
Association between Markers of Synovial Inflammation, Matrix Turnover and Symptoms in Knee Osteoarthritis: A Cross-Sectional Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
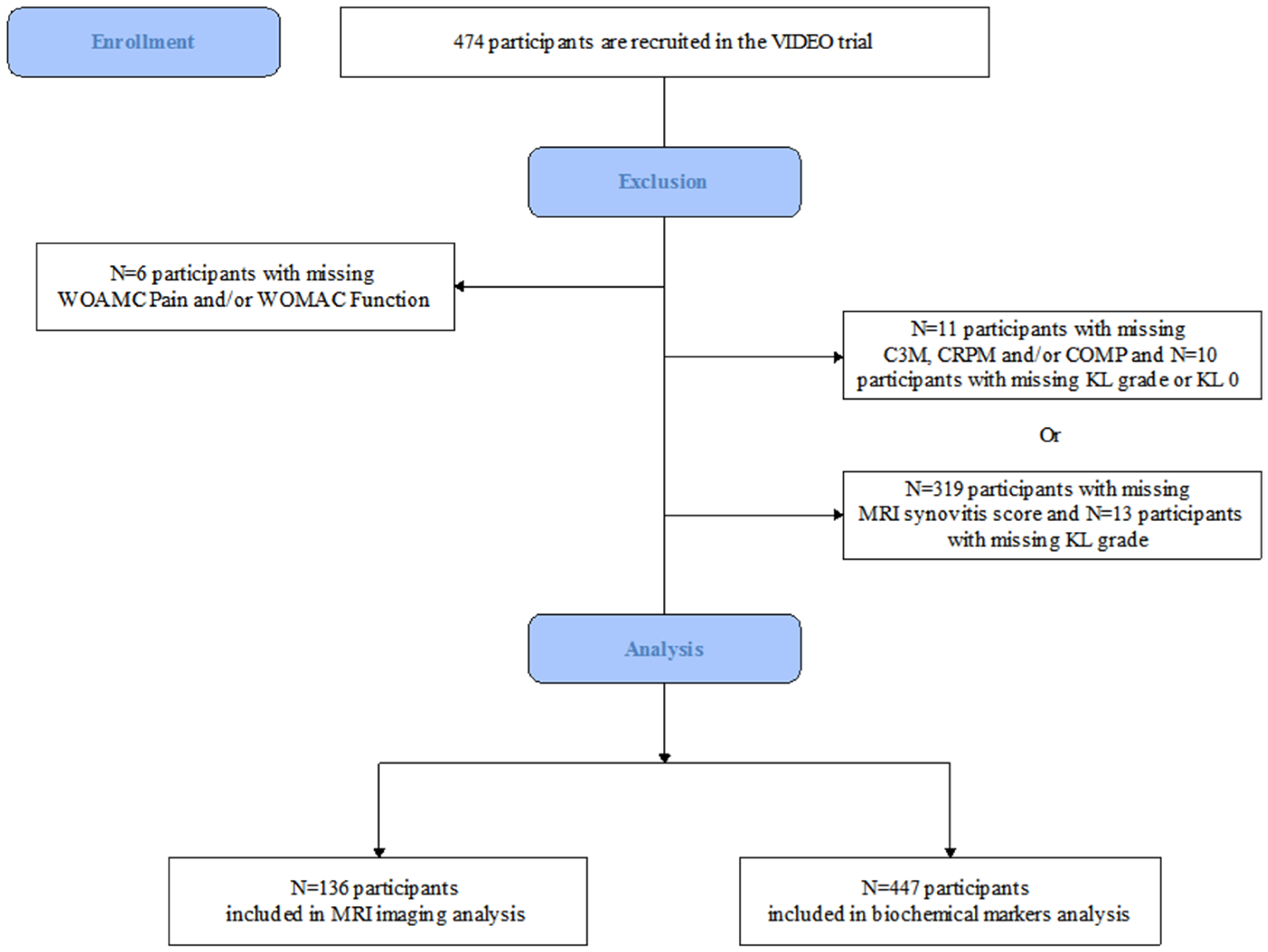
2.1. Study Population
2.2. MRI Acquisition and Assessment
2.3. Biochemical Markers
2.4. Statistical Analysis
3. Results
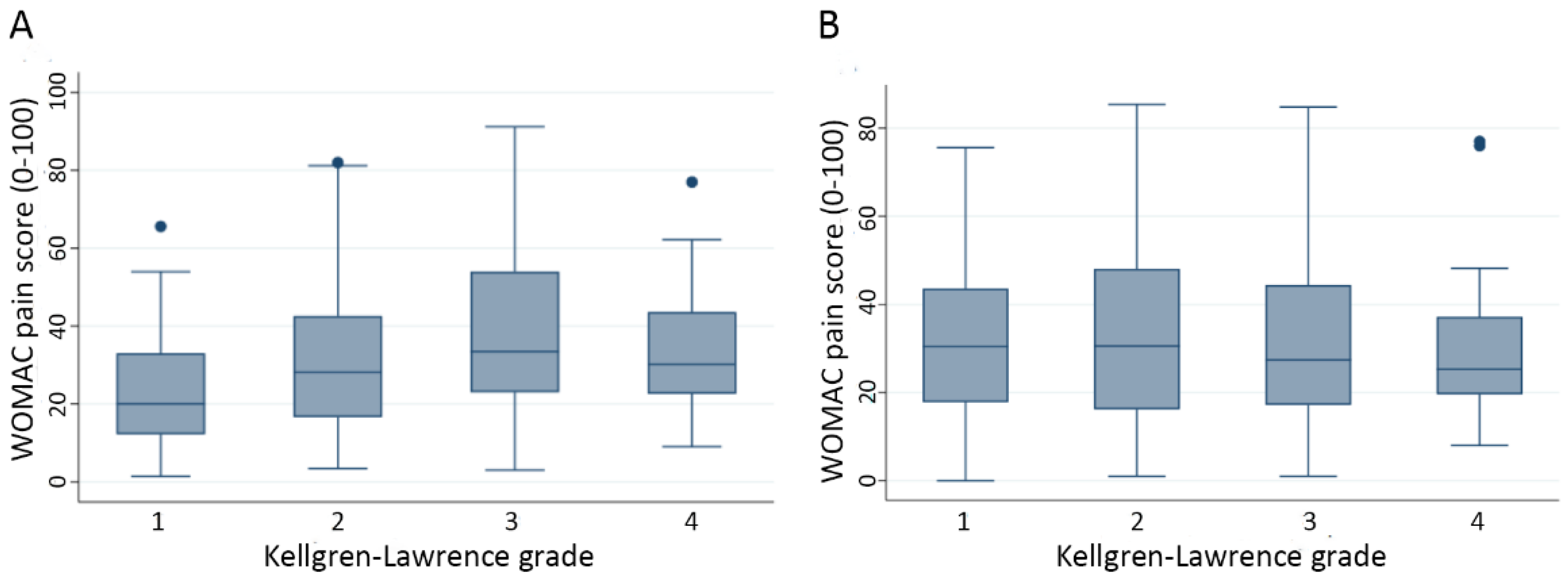
3.1. Participants Characteristics
3.2. MRI-Defined Semi-Quantitative Synovitis Thickness
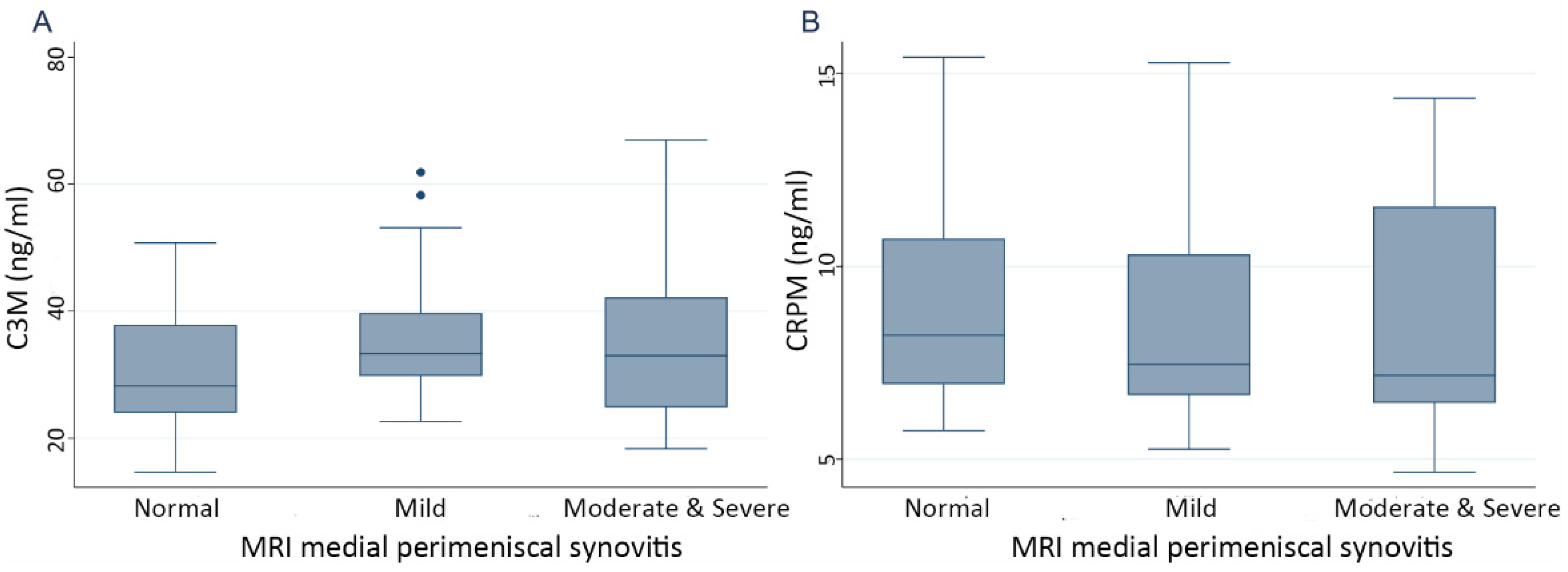
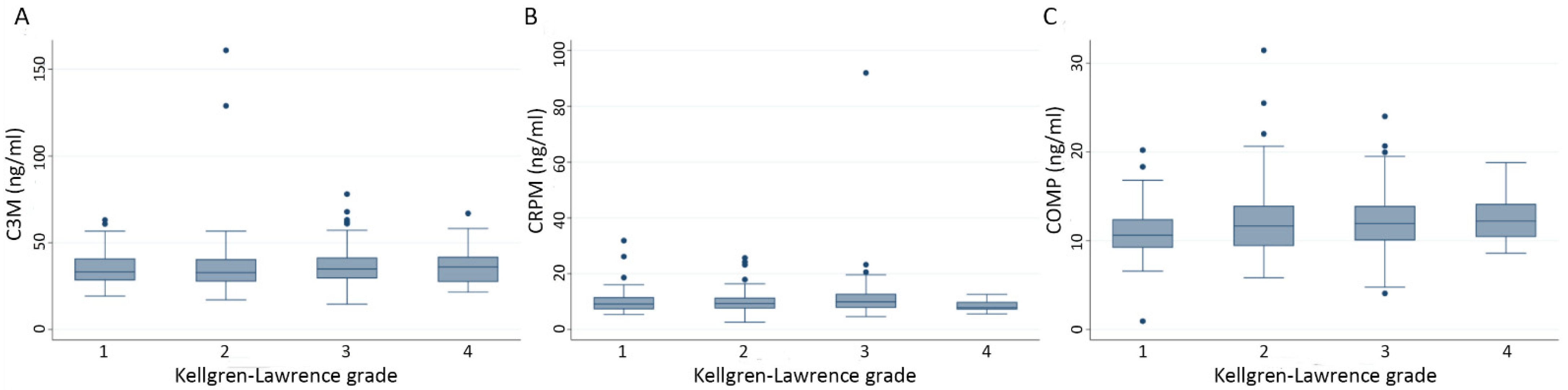
3.3. Biochemical Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

Appendix C

References
- Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Felson, D.T. Clinical practice. osteoarthritis of the knee. N. Engl. J. Med. 2006, 354, 841–848. [Google Scholar] [CrossRef]
- Driban, J.B.; Sitler, M.R.; Barbe, M.F.; Balasubramanian, E. Is osteoarthritis a heterogeneous disease that can be stratified into subsets? Clin. Rheumatol. 2010, 29, 123–131. [Google Scholar] [CrossRef]
- Lories, R.J.; Luyten, F.P. The bone-cartilage unit in osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Sellam, J.; Berenbaum, F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat. Rev. Rheumatol. 2010, 6, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Guermazi, A.; Hayashi, D.; Roemer, F.W.; Zhu, Y.; Niu, J.; Crema, M.D.; Javaid, M.K.; Marra, M.D.; Lynch, J.A.; El-Khoury, G.Y.; et al. Synovitis in knee osteoarthritis assessed by contrast-enhanced magnetic resonance imaging (MRI) is associated with radiographic tibiofemoral osteoarthritis and MRI-detected widespread cartilage damage: The MOST study. J. Rheumatol. 2014, 41, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roemer, F.W.; Guermazi, A.; Felson, D.T.; Niu, J.; Nevitt, M.C.; Crema, M.D.; Lynch, J.A.; Lewis, C.E.; Torner, J.; Zhang, Y. Presence of MRI-detected joint effusion and synovitis increases the risk of cartilage loss in knees without osteoarthritis at 30-month follow-up: The MOST study. Ann. Rheum. Dis. 2011, 70, 1804–1809. [Google Scholar] [CrossRef]
- Collins, J.E.; Losina, E.; Nevitt, M.C.; Roemer, F.W.; Guermazi, A.; Lynch, J.A.; Katz, J.N.; Kent Kwoh, C.; Kraus, V.B.; Hunter, D.J. Semiquantitative imaging biomarkers of knee osteoarthritis progression: Data from the Foundation for the National Institutes of Health Osteoarthritis Biomarkers Consortium. Arthritis Rheumatol. 2016, 68, 2422–2431. [Google Scholar] [CrossRef]
- Rim, Y.A.; Ju, J.H. The role of fibrosis in osteoarthritis progression. Life 2020, 11, 3. [Google Scholar] [CrossRef]
- Remst, D.F.; Blaney Davidson, E.N.; van der Kraan, P.M. Unravelling osteoarthritis-related synovial fibrosis: A step closer to solving joint stiffness. Rheumatology 2015, 54, 1954–1963. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Wang, H.; He, J.Y.; Wang, C.L.; Feng, W.J.; Shen, C.; Zhu, J.F.; Wang, D.L.; Chen, X.D. Inflammatory and fibrosis infiltration in synovium associated with the progression in developmental dysplasia of the hip. Mol. Med. Rep. 2019, 19, 2808–2816. [Google Scholar] [CrossRef] [PubMed]
- Bastick, A.N.; Belo, J.N.; Runhaar, J.; Bierma-Zeinstra, S.M. What are the prognostic factors for radiographic progression of knee osteoarthritis? A meta-analysis. Clin. Orthop. Relat. Res. 2015, 473, 2969–2989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Nevitt, M.; Niu, J.; Lewis, C.; Torner, J.; Guermazi, A.; Roemer, F.; McCulloch, C.; Felson, D.T. Fluctuation of knee pain and changes in bone marrow lesions, effusions, and synovitis on magnetic resonance imaging. Arthritis Rheum. 2011, 63, 691–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, C.L.; Hunter, D.J.; Niu, J.; Clancy, M.; Guermazi, A.; Genant, H.; Gale, D.; Grainger, A.; Conaghan, P.; Felson, D.T. Synovitis detected on magnetic resonance imaging and its relation to pain and cartilage loss in knee osteoarthritis. Ann. Rheum. Dis. 2007, 66, 1599–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, T.A.; Parkes, M.J.; Hodgson, R.J.; Felson, D.T.; Arden, N.K.; O’Neill, T.W. Association between bone marrow lesions & synovitis and symptoms in symptomatic knee osteoarthritis. Osteoarthr. Cartil. 2020, 28, 316–323. [Google Scholar]
- Kraus, V.B.; Burnett, B.; Coindreau, J.; Cottrell, S.; Eyre, D.; Gendreau, M.; Gardiner, J.; Garnero, P.; Hardin, J.; Henrotin, Y.; et al. Application of biomarkers in the development of drugs intended for the treatment of osteoarthritis. Osteoarthr. Cartil. 2011, 19, 515–542. [Google Scholar] [CrossRef] [Green Version]
- Baker, K.; Grainger, A.; Niu, J.; Clancy, M.; Guermazi, A.; Crema, M.; Hughes, L.; Buckwalter, J.; Wooley, A.; Nevitt, M.; et al. Relation of synovitis to knee pain using contrast-enhanced MRIs. Ann. Rheum. Dis. 2010, 69, 1779–1783. [Google Scholar] [CrossRef] [Green Version]
- Loeuille, D.; Sauliere, N.; Champigneulle, J.; Rat, A.C.; Blum, A.; Chary-Valckenaere, I. Comparing non-enhanced and enhanced sequences in the assessment of effusion and synovitis in knee OA: Associations with clinical, macroscopic and microscopic features. Osteoarthr. Cartil. 2011, 19, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- Wallace, G.; Cro, S.; Dore, C.; King, L.; Kluzek, S.; Price, A.; Roemer, F.; Guermazi, A.; Keen, R.; Arden, N. Associations between clinical evidence of inflammation and synovitis in symptomatic knee osteoarthritis: A cross-sectional substudy. Arthritis Care Res. 2017, 69, 1340–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, T.A.; Yang, X.; van Santen, J.; Arden, N.K.; Kluzek, S. Quantitative and semi-quantitative assessment of synovitis on MRI and the relationship with symptoms in symptomatic knee osteoarthritis. Rheumatology 2020, 60, 1763–1773. [Google Scholar] [CrossRef]
- Kaukinen, P.; Podlipska, J.; Guermazi, A.; Niinimaki, J.; Lehenkari, P.; Roemer, F.W.; Nieminen, M.T.; Koski, J.M.; Arokoski, J.P.; Saarakkala, S. Associations between MRI-defined structural pathology and generalized and localized knee pain—The Oulu Knee Osteoarthritis study. Osteoarthr. Cartil. 2016, 24, 1565–1576. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Jin, X.; Han, W.; Cao, Y.; Halliday, A.; Blizzard, L.; Pan, F.; Antony, B.; Cicuttini, F.; Jones, G.; et al. Cross-sectional and longitudinal associations between knee joint effusion synovitis and knee pain in older adults. J. Rheumatol. 2016, 43, 121–130. [Google Scholar] [CrossRef]
- Felson, D.T.; Niu, J.; Neogi, T.; Goggins, J.; Nevitt, M.C.; Roemer, F.; Torner, J.; Lewis, C.E.; Guermazi, A. Synovitis and the risk of knee osteoarthritis: The MOST Study. Osteoarthr. Cartil. 2016, 24, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Patry, R. Contribution a l’étude des lesions traumatiques des menisques. La ménisco-synovite traumatique. Congrés Français Chir. 1926, 35, 149–155. [Google Scholar]
- Ayral, X.; Pickering, E.H.; Woodworth, T.G.; Mackillop, N.; Dougados, M. Synovitis: A potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis—Results of a 1 year longitudinal arthroscopic study in 422 patients. Osteoarthr. Cartil. 2005, 13, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakoor, D.; Demehri, S.; Roemer, F.W.; Loeuille, D.; Felson, D.T.; Guermazi, A. Are contrast-enhanced and non-contrast MRI findings reflecting synovial inflammation in knee osteoarthritis: A meta-analysis of observational studies. Osteoarthr. Cartil. 2020, 28, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Labinsky, H.; Panipinto, P.M.; Ly, K.A.; Khuat, D.K.; Madarampalli, B.; Mahajan, V.; Clabeaux, J.; MacDonald, K.; Verdin, P.J.; Buckner, J.H.; et al. Multiparameter analysis identifies heterogeneity in knee osteoarthritis synovial responses. Arthritis Rheumatol. 2020, 72, 598–608. [Google Scholar] [CrossRef]
- Siebuhr, A.S.; Petersen, K.K.; Arendt-Nielsen, L.; Egsgaard, L.L.; Eskehave, T.; Christiansen, C.; Simonsen, O.; Hoeck, H.C.; Karsdal, M.A.; Bay-Jensen, A.C. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthr. Cartil. 2014, 22, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.K.; Siebuhr, A.S.; Graven-Nielsen, T.; Simonsen, O.; Boesen, M.; Gudbergsen, H.; Karsdal, M.; Bay-Jensen, A.C.; Arendt-Nielsen, L. Sensitization and serological biomarkers in knee osteoarthritis patients with different degrees of synovitis. Clin. J. Pain 2016, 32, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Kluzek, S.; Bay-Jensen, A.C.; Judge, A.; Karsdal, M.A.; Shorthose, M.; Spector, T.; Hart, D.; Newton, J.L.; Arden, N.K. Serum cartilage oligomeric matrix protein and development of radiographic and painful knee osteoarthritis. A community-based cohort of middle-aged women. Biomarkers 2015, 20, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Vilím, V.; Vytásek, R.; Olejárová, M.; Machácek, S.; Gatterová, J.; Procházka, B.; Kraus, V.B.; Pavelka, K. Serum cartilage oligomeric matrix protein reflects the presence of clinically diagnosed synovitis in patients with knee osteoarthritis. Osteoarthr. Cartil. 2001, 9, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Saberi Hosnijeh, F.; Siebuhr, A.S.; Uitterlinden, A.G.; Oei, E.H.; Hofman, A.; Karsdal, M.A.; Bierma-Zeinstra, S.M.; Bay-Jensen, A.C.; van Meurs, J.B. Association between biomarkers of tissue inflammation and progression of osteoarthritis: Evidence from the Rotterdam study cohort. Arthritis Res. 2016, 18, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loeser, R.F.; Beavers, D.P.; Bay-Jensen, A.C.; Karsdal, M.A.; Nicklas, B.J.; Guermazi, A.; Hunter, D.J.; Messier, S.P. Effects of dietary weight loss with and without exercise on interstitial matrix turnover and tissue inflammation biomarkers in adults with knee osteoarthritis: The Intensive Diet and Exercise for Arthritis trial (IDEA). Osteoarthr. Cartil. 2017, 25, 1822–1828. [Google Scholar] [CrossRef] [Green Version]
- Arden, N.K.; Cro, S.; Sheard, S.; Dore, C.J.; Bara, A.; Tebbs, S.A.; Hunter, D.J.; James, S.; Cooper, C.; O’Neill, T.W.; et al. The effect of vitamin D supplementation on knee osteoarthritis, the VIDEO study: A randomised controlled trial. Osteoarthr. Cartil. 2016, 24, 1858–1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roemer, F.W.; Kassim Javaid, M.; Guermazi, A.; Thomas, M.; Kiran, A.; Keen, R.; King, L.; Arden, N.K. Anatomical distribution of synovitis in knee osteoarthritis and its association with joint effusion assessed on non-enhanced and contrast-enhanced MRI. Osteoarthr. Cartil. 2010, 18, 1269–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bay-Jensen, A.C.; Wichuk, S.; Byrjalsen, I.; Leeming, D.J.; Morency, N.; Christiansen, C.; Karsdal, M.A.; Maksymowych, W.P. Circulating protein fragments of cartilage and connective tissue degradation are diagnostic and prognostic markers of rheumatoid arthritis and ankylosing spondylitis. PLoS ONE 2013, 8, e54504. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.A.; Parkes, M.J.; Hodgson, R.; Felson, D.T.; O’Neill, T.W.; Arden, N.K. Effect of vitamin D supplementation on synovial tissue volume and subchondral bone marrow lesion volume in symptomatic knee osteoarthritis. BMC Musculoskelet. Disord. 2019, 20, 76. [Google Scholar] [CrossRef]
- Roemer, F.W.; Felson, D.T.; Yang, T.; Niu, J.; Crema, M.D.; Englund, M.; Nevitt, M.C.; Zhang, Y.; Lynch, J.A.; El Khoury, G.Y.; et al. The association between meniscal damage of the posterior horns and localized posterior synovitis detected on T1-weighted contrast-enhanced MRI--the MOST study. Semin. Arthritis Rheum. 2013, 42, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballegaard, C.; Riis, R.G.; Bliddal, H.; Christensen, R.; Henriksen, M.; Bartels, E.M.; Lohmander, L.S.; Hunter, D.J.; Bouert, R.; Boesen, M. Knee pain and inflammation in the infrapatellar fat pad estimated by conventional and dynamic contrast-enhanced magnetic resonance imaging in obese patients with osteoarthritis: A cross-sectional study. Osteoarthr. Cartil. 2014, 22, 933–940. [Google Scholar] [CrossRef] [Green Version]
- Guermazi, A.; Roemer, F.W.; Hayashi, D.; Crema, M.D.; Niu, J.; Zhang, Y.; Marra, M.D.; Katur, A.; Lynch, J.A.; El-Khoury, G.Y.; et al. Assessment of synovitis with contrast-enhanced MRI using a whole-joint semiquantitative scoring system in people with, or at high risk of, knee osteoarthritis: The MOST study. Ann. Rheum. Dis. 2011, 70, 805–811. [Google Scholar] [CrossRef] [Green Version]
- Arendt-Nielsen, L.; Eskehave, T.N.; Egsgaard, L.L.; Petersen, K.K.; Graven-Nielsen, T.; Hoeck, H.C.; Simonsen, O.; Siebuhr, A.S.; Karsdal, M.; Bay-Jensen, A.C. Association between experimental pain biomarkers and serologic markers in patients with different degrees of painful knee osteoarthritis. Arthritis Rheumatol. 2014, 66, 3317–3326. [Google Scholar] [CrossRef] [PubMed]
- Bay-Jensen, A.C.; Bihlet, A.; Byrjalsen, I.; Andersen, J.R.; Riis, B.J.; Christiansen, C.; Michaelis, M.; Guehring, H.; Ladel, C.; Karsdal, M.A. Serum C-reactive protein metabolite (CRPM) is associated with incidence of contralateral knee osteoarthritis. Sci. Rep. 2021, 11, 6583. [Google Scholar] [CrossRef] [PubMed]
- Organ, L.A.; Duggan, A.R.; Oballa, E.; Taggart, S.C.; Simpson, J.K.; Kang’ombe, A.R.; Braybrooke, R.; Molyneaux, P.L.; North, B.; Karkera, Y.; et al. Biomarkers of collagen synthesis predict progression in the PROFILE idiopathic pulmonary fibrosis cohort. Respir. Res. 2019, 20, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, N.; Ikeda, Y.; Ohnuki, T.; Tanaka, N.; Hikita, A.; Mitomi, H.; Mori, T.; Juji, T.; Katsuragawa, Y.; Yamamoto, S.; et al. Regional differences in chondrocyte metabolism in osteoarthritis: A detailed analysis by laser capture microdissection. Arthritis Rheum. 2008, 58, 154–163. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | MRI Imaging (n = 136) | Serum Biomarkers (n = 447) |
|---|---|---|
| Age (years) 1, median (IQR) | 65 (60–70) | 64 (58–69) |
| Sex, n (%) | ||
| Male | 51 (34.23) | 177 (39.60) |
| Female | 98 (65.77) | 270 (60.40) |
| BMI (kg/m2), median (IQR) | 28.32 (26.44–31.97) | 28.73 (25.86–32.30) |
| WOMAC pain score 2, median (IQR) | 28.3 (16.50–45.37) | 29.80 (17.00–44.40) |
| WOMAC function score, median (IQR) | 33.94 (17.18–53.29) | 32.47 (18.94–50.56) |
| Kellgren–Lawrence grade, n (%) | ||
| 1 | 25 (18.38) | 118 (26.40) |
| 2 | 57 (41.91) | 172 (38.48) |
| 3 | 37 (27.21) | 131 (29.31) |
| 4 | 17 (12.50) | 26 (5.82) |
| Total synovitis score (0–33) 3, median (IQR) | 12 (7–16) | 13 (6–16) |
| C3M (ng/mL) 4, median (IQR) | 31.67 (26.47–39.03) | 34.09 (28.36–41.22) |
| CRPM (ng/mL) 4, median (IQR) | 7.70 (6.56–10.66) | 9.35 (7.47–11.75) |
| COMP (ng/mL) 4, median (IQR) | 12.01 (10.08–14.03) | 11.50 (9.54–13.59) |
| Crude | Adjusted 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Coefficient | p | 95% Conf Interval | Coefficient | p | 95% Conf Interval | |||
| Suprapatellar | Mild (n = 35) | 1.371 | 0.783 | −8.454 | 11.197 | 1.447 | 0.767 | −8.187 | 11.082 |
| Moderate and Severe (n = 71) | 0.713 | 0.870 | −7.886 | 9.313 | 1.288 | 0.764 | −7.193 | 9.77 | |
| Infrapatellar | Mild (n = 46) | 4.963 | 0.211 | −2.849 | 12.776 | 4.003 | 0.311 | −3.777 | 11.782 |
| Moderate and Severe (n = 34) | 1.244 | 0.774 | −7.292 | 9.780 | 1.224 | 0.774 | −7.184 | 9.631 | |
| Medial perimeniscal | Mild (n = 54) | 3.860 | 0.343 | −4.158 | 11.877 | 5.217 | 0.192 | −2.653 | 13.086 |
| Moderate and Severe (n = 40) | 8.330 | 0.058 | −0.280 | 16.939 | 9.825 | 0.024 * | 1.325 | 18.324 | |
| Crude | Adjusted 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Coefficient | p | 95% Conf Interval | Coefficient | p | 95% Conf Interval | |||
| Suprapatellar | Mild (n = 35) | 9.926 | 0.068 | −0.74 | 20.592 | 10.072 | 0.047 * | 0.146 | 19.999 |
| Moderate and Severe (n = 71) | 4.012 | 0.397 | −5.323 | 13.347 | 4.653 | 0.294 | −4.086 | 13.391 | |
| Infrapatellar | Mild (n = 46) | 7.919 | 0.068 | −0.586 | 16.424 | 5.758 | 0.161 | −2.327 | 13.843 |
| Moderate and Severe (n = 34) | −0.556 | 0.906 | −9.848 | 8.737 | −0.851 | 0.847 | −9.589 | 7.887 | |
| Medial perimeniscal | Mild (n = 54) | 4.776 | 0.289 | −4.095 | 13.648 | 7.207 | 0.087 | −1.054 | 15.469 |
| Moderate and Severe (n = 40) | 6.343 | 0.190 | −3.184 | 15.869 | 8.320 | 0.067 | −0.603 | 17.244 | |
| Crude | Adjusted 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Coefficient | p | 95% Conf Interval | Coefficient | p | 95% Conf Interval | |||
| C3M | Second quartile | −4.744 | 0.055 | −9.580 | 0.092 | −5.166 | 0.031 * | −9.866 | −0.466 |
| Third quartile | −6.272 | 0.011 * | −11.108 | −1.436 | −6.966 | 0.004 * | −11.671 | −2.261 | |
| Fourth quartile | 0.271 | 0.913 | −4.576 | 5.118 | −1.691 | 0.486 | −6.452 | 3.070 | |
| CRPM | Second quartile | −4.138 | 0.094 | −8.985 | 0.708 | −3.352 | 0.163 | −8.071 | 1.367 |
| Third quartile | −7.338 | 0.003 * | −12.184 | −2.491 | −7.403 | 0.002 * | −12.124 | −2.682 | |
| Fourth quartile | −3.277 | 0.186 | −8.134 | 1.580 | −3.967 | 0.100 | −8.700 | 0.766 | |
| COMP | Second quartile | −1.183 | 0.635 | −6.075 | 3.709 | −1.818 | 0.453 | −6.573 | 2.937 |
| Third quartile | −0.025 | 0.992 | −4.918 | 4.867 | −1.086 | 0.657 | −5.881 | 3.709 | |
| Fourth quartile | 0.609 | 0.807 | −4.295 | 5.512 | −0.724 | 0.768 | −5.539 | 4.091 | |
| Crude | Adjusted 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Coefficient | p | 95% Conf Interval | Coefficient | p | 95% Conf Interval | |||
| C3M | Second quartile | −1.266 | 0.643 | −6.622 | 4.091 | −1.773 | 0.490 | −6.818 | 3.272 |
| Third quartile | −2.970 | 0.276 | −8.326 | 2.387 | −3.846 | 0.135 | −8.896 | 1.205 | |
| Fourth quartile | 1.710 | 0.532 | −3.658 | 7.079 | −1.147 | 0.659 | −6.258 | 3.964 | |
| CRPM | Second quartile | −5.246 | 0.054 | −10.585 | 0.092 | −3.786 | 0.141 | −8.827 | 1.256 |
| Third quartile | −6.285 | 0.021 * | −11.623 | −0.947 | −5.941 | 0.021 * | −10.984 | −0.898 | |
| Fourth quartile | −3.464 | 0.204 | −8.814 | 1.886 | −4.088 | 0.113 | −9.144 | 0.969 | |
| COMP | Second quartile | 0.878 | 0.748 | −4.488 | 6.244 | −0.118 | 0.963 | −5.175 | 4.938 |
| Third quartile | 0.632 | 0.817 | −4.734 | 5.998 | −1.436 | 0.580 | −6.535 | 3.664 | |
| Fourth quartile | 3.186 | 0.245 | −2.193 | 8.564 | 0.713 | 0.784 | −4.408 | 5.834 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, X.; Thudium, C.S.; Bay-Jensen, A.-C.; Karsdal, M.A.; van Santen, J.; Arden, N.K.; Perry, T.A.; Kluzek, S. Association between Markers of Synovial Inflammation, Matrix Turnover and Symptoms in Knee Osteoarthritis: A Cross-Sectional Study. Cells 2021, 10, 1826. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10071826
Yang X, Thudium CS, Bay-Jensen A-C, Karsdal MA, van Santen J, Arden NK, Perry TA, Kluzek S. Association between Markers of Synovial Inflammation, Matrix Turnover and Symptoms in Knee Osteoarthritis: A Cross-Sectional Study. Cells. 2021; 10(7):1826. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10071826
Chicago/Turabian StyleYang, Xiaotian, Christian S. Thudium, Anne-Christine Bay-Jensen, Morten A. Karsdal, James van Santen, Nigel K. Arden, Thomas A. Perry, and Stefan Kluzek. 2021. "Association between Markers of Synovial Inflammation, Matrix Turnover and Symptoms in Knee Osteoarthritis: A Cross-Sectional Study" Cells 10, no. 7: 1826. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10071826