
Differences in Ovarian and Other Cancers Risks by Population and BRCA Mutation Location


Department of Obstetrics and Gynecology, Niigata University Graduate School of Medical and Dental Sciences, Niigata 951-8510, Japan
*
Author to whom correspondence should be addressed.
Genes 2021, 12(7), 1050; https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071050
Submission received: 21 May 2021
/
Revised: 2 July 2021
/
Accepted: 6 July 2021
/
Published: 8 July 2021
(This article belongs to the Special Issue BRCA1 and BRCA2: Genome Instability and Tumorigenesis)
Abstract
:Hereditary breast and ovarian cancer is caused by a germline mutation in BRCA1 or BRCA2 genes. The frequency of germline BRCA1/2 gene mutation carriers and the ratio of germline BRCA1 to BRCA2 mutations in BRCA-related cancer patients vary depending on the population. Genotype and phenotype correlations have been reported in BRCA mutant families, however, the correlations are rarely used for individual risk assessment and management. BRCA genetic testing has become a companion diagnostic for PARP inhibitors, and the number of families with germline BRCA mutation identified is growing rapidly. Therefore, it is expected that analysis of the risk of developing cancer will be possible in a large number of BRCA mutant carriers, and there is a possibility that personal and precision medicine for the carriers with specific common founder mutations will be realized. In this review, we investigated the association of ovarian cancer risk and BRCA mutation location, and differences of other BRCA-related cancer risks by BRCA1/2 mutation, and furthermore, we discussed the difference in the prevalence of germline BRCA mutation in ovarian cancer patients. As a result, although there are various discussions, there appear to be differences in ovarian cancer risk by population and BRCA mutation location. If it becomes possible to estimate the risk of developing BRCA-related cancer for each BRCA mutation type, the age at risk-reducing salpingo-oophorectomy can be determined individually. The decision would bring great benefits to young women with germline BRCA mutations.
1. Introduction
The BRCA1 gene, located on chromosome 17, and the BRCA2 gene, located on chromosome 13, are involved in the repair of double-strand DNA breaks and cell-cycle checkpoints in response to DNA damage. The functions of two genes preserve genomic stability as tumor suppressor genes [1,2,3,4]. The overall prevalence of germline mutations in BRCA1 and BRCA2 genes in unaffected women has been estimated at 0.11% and 0.24%, respectively [5]. So far, many mutations have been identified in BRCA1/2 genes. Among them, the same mutation has been found in multiple, unrelated families and can be traced back to a common ancestor. Such mutations are so-called common founder mutations observed in specific populations, e.g., 187delAG and 5385insC of BRCA1 and the 6174delT of BRCA2 in the Ashkenazi Jewish and L63X and Q934X of BRCA1 in a Japanese population [6,7,8,9]. Certain common founder mutations have also been identified in other populations [10,11,12,13,14,15,16]. The carriers of BRCA1/2 mutations have a high risk of specific cancer, such as breast, ovarian, pancreatic, and prostate cancer. However, the probability of cancer development in the carriers is variable, even within families with the same variant [17,18,19]. It is still unknown whether the risk of developing cancer in the carriers is related only to the specific mutation or whether additional genetic and environmental factors exist.
In this review article, we used three databases (PubMed, Google Scholar, and Web of Science) and references or related articles to conduct a review of the cancer risk by BRCA mutation types. We identified articles in the databases using the following search string: (“ovarian cancer” OR “breast cancer” OR “common mutation” OR “founder mutation” OR “cancer risk” OR “ethnicity” OR “race” OR “population”) AND “BRCA”. Given the search results, we added the words “Prostate cancer,” “Pancreatic cancer,” “Melanoma,” “risk-reducing salpingo-oophorectomy,” and “risk-reducing mastectomy” to cover all relevant articles.
2. Differences of the Prevalence of Germline BRCA Mutation in Ovarian Cancer Patients
2.1. Prevalence of Germline BRCA1/2 Mutation in Ovarian Cancer Patients
The risk of developing ovarian cancer is thought to increase with early menarche, delayed menopause, nulliparity, infertility, and obesity, however, the strongest risk factor for ovarian cancer is a positive family history of breast and/or ovarian cancer [20,21,22]. The risk of developing ovarian cancer is 2 to 6 times higher in those who have breast cancer or ovarian cancer as first-degree relatives [23,24,25]. Hereditary ovarian cancer occurs as part of a hereditary tumor represented by Hereditary breast and ovarian cancer (HBOC) and Lynch syndrome. Of these, HBOC is the most involved and is estimated to account for about 65–85% of hereditary ovarian cancers [26]. In large-scale epidemiologic studies, the penetrance of the BRCA1/2 gene for female breast cancer was about 70%, and there was almost no difference between BRCA1 and BRCA2 [27]. However, the penetrance of the BRCA1 or BRCA2 gene for ovarian cancer has been reported to be about 40% and 20%, respectively [27]. On the other hand, the risk of developing male breast cancer, prostate cancer, pancreatic cancer, and melanoma in BRCA2 mutation carriers has been reported to be higher than in BRCA1 [26]. Given the genetic risk of developing ovarian cancer in a population, the frequency of BRCA gene carriers in the general population leads to the direct estimation of risk factors. In addition, the frequency of germline BRCA1/2 gene mutation carriers and the ratio of germline BRCA1 to BRCA2 mutations in ovarian cancer patients may vary depending on the population.
Table 1 shows the differences in germline BRCA1/2 mutation prevalence between population and country in ovarian cancer patients [28,29,30,31,32,33,34,35,36,37,38]. The frequency of germline BRCA mutation ranged from 5% to 30%. Among these reports, the high frequency of germline BRCA mutation in Ashkenazi Jews stands out as already reported [22]. The frequency of germline BRCA mutation in the USA, Canada, Australia, and Japan showed average values of about 15% [29,30,35,38]. On the other hand, the frequency of germline BRCA mutation varies in European countries, but that of Finland, Sweden, Denmark and Iceland appear to be relatively low [31,32,33,39]. The ratio of BRCA1 to BRCA2 mutations varies from population to population, but it is consistent with previous reports that germline BRCA1 mutation was more common than germline BRCA2 mutation in ovarian cancer cases. However, reports from Iceland and Poland show that germline BRCA2 mutation was more frequent than germline BRCA1 mutation [39,40]. The exact reason for this event is unknown, but the presence and spread of common founder mutations among ethnically different populations may have affected the proportion of germline BRCA1/2 mutation.
2.2. Histological Subtypes in BRCA-Related Ovarian Cancer
In many mutational analyses of BRCA1/2 genes for epithelial ovarian cancer, we picked up large-scale epidemiological studies of more than 500 ovarian cancer patients. Table 2 shows that the rate of germline BRCA mutation of each histological type varies by the country where the study was conducted [28,29,30,34,35,36,37,38]. Regarding high-grade serous carcinoma, the mutation rate showed a range of 16% to 28%, and the rate tended to be higher in Asian countries than in Western countries. Almost 20% of Low-grade serous carcinoma in Japan or Korea were BRCA mutated, while this was only 6% in the USA or German population. Although it is not clear due to the small number of cases, the frequency of BRCA mutation in Low-grade serous carcinoma may be lower in Asia than that in European countries. Regarding mucinous carcinoma, no case with germline BRCA mutation was found in Western countries and Japan, however, germline BRCA1/2 mutation was found in 4 of 57 cases (7.0%) in China and 1 of 18 cases (5.6%) in South Korea. There is no doubt that patients with mucinous carcinoma rarely have germline BRCA mutation [8], but it is unclear whether the involvement of BRCA gene mutations in the pathogenic mechanism of mucinous carcinoma differs between Western and Asian countries. In the histological diagnosis of ovarian cancer, the existence of a mixed type is also known, and it may be related to the diversity of pathological diagnosis rather than the molecular biological reason. Regarding endometrioid carcinoma, the mutation rate was the lowest in Japan at 6.7% and the highest in Germany and South Korea at 13.0%, but there seems to be no clear difference between the countries. There are few reports on the new classification, Seromucinous tumor of the ovary, but in the analysis of four cases in Japan and seven cases in South Korea, no case with germline BRCA1/2 mutation was found in the tumor.
Regarding clear cell carcinoma, Germany had the lowest rate at 0%, followed by Japan at 2.1%, and other countries at about 7%. There are significant differences between Western and East Asian countries regarding the frequency of clear cell carcinoma in all types of epithelial ovarian cancer. For example, the frequency of clear cell carcinoma in the United States is about 6%, but the frequency of clear cell carcinoma in Japan is about 25%, which is a four-fold difference [45,46]. It is known that the incidence of endometriosis is high in East Asia [47], and it is presumed that this is a factor in the higher frequency of clear cell carcinoma that develops from endometriosis than in Western countries [48]. Especially in Japan, there is a tendency that drug therapy with GnRH agonists and Dienogest is preferred over surgical therapy as a treatment for endometriosis [49], so there is a relatively high possibility that clear cell carcinoma will develop from an endometriotic cyst.
Regarding the difference between BRCA1 and BRCA2 in the frequency of histological types in each country, the frequency of serous carcinoma in cases with BRCA1 or BRCA2 mutation was about 80%, and there was almost no difference between BRCA1 and BRCA2. Among ovarian cancer patients in China and South Korea, five cases of mucinous carcinoma with BRCA1/2 mutation were found, of which three cases had a BRCA1 mutation and two cases had a BRCA2 mutation.
3. Association of Breast/Ovarian Cancer Risk and BRCA Mutation Location
Genotype and phenotype correlations have been reported in BRCA mutant families. At present, such correlations are rarely used for individual risk assessment and management. However, the data of the mutant carriers have accumulated dramatically, so the genotype and phenotype correlations may be utilized for individual risk assessment.
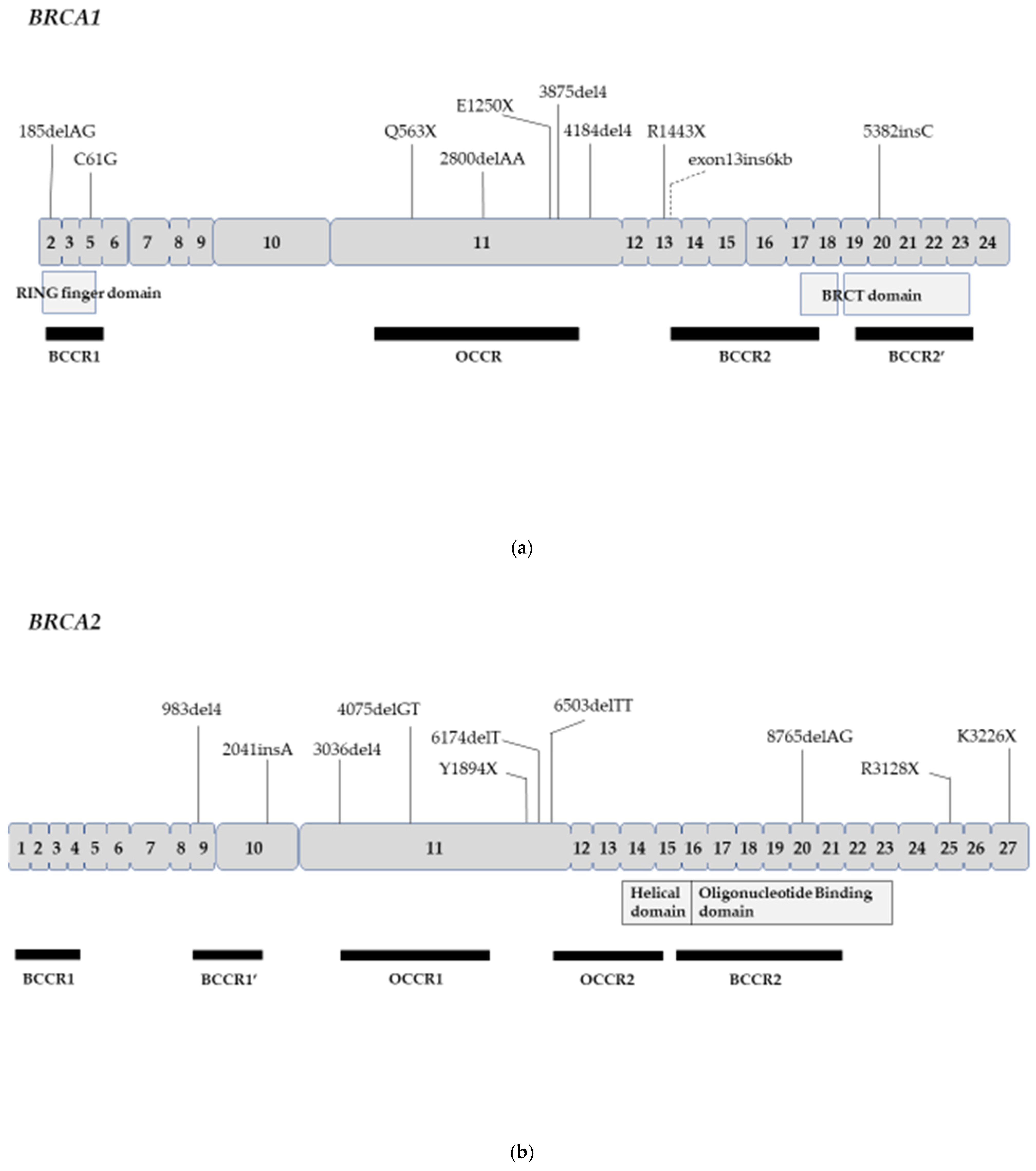
The ovarian cancer cluster region (OCCR) was identified in or near exon 11 in both the BRCA1 and BRCA2 genes. Mutations within the lesion increase the ratio of ovarian cancer to breast cancer, unlike variants elsewhere in both genes. The Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA) revealed that the incidence of ovarian cancer is high in patients with germline BRCA mutation in the OCCR in about 30,000 BRCA mutant carriers in 33 countries around the world [50]. These results are consistent with prior reports of OCCR in BRCA1/2 genes [51,52,53]. On the other hand, regarding the breast cancer cluster region (BCCR), multiple regions other than exon 11 have been reported for both genes [50,54]. Rebbeck et al. speculated why OCCR is present in the BRCA1 gene as follows. Mutations in exon 11 could produce a partial BRCA1 protein encoded by the known exon 11 splice variant, while the full-length protein is lost by the process of nonsense-mediated mRNA decay (NMD). Thus, it is biologically plausible that individuals carrying mutations within exon 11 (and the OCCR) may have a different phenotype than other mutations for BRCA1 [50].
The Breast Cancer Information Core (BIC) database contains DNA sequence variations reported from around the world. The total number of database entries was 15,311 and 14,914 in BRCA1 and BRCA2, respectively [55]. Table 3 shows the top 10 pathogenic mutations in BRCA1 or BRCA2. Regarding the judgment of clinical pathogenic importance, according to the opinion of the BIC steering committee, the sequence change of this type interferes with gene function and results in an increased risk of cancer based on available data [55]. For the BRCA1 gene, the most frequently reported mutation is 185delAG, followed by 5382insC, C61G, 4184del4, R1443X, 3875del4, and exon13ins6kb. The above seven variants showed the number of entries of 100 times or more. Among these common founder mutations, the mutations located within OCCR are Q563X, 2800delAA, E1250X, and 3875del4 in BRCA1 and 4075delGT in BRCA2 (Figure 1). In a recent report, Yoshihara et al. reported that more than 50% of Japanese ovarian cancer patients with BRCA1 or BRCA2 mutations were within the OCCR after excluding 16 cases with L63X founder mutation [56]. On the other hand, Cardoso et al. reported that 33% (20/60) of Argentine ovarian cancer patients with BRCA1 mutations were beyond the OCCR, in stark contrast with 61% (22/36) of the patients with BRCA2 mutations being inside the OCCR [57]. Moreover, Teixeira et al. reported that among Dutch BRCA1 families, ovarian cancer risks were higher in women with OCCR mutations than non-OCCR mutations, but not in BRCA2 families [58].
Rebbeck et al. reported that exon 11 mutations were associated with earlier ages in breast and ovarian cancer diagnosis and mutations conferring NMD or premature termination codon were associated with a later age at breast cancer diagnosis in BRCA1. In BRCA2, the mean age was greater for mutations in OCCR vs. mutations not in OCCR (45.0 vs. 43.9 years, p < 0.001), lower for mutations in BCCR1 vs. mutations not in BCCR1 (42.6 vs. 44.3 years; p = 0.004), and lower for mutations in BCCR2 vs. mutations not in BCCR2 (43.5 vs. 44.3 years, p = 0.04) [50].
Various common founder mutations of the BRCA gene have been reported by different populations in the world [28,59]. It has been reported that some of these mutation carriers have a different risk of developing cancer than the overall mutation carriers. For example, Satagopan et al. reported that the estimated lifetime ovarian cancer risks were 66% (95% CI, 37–100%) due to 185delAG mutation and 29% (95% CI, 16–69%) due to 5382insC mutation [60]. There is also a report that the presence of 5382insC decreased and C61G in BRCA1 increased the risk of peritoneal cancer (p = 0.049 vs. p = 0.013) in the Polish population who underwent risk-reducing salpingo-oophorectomy (RRSO) [61]. Ashkenazi Jewish families with the 6174delT founder mutation were more likely to have a family member with ovarian cancer (OR = 1.58; p = 0.002) [62]. Breast cancer risks for carriers of 6174delT were lower than those of all BRCA1 carriers (43% by age 70, 95% CI, 14% to 62%; p = 0.007 compared with all BRCA1 mutation carriers), on the other hand, the ovarian cancer risks in the carriers were somewhat higher than the average BRCA2 risks (20% vs. 11%) [63]. The corresponding ovarian cancer risks were 14% (95% CI, 2% to 24%), 33% (8% to 50%), and 20% (2% to 35%) in carriers of the 185delAG, 5382insC in BRCA1 and 6174delT mutations in BRCA2, respectively [63]. The K3326X mutation was associated with increased risk of breast cancer (OR = 1.28, 95% CI = 1.17 to 1.40) independent of additional BRCA2 mutations and demonstrated strong association with serous ovarian cancer (OR = 1.46, 95% CI = 1.2 to 1.70), but not with prostate cancer [64].
We found L63X and Q934X as Japanese common founder mutations previously [8]. The clinical characteristics (e.g., subtype and nuclear grade of resultant cancer) of breast cancer patients with L63X might differ from those in patients with other BRCA mutations, however, the elevation of ovarian or breast cancer risk was not detected [65]. After excluding L63X founder mutation, the proportion of patients with a family history of ovarian cancer and germline BRCA1 mutations outside the OCCR was lower and the proportion of patients with a family history of breast cancer and germline BRCA1 mutations within the OCCR was relatively lower [56]. There are, relatively, many reports that BRCA carriers with common founder mutations have different risks of developing breast and ovarian cancer compared with the overall BRCA1/2 mutation, however, the results of only a few common founder mutations have been validated by multiple studies. Since the frequency of specific common founder mutations in each population varies, so does the number of breast and ovarian cancer patients who carry the mutation. In other words, 185delAG in the Ashkenazi Jewish population can be analyzed in many breast and ovarian cancer cases, so it is possible to analyze the risk of developing cancer relatively easily. However, sufficient statistical power is often not obtained in the analysis of other common founder mutations. BRCA genetic testing has become a companion diagnostic for PARP inhibitors, and the number of families with germline BRCA mutation identified is growing rapidly [66]. Therefore, it is expected that analysis of the risk of developing cancer will be possible in a large number of mutant carriers, and there is a possibility that personal and precision medicine for carriers with specific common founder mutations will be realized [67].
4. Differences of other BRCA-Related Cancers Risks by BRCA1/2 Mutation
4.1. Contralateral Breast Cancer Risk
Ten-year cumulative contralateral Breast Cancer (CBC) risks were 21.1% for BRCA1, 10.8% for BRCA2 mutation carriers and 5.1% for non-carriers [68]. On the other hand, the 15-year actuarial risk of CBC was 36.1% for BRCA1 carriers and was 28.5% for BRCA2 carriers [69]. The average cumulative risks by age 70 years for BRCA1 and BRCA2 carriers were estimated to be 83% and 62% for CBC [70,71].
4.2. Male Breast Cancer
Tai et al. reported that the cumulative risks of male breast cancer were higher in both BRCA1 and BRCA2 carriers than in non-carriers at all ages. The relative risks of developing breast cancer were highest for men in their 30s and 40s. Both the relative and cumulative risks were higher for BRCA2 carriers than for BRCA1 carriers. The estimated cumulative risk of breast carcinoma for male BRCA1 mutation carriers at age 70 years was 1.2% and for BRCA2 mutation carriers, 6.8% [72]. In addition, both retrospective and prospective analyses confirmed that breast cancer risk in men was 7.1% by age 70 years and 8.4% by age 80 years in BRCA2 carriers [71,73]. Struewing et al. reported that four (3.6%) and fifteen (13.6%) of 110 Israeli Jewish male breast cancer patients carried the BRCA1 185delAG and BRCA2 6174delT founder mutation, respectively, but not BRCA1 5382insC [74]. Lubinski et al. reported that a high risk of male breast cancer was observed with the BRCA2 6503delTT mutation (OR = 15.7; p = 0.023) [62].
4.3. Prostate Cancer
Based on previously estimated population frequencies of BRCA1 and BRCA2 mutations, it was estimated that BRCA1 mutations confer a relative risk of prostate cancer of approximately 3.7-fold and 8.6-fold, which translates to an 8.6% and 15% cumulative risk by age 65 years [71,75,76]. A recent meta-analysis revealed that the relative risk of prostate cancer is 1.35-fold and 2.64-fold in BRCA1 and BRCA2 carriers, respectively. Overall survival was significantly worse among germline BRCA2 carriers compared to non-carriers [77]. BRCA2-related prostate cancer has been associated with a higher histologic grade and results in a poorer overall survival [78,79]. It was reported that BRCA2, in particular, confers a more aggressive phenotype with a higher probability of locally advanced and metastatic disease, and should be considered a prognostic marker associated with poorer survival [80]. Agalliu et al. reported that BRCA2 mutation confers a 3-fold elevated risk of high-grade prostate cancer. Although BRCA1 mutations were not associated with prostate cancer, the BRCA1 185delAG was associated with high Gleason score tumors [81].
4.4. Pancreatic Cancer
Several studies reported that BRCA2 carriers had higher relative and cumulative risks of pancreatic cancer compared to BRCA1 carriers [71,82,83]. Recently, Mocci et al. reported that BRCA1 carriers were at increased risk of pancreatic cancer [standardized incidence ratios (SIR) = 4.11] as were BRCA2 carriers (SIR = 5.79) in a retrospective cohort analysis [84]. A prospective study of 5,149 females with BRCA1 or BRCA2 carriers showed a significant 2.4-fold increase in the incidence of pancreatic cancer and the increase in the incidence of pancreatic cancer was similar for BRCA1 (SIR = 2.55) and BRCA2 (SIR = 2.13) [85]. Among unselected pancreatic cancer patient cohorts, multiple studies have shown to estimate the incidence of germline BRCA mutations ranged from 0.7–5.7% for BRCA2 and 0.3–2.3% for BRCA1 [86]. Of the 145 Jewish pancreatic adenocarcinoma patients, 8 patients (5.5%) were found to have BRCA mutations, 6 patients (4.1%) carried a BRCA2 mutation (6174delT) and 2 patients (1.3%) carried a BRCA1 mutation (185delAG and 5382insC) [87].
4.5. Melanoma
4.6. Endometrial Cancer
Previous studies suggested that endometrial serous adenocarcinoma is not BRCA-related cancer and is more associated with tamoxifen exposure than with the effects of germline BRCA mutations [90,91]. Recently, in a prospective cohort study of BRCA carriers who received only RRSO, not hysterectomy, endometrial cancer developed in eight patients in a median follow-up of 5.1 years, with no apparent increased risk after RRSO, on the other hand, BRCA1 carriers had an increased risk of endometrial serous adenocarcinoma [92]. Furthermore, a large Dutch nationwide cohort study revealed that BRCA1/2 carriers have a 2- to 3-fold increased risk for endometrial cancer, with the highest risk observed for the rare subgroups of serous-like and p53-abnormal endometrial cancer in BRCA1 carriers [93].
5. Conclusions
Although there are various discussions, there appear to be differences in ovarian cancer risk by ethnicity and BRCA mutation types. These mutation-specific risks coincide with known or hypothesized functional domains and provide a basis around which accurate risk estimates can be generated for women who have inherited a particular BRCA1/2 mutation. While RRSO is certain to reduce the risk of ovarian cancer, there are some concerns about reducing the risk of breast cancer. In a prospective cohort study, Kauff et al. reported that RRSO did not significantly reduce the breast cancer risk in BRCA1 carriers [94]. However, the latest meta-analysis has shown a significant reduction in breast cancer risk and overall mortality rate, regardless of the past history of breast cancer [95]. The risk of breast cancer does not appear to be different between BRCA1 and BRCA2 carriers [95].
The National Comprehensive Cancer Network (NCCN) guidelines state that the age at RRSO should be based on the earlier age at diagnosis of ovarian cancer patients in the family [26]. If it becomes possible to estimate the risk of developing breast and ovarian cancer and the age of onset disease for each BRCA mutation type, the age at RRSO can be determined individually. Solsky et al. reported that for BRCA1/2 carriers who delayed RRSO or who were identified with a mutation later in life, the OCCR mutation tended to be associated with lower life expectancy estimates than the BCCR and non-BCCR/OCCR mutations, so BRCA1/2 cluster regions may provide more precise estimates of life expectancy in counseling and shared decision-making [54]. The decision would bring great benefits to young women with BRCA mutations, so we hope that a lot of verifiable research will be undertaken.
Author Contributions
M.S. wrote the initial draft of the manuscript. T.E. and K.N. critically reviewed the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work in ensuring that questions-related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable for this review article.
Informed Consent Statement
Not required for the review article.
Data Availability Statement
No data are available for this review article.
Conflicts of Interest
M.S. received lecture fees from AstraZeneca. T.E. received lecture fees from AstraZeneca and Chugai Pharmaceutical.
References
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; Liu, Q.; Cochran, C.; Bennett, L.M.; Ding, W.; et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wooster, R.; Neuhausen, S.L.; Mangion, J.; Quirk, Y.; Ford, D.; Collins, N.; Nguyen, K.; Seal, S.; Tran, T.; Averill, D.; et al. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science 1994, 265, 2088–2090. [Google Scholar] [CrossRef] [PubMed]
- Dullens, B.; de Putter, R.; Lambertini, M.; Toss, A.; Han, S.; Van Nieuwenhuysen, E.; Van Gorp, T.; Vanderstichele, A.; Van Ongeval, C.; Keupers, M.; et al. Cancer Surveillance in Healthy Carriers of Germline Pathogenic Variants in BRCA1/2: A Review of Secondary Prevention Guidelines. J. Oncol. 2020, 2020, 9873954. [Google Scholar] [CrossRef] [PubMed]
- Cipak, L.; Watanabe, N.; Bessho, T. The role of BRCA2 in replication-coupled DNA interstrand cross-link repair In Vitro. Nat. Struct. Mol. Biol. 2006, 13, 729–733. [Google Scholar] [CrossRef]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef]
- Foulkes, W.D. Inherited susceptibility to common cancers. N. Engl. J. Med. 2008, 359, 2143–2153. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Poll, A.; Royer, R.; Llacuachaqui, M.; Tulman, A.; Sun, P.; Narod, S.A. Screening for founder mutations in BRCA1 and BRCA2 in unselected Jewish women. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 387–391. [Google Scholar] [CrossRef]
- Sekine, M.; Nagata, H.; Tsuji, S.; Hirai, Y.; Fujimoto, S.; Hatae, M.; Kobayashi, I.; Fujii, T.; Nagata, I.; Ushijima, K.; et al. Mutational analysis of BRCA1 and BRCA2 and clinicopathologic analysis of ovarian cancer in 82 ovarian cancer families: Two common founder mutations of BRCA1 in Japanese population. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2001, 7, 3144–3150. [Google Scholar]
- Sekine, M.; Nagata, H.; Tsuji, S.; Hirai, Y.; Fujimoto, S.; Hatae, M.; Kobayashi, I.; Fujii, T.; Nagata, I.; Ushijima, K.; et al. Localization of a novel susceptibility gene for familial ovarian cancer to chromosome 3p22-p25. Hum. Mol. Genet. 2001, 10, 1421–1429. [Google Scholar] [CrossRef]
- Genetics, A.C. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 103: Hereditary breast and ovarian cancer syndrome. Obstet. Gynecol. 2009, 113, 957–966. [Google Scholar] [CrossRef]
- Csokay, B.; Udvarhelyi, N.; Sulyok, Z.; Besznyak, I.; Ramus, S.; Ponder, B.; Olah, E. High frequency of germ-line BRCA2 mutations among Hungarian male breast cancer patients without family history. Cancer Res. 1999, 59, 995–998. [Google Scholar]
- Ji, J.; Hemminki, K. Familial risk for histology-specific bone cancers: An updated study in Sweden. Eur. J. Cancer 2006, 42, 2343–2349. [Google Scholar] [CrossRef] [PubMed]
- Mikaelsdottir, E.K.; Valgeirsdottir, S.; Eyfjord, J.E.; Rafnar, T. The Icelandic founder mutation BRCA2 999del5: Analysis of expression. Breast Cancer Res. 2004, 6, R284–R290. [Google Scholar] [CrossRef] [Green Version]
- Petrij-Bosch, A.; Peelen, T.; van Vliet, M.; van Eijk, R.; Olmer, R.; Drüsedau, M.; Hogervorst, F.B.; Hageman, S.; Arts, P.J.; Ligtenberg, M.J.; et al. BRCA1 genomic deletions are major founder mutations in Dutch breast cancer patients. Nat. Genet. 1997, 17, 341–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonin, P.N.; Mes-Masson, A.M.; Futreal, P.A.; Morgan, K.; Mahon, M.; Foulkes, W.D.; Cole, D.E.; Provencher, D.; Ghadirian, P.; Narod, S.A. Founder BRCA1 and BRCA2 mutations in French Canadian breast and ovarian cancer families. Am. J. Hum. Genet. 1998, 63, 1341–1351. [Google Scholar] [CrossRef] [Green Version]
- Díez, O.; Osorio, A.; Durán, M.; Martinez-Ferrandis, J.I.; de la Hoya, M.; Salazar, R.; Vega, A.; Campos, B.; Rodríguez-López, R.; Velasco, E.; et al. Analysis of BRCA1 and BRCA2 genes in Spanish breast/ovarian cancer patients: A high proportion of mutations unique to Spain and evidence of founder effects. Hum. Mutat. 2003, 22, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.; Battelli, C.; Allen, B.; Kaldate, R.; Bhatnagar, S.; Bowles, K.; Timms, K.; Garber, J.E.; Herold, C.; Ellisen, L.; et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer 2015, 121, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Buys, S.S.; Sandbach, J.F.; Gammon, A.; Patel, G.; Kidd, J.; Brown, K.L.; Sharma, L.; Saam, J.; Lancaster, J.; Daly, M.B. A study of over 35,000 women with breast cancer tested with a 25-gene panel of hereditary cancer genes. Cancer 2017, 123, 1721–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, M.J.; Obeid, E.; Daly, M.B. Multigene Panels to Evaluate Hereditary Cancer Risk: Reckless or Relevant? J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 4186–4187. [Google Scholar] [CrossRef]
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of ovarian cancer: A review. Cancer Biol. Med. 2017, 14, 9–32. [Google Scholar] [CrossRef] [Green Version]
- La Vecchia, C. Ovarian cancer: Epidemiology and risk factors. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. 2017, 26, 55–62. [Google Scholar] [CrossRef]
- Modan, B.; Hartge, P.; Hirsh-Yechezkel, G.; Chetrit, A.; Lubin, F.; Beller, U.; Ben-Baruch, G.; Fishman, A.; Menczer, J.; Struewing, J.P.; et al. Parity, oral contraceptives, and the risk of ovarian cancer among carriers and noncarriers of a BRCA1 or BRCA2 mutation. N. Engl. J. Med. 2001, 345, 235–240. [Google Scholar] [CrossRef]
- Goldgar, D.E.; Easton, D.F.; Cannon-Albright, L.A.; Skolnick, M.H. Systematic population-based assessment of cancer risk in first-degree relatives of cancer probands. J. Natl. Cancer Inst. 1994, 86, 1600–1608. [Google Scholar] [CrossRef] [PubMed]
- Ebell, M.H. Estimating the risk of ovarian cancer. Am. Fam. Physician 2009, 80, 632–634. [Google Scholar] [PubMed]
- Heintz, A.P.; Hacker, N.F.; Lagasse, L.D. Epidemiology and etiology of ovarian cancer: A review. Obstet. Gynecol. 1985, 66, 127–135. [Google Scholar]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanmughapriya, S.; Nachiappan, V.; Natarajaseenivasan, K. BRCA1 and BRCA2 mutations in the ovarian cancer population across race and ethnicity: Special reference to Asia. Oncology 2013, 84, 226–232. [Google Scholar] [CrossRef]
- Norquist, B.M.; Harrell, M.I.; Brady, M.F.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Bernards, S.S.; Casadei, S.; Yi, Q.; Burger, R.A.; et al. Inherited Mutations in Women With Ovarian Carcinoma. JAMA Oncol. 2016, 2, 482–490. [Google Scholar] [CrossRef]
- Risch, H.A.; McLaughlin, J.R.; Cole, D.E.; Rosen, B.; Bradley, L.; Kwan, E.; Jack, E.; Vesprini, D.J.; Kuperstein, G.; Abrahamson, J.L.; et al. Prevalence and penetrance of germline BRCA1 and BRCA2 mutations in a population series of 649 women with ovarian cancer. Am. J. Hum. Genet. 2001, 68, 700–710. [Google Scholar] [CrossRef] [Green Version]
- Sarantaus, L.; Vahteristo, P.; Bloom, E.; Tamminen, A.; Unkila-Kallio, L.; Butzow, R.; Nevanlinna, H. BRCA1 and BRCA2 mutations among 233 unselected Finnish ovarian carcinoma patients. Eur. J. Hum. Genet. 2001, 9, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Malander, S.; Ridderheim, M.; Måsbäck, A.; Loman, N.; Kristoffersson, U.; Olsson, H.; Nilbert, M.; Borg, A. One in 10 ovarian cancer patients carry germ line BRCA1 or BRCA2 mutations: Results of a prospective study in Southern Sweden. Eur. J. Cancer 2004, 40, 422–428. [Google Scholar] [CrossRef]
- Soegaard, M.; Kjaer, S.K.; Cox, M.; Wozniak, E.; Høgdall, E.; Høgdall, C.; Blaakaer, J.; Jacobs, I.J.; Gayther, S.A.; Ramus, S.J. BRCA1 and BRCA2 mutation prevalence and clinical characteristics of a population-based series of ovarian cancer cases from Denmark. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2008, 14, 3761–3767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harter, P.; Hauke, J.; Heitz, F.; Reuss, A.; Kommoss, S.; Marmé, F.; Heimbach, A.; Prieske, K.; Richters, L.; Burges, A.; et al. Prevalence of deleterious germline variants in risk genes including BRCA1/2 in consecutive ovarian cancer patients (AGO-TR-1). PLoS ONE 2017, 12, e0186043. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, T.; Aoki, D.; Hattori, K.; Jinushi, M.; Kigawa, J.; Takeshima, N.; Tsuda, H.; Watanabe, Y.; Yoshihara, K.; Sugiyama, T. The first Japanese nationwide multicenter study of BRCA mutation testing in ovarian cancer: CHARacterizing the cross-sectionaL approach to Ovarian cancer geneTic TEsting of BRCA (CHARLOTTE). Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 1043–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.; Xie, R.; Zhi, Q.; Deng, Y.; Wu, Y.; Li, W.; Yang, L.; Jiao, Z.; Luo, J.; Zi, Y.; et al. BRCA germline mutations in an unselected nationwide cohort of Chinese patients with ovarian cancer and healthy controls. Gynecol. Oncol. 2018, 151, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Ha, H.I.; Ryu, J.S.; Shim, H.; Kong, S.Y.; Lim, M.C. Reclassification of BRCA1 and BRCA2 variants found in ovarian epithelial, fallopian tube, and primary peritoneal cancers. J. Gynecol. Oncol. 2020, 31, e83. [Google Scholar] [CrossRef]
- Alsop, K.; Fereday, S.; Meldrum, C.; deFazio, A.; Emmanuel, C.; George, J.; Dobrovic, A.; Birrer, M.J.; Webb, P.M.; Stewart, C.; et al. BRCA mutation frequency and patterns of treatment response in BRCA mutation-positive women with ovarian cancer: A report from the Australian Ovarian Cancer Study Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2654–2663. [Google Scholar] [CrossRef] [Green Version]
- Rafnar, T.; Benediktsdottir, K.R.; Eldon, B.J.; Gestsson, T.; Saemundsson, H.; Olafsson, K.; Salvarsdottir, A.; Steingrimsson, E.; Thorlacius, S. BRCA2, but not BRCA1, mutations account for familial ovarian cancer in Iceland: A population-based study. Eur. J. Cancer 2004, 40, 2788–2793. [Google Scholar] [CrossRef]
- Majdak, E.J.; De Bock, G.H.; Brozek, I.; Perkowska, M.; Ochman, K.; Debniak, J.; Milczek, T.; Cornelisse, C.J.; Jassem, J.; Emerich, J.; et al. Prevalence and clinical correlations of BRCA1/BRCA2 unclassified variant carriers among unselected primary ovarian cancer cases-preliminary report. Eur. J. Cancer 2005, 41, 143–150. [Google Scholar] [CrossRef]
- Gupta, S.; Rajappa, S.; Advani, S.; Agarwal, A.; Aggarwal, S.; Goswami, C.; Palanki, S.D.; Arya, D.; Patil, S.; Kodagali, R. Prevalence of BRCA1 and BRCA2 Mutations Among Patients With Ovarian, Primary Peritoneal, and Fallopian Tube Cancer in India: A Multicenter Cross-Sectional Study. JCO Glob. Oncol. 2021, 7, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Yazici, H.; Glendon, G.; Yazici, H.; Burnie, S.J.; Saip, P.; Buyru, F.; Bengisu, E.; Andrulis, I.L.; Dalay, N.; Ozcelik, H. BRCA1 and BRCA2 mutations in Turkish familial and non-familial ovarian cancer patients: A high incidence of mutations in non-familial cases. Hum. Mutat. 2002, 20, 28–34. [Google Scholar] [CrossRef]
- Liede, A.; Malik, I.A.; Aziz, Z.; Rios Pd Pde, L.; Kwan, E.; Narod, S.A. Contribution of BRCA1 and BRCA2 mutations to breast and ovarian cancer in Pakistan. Am. J. Hum. Genet. 2002, 71, 595–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez, A.O.; Llacuachaqui, M.; Pardo, G.G.; Royer, R.; Larson, G.; Weitzel, J.N.; Narod, S.A. BRCA1 and BRCA2 mutations among ovarian cancer patients from Colombia. Gynecol. Oncol. 2012, 124, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Kamura, T.; Kigawa, J.; Terakawa, N.; Kikuchi, Y.; Kita, T.; Suzuki, M.; Sato, I.; Taguchi, K. Clinical characteristics of clear cell carcinoma of the ovary: A distinct histologic type with poor prognosis and resistance to platinum-based chemotherapy. Cancer 2000, 88, 2584–2589. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Brady, W.E.; Farley, J.; Armstrong, A.; Uyar, D.S.; Gershenson, D.M. Phase II study of single-agent cabozantinib in patients with recurrent clear cell ovarian, primary peritoneal or fallopian tube cancer (NRG-GY001). Gynecol. Oncol. 2018, 150, 9–13. [Google Scholar] [CrossRef]
- Yen, C.F.; Kim, M.R.; Lee, C.L. Epidemiologic Factors Associated with Endometriosis in East Asia. Gynecol. Minim. Invasive Ther. 2019, 8, 4–11. [Google Scholar] [CrossRef]
- Zhu, C.; Zhu, J.; Qian, L.; Liu, H.; Shen, Z.; Wu, D.; Zhao, W.; Xiao, W.; Zhou, Y. Clinical characteristics and prognosis of ovarian clear cell carcinoma: A 10-year retrospective study. BMC Cancer 2021, 21, 322. [Google Scholar] [CrossRef]
- Gerlinger, C.; Faustmann, T.; Hassall, J.J.; Seitz, C. Treatment of endometriosis in different ethnic populations: A meta-analysis of two clinical trials. BMC Women Health 2012, 12, 9. [Google Scholar] [CrossRef] [Green Version]
- Rebbeck, T.R.; Mitra, N.; Wan, F.; Sinilnikova, O.M.; Healey, S.; McGuffog, L.; Mazoyer, S.; Chenevix-Trench, G.; Easton, D.F.; Antoniou, A.C.; et al. Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. JAMA 2015, 313, 1347–1361. [Google Scholar] [CrossRef] [Green Version]
- Gayther, S.A.; Warren, W.; Mazoyer, S.; Russell, P.A.; Harrington, P.A.; Chiano, M.; Seal, S.; Hamoudi, R.; van Rensburg, E.J.; Dunning, A.M.; et al. Germline mutations of the BRCA1 gene in breast and ovarian cancer families provide evidence for a genotype-phenotype correlation. Nat. Genet. 1995, 11, 428–433. [Google Scholar] [CrossRef]
- Thompson, D.; Easton, D. Variation in BRCA1 cancer risks by mutation position. Cancer Epidemiol. Biomark. Prev. 2002, 11, 329–336. [Google Scholar]
- Gayther, S.A.; Mangion, J.; Russell, P.; Seal, S.; Barfoot, R.; Ponder, B.A.; Stratton, M.R.; Easton, D. Variation of risks of breast and ovarian cancer associated with different germline mutations of the BRCA2 gene. Nat. Genet. 1997, 15, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Solsky, I.; Chen, J.; Rebbeck, T.R. Precision prophylaxis: Identifying the optimal timing for risk-reducing salpingo-oophorectomy based on type of BRCA1 and BRCA2 cluster region mutations. Gynecol. Oncol. 2020, 156, 363–376. [Google Scholar] [CrossRef]
- Breast Cancer Information Core. Available online: https://research.nhgri.nih.gov/projects/bic/Member/index.shtml (accessed on 18 June 2021).
- Yoshihara, K.; Enomoto, T.; Aoki, D.; Watanabe, Y.; Kigawa, J.; Takeshima, N.; Inomata, H.; Hattori, K.; Jinushi, M.; Tsuda, H.; et al. Association of gBRCA1/2 mutation locations with ovarian cancer risk in Japanese patients from the CHARLOTTE study. Cancer Sci. 2020, 111, 3350–3358. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.C.; Goncalves, S.; Mele, P.G.; Liria, N.C.; Sganga, L.; Diaz Perez, I.; Podesta, E.J.; Solano, A.R. BRCA1 and BRCA2 mutations and clinical interpretation in 398 ovarian cancer patients: Comparison with breast cancer variants in a similar population. Hum. Genom. 2018, 12, 39. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, N.; Mourits, M.J.; Vos, J.R.; Kolk, D.M.; Jansen, L.; Oosterwijk, J.C.; Bock, G.H. Ovarian cancer in BRCA1/2 mutation carriers: The impact of mutation position and family history on the cancer risk. Maturitas 2015, 82, 197–202. [Google Scholar] [CrossRef]
- Felix, G.E.S.; Zheng, Y.; Olopade, O.I. Mutations in context: Implications of BRCA testing in diverse populations. Fam. Cancer 2018, 17, 471–483. [Google Scholar] [CrossRef]
- Satagopan, J.M.; Boyd, J.; Kauff, N.D.; Robson, M.; Scheuer, L.; Narod, S.; Offit, K. Ovarian cancer risk in Ashkenazi Jewish carriers of BRCA1 and BRCA2 mutations. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2002, 8, 3776–3781. [Google Scholar]
- Menkiszak, J.; Chudecka-Głaz, A.; Gronwald, J.; Cymbaluk-Płoska, A.; Celewicz, A.; Świniarska, M.; Wężowska, M.; Bedner, R.; Zielińska, D.; Tarnowska, P.; et al. Prophylactic salpingo-oophorectomy in BRCA1 mutation carriers and postoperative incidence of peritoneal and breast cancers. J. Ovarian Res. 2016, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Lubinski, J.; Phelan, C.M.; Ghadirian, P.; Lynch, H.T.; Garber, J.; Weber, B.; Tung, N.; Horsman, D.; Isaacs, C.; Monteiro, A.N.; et al. Cancer variation associated with the position of the mutation in the BRCA2 gene. Fam. Cancer 2004, 3, 1–10. [Google Scholar] [CrossRef]
- Antoniou, A.C.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Olsson, H.; Johannsson, O.; Borg, A.; Pasini, B.; et al. Breast and ovarian cancer risks to carriers of the BRCA1 5382insC and 185delAG and BRCA2 6174delT mutations: A combined analysis of 22 population based studies. J. Med. Genet. 2005, 42, 602–603. [Google Scholar] [CrossRef] [Green Version]
- Meeks, H.D.; Song, H.; Michailidou, K.; Bolla, M.K.; Dennis, J.; Wang, Q.; Barrowdale, D.; Frost, D.; McGuffog, L.; Ellis, S.; et al. BRCA2 Polymorphic Stop Codon K3326X and the Risk of Breast, Prostate, and Ovarian Cancers. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef]
- Yoshida, R.; Watanabe, C.; Yokoyama, S.; Inuzuka, M.; Yotsumoto, J.; Arai, M.; Nakamura, S. Analysis of clinical characteristics of breast cancer patients with the Japanese founder mutation BRCA1 L63X. Oncotarget 2019, 10, 3276–3284. [Google Scholar] [CrossRef] [Green Version]
- Sekine, M.; Nishino, K.; Enomoto, T. BRCA Genetic Test and Risk-Reducing Salpingo-Oophorectomy for Hereditary Breast and Ovarian Cancer: State-of-the-Art. Cancers 2021, 13, 2562. [Google Scholar] [CrossRef]
- Sekine, M.; Enomoto, T. Precision medicine for hereditary tumors in gynecologic malignancies. J. Obstet. Gynaecol. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- van den Broek, A.J.; van ’t Veer, L.J.; Hooning, M.J.; Cornelissen, S.; Broeks, A.; Rutgers, E.J.; Smit, V.T.; Cornelisse, C.J.; van Beek, M.; Janssen-Heijnen, M.L.; et al. Impact of Age at Primary Breast Cancer on Contralateral Breast Cancer Risk in BRCA1/2 Mutation Carriers. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 409–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, K.; Gershman, S.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Kim-Sing, C.; Olopade, O.I.; Domchek, S.; McLennan, J.; Eisen, A.; et al. Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Br. J. Cancer 2011, 104, 1384–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavaddat, N.; Peock, S.; Frost, D.; Ellis, S.; Platte, R.; Fineberg, E.; Evans, D.G.; Izatt, L.; Eeles, R.A.; Adlard, J.; et al. Cancer risks for BRCA1 and BRCA2 mutation carriers: Results from prospective analysis of EMBRACE. J. Natl. Cancer Inst. 2013, 105, 812–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrucelli, N.; Daly, M.B.; Pal, T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. In GeneReviews(®); Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993; Copyright © 1993-2021, University of Washington, Seattle. GeneReviews is a registered trademark of the University of Washington, Seattle. All rights reserved.: Seattle (WA), 1993. [Google Scholar]
- Tai, Y.C.; Domchek, S.; Parmigiani, G.; Chen, S. Breast cancer risk among male BRCA1 and BRCA2 mutation carriers. J. Natl. Cancer Inst. 2007, 99, 1811–1814. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Susnerwala, I.; Dawson, J.; Woodward, E.; Maher, E.R.; Lalloo, F. Risk of breast cancer in male BRCA2 carriers. J. Med. Genet. 2010, 47, 710–711. [Google Scholar] [CrossRef] [Green Version]
- Struewing, J.P.; Coriaty, Z.M.; Ron, E.; Livoff, A.; Konichezky, M.; Cohen, P.; Resnick, M.B.; Lifzchiz-Mercerl, B.; Lew, S.; Iscovich, J. Founder BRCA1/2 mutations among male patients with breast cancer in Israel. Am. J. Hum. Genet. 1999, 65, 1800–1802. [Google Scholar] [CrossRef] [Green Version]
- Leongamornlert, D.; Mahmud, N.; Tymrakiewicz, M.; Saunders, E.; Dadaev, T.; Castro, E.; Goh, C.; Govindasami, K.; Guy, M.; O’Brien, L.; et al. Germline BRCA1 mutations increase prostate cancer risk. Br. J. Cancer 2012, 106, 1697–1701. [Google Scholar] [CrossRef] [Green Version]
- Kote-Jarai, Z.; Leongamornlert, D.; Saunders, E.; Tymrakiewicz, M.; Castro, E.; Mahmud, N.; Guy, M.; Edwards, S.; O’Brien, L.; Sawyer, E.; et al. BRCA2 is a moderate penetrance gene contributing to young-onset prostate cancer: Implications for genetic testing in prostate cancer patients. Br. J. Cancer 2011, 105, 1230–1234. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.; Alkhushaym, N.; Fallatah, S.; Althagafi, A.; Aljadeed, R.; Alsowaida, Y.; Jeter, J.; Martin, J.R.; Babiker, H.M.; McBride, A.; et al. The association of BRCA1 and BRCA2 mutations with prostate cancer risk, frequency, and mortality: A meta-analysis. Prostate 2019, 79, 880–895. [Google Scholar] [CrossRef]
- Gallagher, D.J.; Gaudet, M.M.; Pal, P.; Kirchhoff, T.; Balistreri, L.; Vora, K.; Bhatia, J.; Stadler, Z.; Fine, S.W.; Reuter, V.; et al. Germline BRCA mutations denote a clinicopathologic subset of prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2010, 16, 2115–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorne, H.; Willems, A.J.; Niedermayr, E.; Hoh, I.M.; Li, J.; Clouston, D.; Mitchell, G.; Fox, S.; Hopper, J.L.; Bolton, D. Decreased prostate cancer-specific survival of men with BRCA2 mutations from multiple breast cancer families. Cancer Prev. Res. 2011, 4, 1002–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leão, R.R.N.; Price, A.J.; James Hamilton, R. Germline BRCA mutation in male carriers-ripe for precision oncology? Prostate Cancer Prostatic Dis. 2018, 21, 48–56. [Google Scholar] [CrossRef]
- Agalliu, I.; Gern, R.; Leanza, S.; Burk, R.D. Associations of high-grade prostate cancer with BRCA1 and BRCA2 founder mutations. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2009, 15, 1112–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.; Easton, D.F. Cancer Incidence in BRCA1 mutation carriers. J. Natl. Cancer Inst. 2002, 94, 1358–1365. [Google Scholar] [CrossRef] [Green Version]
- Risch, H.A.; McLaughlin, J.R.; Cole, D.E.; Rosen, B.; Bradley, L.; Fan, I.; Tang, J.; Li, S.; Zhang, S.; Shaw, P.A.; et al. Population BRCA1 and BRCA2 mutation frequencies and cancer penetrances: A kin-cohort study in Ontario, Canada. J. Natl. Cancer Inst. 2006, 98, 1694–1706. [Google Scholar] [CrossRef] [PubMed]
- Mocci, E.; Milne, R.L.; Méndez-Villamil, E.Y.; Hopper, J.L.; John, E.M.; Andrulis, I.L.; Chung, W.K.; Daly, M.; Buys, S.S.; Malats, N.; et al. Risk of pancreatic cancer in breast cancer families from the breast cancer family registry. Cancer Epidemiol. Biomark. Prev. 2013, 22, 803–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, J.; Ragone, A.; Lubinski, J.; Lynch, H.T.; Moller, P.; Ghadirian, P.; Foulkes, W.D.; Armel, S.; Eisen, A.; Neuhausen, S.L.; et al. The incidence of pancreatic cancer in BRCA1 and BRCA2 mutation carriers. Br. J. Cancer 2012, 107, 2005–2009. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.N.; Goodwin, R.A.; Vickers, M.M. BRCA mutated pancreatic cancer: A change is coming. World J. Gastroenterol. 2021, 27, 1943–1958. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Levine, D.A.; Tang, L.H.; Allen, P.J.; Jarnagin, W.; Brennan, M.F.; Offit, K.; Robson, M.E. BRCA germline mutations in Jewish patients with pancreatic adenocarcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Hearle, N.; Damato, B.E.; Humphreys, J.; Wixey, J.; Green, H.; Stone, J.; Easton, D.F.; Houlston, R.S. Contribution of germline mutations in BRCA2, P16(INK4A), P14(ARF) and P15 to uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 458–462. [Google Scholar] [CrossRef] [Green Version]
- Moran, A.; O’Hara, C.; Khan, S.; Shack, L.; Woodward, E.; Maher, E.R.; Lalloo, F.; Evans, D.G. Risk of cancer other than breast or ovarian in individuals with BRCA1 and BRCA2 mutations. Fam. Cancer 2012, 11, 235–242. [Google Scholar] [CrossRef]
- Goshen, R.; Chu, W.; Elit, L.; Pal, T.; Hakimi, J.; Ackerman, I.; Fyles, A.; Mitchell, M.; Narod, S.A. Is uterine papillary serous adenocarcinoma a manifestation of the hereditary breast-ovarian cancer syndrome? Gynecol. Oncol. 2000, 79, 477–481. [Google Scholar] [CrossRef]
- Beiner, M.E.; Finch, A.; Rosen, B.; Lubinski, J.; Moller, P.; Ghadirian, P.; Lynch, H.T.; Friedman, E.; Sun, P.; Narod, S.A. The risk of endometrial cancer in women with BRCA1 and BRCA2 mutations. A prospective study. Gynecol. Oncol. 2007, 104, 7–10. [Google Scholar] [CrossRef]
- Shu, C.A.; Pike, M.C.; Jotwani, A.R.; Friebel, T.M.; Soslow, R.A.; Levine, D.A.; Nathanson, K.L.; Konner, J.A.; Arnold, A.G.; Bogomolniy, F.; et al. Uterine Cancer After Risk-Reducing Salpingo-oophorectomy Without Hysterectomy in Women With BRCA Mutations. JAMA Oncol. 2016, 2, 1434–1440. [Google Scholar] [CrossRef] [Green Version]
- de Jonge, M.M.; de Kroon, C.D.; Jenner, D.J.; Oosting, J.; de Hullu, J.A.; Mourits, M.J.E.; Garcia, E.B.G.; Ausems, M.; Collée, J.M.; van Engelen, K.; et al. Endometrial Cancer Risk in Women with Germline BRCA1 or BRCA2 Mutations: Multicenter Cohort Study. J. Natl. Cancer Inst. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kauff, N.D.; Domchek, S.M.; Friebel, T.M.; Robson, M.E.; Lee, J.; Garber, J.E.; Isaacs, C.; Evans, D.G.; Lynch, H.; Eeles, R.A.; et al. Risk-reducing salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: A multicenter, prospective study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 1331–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Y.L.; Wang, K.; Liu, Q.; Li, J.; Zhang, X.; Li, H.Y. Risk Reduction and Survival Benefit of Risk-Reducing Salpingo-oophorectomy in Hereditary Breast Cancer: Meta-analysis and Systematic Review. Clin. Breast Cancer 2019, 19, e48–e65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Prevalence of (a) BRCA1 and (b) BRCA2 common founder mutations by location. Putative functional domains are shown in the middle. Regions inferred to be breast cancer cluster region (BCCR) and ovarian cancer cluster region (OCCR) are shown at the bottom.
Figure 1.
Prevalence of (a) BRCA1 and (b) BRCA2 common founder mutations by location. Putative functional domains are shown in the middle. Regions inferred to be breast cancer cluster region (BCCR) and ovarian cancer cluster region (OCCR) are shown at the bottom.


{kind=link}
Table 1.
Differences of BRCA1/2 mutation prevalence between race and country in ovarian cancer patients.
Table 1.
Differences of BRCA1/2 mutation prevalence between race and country in ovarian cancer patients.
| Country/Population | No. of Cases | BRCA1 | BRCA2 | Ratio |
|---|---|---|---|---|
| BRCA1:BRCA2 | ||||
| Ashkenazi Jews [22] | 840 | 182 (21.7%) | 64 (7.6%) | 2.8:1 |
| USA [29] | 1915 | 182 (8.5%) | 98 (6.3%) | 1.9:1 |
| Canada [30] | 977 | 75 (7.7%) | 54 (5.5%) | 1.4:1 |
| Finland [31] | 233 | 11 (4.7%) | 2 (0.9%) | 5.5:1 |
| Sweden [32] | 161 | 12 (7.5%) | 1 (0.6%) | 12:1 |
| Denmark [33] | 445 | 22 (4.9%) | 4 (0.9%) | 5.5:1 |
| Iceland [39] | 179 | 2 (1.1%) | 10 (5.6%) | 0.5:1 |
| Poland [40] | 309 | 23 (7.4%) | 29 (9.4%) | 0.8:1 |
| Germany [34] | 523 | 81 (15.5%) | 28 (5.4%) | 2.9:1 |
| India [41] | 239 | 37 (15.5%) | 14 (5.9%) | 2.6:1 |
| Turkey [42] | 102 | 10 (9.8%) | 7 (6.9%) | 1.4:1 |
| Pakistan [43] | 120 | 16 (13.3%) | 3 (2.5%) | 5.3:1 |
| Colombia [44] | 100 | 13 (13.0%) | 2 (0.2%) | 6.5:1 |
| Australia [38] | 809 | 70 (8.7%) | 39 (4.8%) | 1.8:1 |
| Japan [35] | 634 | 63 (9.9%) | 30 (4.7%) | 2.1:1 |
| China [36] | 1331 | 228 (17.1%) | 70 (5.3%) | 3.3:1 |
| Korea [37] | 805 | 106 (13.2%) | 51 (6.3%) | 2.1:1 |
Table 2.
Prevalence of germline BRCA mutation by histological type in ovarian cancer patients.
| Histological Classification | USA [29] (n = 1699) | Australia [38] (n = 891) | Germany [34] (n = 462) | Japan [35] (n = 609) | China [36] (n = 1044) | Korea [37] (n = 591) |
|---|---|---|---|---|---|---|
| High-grade serous | 16.0% (240/1498) | 16.6% * (118/709) | 23.2% (94/406) | 28.5% (78/274) | 27.2% * (229/843) | 22.3% (95/426) |
| Low-grade serous | 5.7% (4/70) | N/A * | 5.6% (1/18) | 20.0% (1/5) | N/A * | 19.4% (6/31) |
| Endometrioid | 10.9% (7/64) | 8.4% (10/119) | 13.0% (3/23) | 6.7% (8/120) | 10.8% (7/65) | 13.0% (7/54) |
| Clear cell | 6.9% (4/58) | 6.3% (4/63) | 0.0% (0/6) | 2.1% (4/187) | 7.6% (6/79) | 7.3% (4/55) |
| Mucinous | 0.0% (0/9) | N/A | 0.0% (0/9) | 0.0% (0/19) | 7.0% (4/57) | 5.6% (1/18) |
| Seromucinous | N/A | N/A | N/A | 0.0% (0/4) | N/A | 0.0% (0/7) |
N/A: not applicable; * including either grade.
Table 3.
Common mutation types of BRCA1 or BRCA2 genes in the BIC database.
| BIC Designation | Number of Entries | Exon | HGVS cDNA | HGVS Protein | Mutation Type | Population |
|---|---|---|---|---|---|---|
| BRCA1 | ||||||
| 185delAG | 2038 | 2 | c.66_67delAG | p.Glu23ValfsTer17 | Frameshift | Ashkenazi Jewish |
| 5382insC | 1093 | 20 | c.5263_5264insC | p.Gln1756ProfsTer74 | Frameshift | Ashkenazi Jewish |
| C61G | 239 | 5 | c.181T>G | p.Cys61Gly | Missense | Europe |
| 4184del4 | 144 | 11 | c.4065_4068delTCAA | p.Asn1355LysfsTer10 | Frameshift | Asia |
| R1443X | 136 | 13 | c.4327C>T | p.Arg1443Ter | Nonsense | Europe |
| 3875del4 | 124 | 11 | c.3756_3759delGTCT | p.Ser1253ArgfsTer10 | Frameshift | Europe |
| exon13ins6kb | 111 | 13 | N/A | N/A | Frameshift | N/A |
| E1250X | 98 | 11 | c.3748G>T | p.Glu1250Ter | Nonsense | Europe/Americas |
| Q563X | 94 | 11 | c.1687C>T | p.Gln563Ter | Nonsense | N/A |
| 2800delAA | 81 | 11 | c.2681_2682delAA | p.Lys894ThrfsTer8 | Frameshift | Europe |
| BRCA2 | ||||||
| 6174delT | 1093 | 11 | c.5946_5946delT | p.Ser1982ArgfsTer22 | Frameshift | Ashkenazi Jewish |
| K3326X | 301 | 27 | c.9976A>T | p.Lys3326Ter | Nonsense | N/A |
| 3036del4 | 111 | 11 | c.2808_2811delACAA | p.Ala938ProfsTer21 | Frameshift | Americas |
| 6503delTT | 95 | 11 | c.6275_6276delTT | p.Leu2092ProfsTer7 | Frameshift | Americas/Europe |
| 8765delAG | 76 | 20 | c.8537_8538delAG | p.Glu2846GlyfsTer22 | Frameshift | Americas/Europe |
| 2041insA | 75 | 10 | c.1813_1814insA | p.Asp605GlufsTer2 | Frameshift | Europe |
| 4075delGT | 64 | 11 | c.3847_3848delGT | p.Val1283LysfsTer2 | Frameshift | N/A |
| Y1894X | 62 | 11 | c.5682C>G | p.Tyr1894Ter | Nonsense | N/A |
| 983del4 | 61 | 9 | c.755_758delACAG | p.Asp252ValfsTer24 | Frameshift | N/A |
| R3128X | 50 | 25 | c.9382C>T | p.Arg3128Ter | Nonsense | Europe |
N/A: not applicable.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sekine, M.; Nishino, K.; Enomoto, T. Differences in Ovarian and Other Cancers Risks by Population and BRCA Mutation Location. Genes 2021, 12, 1050. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071050
AMA Style
Sekine M, Nishino K, Enomoto T. Differences in Ovarian and Other Cancers Risks by Population and BRCA Mutation Location. Genes. 2021; 12(7):1050. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071050
Chicago/Turabian StyleSekine, Masayuki, Koji Nishino, and Takayuki Enomoto. 2021. "Differences in Ovarian and Other Cancers Risks by Population and BRCA Mutation Location" Genes 12, no. 7: 1050. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071050
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.