei, J.J. Endometriosis. Endocr. Rev. 2019, 40, 1048–1079. [Google Scholar] [CrossRef]
- Samimi, M.; Pourhanifeh, M.H.; Mehdizadehkashi, A.; Eftekar, T.; Asemi, Z. The role of inflammation, oxidative stress, angiogenesis, and apoptosis in the pathophysiology of endometrio-sis: Basis science and new insights based on gene expression. J. Cell. Physiol. 2018, 234, 19384–19392. [Google Scholar] [CrossRef] [PubMed]
- Young, V.J.; Brown, J.K.; Saunders, P.T.; Horne, A.W. The role of the peritoneum in the pathogenesis of endometriosis. Hum. Reprod. Update 2013, 19, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Shakiba, K.; Bena, J.F.; McGill, K.; Minger, J.; Falcone, T. Surgical treatment of endometriosis. A 7-year follow-up on the requirement for further surgery. Obstet. Gynecol. 2008, 111, 1285–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alifano, M.; Trisolini, R.; Cancellieri, A.; Regnard, J.F. Thoracic endometriosis: Current knowledge. Ann. Thor. Surg. 2006, 81, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Andres, M.P.; Arcoverde, F.V.L.; Souza, C.C.C.; Fernandes, L.F.C.; Abrão, M.S.; Kho, R.M. Extrapelvic endometriosis: A systematic review. J. Minim. Invasive Gynecol. 2020, 27, 373–389. [Google Scholar] [CrossRef] [Green Version]
- Haga, T.; Kataoka, H.; Ebana, H.; Otsuji, M.; Seyama, K.; Tatsumi, K.; Kurihara, M. Thoracic endometriosis-related pneumothorax distinguished from primary spontaneous pneumothorax in females. Lung 2014, 192, 583–587. [Google Scholar] [CrossRef]
- Alifano, M.; Roth, T.; Camilleri-Broet, S.; Schussler, O.; Magdeleinat, P.; Regnard, J.F. Catamenial pneumothorax: A prospective study. Chest 2003, 124, 1004–1008. [Google Scholar] [CrossRef] [Green Version]
- Hiyama, N.; Sasabuchi, Y.; Jo, T.; Hirata, T.; Osuga, Y.; Nakajima, J.; Yasunaga, H. The three peaks in age distribution of females with pneumothorax: A nationwide database study in Japan. Eur. J. Cardiothorac. Surg. 2018, 54, 572–578. [Google Scholar] [CrossRef]
- Nakamura, H.; Konishiike, J.; Sugamura, A.; Takeno, Y. Epidemiology of spontaneous pneumothorax in women. Chest 1986, 89, 378–382. [Google Scholar] [CrossRef] [Green Version]
- Shearin, R.P.; Hepper, N.G.; Payne, W.S. Recurrent spontaneous pneumothorax concurrent with menses. Mayo Clin. Proc. 1974, 49, 98–101. [Google Scholar] [CrossRef]
- Bobbio, A.; Dechartres, A.; Bouam, S.; Damotte, D.; Rabbat, A.; Régnard, J.F.; Roche, N.; Ali-fano, M. Epidemiology of spontaneous pneumothorax: Gender-related differences. Thorax 2015, 70, 653–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirata, T.; Koga, K.; Osuga, Y. Extra-pelvic endometriosis: A review. Reprod. Med. Biol. 2020, 19, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Rousset, P.; Gregory, J.; Rousset-Jablonski, C.; Hugon-Rodin, J.; Regnard, J.F.; Chapron, C.; Coste, J.; Golfier, F.; Revel, M.P. MR diagnosis of diaphragmatic endometriosis. Eur. Radiol. 2016, 26, 3968–3977. [Google Scholar] [CrossRef] [PubMed]
- Ceccaroni, M.; Roviglione, G.; Giampaolino, P.; Clarizia, R.; Bruni, F.; Ruffo, G.; Patrelli, T.S.; De Placido, G.; Minelli, L. Laparoscopic surgical treatment of diaphragmatic endometriosis: A 7-year single-institution retrospective review. Surg. Endosc. 2013, 27, 625–632. [Google Scholar] [CrossRef]
- Alifano, M.; Jablonski, C.; Kadiri, H.; Falcoz, P.; Gompel, A.; Camilleri-Broet, S.; Regnard, J.F. Catamenial and noncatamenial, endometriosis-related or nonendometriosis-related pneumothorax referred for surgery. Am. J. Respir. Crit. Care Med. 2007, 176, 1048–1053. [Google Scholar] [CrossRef]
- Flieder, D.B.; Moran, C.A.; Travis, W.D.; Koss, M.N.; Mark, E.J. Pleuro-pulmonary endometriosis and pulmonary ectopic deciduosis: A clinicopathologic and immunohistochemical study of 10 cases with emphasis on diagnostic pitfalls. Hum. Pathol. 1998, 29, 1495–1503. [Google Scholar] [CrossRef]
- Haga, T.; Kumasaka, T.; Kurihara, M.; Kataoka, H.; Miura, M. Immunohistochemical analysis of thoracic endometriosis. Pathol. Int. 2013, 63, 429–434. [Google Scholar] [CrossRef]
- Hiraike, O.; Kurihara, M.; Fujii, T.; Osuga, Y. IFITM1 is a novel, highly sensitive marker for endometriotic stromal cells in ovarian and extragenital endometriosis. Reprod. Sci. 2020, 27, 1595–1601. [Google Scholar]
- Mataca, E.; Rossi, G.; Colby, T.V. The helpful role of CD10 and hormonal receptors co-expression in the histologic diagnosis of catamenial pneumothorax. Int. J. Surg. Pathol. 2019, 27, 593–597. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Hanaoka, J.; Ohshio, Y.; Igarashi, T.; Okamoto, K.; Kaku, R.; Hayashi, K.; Ishida, M. Diagnosis of thoracic endometriosis with immunohistochemistry. J. Thorac. Dis. 2018, 10, 3468–3472. [Google Scholar] [CrossRef]
- Arakawa, T.; Fukuda, S.; Hirata, T.; Neriishi, K.; Wang, Y.; Takeuchi, A.; Saeki, A.; Harada, M.; Hirota, Y.; Matsumoto, T.; et al. Pax8: A highly sensitive marker for the glands in extragenital endometriosis. Reprod. Sci. 2020, 27, 1580–1586. [Google Scholar] [CrossRef] [PubMed]
- Channabasavaiah, A.D.; Joseph, J.V. Thoracic endometriosis: Revisiting the association between clinical presentation and thoracic pathology based on thoracoscopic findings in 110 patients. Medicine 2010, 89, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Kumakiri, J.; Kumakiri, Y.; Miyamoto, H.; Kikuchi, I.; Arawaka, A.; Kitade, M.; Takeda, S. Gynecologic evaluation of catamenial pneumothorax associated with endometriosis. J. Minim. Invasive Gynecol. 2010, 17, 593–599. [Google Scholar] [CrossRef]
- Maniglio, P.; Ricciardi, E.; Meli, F.; Vitale, S.G.; Noventa, M.; Vitagliano, A.; Valenti, G.; La Rosa, V.L.; Laganà, A.S.; Caserta, D. Catamenial pneumothorax caused by thoracic endometriosis. Radiol. Case Rep. 2018, 13, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D.P.; McCluggage, W.G. Peritoneal stromal endometriosis: A detailed morphological analysis of a large series of cases of common and under-recognised form of endometriosis. J. Clin. Pathol. 2009, 62, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Kanzaki, H.; Fujiwara, H.; Kariya, M.; Okamoto, N.; Takakura, K.; Maeda, M.; Mori, T. Expression of aminopeptidase N and neutral endopeptidase on the endometrial stromal cells in endometriosis and adenomyosis. Hum. Reprod. 1992, 7, 1326–1328. [Google Scholar] [CrossRef]
- Sumathi, V.P.; McGluggage, W.G. CD10 is useful in demonstrating endometrial sites and in confirming a diagnosis of endometriosis. J. Clin. Pathol. 2002, 55, 391–392. [Google Scholar] [CrossRef] [Green Version]
- Capobianco, G.; Wenger, J.M.; Cosmi, E.; Ambrosini, G.; Dessole, M.; Cherchi, P.L. Immunohistochemical evaluation of epithelial antigen Ber-Ep4 and CD10: New markers for endometriosis? Eur. J. Gynaecol. Oncol. 2013, 34, 254–256. [Google Scholar]
- Groisman, G.M.; Meir, A. CD10 is helpful in detecting occult or inconspicuous endometrial stromal cells in cases of presumptive endometriosis. Arch. Pathol. Lab. Med. 2003, 127, 1003–1006. [Google Scholar]
- Branscomb, L. Habitual premenstrual spotting following electrocauterization of the cervix: A newly observed phenomenon. Am. J. Obstet. Gynecol. 1960, 79, 16–23. [Google Scholar] [CrossRef]
- Viganó, P.; Ottolina, J.; Bartiromo, L.; Bonavina, G.; Schimberni, M.; Villanacci, R.; Candiani, M. Cellular components contributing to fibrosis in endometriosis: A literature review. J. Minim. Invasive Gynecol. 2020, 27, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Marchino, G.L.; Gennarelli, G.L.; Enria, R.; Bongioanni, F.; Lipari, G.; Massobrio, M. Diagnosis of pelvic endometriosis with use of macroscopic versus histological findings. Fertil. Steril. 2005, 84, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Governini, L.; Carrarelli, P.; Rocha, A.L.L.; De Leo, V.; Luddi, A.; Arcuri, F.; Piombino, P.; Chapron, C.; Bilezkjian, L.M.; Petraglia, F. FOXL2 in human endometrium: Hyperexpressed in endometriosis. Reprod. Sci. 2014, 21, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Evers, J.L.H.; Dunselman, G.A.J.; Groothuis, P. Now you see them, now you don’t. Fertil. Steril. 2005, 84, 31–32. [Google Scholar] [CrossRef]
- Al-Taher, M.; Hsien, S.; Schols, R.M.; Hanegem, N.V.; Bouvy, N.D.; Dunselman, G.A.J.; Stas-sen, L.P.S. Intraoperative enhanced imaging for detection of endometriosis: A systematic review of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 108–116. [Google Scholar] [CrossRef]
- Lee, J.W.; Park, C.H.; Lee, S.M.; Jeong, M.; Hur, J. Planting seeds into the lung: Image-guided percutaneous localization to guide minimally invasive thoracic surgery. Korean J. Radiol. 2019, 20, 1498–1514. [Google Scholar] [CrossRef]
- Rodrigues, J.C.L.; Pierre, A.F.; Hanneman, K.; Cabanero, M.; Kavanagh, J.; Waddell, T.K.; Chung, T.B.; Pakkal, M.; Keshavjee, S.; Cypel, M.; et al. CT-guided micro-coil pulmonary nodule localization prior to video-assisted thoracoscopic surgery: Diagnostic utility and recurrence-free survival. Radiology 2019, 291, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.M. Catamenial pneumothorax and other thoracic manifestations of endometriosis. Clin. Chest Med. 2004, 25, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Konrad, L.; Dietze, R.; Kudipudi, P.K.; Horné, F.; Meinhold-Heerlein, I. Endometriosis in MRKH cases as a proof for the coelomic metaplasia hypothesis? Reproduction 2019, 158, R41–R47. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.S. Endometrial cells derived from donor stem cells in bone marrow transplant recipients. JAMA 2004, 292, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Nicholes, K.; Shih, L.M. The origin and pathogenesis of endometriosis. Ann. Rev. Pathol. 2020, 15, 71–95. [Google Scholar] [CrossRef] [Green Version]
- Konrad, L.; Gronbach, J.; Horné, F.; Mecha, E.O.; Berkes, E.; Frank, M.; Gattenlöhner, S.; Omwandho, C.O.; Oehmke, F.; Tinneberg, H.R. Similar characteristics of the endometrial and endo-metriotic epithelium. Reprod. Sci. 2019, 26, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Yovich, J.L.; Rowlands, P.K.; Lingham, S.; Sillender, M.; Srinivasan, S. Pathogenesis of endometriosis: Look no further than John Sampson. Reprod. Biomed. Online 2020, 40, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omwandho, C.O.A.; Konrad, L.; Halis, G.; Oehmke, F.; Tinneberg, H.R. Role of TGF-βs in normal human endometrium and endometriosis. Hum. Reprod. 2010, 25, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paget, S. The distribution of secondary growths in cancer of the breast. Lancet 1889, 133, 571–573. [Google Scholar] [CrossRef] [Green Version]
- Konrad, L.; Dietze, R.; Riaz, M.A.; Scheiner-Bobis, G.; Behnke, J.; Horné, F.; Hoerscher, A.; Reising, C.; Meinhold-Heerlein, I. Epithelial-mesenchymal transition in endometriosis—When does it happen? J. Clin. Med. 2020, 9, 1915. [Google Scholar] [CrossRef]
- Webb, C.A.J.; Weber, G.M.; Raker, R.K. Anesthetic evaluation and management of a patient with thoracic endometriosis syndrome presenting for elective surgery. J. Clin. Anesth. 2013, 25, 220–223. [Google Scholar] [CrossRef]
- Hobbs, J.E.; Bortnick, A.R. Endometriosis of the lungs: An experimental and clinical study. Am. J. Obstet. Gynecol. 1940, 40, 832–843. [Google Scholar] [CrossRef]
- Samani, E.N.; Mamillapalli, R.; Li, F.; Mutlu, L.; Hufnagel, D.; Krikun, G.; Taylor, H.S. Micrometastases of endometriosis to distant organs in a murine model. Oncotarget 2019, 10, 2282–2291. [Google Scholar] [CrossRef] [Green Version]
- Kiss, I.; Pospisilova, E.; Kolostova, K.; Maly, V.; Stanek, I.; Lischke, R.; Schutzner, J.; Pawlak, I.; Bobek, V. Circulating endometrial cells in women with spontaneous pneumothorax. Chest 2020, 157, 342–355. [Google Scholar] [CrossRef]
- Fukuda, S.; Hirata, T.; Neriishi, K. Thoracic endometriosis syndrome: Comparison between catamenial pneumothorax or endometriosis-related pneumothorax and catamenial hemoptysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Sugimura, K.; Sasaki, O.; Shinoda, M.; Kawasaki, S.; Shinkai, M. Catamenial pneumothorax: A cause of monthly breathlessness. Lancet 2019, 394, 952. [Google Scholar] [CrossRef]
- Shresta, B.; Shresta, S.; Peters, P.; Ura, M.; Windsor, M.; Naidoo, R. Catamenial pneumotho-rax, a commonly misdiagnosed thoracic condition: Multicentre experience and audit of a small case series with review of the literature. Heart Lung Circ. 2019, 28, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, I.; Hidaka, T.; Kusabiraki, T.; Kochi, K.; Yasoshima, K.; Takagawa, K.; Saito, S. Chemical pleurodesis with autologous blood and freeze-dried concentrated human thrombin im-proved spontaneous pneumothorax and thoracic endometriosis: The first case involving a preg-nant woman. Taiwan J. Obstet. Gynecol. 2018, 57, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Kurihara, M.; Mizobuchi, T.; Ebana, H.; Yamanaka, S. Left-sided catamenial pneumothorax with thoracic endometriosis and bullae in the alveolar wall. Ann. Thorac. Cardiovasc. Surg. 2017, 23, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Yukumi, S.; Suzuki, H.; Morimoto, M.; Shigematsu, H.; Okazaki, M.; Abe, M.; Kitazawa, S.; Nakamura, K.; Sano, Y. Two young women with left-sided pneumothorax due to thoracic endometriosis. Intern. Med. 2016, 55, 3491–3493. [Google Scholar] [CrossRef] [Green Version]
- Ghigna, M.R.; Mercier, O.; Mussot, S.; Fabre, D.; Fadel, E.; Dorfmuller, P.; de Montepreville, V.T. Thoracic endometriosis: Clinicopathologic updates and issues about 18 cases from a tertiary referring center. Ann. Diagn. Pathol. 2015, 19, 320–325. [Google Scholar] [CrossRef]
- Ichiki, Y.; Nagashima, A.; Yasuda, M.; Takenoyama, M.; Toyoshima, S. Surgical treatment of catamenial pneumothorax: Report of three cases. Asian J. Surg. 2015, 38, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Nemeş, R.M.; Paleru, C.; Dănăilă, O.; Ianoşi, E.S.; Pop, C.S.; Diţescu, D.; Streba, C.T.; Niţu, M.F. Thoracic endometriosis with a long delay in diagnosis. Rom. J. Morphol. Embryol. 2015, 56, 295–300. [Google Scholar]
- Inoue, T.; Chida, M.; Inaba, H.; Tamura, M.; Kobayashi, S.; Sado, T. Juvenile catamenial pneumothorax: Institutional report and review. J. Cardiothorac. Surg. 2015, 10, 83. [Google Scholar] [CrossRef] [Green Version]
- Kawaguchi, Y.; Fujita, T.; Hanaoka, J. Catamenial pneumothorax with bullae. Ann. Thorac. Surg. 2015, 99, 1075–1078. [Google Scholar] [CrossRef] [PubMed]
- Legras, A.; Mansuet-Lupo, A.; Rousset-Jablonski, C.; Bobbio, A.; Magdeleinat, P.; Roche, N.; Regnard, J.F.; Gompel, A.; Damotte, D.; Alifano, M. Pneumothorax in women of child-bearing age. Chest 2014, 145, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, M.; Yamaura, T.; Kanno, R.; Suzuki, H.; Asano, S.; Gotoh, M. Incidental early lung adenocarcinoma after surgery for catamenial pneumothorax. Fukushima J. Med. Sci. 2012, 58, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, H.Y.; Jan, C.I.; Chen, C.K.; Chen, W.T.L. Catamenial pneumothorax due to bilateral pulmonary endometriosis. Respir. Care 2012, 57, 1182–1185. [Google Scholar] [CrossRef] [PubMed]
- Poh, C.L.; Yan, T.D.; Vallely, M.P.; Bannon, P.G.; McCaughan, B.C. Pulmonary parenchymal endometriosis presenting as bilateral pneumothoraces. J. Obstet. Gynaecol. 2011, 31, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.D.; Min, K.O.; Moon, S.W. Thorascopic treatment of recurrent pneumothorax in a pregnant woman: A case of ectopic deciduosis. Thorac. Cardiovasc. Surg. 2010, 58, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Kumakiri, J.; Takeuchi, H.; Miyamoto, H.; Shimanuki, H.; Kobayashi, Y.; Kuroda, K. An advanced flexible laparoscope with wide optic angle for observing diaphragmatic lesions associated with catamenial pneumothorax. Fertil. Steril. 2008, 90, 1200.e11–1200.e14. [Google Scholar] [CrossRef]
- Morcos, M.; Alifano, M.; Gompel, A.; Regnard, J.F. Life-threatening endometriosis-related hemopneumothorax. Ann. Thorac. Surg. 2006, 82, 726–729. [Google Scholar] [CrossRef]
- Korom, S.; Canyurt, H.; Missbach, A.; Schneiter, D.; Kurrer, M.O.; Haller, U.; Keller, P.J.; Fur-rer, M.; Weder, W. Catamenial pneumothorax revisited: Clinical approach and systematic review of the literature. J. Thorac. Cardiovasc. Surg. 2004, 128, 502–508. [Google Scholar] [CrossRef] [Green Version]
- Fukunaga, M. Catamenial pneumothorax caused by diaphragmatic stromal endometriosis. APMIS 1999, 107, 685–688. [Google Scholar] [CrossRef]
- Tsunezuka, Y.; Sato, H.; Kodama, T.; Shimizu, H.; Kurumaya, H. Expression of CA125 in thoracic endometriosis in a patient with catamenial pneumothorax. Respiration 1999, 66, 470–472. [Google Scholar] [CrossRef]
- AlAqeel, S.; AlJehani, Y.; AlMuhaish, M. Bilateral catamenial hemopneumothorax: Diagnostic & management challenges. Int. J. Surg. Case Rep. 2019, 61, 271–274. [Google Scholar] [PubMed]
- Junejo, S.Z.; Singh Lubana, S.; Singh Shina, S.; Singh Tuli, S. A case of thoracic endometriosis syndrome presenting with recurrent catamenial pneumothorax. Am. J. Case Rep. 2018, 19, 573–576. [Google Scholar] [CrossRef]
- Furuta, C.; Yano, M.; Numanami, H.; Yamaji, M.; Taguchi, R.; Haniuda, M. Nine cases of catamenial pneumothorax: A report of a single-center experience. J. Thorac. Dis. 2018, 10, 4801–4805. [Google Scholar] [CrossRef] [PubMed]
- Larraín, D.; Suárez, F.; Braun, H.; Chapochnick, J.; Diaz, L.; Rojas, I. Thoracic and diaphragmatic endometriosis: Single-institution experience using novel, broadened diagnostic criterial. J. Turk. Ger. Gynecol. Assoc. 2018, 19, 116–121. [Google Scholar] [CrossRef]
- Tulandi, T.; Sirois, C.; Sabban, H.; Cohen, A.; Murji, A.; Singh, S.S.; Chen, I.; Belland, L. Relationship between catamenial pneumothorax or non-catamenial pneumothorax and endometriosis. J. Minim. Invasive Gynecol. 2018, 25, 480–483. [Google Scholar] [CrossRef]
- Ottolina, J.; De Stefano, F.; Viganò, P.; Ciriaco, P.; Zannini, P.; Candiani, M. Thoracic endometriosis syndrome: Association with pelvic endometriosis and fertility status. J. Minim. Invasive Gynecol. 2017, 24, 461–465. [Google Scholar] [CrossRef]
- Aissa, S.; Benzarti, W.; Alimi, F.; Gargouri, I.; Salem, H.B.; Aissa, A.; Fathallah, K.; Abdelkade, A.B.; Alouini, R.; Garrouche, A.; et al. Catamenial pneumothorax revealing diaphragmatic endometriosis: A case report and revue of the literature. Pan Afr. Med. J. 2017, 27, 112. [Google Scholar] [CrossRef] [PubMed]
- Subotic, D.; Mikovic, Z.; Atanasijadis, N.; Savic, M.; Moskovljevic, D.; Subotic, D. Hormonal therapy after the operation for catamenial pneumothorax—Is it always necessary? J. Cardiothorac. Surg. 2016, 11, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, S.S.; Nayar, J. Thoracic endometriosis syndrome: A veritable pandora’s box. J. Clin. Diagn. Res. 2016, 10, QR04. [Google Scholar] [CrossRef]
- Elia, S.; De Felice, L.; Varvaras, D.; Sorrenti, G.; Mauriello, A.; Petrella, G. Catamenial pneumothorax due to solitary localization of diaphragmatic endometriosis. Int. J. Surg. Case Rep. 2015, 12, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.M.; Lee, C.W.; Lee, B.S.; Park, J.H. Clinical features of thoracic endometriosis: A single center analysis. Obstet. Gynecol. Sci. 2015, 58, 223–231. [Google Scholar] [CrossRef]
- Takahashi, M.; Matsukura, T.; Hirai, T.; Mino, N. Recurrent catamenial hemopneumothorax treated by coverage with polyglycolic acid sheets. J. Thorac. Cardiovasc. Surg. 2013, 145, 300–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, L.M.; Redan, J.; Reich, H. Extraperitoneal endometriosis with catamenial pneumothoraces: A review of the literature. JSLS 2003, 7, 371–375. [Google Scholar] [PubMed]
- Redwine, D.B. Diaphragmatic endometriosis: Diagnosis, surgical management, and long-term results of treatment. Fertil. Steril. 2002, 77, 288–296. [Google Scholar] [CrossRef]
- Blanco, S.; Hernando, F.; Gómez, A.; González, M.J.; Torres, A.J.; Balibrea, J.L. Catamenial pneumothorax caused by diaphragmatic endometriosis. J. Thorac. Cardiovasc.Surg. 1998, 116, 179–180. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parameters | CPE | CPH | p Values |
|---|---|---|---|
| Age | 36.3 ± 8.7 | 37.0 ± 6.2 | n.s. |
| Chest pain | 82.9% | 82.1% | n.s. |
| Dyspnea | 92.7% | 74.4% | n.s. |
| Cough | 58.5% | 48.7% | n.s. |
| Imaging | |||
| Chest, X-ray | 20.2% | 26.5% | n.c. |
| CT | 7.7% | 46.9% | n.c. |
| Operation | |||
| VATS | 71.9% | 76.0% | n.s. |
| Lesions found | |||
| Diaphragm | 81.8% | 85.7% | n.s. |
| Pleura | 31.4% | 22.0% | n.s. |
| Lung | 10.5% | 8.7% | n.s. |
| CP, right-sided | 90.7% | 89.8% | n.s. |
| CP, bilateral | 2.8% | 8.2% | n.c. |
| CP, left-sided | 3.7% | 0% | n.c. |
| Concomitant pelvic endometriosis | 43.1% | 70.7% | 0.0012 |
| TE | |||
| Stromal | 52.7% | 10.2% | <0.0001 |
| Glands/stroma | 36.8% | 55.1% | =0.0185 |
| Glands | 1.4% | 0% | n.c. |
| Positive, n.sp. | 2.3% | 4.1% | n.c. |
| Negative | 6.8% | 30.6% | n.c. |
| Detection | |||
| ER | 95.1% | ||
| PR | 94.7% | ||
| CD10 | 91.3% | ||
| All three | 88.3% |
| Recurrence | No Recurrence | p Values | |
|---|---|---|---|
| Glands/stroma | 10 | 20 | n.s. |
| Stroma | 9 | 8 | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mecha, E.; Makunja, R.; Maoga, J.B.; Mwaura, A.N.; Riaz, M.A.; Omwandho, C.O.A.; Meinhold-Heerlein, I.; Konrad, L. The Importance of Stromal Endometriosis in Thoracic Endometriosis. Cells 2021, 10, 180. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10010180
Mecha E, Makunja R, Maoga JB, Mwaura AN, Riaz MA, Omwandho COA, Meinhold-Heerlein I, Konrad L. The Importance of Stromal Endometriosis in Thoracic Endometriosis. Cells. 2021; 10(1):180. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10010180
Chicago/Turabian StyleMecha, Ezekiel, Roselydiah Makunja, Jane B. Maoga, Agnes N. Mwaura, Muhammad A. Riaz, Charles O. A. Omwandho, Ivo Meinhold-Heerlein, and Lutz Konrad. 2021. "The Importance of Stromal Endometriosis in Thoracic Endometriosis" Cells 10, no. 1: 180. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10010180