
Heritable Connective Tissue Disorders in Childhood: Increased Fatigue, Pain, Disability and Decreased General Health

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Procedures
2.4. Participant Characteristics
2.5. PROMIS Fatigue Pediatric Self-Report and Parent Proxy
2.6. Childhood Health Assessment Questionnaire (CHAQ), Pain VAS and General Health VAS
2.7. Statistical Analysis
3. Results
3.1. Participants
3.1.1. Fatigue Pediatric self-Report
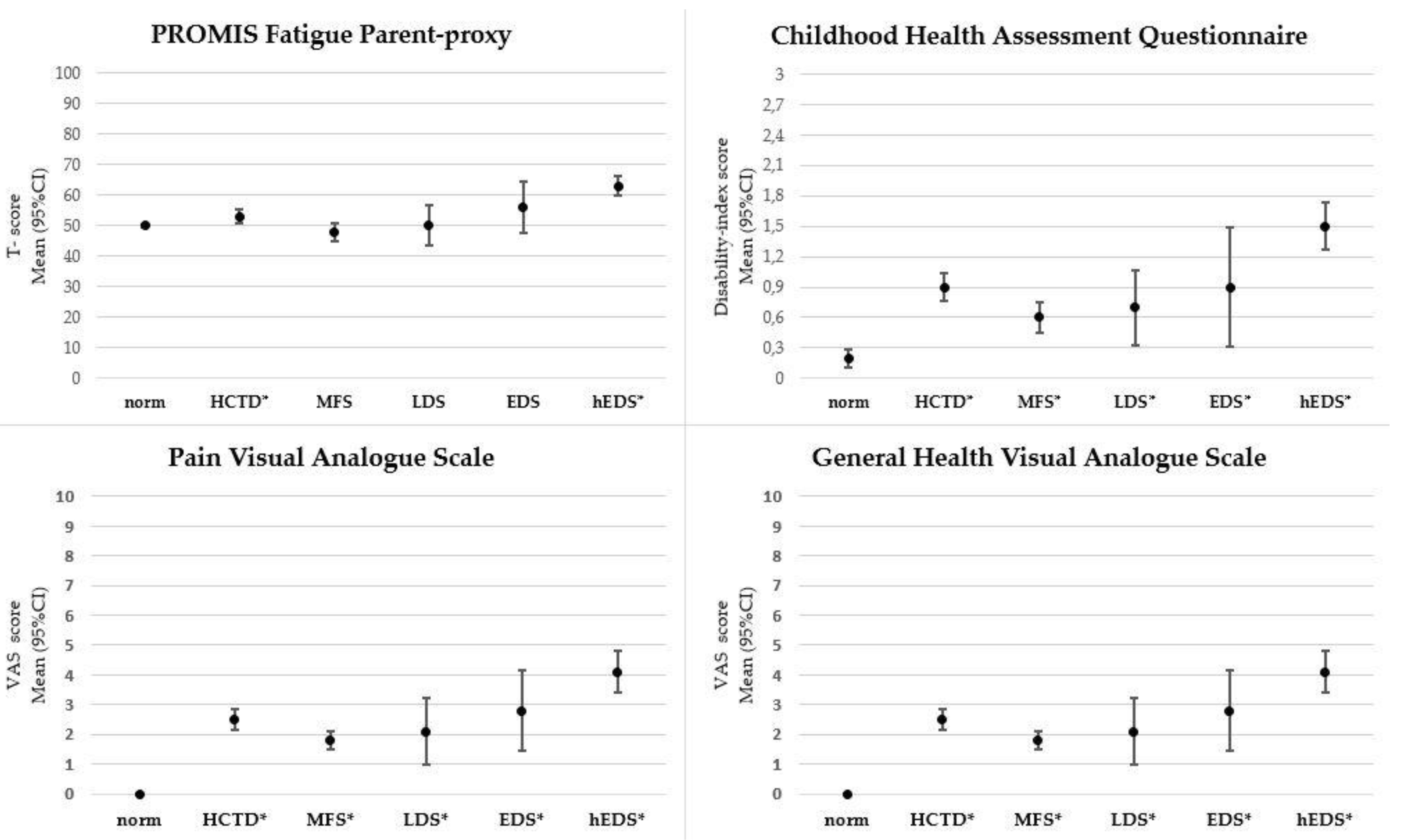
3.1.2. Fatigue Parent-Proxy
3.1.3. Disability
3.1.4. Pain
3.1.5. General Health
3.1.6. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loeys, B.L.; Dietz, H.C.; Braverman, A.C.; Callewaert, B.; De Backer, J.; Devereux, R.B.; Hilhorst-Hofstee, Y.; Jondeau, G.; Faivre, L.; Milewicz, D.M.; et al. The revised Ghent nosology for the Marfan syndrome. J. Med. Genet. 2010, 47, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Loeys, B.L.; Dietz, H.C. Loeys-Dietz Syndrome. In GeneReviews® [Internet]; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wal-lace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993–2021. [Google Scholar]
- Malfait, F.; Francomano, C.; Byers, P.; Belmont, J.; Berglund, B.; Black, J.; Bloom, L.; Bowen, J.M.; Brady, A.F.; Burrows, N.P.; et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 8–26. [Google Scholar] [CrossRef] [Green Version]
- MacCarrick, G.; Black, J.H.; Bowdin, S.; El-Hamamsy, I.; Frischmeyer-Guerrerio, P.A.; Guerrerio, A.L.; Sponseller, P.D.; Loeys, B.; Dietz, H.C. Loeys–Dietz syndrome: A primer for diagnosis and management. Genet. Med. 2014, 16, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Meester, J.A.N.; Verstraeten, A.; Schepers, D.; Alaerts, M.; Van Laer, L.; Loeys, B.L. Differences in manifestations of Marfan syndrome, Ehlers-Danlos syndrome, and Loeys-Dietz syndrome. Ann. Cardiothorac. Surg. 2017, 6, 582–594. [Google Scholar] [CrossRef] [Green Version]
- Van Laer, L.; Dietz, H.; Loeys, B. Loeys-Dietz Syndrome. Adv. Exp. Med. Biol. 2013, 802, 95–105. [Google Scholar] [CrossRef]
- Castori, M.; Tinkle, B.; Levy, H.; Grahame, R.; Malfait, F.; Hakim, A. A framework for the classification of joint hypermobility and related conditions. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 148–157. [Google Scholar] [CrossRef] [Green Version]
- WHO. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Warnink-Kavelaars, J.; Beelen, A.; Goedhart, T.M.H.J.; De Koning, L.E.; Nollet, F.; Alsem, M.W.; Menke, L.A.; Engelbert, R.H.H. Marfan syndrome in adolescence: Adolescents’ perspectives on (physical) functioning, disability, contextual factors and support needs. Eur. J. Nucl. Med. Mol. Imaging 2019, 178, 1883–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnink-Kavelaars, J.; Beelen, A.; Dekker, S.; Nollet, F.; Menke, L.A.; Engelbert, R.H.H. Marfan syndrome in childhood: Parents’ perspectives of the impact on daily functioning of children, parents and family; a qualitative study. BMC Pediatrics 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Tinkle, B.T.; Saal, H.M.; The Committee on Genetics; Saul, R.A.; Braddock, S.R.; Chen, E.; Freedenberg, D.L.; Jones, M.C.; Perrin, J.M.; Tarini, B.A. Health Supervision for Children With Marfan Syndrome. Pediatrics 2013, 132, e1059–e1072. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.B.; Davis, J.G.; Boxer, R.A.; Fisher, M.; Friedman, S.B. Marfan syndrome in adolescents and young adults: Psychosocial functioning and knowledge. J. Dev. Behav. Pediatrics 1990, 11, 122–127. [Google Scholar] [CrossRef]
- Cattalini, M.; Khubchandani, R.; Cimaz, R. When flexibility is not necessarily a virtue: A review of hypermobility syndromes and chronic or recurrent musculoskeletal pain in children. Pediatr. Rheumatol. 2015, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Scheper, M.C.; Juul-Kristensen, B.; Rombaut, L.; Rameckers, E.A.; Verbunt, J.; Engelbert, R.H. Disability in Adolescents and Adults Diagnosed With Hypermobility-Related Disorders: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2016, 97, 2174–2187. [Google Scholar] [CrossRef] [PubMed]
- Lidal, I.B.; Bathen, T.; Johansen, H.; Velvin, G. A scoping review presenting a wide variety of research on paediatric and adolescent patients with Marfan syndrome. Acta Paediatr. 2020, 109, 1758–1771. [Google Scholar] [CrossRef]
- Tinkle, B.; Castori, M.; Berglund, B.; Cohen, H.; Grahame, R.; Kazkaz, H.; Levy, H. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type): Clinical description and natural history. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 48–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Meulenbroek, T.; Huijnen, I.P.; Simons, L.E.; Conijn, A.E.; Engelbert, R.H.; Verbunt, J.A. Exploring the underlying mechanism of pain-related disability in hypermobile adolescents with chronic musculoskeletal pain. Scand. J. Pain 2021, 21, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Mu, W.; Muriello, M.; Clemens, J.L.; Wang, Y.; Smith, C.H.; Tran, P.T.; Rowe, P.C.; Francomano, C.A.; Kline, A.D.; Bodurtha, J. Factors affecting quality of life in children and adolescents with hypermobile Ehlers-Danlos syndrome/hypermobility spectrum disorders. Am. J. Med. Genet. Part A 2019, 179, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Warnink-Kavelaars, J.; Van Oers, H.A.; Haverman, L.; Buizer, A.I.; Alsem, M.W.; Engelbert, R.H.H.; Menke, L.A. Parenting a child with Marfan syndrome: Distress and everyday problems. Am. J. Med. Genet. Part A 2021, 185, 50–59. [Google Scholar] [CrossRef]
- Scheper, M.C.; Nicholson, L.L.; Adams, R.D.; Tofts, L.; Pacey, V. The natural history of children with joint hypermobility syndrome and Ehlers–Danlos hypermobility type: A longitudinal cohort study. Rheumatology 2017, 56, 2073–2083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheper, M.C.; Pacey, V.; Rombaut, L.; Adams, R.D.; Tofts, L.; Calders, P.; Nicholson, L.L.; Engelbert, R.H.H. Generalized Hyperalgesia in Children and Adults Diagnosed With Hypermobility Syndrome and Ehlers-Danlos Syndrome Hypermobility Type: A Discriminative Analysis. Arthritis Rheum. 2016, 69, 421–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erkula, G.; Sponseller, P.D.; Paulsen, L.C.; Oswald, G.L.; Loeys, B.L.; Dietz, H.C. Musculoskeletal Findings of Loeys-Dietz Syndrome. J. Bone Jt. Surg. Am. 2010, 92, 1876–1883. [Google Scholar] [CrossRef] [PubMed]
- Johansen, H.; Velvin, G.; Lidal, I. Adults with Loeys–Dietz syndrome and vascular Ehlers–Danlos syndrome: A cross-sectional study of health burden perspectives. Am. J. Med. Genet. Part A 2019, 182, 137–145. [Google Scholar] [CrossRef]
- Voermans, N.C.; Knoop, H.; Van De Kamp, N.; Hamel, B.C.; Bleijenberg, G.; Van Engelen, B.G. Fatigue Is a Frequent and Clinically Relevant Problem in Ehlers-Danlos Syndrome. Semin. Arthritis Rheum. 2010, 40, 267–274. [Google Scholar] [CrossRef]
- Rombaut, L.; Malfait, F.; Cools, A.; De Paepe, A.; Calders, P. Musculoskeletal complaints, physical activity and health-related quality of life among patients with the Ehlers–Danlos syndrome hypermobility type. Disabil. Rehabil. 2010, 32, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Speed, T.J.; Mathur, V.A.; Hand, M.; Christensen, B.; Sponseller, P.D.; Williams, K.A.; Campbell, C.M. Characterization of pain, disability, and psychological burden in Marfan syndrome. Am. J. Med. Genet. Part A 2017, 173, 315–323. [Google Scholar] [CrossRef]
- Velvin, G.; Bathen, T.; Rand-Hendriksen, S.; Geirdal, A. Østertun Systematic review of chronic pain in persons with Marfan syndrome. Clin. Genet. 2016, 89, 647–658. [Google Scholar] [CrossRef]
- Castori, M.; Morlino, S.; Celletti, C.; Ghibellini, G.; Bruschini, M.; Grammatico, P.; Blundo, C.; Camerota, F. Re-writing the natural history of pain and related symptoms in the joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. Am. J. Med. Genet. Part A 2013, 161, 2989–3004. [Google Scholar] [CrossRef] [PubMed]
- Haverman, L.; Grootenhuis, M.A.; Raat, H.; Van Rossum, M.A.J.; Broeder, E.V.D.-D.; Hoppenbrouwers, K.; Correia, H.; Cella, D.; Roorda, L.D.; Terwee, C.B. Dutch–Flemish translation of nine pediatric item banks from the Patient-Reported Outcomes Measurement Information System (PROMIS)®. Qual. Life Res. 2016, 25, 761–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luijten, M.A.; Terwee, C.B.; van Oers, H.A.; Joosten, M.M.; van den Berg, J.M.; Schonenberg-Meinema, D.; Dolman, K.M.; Ten Cate, R.; Roorda, L.D.; Grootenhuis, M.A.; et al. Psychometric properties of the pediatric Patient-Reported Outcomes Measurement Information System (PROMIS(R)) item banks in a Dutch clinical sample of children with Juvenile Idiopathic Arthritis. Arthritis Care Res. 2019, 72, 1780–1789. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.-S.; Stucky, B.D.; Thissen, D.; Varni, J.W.; DeWitt, E.M.; Irwin, D.E.; Yeatts, K.B.; DeWalt, D.A. Development and psychometric properties of the PROMIS® pediatric fatigue item banks. Qual. Life Res. 2013, 22, 2417–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, G.; Athreya, B.H.; Fries, J.F.; Goldsmith, D.P. Measurement of health status in children with juvenile rheumatoid arthritis. Arthritis Rheum. 1994, 37, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Wulffraat, N.; Van Der Net, J.J.; Ruperto, N.; Kamphuis, S.; Prakken, B.J.; Cate, R.T.; Van Soesbergen, R.M.; Van Rossum, M.A.; Raat, H.; Landgraf, J.M.; et al. The Dutch version of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ). Clin. Exp. Rheumatol. 2001, 19, S111–S115. [Google Scholar]
- Huber, A.M.; Hicks, J.E.; Lachenbruch, P.A.; Perez, M.D.; Zemel, L.S.; Rennebohm, R.M.; Wallace, C.A.; Lindsley, C.B.; Passo, M.H.; Ballinger, S.H.; et al. Validation of the Childhood Health Assessment Questionnaire in the juvenile idiopathic myopathies. Juvenile Dermatomyositis Disease Activity Collaborative Study Group. J. Rheumatol. 2001, 28, 1106–1111. [Google Scholar]
- Dempster, H.; Porepa, M.; Young, N.; Feldman, B.M. The clinical meaning of functional outcome scores in children with juvenile arthritis. Arthritis Rheum. 2001, 44, 1768–1774. [Google Scholar] [CrossRef]
- Field, A.P. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Carmichael, M., Ed.; SAGE: Los Angeles, CA, USA, 2018. [Google Scholar]
- Mann, C.M.; Schanberg, L.E.; Wang, M.; Von Scheven, E.; Lucas, N.; Hernandez, A.; Ringold, S.; Reeve, B.B. Identifying clinically meaningful severity categories for PROMIS pediatric measures of anxiety, mobility, fatigue, and depressive symptoms in juvenile idiopathic arthritis and childhood-onset systemic lupus erythematosus. Qual. Life Res. 2020, 29, 2573–2584. [Google Scholar] [CrossRef]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W.; Schuler, T.C. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Brunner, H.I.; Klein-Gitelman, M.S.; Miller, M.J.; Barron, A.; Baldwin, N.; Trombley, M.; Johnson, A.L.; Kress, A.; Lovell, D.J.; Giannini, E.H. Minimal clinically important differences of the childhood health assessment questionnaire. J. Rheumatol. 2005, 32, 150–161. [Google Scholar] [PubMed]
- Thissen, D.; Liu, Y.; Magnus, B.; Quinn, H.; Gipson, D.S.; Dampier, C.; Huang, I.-C.; Hinds, P.S.; Selewski, D.T.; Reeve, B.B.; et al. Estimating minimally important difference (MID) in PROMIS pediatric measures using the scale-judgment method. Qual. Life Res. 2016, 25, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]


{kind=link}
| Child | HCTD | MFS | LDS | EDS | hEDS | Among HCTD- Subgroups p-Value |
|---|---|---|---|---|---|---|
| n (%) | 107 (100) | 62 (58) | 7 (7) | 9 (8) | 29 (27) | |
| Sex, n (%), Female | 48 (45) | 20 (32) | 5 (71) | 6 (67) | 17 (59) | 0.02 * |
| Age in years, M (SD) | 10.2 (4.0) | 10.1 (4.1) | 11.0 (3.9) | 10.8 (4.8) | 10.0 (3.7) | 0.90 |
| Nationality, n (%) | 0.03 * | |||||
| Dutch | 97 (90) | 56 (90) | 6 (86) | 6 (67) | 29 (100) | |
| Belgium | 10 (10) | 6 (10) | 1 (14) | 3 (33) | 0 (0) | |
| Parent | ||||||
| n (%) | 107 (100) | 62 (58) | 7 (7) | 9 (8) | 29 (27) | |
| Sex, n (%), Female | 86 (80) | 46 (74) | 6 (86) | 7 (78) | 27 (93) | 0.20 |
| Age in years, M (SD) a | 42,5 (7.1) | 43.5 (8.1) | 42.3 (6.3) | 42.6 (4.2) | 40.2 (4.9) | 0.18 |
| Nationality, n (%) | 0.03 * | |||||
| Dutch | 97 (90) | 56 (90) | 6 (86) | 6 (67) | 29 (100) | |
| Belgium | 10 (10) | 6 (10) | 1 (14) | 3 (33) | 0 (0) |
| PROMIS Fatigue Pediatric Self-Report 8–18 Years | HCTD | norm | HCTD vs Norm p-Value | Effect size Cohen’s d/OR(95%CI) | MFS | LDS | EDS | hEDS | Among HCTD-Subgroups p-Value |
|---|---|---|---|---|---|---|---|---|---|
| n (%) | 62 (100) a | 3042 (100) | 36 (58) b | 5 (8) | 6 (10) c | 15 (24) c | |||
| Sex, n (%), Female | 30 (48) | 1578 (52) | 0.6 | 14 (39) | 4 (80) | 4 (67) | 8 (53) | 0.24 | |
| Age-groups, n (%) | 0.08 * | 0.50 | |||||||
| 8–12 years | 26 (42) | 1616 (53) | |||||||
| 13–18 years | 36 (58) | 1426 (47) | |||||||
| T scores, M (SD) | 49 (13) | 50 (10) | 0.44 | 44 (11) | 47 (8) | 52 (19) | 61 (9) | <0.001 * | |
| T score > 70, n (%) | 8 (13) | 213 (7) | 0.07 * | 2.0 (0.94–4.1) | 1 (3) | 0 | 2 (33) | 5 (33) | 0.02 * |
| PROMIS Fatigue Parent proxy 4–18 years | |||||||||
| n (%) | 98 (100) a | 1980 | 57 (58) b | 7 | 9 | 25 (26) c | |||
| T scores, M (SD) | 53 (12) | 50 (10) | 0.004 * | 0.27 | 48 (11) | 50 (9) | 56 (13) | 63 (8) | <0.001 * |
| T score > 70, n (%) | 17 (16) | 138 (7) | <0.001 * | 2.83 (1.63–4.9) | 3 (5) | 0 (0) | 3 (33) | 11 (38) | 0.023 * |
| CHAQ | HCTD | norm | HCTD vs Norm p-Value | Effect Size Cohen’s d | MFS | LDS | EDS | hEDS | Among HCTD-Subgroups p-Value |
|---|---|---|---|---|---|---|---|---|---|
| n (%) | 99 (100) a | 80 | 58 (59) b | 7 (7) | 9 (9) | 25 (25) b | |||
| Sex, n (%) Female | 44 (45) | 33 (41) | 0.59 | 19 (33) | 5 (71) | 6 (67) | 14 (56) | 0.04 | |
| Age in years, M (SD) | 10.1 (4.1) | 8.1 (3.6) | <0.001 * | 0.49 | 10.1 (4.2) | 11.0 (3.9) | 10.8 (4.8) | 9.6 (3.7) | 0.81 |
| Domain scores (0–3) M (SD) | |||||||||
| Dressing | 0.8 (1.0) | 0.5 (0.8) | 0.03 * | 0.33 | 0.6 (.9) | 0.4 (0.8) | 1.0 (0.9) | 1.3 (1.3) | |
| Arising | 0.7 (.8) | 0.1 (0.3) | <0.001 * | 0.99 | 0.4 (.7) | 0.9 (0.9) | 0.7 (0.8) | 1.4 (0.9) | |
| Eating | 1.0 (.9) | 0.4 (0.7) | <0.001 * | 0.74 | 0.7 (.8) | 0.7 (0.8) | 0.9 (0.9) | 1.7 (0.9) | |
| Walking | 0.6 (.9) | 0.0 (0.1) | <0.001 * | 0.94 | 0.3 (.7) | 0.1 (0.4) | 0.6 (0.9) | 1.3 (0.9) | |
| Hygiene | 0.8 (1.0) | 0.3 (0.6) | <0.001 * | 0.60 | 0.5 (.8) | 0.1 (0.4) | 0.8 (0.9) | 1.4 (1.1) | |
| Reach | 0.9 (.8) | 0.2 (0.5) | <0.001 * | 1.0 | 0.5 (.8) | 0.9 (0.7) | 0.9 (0.9) | 1.5 (0.6) | |
| Grip | 1.1 (.9) | 0.2 (0.6) | <0.001 * | 1.18 | 0.8 (.8) | 1.1 (0.9) | 1.1 (1.1) | 1.7 (0.9) | |
| Activity | 1.1 (1.0) | 0.2 (0.5) | <0.001 * | 1.14 | 0.7 (.8) | 1.1 (0.7) | 1.4 (1.2) | 1.9 (0.7) | |
| CHAQ-DI scores (0–3) | |||||||||
| M (SD); median (IQR) | 0.9 (0.7); 0.6 (1.1) | 0.2 (0.4) | <0.001 * | 1.23 | 0.6 (0.6); 0.4 (0.8) | 0.7 (0.5); 0.6 (0.6) | 0.9 (0.9); 0.5 (1.8) | 1.5 (0.6); 1.5 (1.1) | <0.001 * |
| Pain VAS scores (0–10) | |||||||||
| n (%) | 93 (100) c | 80 | 54 (58) a | 7 (7) | 9 (10) | 23 (25) d | |||
| M (SD); median (IQR) | 2.8 (3.1); 1.9 (5.5) | 0.0 (0.2) | <0.001 * | 1.27 | 1.3 (2.3); 0 (2.0) | 2.8 (2.7); 2.5 (5.7) | 3.6 (2.2); 2.9 (3.2) | 6.1(2.7); 7.0 (3.7) | <0.001 * |
| General health VAS scores (0–10) | |||||||||
| n (%) | 82 (100) e | 80 | 48 (59) f | 6 (7) g | 6 (7) h | 22 (27) i | |||
| M (SD); median (IQR) | 2.5 (1.8); 2.0 (2.5) | 0.0 (0.1) | <0.001 * | 2.04 | 1.8 (1.2); 1.5 (1.6) | 2.1 (1.5); 2.4 (2.5) | 2.8 (2.1); 2.3 (1.7) | 4.1 (1.8); 4.1 (3.3) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warnink-Kavelaars, J.; de Koning, L.E.; Rombaut, L.; Alsem, M.W.; Menke, L.A.; Oosterlaan, J.; Buizer, A.I.; Engelbert, R.H.H.; on behalf of the Pediatric Heritable Connective Tissue Disorders Study Group. Heritable Connective Tissue Disorders in Childhood: Increased Fatigue, Pain, Disability and Decreased General Health. Genes 2021, 12, 831. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12060831
Warnink-Kavelaars J, de Koning LE, Rombaut L, Alsem MW, Menke LA, Oosterlaan J, Buizer AI, Engelbert RHH, on behalf of the Pediatric Heritable Connective Tissue Disorders Study Group. Heritable Connective Tissue Disorders in Childhood: Increased Fatigue, Pain, Disability and Decreased General Health. Genes. 2021; 12(6):831. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12060831
Chicago/Turabian StyleWarnink-Kavelaars, Jessica, Lisanne E. de Koning, Lies Rombaut, Mattijs W. Alsem, Leonie A. Menke, Jaap Oosterlaan, Annemieke I. Buizer, Raoul H. H. Engelbert, and on behalf of the Pediatric Heritable Connective Tissue Disorders Study Group. 2021. "Heritable Connective Tissue Disorders in Childhood: Increased Fatigue, Pain, Disability and Decreased General Health" Genes 12, no. 6: 831. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12060831