TLR4 Polymorphism, Nasopharyngeal Bacterial Colonization, and the Development of Childhood Asthma: A Prospective Birth-Cohort Study in Finnish Children

Abstract
:1. Introduction
2. Materials and Methods
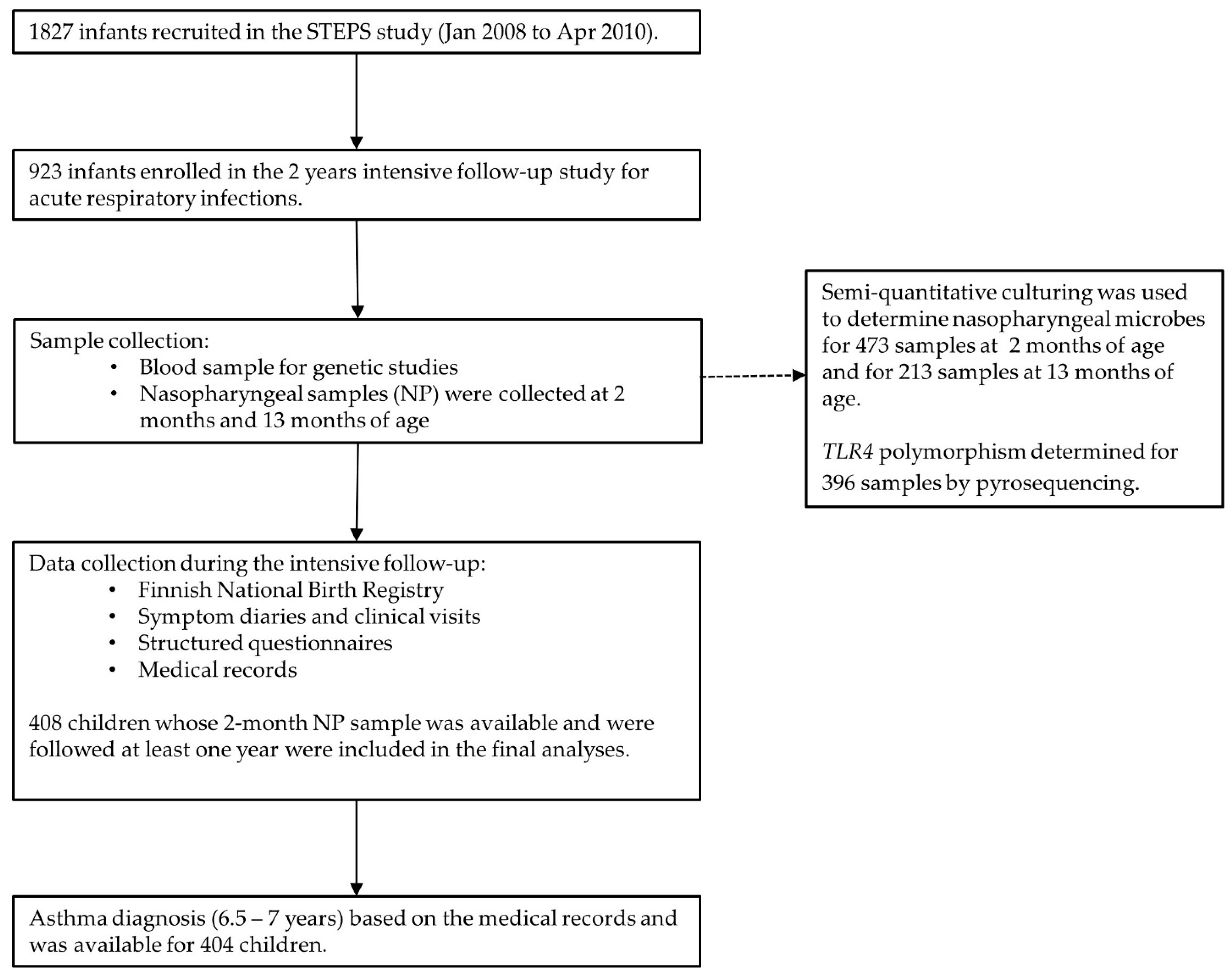
2.1. Study Design and Sample Collection
2.2. Study Subjects, Genetic Analyses, and Bacterial Culture
2.3. Statistical Analysis
3. Results
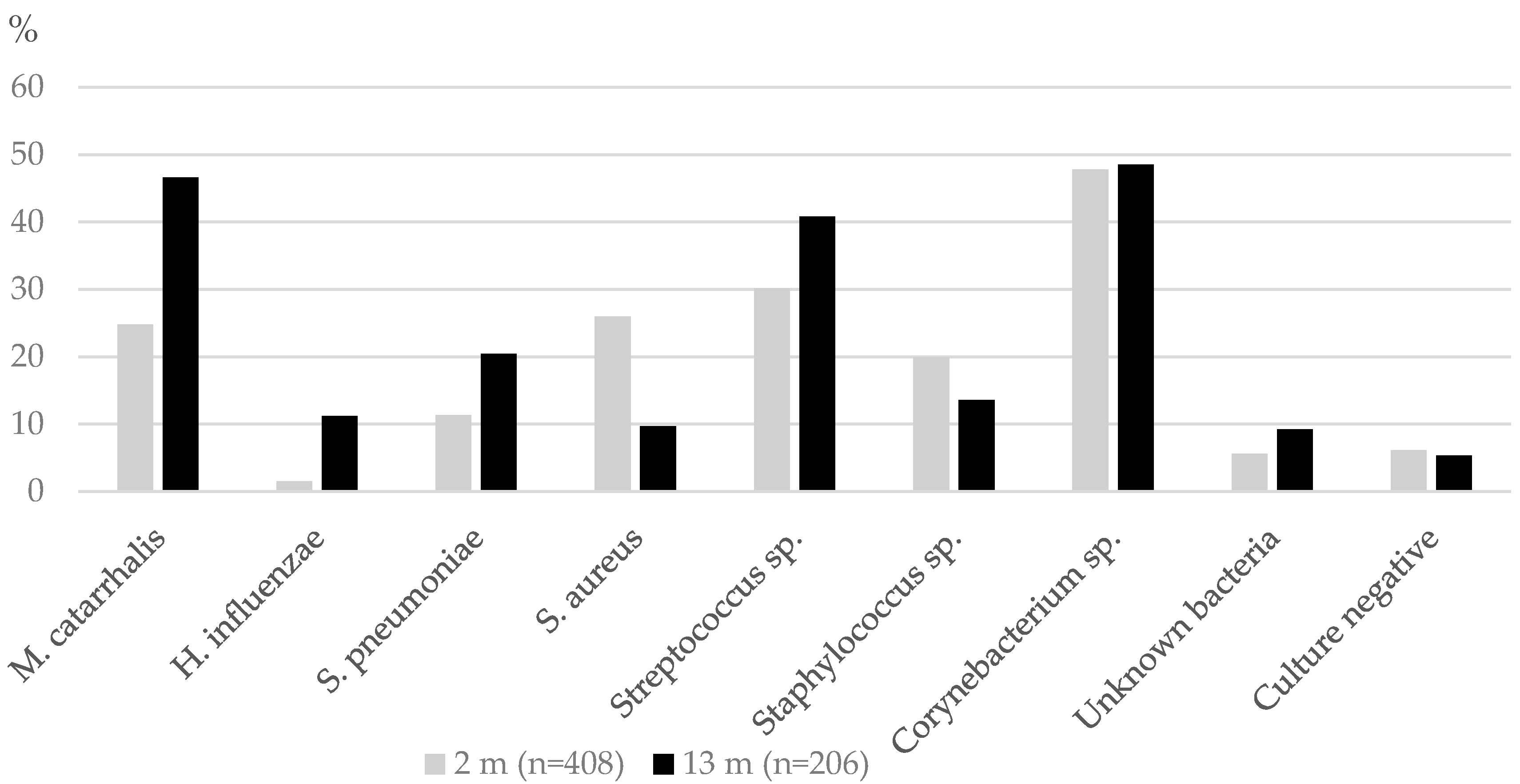
3.1. TLR4 Polymorphisms and Nasopharyngeal Bacterial Colonization
3.2. The impact of TLR4 Polymorphism and Nasopharyngeal Bacteria Colonization to Asthma-Susceptibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bosch, A.A.T.M.; de Steenhuijsen Piters, W.A.A.; van Houten, M.A.; Chu, M.L.J.N.; Biesbroek, G.; Kool, J.; Pernet, P.; de Groot, P.-K.C.M.; Eijkemans, M.J.C.; Keijser, B.J.F.; et al. Maturation of the infant respiratory microbiota, environmental drivers, and health consequences. A prospective cohort study. Am. J. Respir. Crit. Care Med. 2017, 15, 1582–1590. [Google Scholar] [CrossRef]
- Bisgaard, H.; Hermansen, M.N.; Buchvald, F.; Loland, L.; Halkjaer, L.B.; Bønnelykke, K.; Heltberg, A.; Vissing, N.H.; Thorsen, S.V.; Stage, M.; et al. Childhood asthma after bacterial colonization of the airway in neonates. N. Engl. J. Med. 2007, 357, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.M.; Tang, H.H.F.; Mok, D.; Judd, L.M.; Watts, S.C.; Pham, K.; Holt, B.J.; Kuse, M.; Serralha, M.; Troy, N.; et al. Airway microbiota dynamics uncover a critical window for interplay of pathogenic bacteria and allergy in childhood respiratory disease. Cell Host Microbe 2018, 24, 341–352. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, G.; La Grutta, S. The burden of pediatric asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekkanen, J.; Remes, S.T.; Husman, T.; Lindberg, M.; Kajosaari, M.; Koivikko, A.; Soininen, L. Prevalence of asthma symptoms in video and written questionnaires among children in four regions of Finland. Eur. Respir. J. 1997, 10, 1787–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaisho, T.; Akira, S. Toll-like receptor function and signaling. J. Allergy Clin. Immunol. 2006, 117, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Ro, M.J.; Cho, K.J.; Kim, J.H. Lipopolysaccharide/TLR4 Stimulates IL-13 Production through a MyD88-BLT2–Linked Cascade in Mast Cells, Potentially Contributing to the Allergic Response. J. Immunol. 2017, 199, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Ensmble 2020. TLR4 rs4986791 FIN Population Export Location Data. Available online: https://www.ensembl.org/index.html (accessed on 29 June 2020).
- Korppi, M.; Teräsjärvi, J.; Lauhkonen, E.; Huhtala, H.; Nuolivirta, K.; He, Q. Toll-like Receptor 4 Polymorphisms Were Associated With Low Serum Pro-Inflammatory Cytokines in BCG Osteitis Survivors. Acta Paediatr. 2020, 109, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; O’Connor, B.P.; Zemans, R.L.; Zhou, X.; Yang, I.V.; Schwartz, D.A. The Toll-like receptor 4 polymorphism Asp299Gly but not Thr399Ile influences TLR4 signalling and function. PLoS ONE 2014, 9, e93550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagström, H.; Rautava, P.; Kaljonen, A.; Räihä, H.; Pihlaja, P.; Korpilahti, P.; Peltola, V.; Rautakoski, P.; Österbacka, E.; Simell, O.; et al. Cohort profile: Steps to the healthy development and well-being of children (the STEPS Study). Int. J. Epidemiol. 2013, 42, 1273–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuononvirta, J.; Toivonen, L.; Gröndahl-Yli-Hannuksela, K.; Barkoff, A.-M.; Lindholm, L.; Mertsola, J.; Peltola, V.; He, Q. Nasopharyngeal bacterial colonization and gene polymorphisms of mannose-binding lectin and toll-like receptors 2 and 4 in infants. PLoS ONE 2011, 6, e26198. [Google Scholar] [CrossRef] [PubMed]
- Toivonen, L.; Forsström, V.; Waris, M.; Peltola, V. Acute respiratory infections in early childhood and risk of asthma at age 7 years. J. Allergy Clin. Immunol. 2019, 143, 407–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koponen, P.; Vuononvirta, J.; Nuolivirta, K.; Helminen, M.; He, Q.; Korppi, M. The association of genetic variants in toll-like receptor 2 subfamily with allergy and asthma after hospitalization for bronchiolitis in infancy. Pediatr. Infect. Dis. J. 2014, 33, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Pyrosequencing of toll-like receptor polymorphisms of functional relevance. In Methods in Molecular Biology; Ahmad-Nejad, P. (Ed.) Springer: Berlin, Germany, 2009; Volume 496. [Google Scholar]
- Woehrle, T.; Du, W.; Goetz, A.; Hsu, H.-Y.; Joos, T.O.; Weiss, M.; Bauer, U.; Bruecknerd, U.B.; Schneider, E.M. Pathogen specific cytokine release reveals an effect of TLR2 Arg753Gln during candida sepsis in humans. Cytokine 2008, 41, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Roos, A.; Dieltjes, P.; Vossen, R.H.A.M.; Daha, M.R.; de Knijff, P. Detection of three single nucleotide polymorphisms in the gene encoding mannose-binding lectin in a single pyrosequencing reaction. J. Immunol. Methods 2006, 309, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Cleary, D.W.; Clarke, S.C. The nasopharyngeal microbiome. Emerg. Top. Life Sci. 2017, 1, 297–312. [Google Scholar]
- Kumpitsch, C.; Koskinen, K.; Schöpf, V.; Moissl-Eichinger, C. The microbiome of the upper respiratory tract in health and disease. BMC Biol. 2019, 17, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böttcher, M.F.; Hmani-Aifa, M.; Lindström, A.; Jenmalm, M.C.; Mai, X.-M.; Nilsson, L.; Zdolsek, H.A.; Björkstén, B.; Söderkvist, P.; Vaarala, O. A TLR4 Polymorphism Is Associated with Asthma and Reduced Lipopolysaccharide-Induced interleukin-12(p70) Responses in Swedish Children. J. Allergy Clin. Immunol. 2004, 114, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Douville, R.N.; Lissitsyn, Y.; Hirschfeld, A.F.; Becker, A.B.; Kozyrskyj, A.L.; Liem, J.; Bastien, N.; Li, Y.; Victor, R.E.; Sekhon, M.; et al. TLR4 Asp299Gly and Thr399Ile Polymorphisms: No Impact on Human Immune Responsiveness to LPS or Respiratory Syncytial Virus. PLoS ONE 2010, 5, e12087. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | n = 473 (%) |
|---|---|
| Gender | |
| Female | 221 (46.7) |
| Male | 252 (53.3) |
| Mode of Delivery | |
| Vaginal | 402 (85) |
| Caesarean section | 67 (14.2) |
| Missing data | 4 (0.8) |
| Feeding | |
| Exclusive breast feeding | 190 (40.2) |
| Partial breast feeding | 160 (33.8) |
| Formula | 28 (5.9) |
| Missing data | 95 (20.1) |
| Older siblings | 283 (59.8) |
| Missing data | 2 (0.5) |
| Atopy at 13 months of age | 57 (15.1) |
| Missing data | 31 (7.6) |
| Recurrent Wheezing | 48 (12.0) |
| Missing data | 2 (0.5) |
| Parental asthma | 51 (1.6) |
| Missing data | 2 (0.5) |
| Asthma diagnose (6.5–7.5years) | 32 (7.9) |
| Missing data | 4 (1.0) |
| Genotypes | |
| TLR4 (rs4986790) HWE * p = 0.54 | |
| AA | 326 (83) |
| AG | 64 (16) |
| GG | 2 (1) |
| TLR4 Genotype | ||||
|---|---|---|---|---|
| Cultured Bacteria (2 Months) | A/A (n = 252) | A/G or G/G (n = 53) | aOR (95% Cl) † | p value |
| M. catarrhalis | 55 (21.8) | 21 (40.4) | 2.47 (1.25–4.89) | 0.009 * |
| H. influenzae | 5 (2.0) | 0 (0) | - | 0.99 |
| S. pneumoniae | 28 (11.1) | 8 (15.1) | 1.3 (0.52–3.24) | 0.58 |
| S. aureus | 63 (25.0) | 13 (24.5) | 0.99 (0.5–2.00) | 0.99 |
| Streptococcus sp. | 77 (30.6) | 13 (24.5) | 0.77 (0.38–1.53) | 0.45 |
| Staphylococcus sp. | 54 (21.4) | 6 (11.3) | 0.46 (0.19–1.13) | 0.10 |
| Corynebacterium sp. | 121 (48.0) | 23 (43.4) | 0.84 (0.46–1.54) | 0.57 |
| Neisseria sp. | 3 (1.2) | 0 (0.00) | - | 0.99 |
| No cultured bacteria | 14 (5.6) | 3 (5.7) | 1.00 (0.27–3.72) | 0.99 |
| Cultured Bacteria (13 months) | A/A (n = 117) | A/G or A/A (n = 23) | aOR (95% Cl) † | p value |
| M. catarrhalis | 53 (45.3) | 13 (56.5) | 1.82 (0.69–4.80) | 0.23 |
| H. influenzae | 11 (9.4) | 6 (26.1) | 4.18 (1.28–13.63) | 0.018 * |
| S. pneumoniae | 25 (21.4) | 2 (8.7) | 0.33 (0.07–1.55) | 0.16 |
| S. aureus | 12 (10.3) | 1 (4.3) | 0.36 (0.04–3.15) | 0.36 |
| Streptococcus sp. | 41 (35.0) | 12 (52.2) | 2.12 (0.85–5.30) | 0.11 |
| Staphylococcus sp. | 17 (14.5) | 4 (17.4) | 1.22 (0.36–4.16) | 0.75 |
| Corynebacterium sp. | 56 (47.9) | 13 (56.5) | 1.58 (0.63–4.00) | 0.33 |
| Neisseria sp. | 5 (4.3) | 1 (4.3) | 0.96 (0.10–9.25) | 0.97 |
| No cultured bacteria | 6 (5.1) | 1 (4.3) | 0.65 (0.07–6.05) | 0.71 |
| Cultured Bacteria(2 Months) | Number of Children (n = 371) | Number of Children with Asthma at 7 Years of Age § (n = 29) | aOR (95% Cl) ‡,† | pValue |
| M. catarrhalis | Yes, n = 91 | 9 (9.9) | 1.04 (0.4–2.73) | 0.94 |
| No, n = 280 | 20 (7.1) | reference | ||
| H. influenzae | Yes, n = 6 | 2 (33.3) | 2.41 (0.26–22.54) | 0.44 |
| No, n = 365 | 27 (7.4) | reference | ||
| S. pneumoniae | Yes, n = 40 | 4 (10) | 1.10 (0.27–4.39) | 0.90 |
| No, n = 331 | 25 (7.6) | reference | ||
| S. aureus | Yes, n=95 | 9 (9.5) | 0.85 (0.32–2.24) | 0.74 |
| No, n = 276 | 20 (7.2) | reference | ||
| Cultured Bacteria (13 months) | Number of Children (n = 189) | Number of Children with Asthma at 7 years of age § (n = 15) | aOR (95% Cl) † | p value |
| M. catarrhalis | Yes, n = 90 | 9 (10.0) | 1.49 (0.39–5.74) | 0.56 |
| No, n = 99 | 6 (6.1) | reference | ||
| H. influenzae | Yes, n = 22 | 5 (22.7) | 11.56 (2.14–62.45) | 0.004 * |
| No, n = 167 | 10 (6.0) | reference | ||
| S. pneumoniae | Yes, n = 39 | 4 (10) | 2.54 (0.51–12.63) | 0.25 |
| No, n = 150 | 11 (7.3) | reference | ||
| S. aureus | Yes, n = 18 | 4 (22.2) | 4.36 (0.82–23.24) | 0.09 |
| No, n = 171 | 11 (6.4) | reference |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teräsjärvi, J.T.; Toivonen, L.; Vuononvirta, J.; Mertsola, J.; Peltola, V.; He, Q. TLR4 Polymorphism, Nasopharyngeal Bacterial Colonization, and the Development of Childhood Asthma: A Prospective Birth-Cohort Study in Finnish Children. Genes 2020, 11, 768. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11070768
Teräsjärvi JT, Toivonen L, Vuononvirta J, Mertsola J, Peltola V, He Q. TLR4 Polymorphism, Nasopharyngeal Bacterial Colonization, and the Development of Childhood Asthma: A Prospective Birth-Cohort Study in Finnish Children. Genes. 2020; 11(7):768. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11070768
Chicago/Turabian StyleTeräsjärvi, Johanna T., Laura Toivonen, Juho Vuononvirta, Jussi Mertsola, Ville Peltola, and Qiushui He. 2020. "TLR4 Polymorphism, Nasopharyngeal Bacterial Colonization, and the Development of Childhood Asthma: A Prospective Birth-Cohort Study in Finnish Children" Genes 11, no. 7: 768. https://0-doi-org.brum.beds.ac.uk/10.3390/genes11070768