Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Clinical Data: Periodontal Examination and Collection
2.4. Power and Sample Size
2.5. Laboratory Analyses
2.6. Statistical Analysis
3. Results
3.1. Study Participants
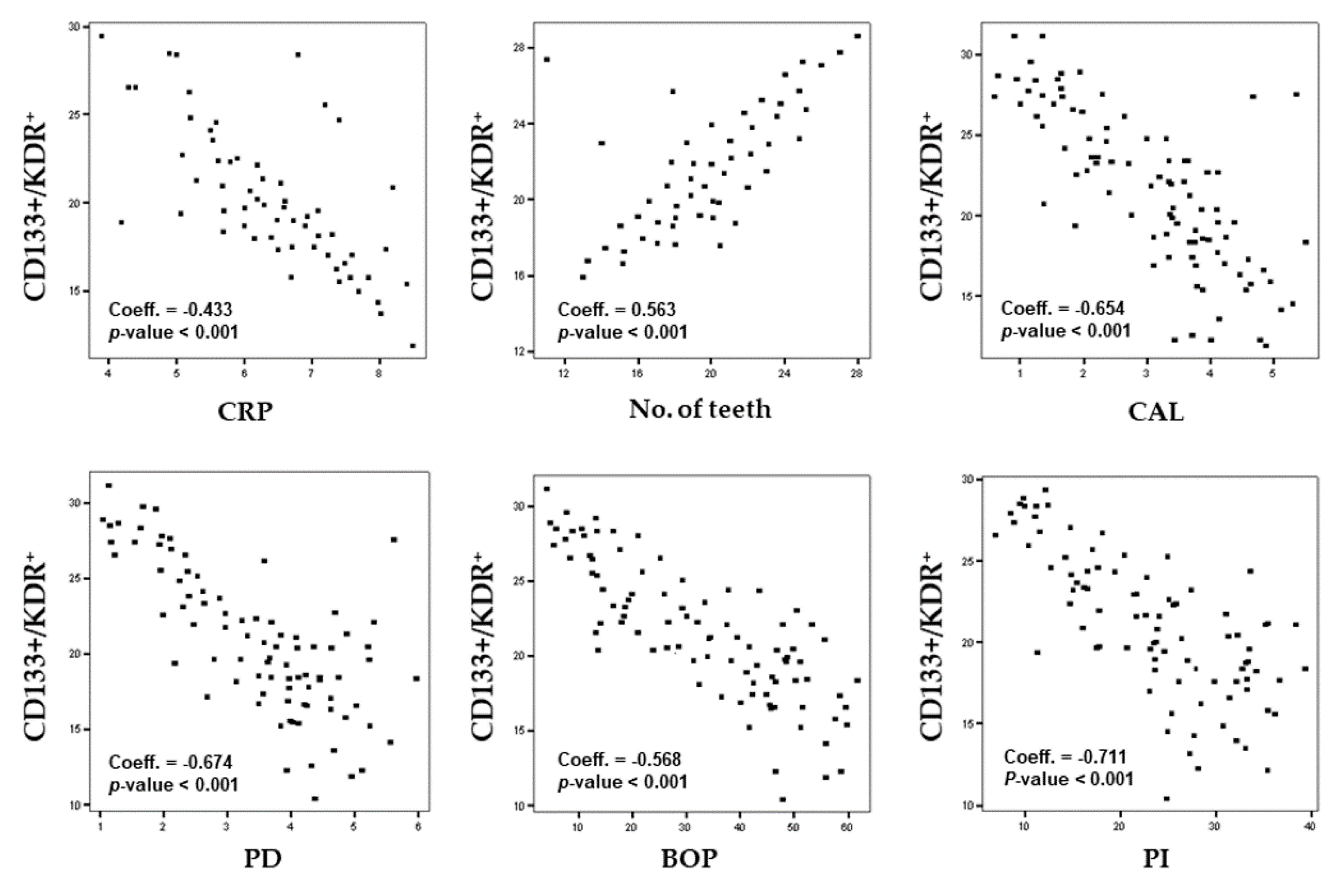
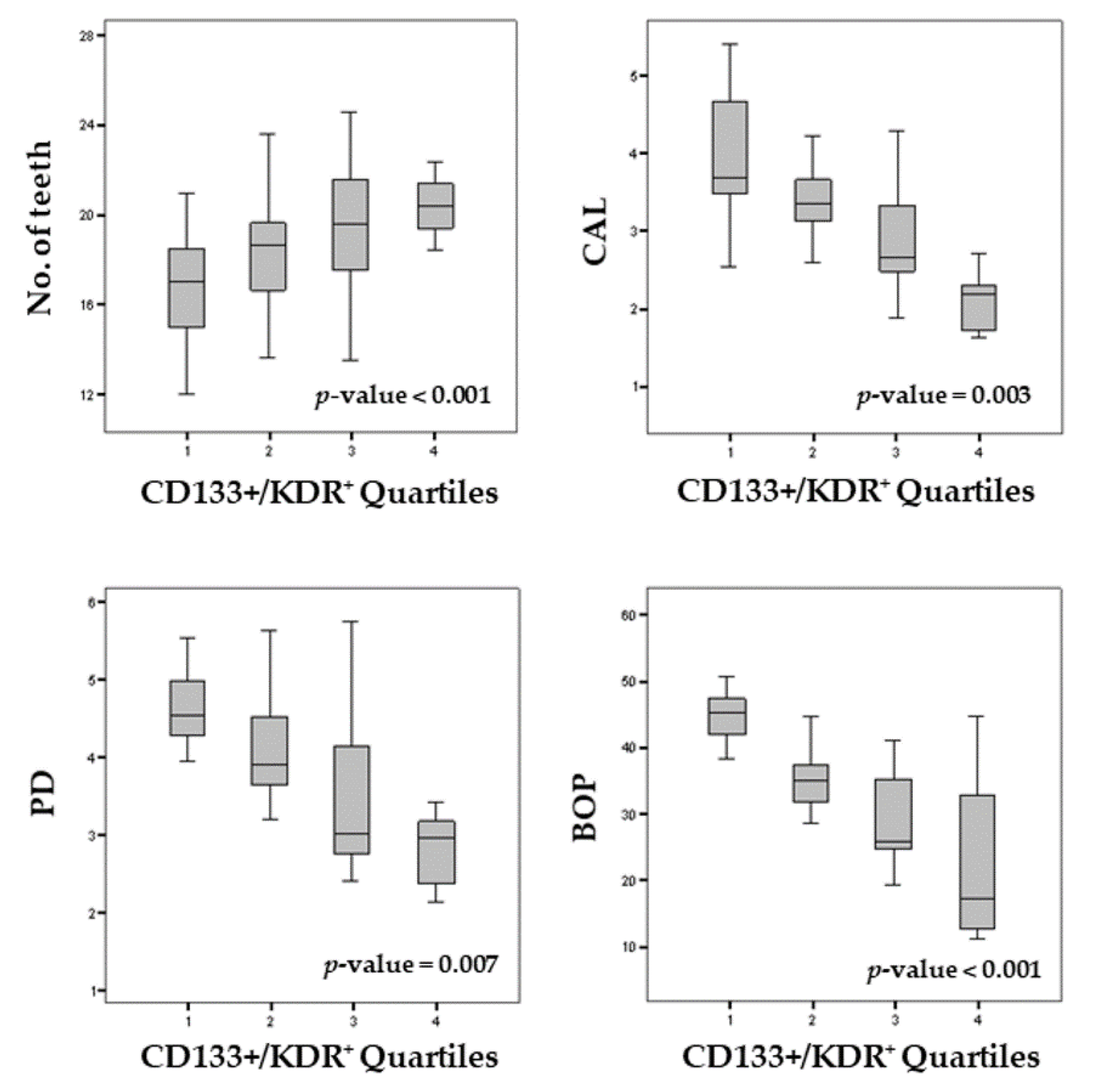
3.2. Periodontal Status and CD133+/KDR+ Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri−Implant Diseases and Conditions. J. Periodontol. 2018, 89, S74–S84. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Ngo, L.Q.; Promsudthi, A.; Surarit, R. Salivary oxidative stress biomarkers in chronic periodontitis and acute coronary syndrome. Clin. Oral Investig. 2017, 21, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedullà, E.; Rapisarda, E.; Iorio−Siciliano, V. Association between periodontitis and glycosylated hemoglobin before diabetes onset: A cross−sectional study. Clin. Oral Investig. 2019. [Google Scholar] [CrossRef] [PubMed]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal Disease: A Risk Factor for Diabetes and Cardiovascular Disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzawa, Y.; Lerman, A. Endothelial dysfunction and coronary artery disease: Assessment, prognosis, and treatment. Coron. Artery Dis. 2014, 25, 713–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gocke, C.; Holtfreter, B.; Meisel, P.; Grotevendt, A.; Jablonowski, L.; Nauck, M.; Markus, M.R.; Kocher, T. Abdominal obesity modifies long−term associations between periodontitis and markers of systemic inflammation. Atherosclerosis 2014, 235, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Garg, U.C.; Hassid, A. Nitric oxide−generating vasodilators and 8−bromo−cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular smooth muscle cells. J. Clin. Investig. 1989, 83, 1774. [Google Scholar] [CrossRef] [Green Version]
- Asahara, T.; Murohara, T.; Sullivan, A.; Silver, M.; van der Zee, R.; Li, T.; Witzenbichler, B.; Schatteman, G.; Isner, J.M. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997, 275, 964–967. [Google Scholar] [CrossRef]
- Hristov, M.; Erl, W.; Weber, P.C. Endothelial progenitor cells: Mobilization, differentiation, and homing. Arterioscler. Thromb. Vasc. Biol. 2003, 223, 1185–1189. [Google Scholar] [CrossRef] [Green Version]
- Fadini, G.P.; de Kreutzenberg, S.V.; Coracina, A.; Baesso, I.; Agostini, C.; Tiengo, A.; Avogaro, A. Circulating CD34+ cells, metabolic syndrome, and cardiovascular risk. Eur. Heart J. 2006, 27, 2247–2255. [Google Scholar] [CrossRef]
- Wojakowski, W.; Kucia, M.; Kazmierski, M.; Ratajczak, M.Z.; Tendera, M. Circulating progenitor cells in stable coronary heart disease and acute coronary syndromes: Relevant reparatory mechanism? Heart 2008, 94, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Kunz, G.A.; Liang, G.; Cuculi, F.; Gregg, D.; Vata, K.C.; Shaw, L.K.; Goldschmidt−Clermont, P.J.; Dong, C.; Taylor, D.A.; Peterson, E.D. Circulating endothelial progenitor cells predict coronary artery disease severity. Am. Heart J. 2006, 152, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M.; Zalos, G.; Halcox, J.P.; Schenke, W.H.; Waclawiw, M.A.; Quyyumi, A.A.; Finkel, T. Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N. Engl. J. Med. 2003, 348, 593–600. [Google Scholar] [CrossRef]
- Jönsson, D.; Spinell, T.; Vrettos, A.; Stoecklin−Wasmer, C.; Celenti, R.; Demmer, R.T.; Kebschull, M.; Papapanou, P.N. Circulating endothelial progenitor cells in periodontitis. J. Periodontol. 2014, 85, 1739–1747. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Tse, H.F.; You, K.H.; Jia, N.; Chen, H.; Li, L.S.; Jin, L. Increased levels of circulating endothelial progenitor cells in subjects with moderate to severe chronic periodontitis. J. Clin. Periodontol. 2009, 36, 933–939. [Google Scholar] [CrossRef]
- Kebschull, M.; Haupt, M.; Jepsen, S.; Deschner, J.; Nickenig, G.; Werner, N. Mobilization of endothelial progenitors by recurrent bacteremias with a periodontal pathogen. PLoS ONE 2013, 8, e54860. [Google Scholar] [CrossRef]
- Li, X.; Tse, H.F.; Jin, L.J. Novel endothelial biomarkers: Implications for periodontal disease and CVD. J. Dent. Res. 2011, 90, 1062–1069. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [Green Version]
- Lindhe, J.; Ranney, R.; Lamster, R.I.; Charles, A.; Chung, C.P.; Flemmig, T.; Kinane, D.; Listgarten, M.; Löe, H.; Schoor, R.; et al. Consensus report: Chronic periodontitis. Ann. Periodontol. 1999, 4, 38. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Iorio−Siciliano, V.; Cordasco, G.; Matarese, G. Efficacy of a drug composed of herbal extracts on postoperative discomfort after surgical removal of impacted mandibular third molar: A randomized, triple−blind, controlled clinical trial. Clin. Oral Investig. 2019, 23, 2443–2453. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Cicciù, M.; Matarese, G. Evaluation of the efficacy of celecoxib and ibuprofen on postoperative pain, swelling, and mouth opening after surgical removal of impacted third molars: A randomized, controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2019, 48, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Lo Giudice, G.; Briguglio, F.; Alibrandi, A.; Crupi, A.; Cordasco, G.; Ramaglia, L. A New Approach for the Treatment of Lateral Periodontal Cysts with an 810−nm Diode Laser. Int. J. Periodontics Restor. Dent. 2017, 37, e120–e129. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Cordasco, G.; Rotondo, F.; Crupi, A.; Ramaglia, L. Anticoagulant therapy in patients undergoing dental interventions: A critical review of the literature and current perspectives. Minerva Stomatol. 2015, 64, 21–46. [Google Scholar] [PubMed]
- Lo Giudice, A.; Barbato, E.; Cosentino, L.; Ferraro, C.M.; Leonardi, R. Alveolar bone changes after rapid maxillary expansion with tooth−born appliances: A systematic review. Eur. J. Orthod. 2018, 40, 296–303. [Google Scholar] [CrossRef]
- Isola, G.; Perillo, L.; Migliorati, M.; Matarese, M.; Dalessandri, D.; Grassia, V.; Alibrandi, A.; Matarese, G. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur. J. Orthod. 2019, 41, 117–124. [Google Scholar] [CrossRef]
- Lau, K.K.; Chan, Y.H.; Yiu, K.H.; Li, S.W.; Tam, S.; Lau, C.P.; Kwong, Y.L.; Tse, H.F. Burden of carotid atherosclerosis in patients with stroke: Relationships with circulating endothelial progenitor cells and hypertension. J. Hum. Hypertens. 2007, 21, 445–451. [Google Scholar] [CrossRef]
- Gurav, A.N. The implication of periodontitis in vascular endothelial dysfunction. Eur. J. Clin. Investig. 2014, 44, 1000–1009. [Google Scholar] [CrossRef] [Green Version]
- Leira, Y.; Rodríguez−Yáñez, M.; Arias, S.; López−Dequidt, I.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis is associated with systemic inflammation and vascular endothelial dysfunction in patients with lacunar infarct. J. Periodontol. 2018. [Google Scholar] [CrossRef]
- Punj, A.; Shenoy, S.B.; Subramanyam, K. Comparison of endothelial function in healthy patients and patients with chronic periodontitis and myocardial infarction. J. Periodontol. 2017, 88, 1234–1243. [Google Scholar] [CrossRef]
- Moura, M.F.; Navarro, T.P.; Silva, T.A.; Cota, L.O.M.; Soares Dutra Oliveira, A.M.; Costa, F.O. Periodontitis and Endothelial Dysfunction: Periodontal Clinical Parameters and Levels of Salivary Markers Interleukin−1β, Tumor Necrosis Factor−α, Matrix Metalloproteinase−2, Tissue Inhibitor of Metalloproteinases−2 Complex, and Nitric Oxide. J. Periodontol. 2017, 88, 778–787. [Google Scholar] [CrossRef]
- Cannavale, R.; Matarese, G.; Isola, G.; Grassia, V.; Perillo, L. Early treatment of an ectopic premolar to prevent molar−premolar transposition. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Piancino, M.G.; Isola, G.; Cannavale, R.; Cutroneo, G.; Vermiglio, G.; Bracco, P.; Anastasi, G.P. From periodontal mechanoreceptors to chewing motor control: A systematic review. Arch. Oral Biol. 2017, 78, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, L.; Li, C.; Xie, H.; Lu, Y.; Wu, Y.; Liu, H. Bone marrow−derived cells homing for self−repair of periodontal tissues: A histological characterization and expression analysis. Int. J. Clin. Exp. Pathol. 2015, 8, 12379. [Google Scholar]
- Pink, C.; Kocher, T.; Meisel, P.; Dörr, M.; Markus, M.R.; Jablonowski, L.; Grotevendt, A.; Nauck, M.; Holtfreter, B. Longitudinal effects of systemic inflammation markers on periodontitis. J. Clin. Periodontol. 2015, 42, 988–997. [Google Scholar] [CrossRef]
- Facciolo, MT.; Riva, F.; Gallenzi, P.; Patini, R.; Gaglioti, D. A rare case of oral multisystem Langerhans cell histiocytosis. J. Clin. Exp. Dent. 2017, 9, e820–e824. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, E.; Ikeda, Y.; Wang, Y.; Fine, N.; Sheikh, Z.; Viniegra, A.; Barzilay, O.; Ganss, B.; Tenenbaum, H.C.; Glogauer, M. Resveratrol derivative−rich melinjo seed extract induces healing in a murine model of established periodontitis. J. Periodontol. 2018, 89, 586–595. [Google Scholar] [CrossRef]
- Pussinen, P.J.; Jauhiainen, M.; Vilkuna−Rautiainen, T.; Sundvall, J.; Vesanen, M.; Mattila, K.; Palosuo, T.; Alfthan, G.; Asikainen, S. Periodontitis decreases the antiatherogenic potency of high density lipoprotein. J. Lipid Res. 2004, 45, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Alibrandi, A.; Currò, M.; Matarese, M.; Ricca, S.; Matarese, G.; Kocher, T. Evaluation of salivary and serum ADMA levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol. 2019. In press. [Google Scholar]
- Isola, G.; Polizzi, A.; Muraglie, S.; Leonardi, R.; Lo Giudice, A. Assessment Of Vitamin C And Antioxidants Profiles In Saliva And Serum On Patients With Periodontitis And Ischemic Heart Disease. Nutrients 2019, 11, 2956. [Google Scholar] [CrossRef] [Green Version]
- Masi, S.; Orlandi, M.; Parkar, M.; Bhowruth, D.; Kingston, I.; O’Rourke, C.; Virdis, A.; Hingorani, A.; Hurel, S.J.; Donos, N.; et al. Mitochondrial oxidative stress, endothelial function and metabolic control in patients with type II diabetes and periodontitis: A randomised controlled clinical trial. Int. J. Cardiol. 2018, 271, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Brito, L.C.; DalBó, S.; Striechen, T.M.; Farias, J.M.; Olchanheski, L.R., Jr.; Mendes, R.T.; Vellosa, J.C.; Fávero, G.M.; Sordi, R.; Assreuy, J.; et al. Experimental periodontitis promotes transient vascular inflammation and endothelial dysfunction. Arch. Oral Biol. 2013, 58, 1187–1198. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Tse, H.F.; You, K.H.; Li, L.S.; Jin, L. Effect of periodontal treatment on circulating CD34(+) cells and peripheral vascular endothelial function: A randomized controlled trial. J. Clin. Periodontol. 2011, 38, 148–156. [Google Scholar] [CrossRef]
- Patini, R.; Staderini, E.; Gallenzi, P. Multidisciplinary surgical management of Cowden syndrome: Report of a case. J. Clin. Exp. Dent. 2016, 18, 472–474. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of periodontitis and endothelial function. N. Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef] [Green Version]
- Ninomiya, M.; Hashimoto, M.; Yamanouchi, K.; Fukumura, Y.; Nagata, T.; Naruishi, K. Relationship of oral conditions to the incidence of infective endocarditis in periodontitis patients with valvular heart disease: A cross−sectional study. Clin. Oral Investig. 2019. [Google Scholar] [CrossRef]
- Elter, J.R.; Hinderliter, A.L.; Offenbacher, S.; Beck, J.D.; Caughey, M.; Brodala, N.; Madianos, P.N. The effects of periodontal therapy on vascular endothelial function: A pilot trial. Am. Heart J. 2006, 151, 47. [Google Scholar] [CrossRef]
- Schulz, S.; Seitter, L.; Werdan, K.; Hofmann, B.; Schaller, H.G.; Schlitt, A.; Reichert, S. Single nucleotide polymorphisms in long noncoding RNA, ANRIL, are not associated with severe periodontitis but with adverse cardiovascular events among patients with cardiovascular disease. J. Periodontal Res. 2018, 53, 714–720. [Google Scholar] [CrossRef]
- Maamoun, H.; Abdelsalam, S.S.; Zeidan, A.; Korashy, H.M.; Agouni, A. A Endoplasmic Reticulum Stress: A Critical Molecular Driver of Endothelial Dysfunction and Cardiovascular Disturbances Associated with Diabetes. Int. J. Mol. Sci. 2019, 20, 1658. [Google Scholar] [CrossRef] [Green Version]
- Otto, M.; Blatt, S.; Pabst, A.; Mandic, R.; Schwarz, J.; Neff, A.; Ziebart, T. Influence of buffy coat−derived putative endothelial progenitor cells on tumor growth and neovascularization in oral squamous cell carcinoma xenografts. Clin. Oral Investig. 2019, 23, 3767–3775. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Ferlito, S. Expression of Salivary and Serum Malondialdehyde and Lipid Profile of Patients with Periodontitis and Coronary Heart Disease. Int. J. Mol. Sci. 2019, 20, 6061. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Alibrandi, A.; Pedullà, E.; Grassia, V.; Ferlito, S.; Perillo, L.; Rapisarda, E. Analysis of the Effectiveness of Lornoxicam and Flurbiprofen on Management of Pain and Sequelae Following Third Molar Surgery: A Randomized, Controlled, Clinical Trial. J. Clin. Med. 2019, 8, 325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matarese, G.; Isola, G.; Ramaglia, L.; Dalessandri, D.; Lucchese, A.; Alibrandi, A.; Fabiano, F.; Cordasco, G. Periodontal biotype: Characteristic, prevalence and dimensions related to dental malocclusion. Minerva Stomatol. 2016, 65, 231–238. [Google Scholar] [PubMed]
- Caccianiga, G.; Paiusco, A.; Perillo, L.; Nucera, R.; Pinsino, A.; Maddalone, M.; Cordasco, G.; Lo Giudice, A. Does low-level laser therapy enhance the efficiency of orthodontic dental alignment? Results from a randomized pilot study. Photomed. Laser Surg. 2017, 35, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Apatzidou, D.A.; Nile, C.; Bakopoulou, A.; Konstantinidis, A.; Lappin, D.F. Stem cell-like populations and immunoregulatory molecules in periodontal granulation tissue. J. Periodontal Res. 2018, 53, 610–621. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Features | Reference Values | Healthy Controls (n = 79) | Periodontitis (n = 88) | p-Value |
|---|---|---|---|---|
| Male, n (%) | 45 (56.9) | 49 (55.6) | 0.126 | |
| Age, mean ± SD | 51.9 ± 5.2 | 52.8 ± 4.1 | 0.076 | |
| Education level | ||||
| Primary school, n (%) | 29 (36.7) | 31 (35.2) | 0.558 | |
| High school, n (%) | 28 (35.4) | 32 (36.3) | 0.641 | |
| College or university, n (%) | 22 (27.8) | 25 (28.4) | 0.589 | |
| BMI, kg/m2, mean ± SD | 24.2 ± 4.1 | 23.9 ± 4.2 | 0.075 | |
| Smoker, n (%) | 17 (21.5) | 19 (21.6) | 0.321 | |
| Current, n (%) | 10 (12.6) | 11 (12.5) | 0.311 | |
| Never, n (%) | 48 (60.7) | 53 (60.2) | 0.158 | |
| Past, n (%) | 4 (5) | 5 (5.6) | 0.233 | |
| Glucose, mg/dL | 65–110 | 96.4 (83.1; 104.5) | 97.9 (91.4; 138.2) | 0.356 |
| HbA1c, mmol/mol | up to 40 | 35.3 (29.6; 38.6) | 36.1 (28.8; 50.2) | 0.078 |
| Uric acid, mg/dL | 1.9–8 | 2 (1.5; 2.6) | 2.9 (1.8; 3.9) | <0.001 |
| Albumin, g/L | 35–50 | 36.9 (32.4; 38.8) | 37.6 (35.2; 41.5) | 0.388 |
| Fibrinogen, mg/dL | 150–400 | 278.5 (221.4; 279.3) | 282.7 (266.4; 318.5) | 0.554 |
| Apolipoprotein A, mg/dL | >120–140 | 130.4 (122.2; 137.6) | 133.6 (129.5; 138.2) | 0.667 |
| Total cholesterol, mg/dL | <200 | 172.3 (154.1: 184.5) | 178.1 (155.1; 185.5) | 0.564 |
| HDL-cholesterol, mg/dL | <40–60 | 50.5 (47.2; 58.1) | 52.9 (47.8; 56.2) | 0.602 |
| LDL-Cholesterol mg/dL | <100–130 | 112.1 (105.5; 122.1) | 118.6 (110.9; 127.2) | 0.555 |
| BUN, mg/dL | 7–30 | 27.6 (25.5; 30.1) | 29.1 (24.5; 30.6) | 0.369 |
| CRP(C-reactive protein), mg/L | <0.8 | 3.3 (2.7; 3.5) | 4.1 (3.5; 4.9) | <0.001 |
| Systolic pressure, mm/hg | 110–130 | 120.5 (112.6; 132.3) | 123.6 (117.1; 134.6) | 0.557 |
| Diastolic pressure, mm/hg | 70–85 | 81.9 (74.5; 85.4) | 83.9 (79.1; 85.5) | 0.058 |
| Ferritin, ng/mL | 12–300 | 77.3 (70.5; 81.4) | 84.2 (73.4; 86.5) | 0.056 |
| Vitamin D, ng/mL | 5–75 | 28.5 (25.7; 35.1) | 27.2 (20.4; 31.2) | 0.114 |
| CD34+/KDR+ EPC (cells/µL) | 162.1 (55.1–289.5) | 141.0 (19.4–896.2) | 0.049 | |
| Low count (no. (%)) | 75 (94.3) | 59 (67) | 0.042 | |
| High count (no. (%)) | 4 (5) | 29 (32.9) | ||
| CD133+/KDR+ EPC (cells/µL) | 79.7 (24.1–156.4) | 66.4 (45.5-169.6) | <0.001 | |
| Low count (no. (%)) | 76 (96.2) | 55 (62.5) | 0.056 | |
| High count (no. (%)) | 3 (3.8) | 33 (37.5) |
| Periodontal Parameters | Healthy Controls (n = 79) | Periodontitis (n = 88) | p-Value |
|---|---|---|---|
| Number of teeth, no., mean ± SD | 24.8 ± 1.6 | 16.5 ± 1.4 | <0.001 |
| CAL, mm, mean ± SD | 1.52 ± 0.8 | 3.91 ± 0.5 | <0.001 |
| % of sites with CAL 4 to 5 mm, ± SD | − | 38.4 ± 3.4 | <0.001 |
| % of sites with CAL ≥6 mm, ± SD | − | 21.2 ± 2.5 | <0.001 |
| PD, mm, mean ± SD | 1.52 ± 1.3 | 4.61 ± 0.7 | <0.001 |
| % of sites with PD 4 to 5 mm, ± SD | − | 44.7 ± 4.4 | <0.001 |
| % of sites with PD ≥6 mm, ± SD | − | 23.4 ± 4.4 | <0.001 |
| BOP, mean % ± SD | 9.2 ± 9.7 | 45.7 ± 3.1 | <0.001 |
| Plaque index (PI), mean ± SD | 0.71 ± 0.3 | 0.86 ± 0.5 | 0.511 |
| Number of Teeth | CAL | |||||
| Variables | Coeff. | 95% CI | p-Value | Coeff. | 95% CI | p-Value |
| Age | −0.15 | −0.24; −0.04 | 0.016 | 0.03 | 0.02; 0.65 | 0.026 |
| Gender | 1.62 | 0.48; 2.81 | 0.009 | − | − | n.s. |
| CD133+/KDR+ | 0.34 | 0.16; 0.41 | <0.001 | −0.11 | −0.14; −0.65 | <0.001 |
| CRP | −2.49 | −3.17; −1.81 | <0.001 | 0.46 | 0.25; 0.59 | <0.001 |
| HDL-Cholesterol | 0.01 | 0.01 | 0.028 | − | − | n.s. |
| PD | BOP | |||||
| Variables | Coeff. | 95% CI | p-value | Coeff. | 95% CI | p-value |
| Age | 0.03 | −0.02; 0.79 | 0.061 | 0.74 | 0.22; 1.36 | 0.129 |
| CD133+/KDR+ | −0.09 | −0.14; −0.49 | <0.001 | −1.69 | −2.25; −1.17 | <0.001 |
| CRP | 0.42 | 0.23; 0.65 | <0.001 | 8.48 | 5.37; 10.45 | <0.001 |
| HDL-Cholesterol | −0.12 | −0.02; 0.28 | 0.074 | − | − | n.s. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isola, G.; Giudice, A.L.; Polizzi, A.; Alibrandi, A.; Patini, R.; Ferlito, S. Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study. Genes 2019, 10, 1022. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10121022
Isola G, Giudice AL, Polizzi A, Alibrandi A, Patini R, Ferlito S. Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study. Genes. 2019; 10(12):1022. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10121022
Chicago/Turabian StyleIsola, Gaetano, Antonino Lo Giudice, Alessandro Polizzi, Angela Alibrandi, Romeo Patini, and Sebastiano Ferlito. 2019. "Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study" Genes 10, no. 12: 1022. https://0-doi-org.brum.beds.ac.uk/10.3390/genes10121022