Analytical Sensitivity and Specificity of Two RT-qPCR Protocols for SARS-CoV-2 Detection Performed in an Automated Workflow

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Primary Samples Collection and Processing
2.2. Nucleic Acid Extraction
2.3. SARS-CoV-2 Assays Evaluated
2.4. One-Step RT-qPCR Reaction and Thermocycling Conditions
2.5. SARS-CoV-2 Diagnostic Synthetic Sequence Production
2.6. Artificial Process Control Production
2.7. Amplification Efficiency
2.8. Determining Limit of Detection of Assays
2.9. Cross-Reaction
2.10. On-Going Test Accuracy Evaluation and Analysis of SARS-CoV-2 Laboratory Test Results Database
2.11. Ethical Considerations
3. Results
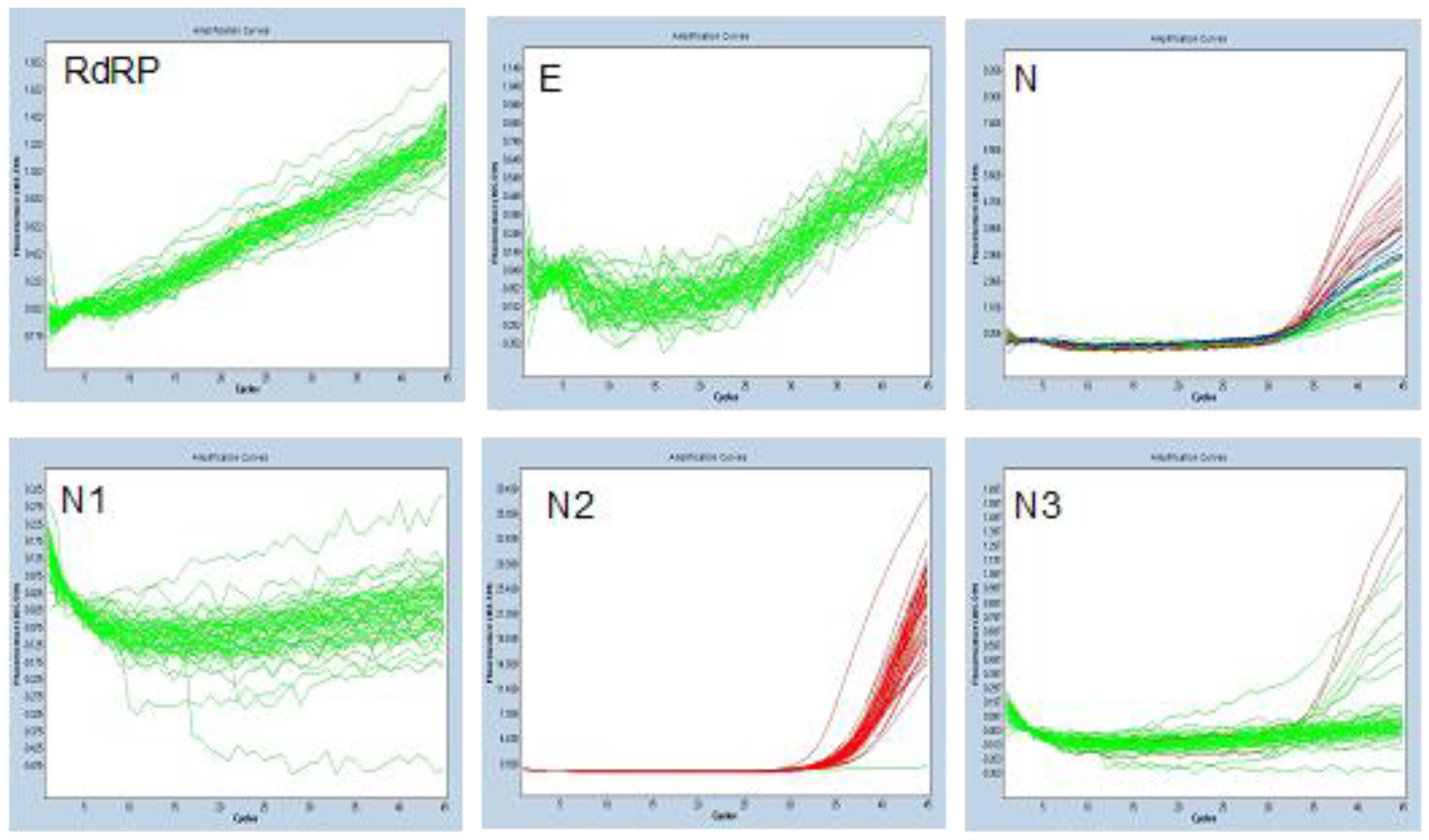
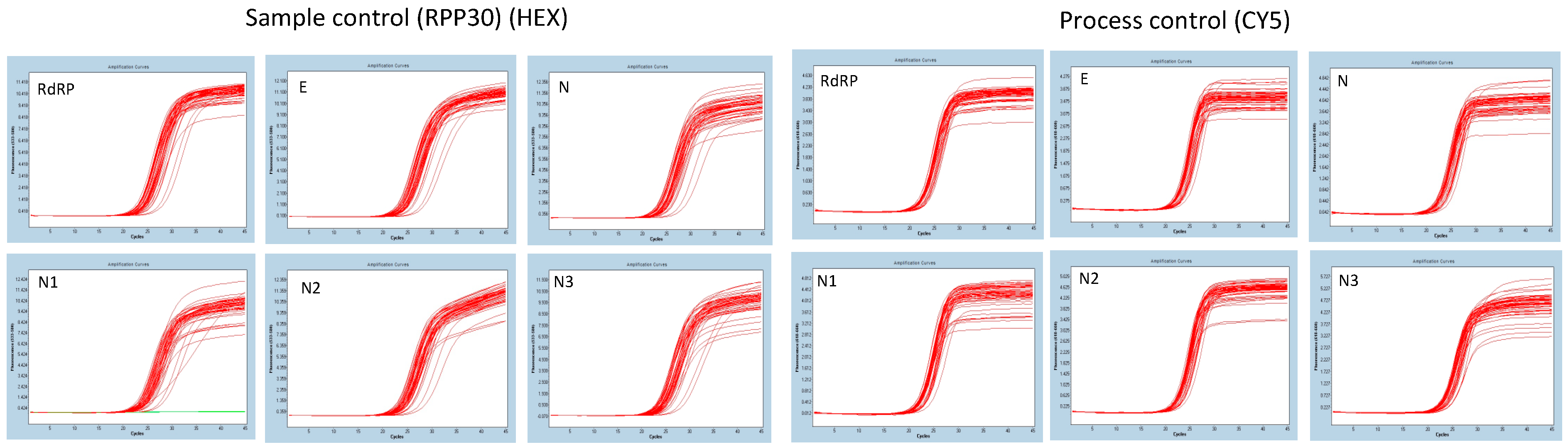
3.1. Analytical Specificity
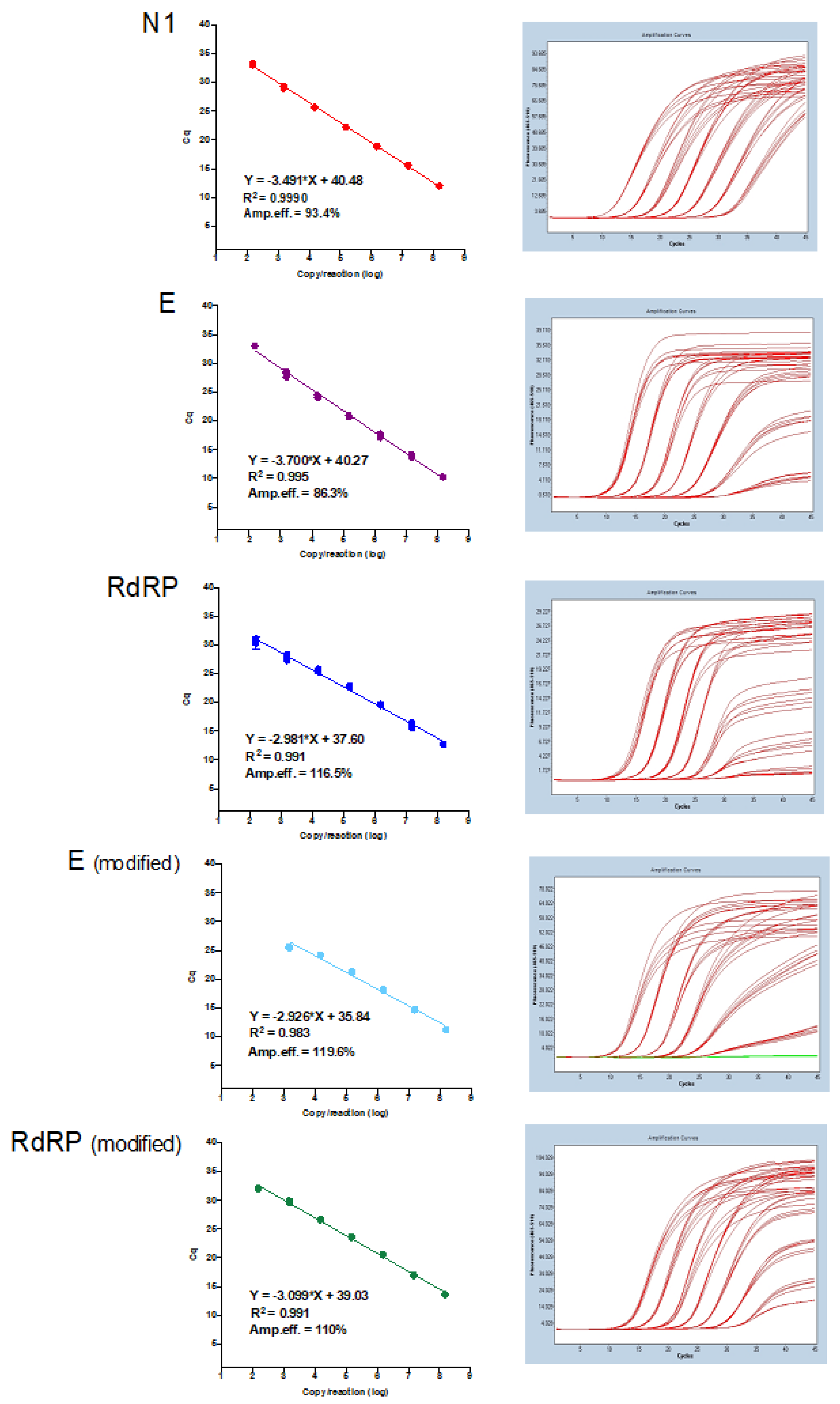
3.2. Amplification Efficiencies
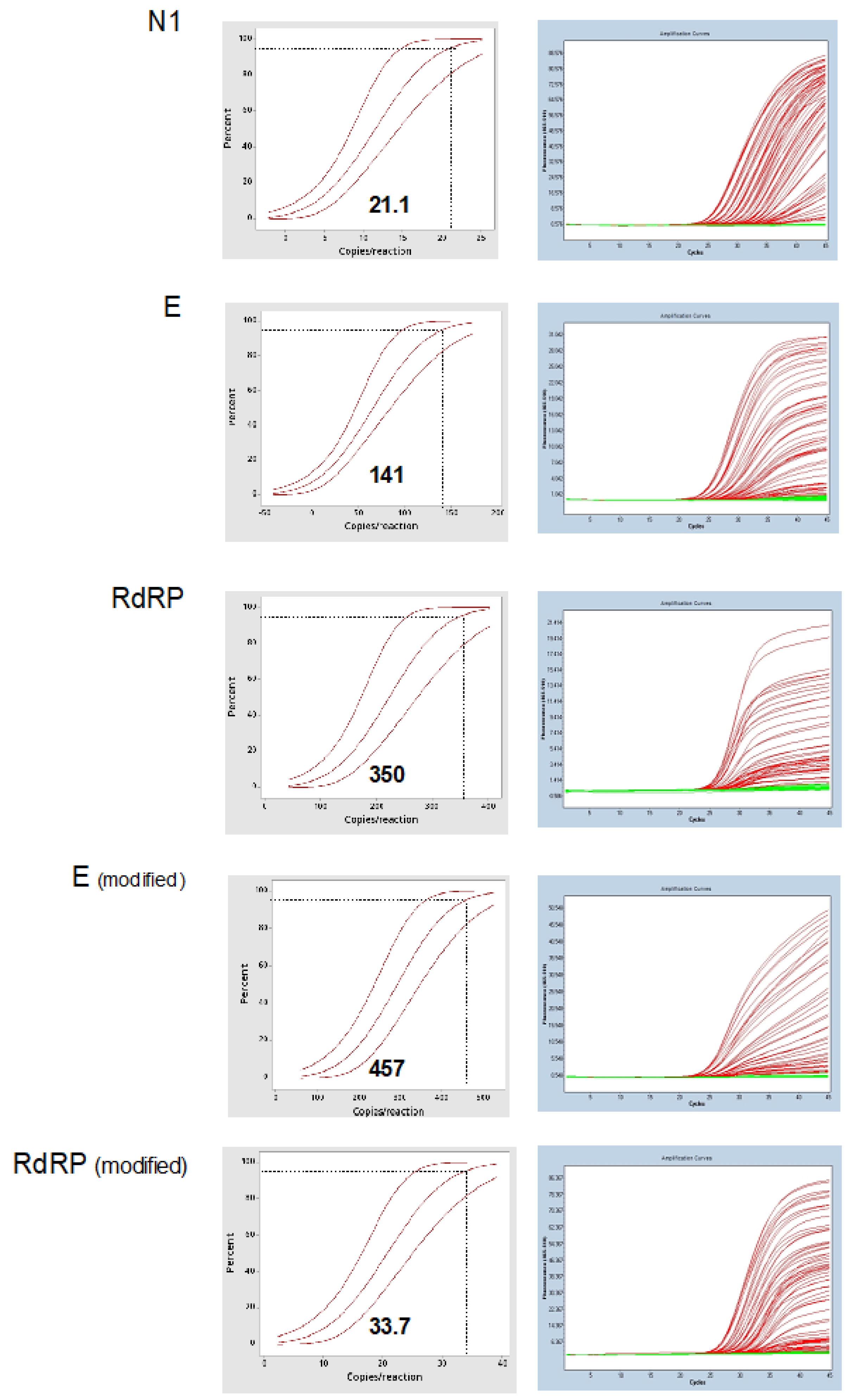
3.3. Limit of Detection
3.4. Cross-Reaction
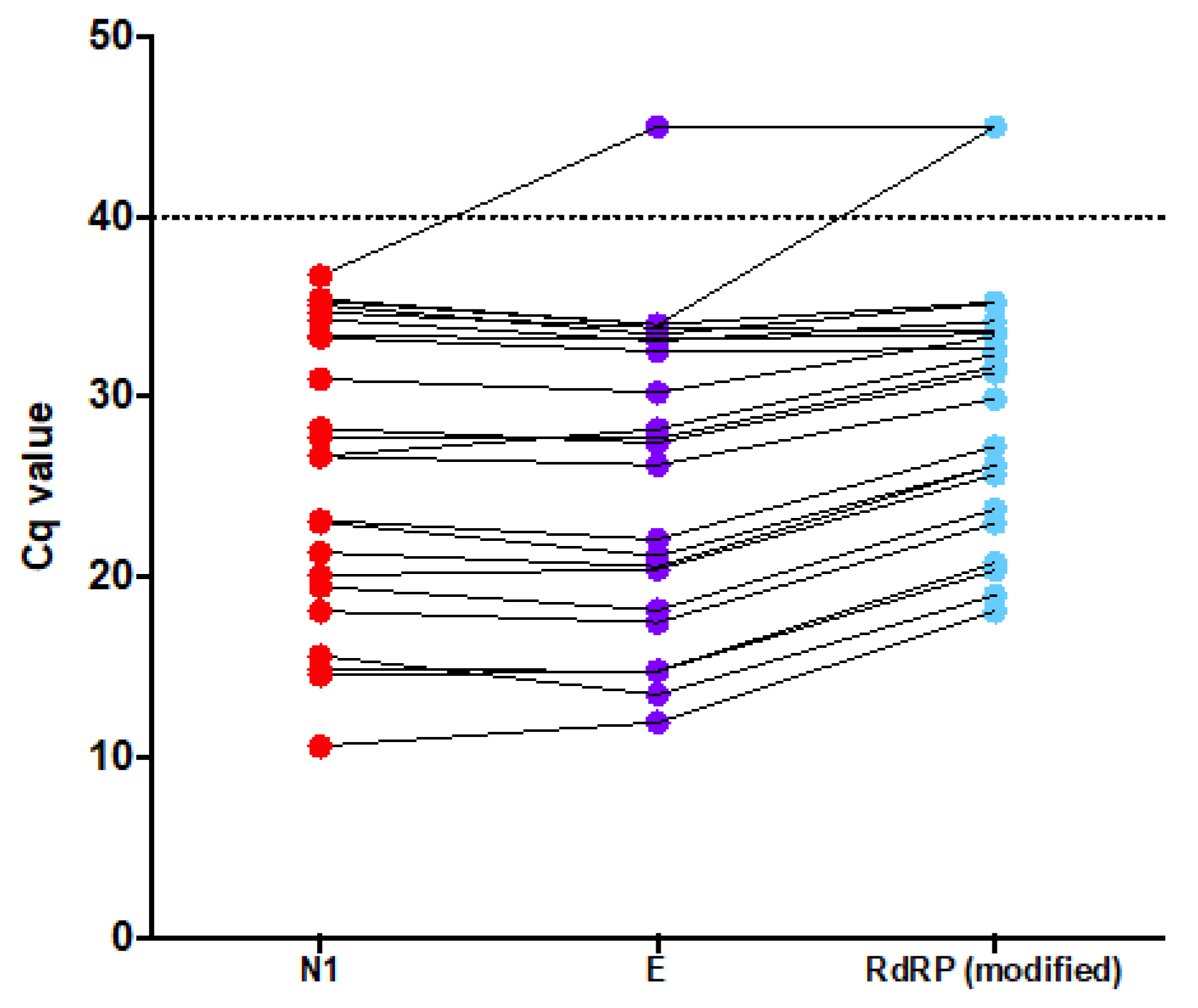
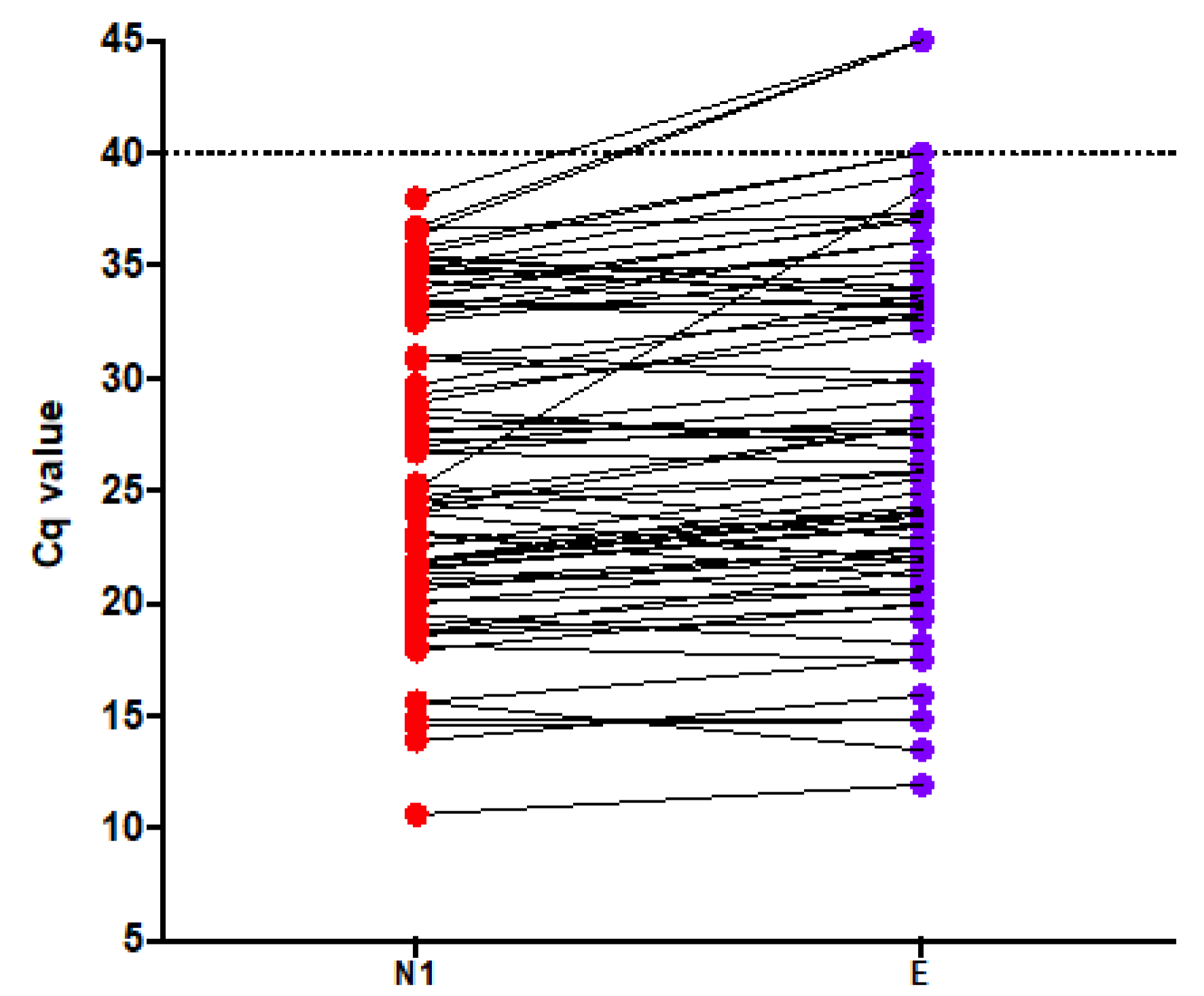
3.5. On-Going Test Accuracy Evaluation
3.6. Analysis of SARS-CoV-2 Laboratory Test Results Database
3.7. Results Summary
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (sars-cov-2) and coronavirus disease-2019 (covid-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. Who declares covid-19 a pandemic. Acta Bio Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar]
- World Health Organization. World Experts and Funders Set Priorities for Covid-19 Research. Available online: https://http://www.who.int/news-room/detail/12-02-2020-world-experts-and-funders-set-priorities-for-covid-19-research (accessed on 18 February 2020).
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-ncov) by real-time rt-pcr. Eurosurveill. Bull. Eur. Mal. Transmissibles Eur. Commun. Dis. Bull. 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Coronavirus Disease (Covid-19) Technical Guidance: Laboratory Testing for 2019-Ncov in Humans. Available online: https://http://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance (accessed on 18 February 2020).
- Centers for Disease Control and Prevention. 2019-Novel Coronavirus (2019-ncov) Real-Time rrt-pcr Panel. Primers and Probes. Available online: https://http://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html (accessed on 21 June 2020).
- Lippi, G.; Simundic, A.M.; Plebani, M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (covid-19). Clin. Chem. Lab. Med. 2020, 58, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Cdc 2019-Novel Coronavirus (2019-ncov) Real-Time rt-pcr Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 21 June 2020).
- Food and Drug Administration. Policy for Coronavirus Disease-2019 Tests during the Public Health Emergency. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/policy-coronavirus-disease-2019-tests-during-public-health-emergency-revised (accessed on 21 June 2020).
- Pfefferle, S.; Reucher, S.; Norz, D.; Lutgehetmann, M. Evaluation of a quantitative rt-pcr assay for the detection of the emerging coronavirus sars-cov-2 using a high throughput system. Eurosurveill. Bull. Eur. Mal. Transm. Eur. Commun. Dis. Bull. 2020, 25, 2000152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravchenko, A.V.; Chetverina, E.V.; Chetverin, A.B. Retention of nucleic acid integrity in guanidine thiocyanate lysates of whole blood. Bioorganicheskaia Khimiia 2006, 32, 609–614. [Google Scholar] [PubMed]
- Tang, Y.W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory diagnosis of covid-19: Current issues and challenges. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, S.R.; Davies, K.A.; Buczkowski, H.; Hettiarachchi, N.; Green, N.; Arnold, U.; Jones, M.; Hannah, M.J.; Evans, R.; Burton, C.; et al. Inactivation analysis of sars-cov-2 by specimen transport media, nucleic acid extraction reagents, detergents and fixatives. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Blow, J.A.; Dohm, D.J.; Negley, D.L.; Mores, C.N. Virus inactivation by nucleic acid extraction reagents. J. Virol. Methods 2004, 119, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Wang, L.; Sakthivel, S.K.; Whitaker, B.; Murray, J.; Kamili, S.; Lynch, B.; Malapati, L.; Burke, S.A.; Harcourt, J.; et al. Us cdc real-time reverse transcription pcr panel for detection of severe acute respiratory syndrome coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1654. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Murcia, A.; Bru, G.; Navarro, A.; RosTárraga, P.; García Sirera, A.; Pérez, L. In silico analysis of rt-qpcr designs recommended by who for detection of 2 sars-cov-2 and a commercial kit validated following une/en iso 17025:2005 and 3 two reference laboratories. BioRxiv 2020. [Google Scholar] [CrossRef]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The miqe guidelines: Minimum information for publication of quantitative real-time pcr experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruijter, J.M.; Ramakers, C.; Hoogaars, W.M.; Karlen, Y.; Bakker, O.; van den Hoff, M.J.; Moorman, A.F. Amplification efficiency: Linking baseline and bias in the analysis of quantitative pcr data. Nucleic Acids Res. 2009, 37, e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.Y.T.; Buckley, C.; Bletchly, C.; Harris, P.; Whiley, D. Contamination of sars-cov-2 rt-pcr probes at the oligonucleotide manufacturer. Pathology 2020. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, J.Y.; Yang, J.S.; Kim, J.W.; Kim, V.N.; Chang, H. The architecture of sars-cov-2 transcriptome. Cell 2020, 181, 914–921.e10. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.D.; Williamson, M.K.; Lewis, S.; Shoemark, D.; Carroll, M.W.; Heesom, K.J.; Zambon, M.; Ellis, J.; Lewis, P.A.; Hiscox, J.A.; et al. Characterisation of the transcriptome and proteome of sars-cov-2 reveals a cell passage induced in-frame deletion of the furin-like cleavage site from the spike glycoprotein. Genome Med. 2020, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Ulferts, R.; Imbert, I.; Canard, B.; Ziebuhr, J. Expression and functions of sars coronavirus replicative proteins. Molecular biology of the sars-coronavirus. In Molecular Biology of the SARS-Coronavirus; Springer: Berlin/Heidelberg, Germany, 2009; pp. 75–98. [Google Scholar]
- Pan American Health Organization. Laboratory Guidelines for the Detection and Diagnosis of covid-19 Virus Infection; PAHO/IMS/PHE/COVID-19/20-0038; PAHO: Washington, DC, USA, 2020. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assay | Name | Sequence (5′–3′) | Stock Solution |
|---|---|---|---|
| E | Primer F | ACAGGTACGTTAATAGTTAATAGCGT | 4 μM (E) or 15 μM (E modified) |
| E | Primer R | ATATTGCAGCAGTACGCACACA | 4 μM (E) or 15 μM (E modified) |
| E | Probe | FAM-ACACTAGCC/ZEN/ATCCTTACTGCGCTTCG-ABkFQ | 2 μM (E) or 3.75 μM (E modified) |
| RdRP | Primer F | GTGARATGGTCATGTGTGGCGG | 6 μM (RdRP) or 15 μM (RdRP modified) |
| RdRP | Primer R | CARATGTTAAASACACTATTAGCATA | 8 μM (RdRP) or 1 5 μM (RdRP modified) |
| RdRP | Probe 1 | FAM-CCAGGTGGW/ZEN/ACRTCATCMGGTGATGC-ABkFQ | 1 μM (RdRP) or 3.75 μM (RdRP modified) |
| RdRP | Probe 2 | FAM-CAGGTGGAA/ZEN/CCTCATCAGGAGATGC-ABkFQ | 1 μM (RdRP) or 3.75 μM (RdRP modified) |
| N | Primer F | CACATTGGCACCCGCAATC | 6 μM |
| N | Primer R | GAGGAACGAGAAGAGGCTTG | 8 μM |
| N | Probe | FAM-ACTTCCTCA/ZEN/AGGAACAACATTGCCA-ABkFQ | 2 μM |
| Assay | Name | Sequence (5′–3′) | Stock Solution |
|---|---|---|---|
| N1 | Primer F | GACCCCAAAATCAGCGAAAT | 15 μM |
| N1 | Primer R | TCTGGTTACTGCCAGTTGAATCTG | 15 μM |
| N1 | Probe | FAM-ACCCCGCAT/ZEN/TACGTTTGGTGGACC-ABkFQ | 3.75 μM |
| N2 | Primer F | TTACAAACATTGGCCGCAAA | 15 μM |
| N2 | Primer R | GCGCGACATTCCGAAGAA | 15 μM |
| N2 | Probe | FAM-ACAATTTGC/ZEN/CCCCAGCGCTTCAG-ABkFQ | 3.75 μM |
| N3 | Primer F | GGGAGCCTTGAATACACCAAAA | 15 μM |
| N3 | Primer R | TGTAGCACGATTGCAGCATTG | 15 μM |
| N3 | Probe | FAM-AYCACATTG/ZEN/GCACCCGCAATCCTG-ABkFQ | 3.75 μM |
| Assay | Name | Sequence (5′–3′) | Stock Solution |
|---|---|---|---|
| RPP30 | Primer F | AGATTTGGACCTGCGAGCG | 4 μM |
| RPP30 | Primer R | GAGCGGCTGTCTCCACAAGT | 4 μM |
| RPP30 | Probe | HEX-TTCTGACCT/ZEN/GAAGGCTCTGCGCG-ABkFQ | 2 μM |
| AEC | Primer F | GGGACTTTAAGCCGAGTCAAT | 4 μM |
| AEC | Primer R | TGGTGGATCACAGTTTGTCAG | 4 μM |
| AEC | Probe | Cy5-ACAGAGTTT/TAO/ACCGCATCTTGCCGT-IAbRQSp | 2 μM |
| State | Total (n) | Positive (n and %) |
|---|---|---|
| Acre | 3 | 1 (33.3%) |
| Amazonas | 5964 | 2811 (47.1%) |
| Bahia | 1162 | 102 (8.7%) |
| Ceará | 1 | 0 |
| Distrito Federal | 14488 | 1031 (7.1%) |
| Espirito Santo | 1 | 0 |
| Goiás | 635 | 58 (9.1%) |
| Maranhão | 1 | 0 |
| Minas Gerais | 1459 | 134 (9.1%) |
| Mato Grosso do Sul | 374 | 33 (8.8%) |
| Mato Grosso | 672 | 35 (5.2%) |
| Pará | 1156 | 790 (68.3%) |
| Paraná | 806 | 70 (8.6%) |
| Rio de Janeiro | 15 | 3 (20%) |
| Rio Grande do Norte | 5 | 1 (20%) |
| Rondônia | 2 | 1 (50%) |
| Roraima | 131 | 18 (13.7%) |
| Rio Grande do Sul | 2 | 0 (0) |
| Santa Catarina | 931 | 110 (11.8%) |
| Sergipe | 1 | 0 (0) |
| São Paulo | 2665 | 382 (14.3%) |
| Tocantins | 225 | 16 (7.1%) |
| Assay | Analytical Specificity (False-Positives) | Amplification Efficiencies (%) | Limit of Detection (Copies/Reaction—(95% CI ) | Cross Reaction | Positive Agreement with N1 | Negative Agreement with N1 |
|---|---|---|---|---|---|---|
| E (Charité) | 0 out of 60 | 86.3 | 141 (109–207) | No | 72/75 (96%) | 2117/2120 (99.8%) |
| RdRP (Charité) | 0 out of 60 | 116.5 | 350 (281–508) | No | Excluded # | Excluded # |
| N (Charité) | 60 out of 60 | Excluded * | Excluded * | Excluded * | Excluded * | Excluded * |
| N1 (cdc) | 0 out of 60 | 93.4 | 21 (16.5–31.1) | No | Reference | Reference |
| N2 (cdc) | 60 out of 60 | Excluded * | Excluded * | Excluded * | Excluded * | Excluded * |
| N3 (cdc) | 13 out of 60 | Excluded * | Excluded * | Excluded * | Excluded * | Excluded * |
| E_Modified | 0 out of 60 | 119.6 | 457 (382–598) | No | Excluded # | Excluded # |
| RDRP_modified | 0 out of 60 | 110 | 33.7 (27.6–46.8) | No | 21/23 (91.3%) | 942/945 (99.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barra, G.B.; Santa Rita, T.H.; Mesquita, P.G.; Jácomo, R.H.; Nery, L.F.A. Analytical Sensitivity and Specificity of Two RT-qPCR Protocols for SARS-CoV-2 Detection Performed in an Automated Workflow. Genes 2020, 11, 1183. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11101183
Barra GB, Santa Rita TH, Mesquita PG, Jácomo RH, Nery LFA. Analytical Sensitivity and Specificity of Two RT-qPCR Protocols for SARS-CoV-2 Detection Performed in an Automated Workflow. Genes. 2020; 11(10):1183. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11101183
Chicago/Turabian StyleBarra, Gustavo Barcelos, Ticiane Henriques Santa Rita, Pedro Góes Mesquita, Rafael Henriques Jácomo, and Lídia Freire Abdalla Nery. 2020. "Analytical Sensitivity and Specificity of Two RT-qPCR Protocols for SARS-CoV-2 Detection Performed in an Automated Workflow" Genes 11, no. 10: 1183. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11101183