
Whole-Gene Deletions of FZD4 Cause Familial Exudative Vitreoretinopathy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Assessments
2.3. DNA Extraction
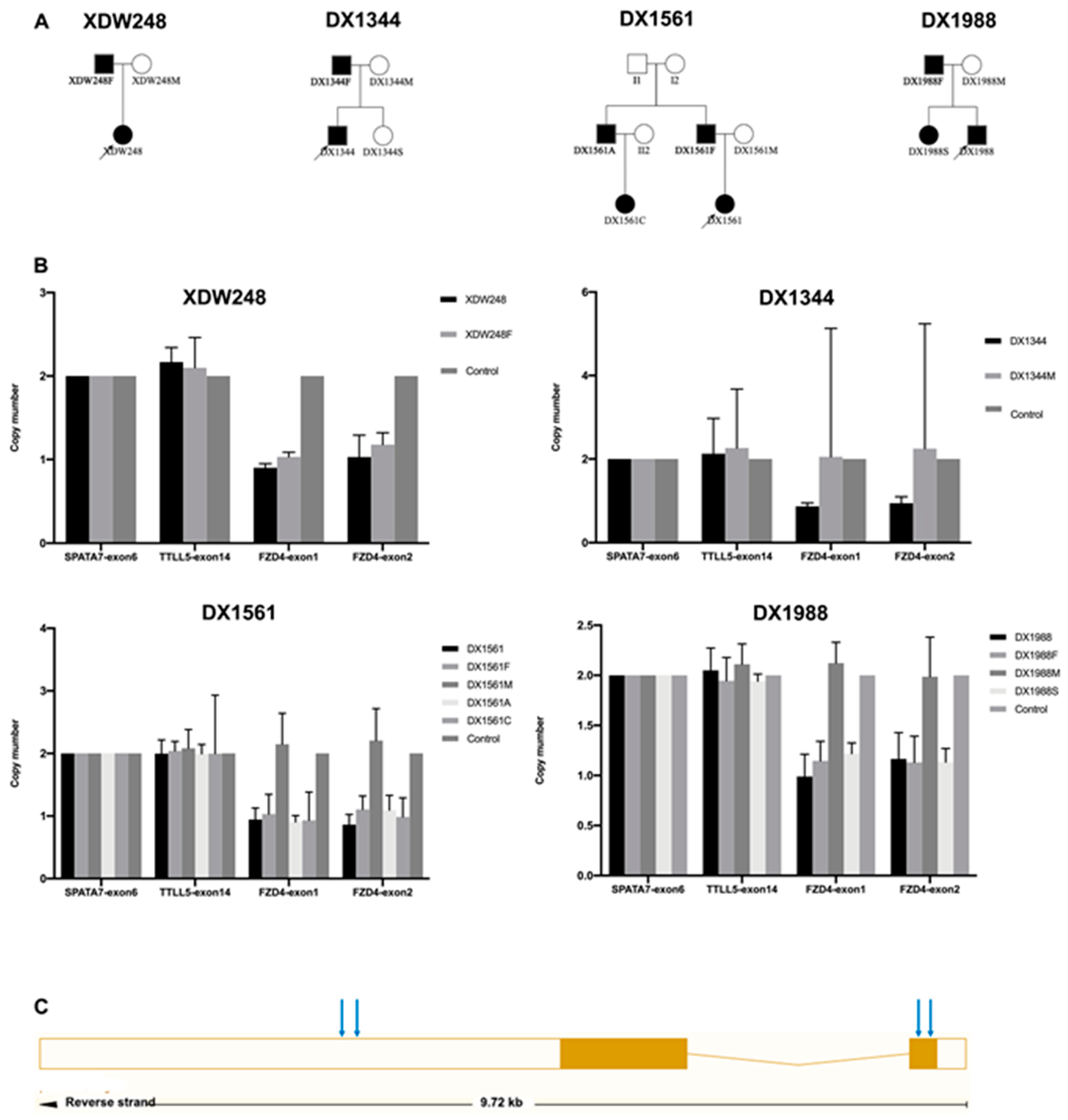
2.4. CNV Assessments
3. Results
3.1. Clinical Features of Probands with FZD4 CNVs
3.2. FZD4 CNVs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Criswick, V.; Schepens, C. Familial Exudative Vitreoretinopathy. Am. J. Ophthalmol. 1969, 68, 578–594. [Google Scholar] [CrossRef]
- Tauqeer, Z.; Yonekawa, Y. Familial Exudative Vitreoretinopathy: Pathophysiology, Diagnosis, and Management. Asia Pac. J. Ophthalmol. 2018, 7, 176–182. [Google Scholar] [CrossRef]
- Poulter, J.A.; Ali, M.; Gilmour, D.F.; Rice, A.; Kondo, H.; Hayashi, K.; Mackey, D.A.; Kearns, L.S.; Ruddle, J.B.; Craig, J.E.; et al. Mutations in TSPAN12 Cause Autosomal-Dominant Familial Exudative Vitreoretinopathy. Am. J. Hum. Genet. 2016, 98, 592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.-Y.; Battinelli, E.; Fielder, A.; Bundey, S.; Sims, K.; Breakefield, X.; Craig, I. A mutation in the Norrie disease gene (NDP) associated with X–linked familial exudative vitreoretinopathy. Nat. Genet. 1993, 5, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, J.; MacDonald, M.; Kaykas, A.; Sheldahl, L.; Zeisler, J.; Dubé, M.-P.; Zhang, L.-H.; Singaraja, R.R.; Guernsey, D.L.; Zheng, B.; et al. Mutant frizzled-4 disrupts retinal angiogenesis in familial exudative vitreoretinopathy. Nat. Genet. 2002, 32, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X.; Ventruto, V.; Trese, M.T.; Shastry, B.S.; Hejtmancik, J. Autosomal Recessive Familial Exudative Vitreoretinopathy Is Associated with Mutations in LRP5. Am. J. Hum. Genet. 2004, 75, 878–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikopoulos, K.; Gilissen, C.; Hoischen, A.; van Nouhuys, C.E.; Boonstra, F.N.; Blokland, E.A.; Arts, P.; Wieskamp, N.; Strom, T.M.; Ayuso, C.; et al. Next-Generation Sequencing of a 40 Mb Linkage Interval Reveals TSPAN12 Mutations in Patients with Familial Exudative Vitreoretinopathy. Am. J. Hum. Genet. 2010, 86, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Collin, R.W.J.; Nikopoulos, K.; Dona, M.; Gilissen, C.; Hoischen, A.; Boonstra, F.N.; Poulter, J.A.; Kondo, H.; Berger, W.; Toomes, C.; et al. ZNF408 is mutated in familial exudative vitreoretinopathy and is crucial for the development of zebrafish retinal vasculature. Proc. Natl. Acad. Sci. USA 2013, 110, 9856–9861. [Google Scholar] [CrossRef] [Green Version]
- Li, J.-K.; Fei, P.; Li, Y.; Huang, Q.-J.; Zhang, Q.; Zhang, X.; Rao, Y.-Q.; Li, J.; Zhao, P. Identification of novel KIF11 mutations in patients with familial exudative vitreoretinopathy and a phenotypic analysis. Sci. Rep. 2016, 6, 26564. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Xiao, X.; Li, S.; Jia, X.; Wang, P.; Zhang, Q. Germline Mutations in CTNNB1 Associated with Syndromic FEVR or Norrie Disease. Investig. Opthalmol. Vis. Sci. 2019, 60, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zhang, X.; Xu, H.; Huang, L.; Bs, S.Z.; Liu, W.; Yang, Y.; Fei, P.; Li, S.; Yang, M.; et al. Exome sequencing revealed Notch ligand JAG1 as a novel candidate gene for familial exudative vitreoretinopathy. Genet. Med. 2019, 22, 77–84. [Google Scholar] [CrossRef]
- Zhu, X.; Yang, M.; Zhao, P.; Li, S.; Zhang, L.; Huang, L.; Huang, Y.; Fei, P.; Yang, Y.; Zhang, S.; et al. Catenin α 1 mutations cause familial exudative vitreoretinopathy by overactivating Norrin/β-catenin signaling. J. Clin. Investig. 2021, 131, 139869. [Google Scholar] [CrossRef]
- Zhu, X.; Sun, K.; Huang, L.; Ma, S.; Hao, F.; Yang, Z.; Sundaresan, P.; Zhu, X. Identification of Novel Mutations in the FZD4 and NDP Genes in Patients with Familial Exudative Vitreoretinopathy in South India. Genet. Test. Mol. Biomarkers 2020, 24, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Salvo, J.S.; Lyubasyuk, V.; Xu, M.; Wang, H.; Wang, F.; Nguyen, D.; Wang, K.; Luo, H.; Wen, C.; Shi, C.; et al. Next-Generation Sequencing and Novel Variant Determination in a Cohort of 92 Familial Exudative Vitreoretinopathy Patients. Investig. Opthalmol. Vis. Sci. 2015, 56, 1937–1946. [Google Scholar] [CrossRef]
- Kirikoshi, H.; Sagara, N.; Koike, J.; Tanaka, K.; Sekihara, H.; Hirai, M.; Katoh, M. Molecular cloning and characterization of human Frizzled-4 on chromosome 11q14-q21. Biochem. Biophys. Res. Commun. 1999, 264, 955–961. [Google Scholar] [CrossRef]
- Seemab, S.; Pervaiz, N.; Zehra, R.; Anwar, S.; Bao, Y.; Abbasi, A.A. Molecular evolutionary and structural analysis of familial exudative vitreoretinopathy associated FZD4 gene. BMC Evol. Biol. 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, M.; Ding, X.; Li, J.; Hu, A.; Yuan, M.; Yang, Y.; Zhan, Z.; Li, Z.; Lu, L. Novel mutations in FZD4 and phenotype–genotype correlation in Chinese patients with familial exudative vitreoretinopathy. Mol. Vis. 2016, 22, 917–932. [Google Scholar] [PubMed]
- Zhao, M.; Wang, Q.; Wang, Q.; Jia, P.; Zhao, Z. Computational tools for copy number variation (CNV) detection using next-generation sequencing data: Features and perspectives. BMC Bioinform. 2013, 14, S1. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Liu, X.; Zhang, A.; Chen, H.; Huo, Q.; Li, W.; Ye, R.; Chen, Z.; Liang, L.; Liu, Q.A.; et al. The correlation of copy number variations with longevity in a genome-wide association study of Han Chinese. Aging 2018, 10, 1206–1222. [Google Scholar] [CrossRef] [Green Version]
- Seo, S.H.; Kim, M.J.; Park, S.W.; Yu, Y.S.; Song, J.Y.; Cho, S.I.; Ahn, J.H.; Oh, Y.H.; Lee, J.-S.; Seong, M.-W. Large Deletions of TSPAN12 Cause Familial Exudative Vitreoretinopathy (FEVR). Investig. Opthalmol. Vis. Sci. 2016, 57, 6902. [Google Scholar] [CrossRef] [Green Version]
- Malvezzi, J.V.; Magalhaes, I.H.; Costa, S.S.; A Otto, P.; Rosenberg, C.; Bertola, D.R.; Fernandes, W.L.; Vianna-Morgante, A.M.; Krepischi, A.C. KIF11 microdeletion is associated with microcephaly, chorioretinopathy and intellectual disability. Hum. Genome Var. 2018, 5, 18010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narumi, S.; Numakura, C.; Shiihara, T.; Seiwa, C.; Nozaki, Y.; Yamagata, T.; Momoi, M.Y.; Watanabe, Y.; Yoshino, M.; Matsuishi, T.; et al. Various types of LRP5 mutations in four patients with osteoporosis-pseudoglioma syndrome: Identification of a 7.2-kb microdeletion using oligonucleotide tiling microarray. Am. J. Med. Genet. Part A 2009, 152A, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Schuback, D.E.; Chen, Z.Y.; Craig, I.W.; Breakefield, X.O.; Sims, K.B. Mutations in the Norrie disease gene. Hum. Mutat. 1995, 5, 285–292. [Google Scholar] [CrossRef]
- Hehir-Kwa, J.Y.; Tops, B.; Kemmeren, P. The clinical implementation of copy number detection in the age of next-generation sequencing. Expert Rev. Mol. Diagn. 2018, 18, 907–915. [Google Scholar] [CrossRef]
- Kashani, A.H.; Brown, K.T.; Chang, E.; Drenser, K.A.; Capone, A.; Trese, M.T. Diversity of Retinal Vascular Anomalies in Patients with Familial Exudative Vitreoretinopathy. Ophthalmology 2014, 121, 2220–2227. [Google Scholar] [CrossRef]
- Ranchod, T.M.; Ho, L.Y.; Drenser, K.A.; Capone, A.; Trese, M.T. Clinical Presentation of Familial Exudative Vitreoretinopathy. Ophthalmology 2011, 118, 2070–2075. [Google Scholar] [CrossRef]
- Pendergast, S.D.; Trese, M.T. Familial exudative vitreoretinopathy. Results of surgical management. Ophthalmology 1998, 105, 1015–1023. [Google Scholar] [CrossRef]
- Chen, C.; Sun, L.; Li, S.; Huang, L.; Zhang, T.; Wang, Z.; Yu, B.; Luo, X.; Ding, X. Novel variants in familial exudative vitreoretinopathy patients with KIF11 mutations and the Genotype–Phenotype correlation. Exp. Eye Res. 2020, 199, 108165. [Google Scholar] [CrossRef]
- Chen, Y.; Zhao, L.; Wang, Y.; Cao, M.; Gelowani, V.; Xu, M.; Agrawal, S.A.; Li, Y.; Daiger, S.P.; Gibbs, R.; et al. SeqCNV: A novel method for identification of copy number variations in targeted next-generation sequencing data. BMC Bioinform. 2017, 18, 147. [Google Scholar] [CrossRef] [Green Version]
- Schouten, J.P.; McElgunn, C.J.; Waaijer, R.; Zwijnenburg, D.; Diepvens, F.; Pals, G. Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acids Res. 2002, 30, e57. [Google Scholar] [CrossRef] [Green Version]
- Li, J.-K.; Li, Y.; Zhang, X.; Chen, C.-L.; Rao, Y.-Q.; Fei, P.; Zhang, Q.; Zhao, P.; Li, J. Spectrum of Variants in 389 Chinese Probands With Familial Exudative Vitreoretinopathy. Investig. Opthalmol. Vis. Sci. 2018, 59, 5368–5381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Chen, C.; Sun, L.; Zhang, A.; Liu, C.; Huang, L.; Ding, X. Symmetry of folds in FEVR: A genotype-phenotype correlation study. Exp. Eye Res. 2019, 186, 107720. [Google Scholar] [CrossRef] [PubMed]
- Ellingford, J.M.; Horn, B.; Campbell, C.; Arno, G.; Barton, S.; Tate, C.; Bhaskar, S.; I Sergouniotis, P.; Taylor, R.L.; Carss, K.; et al. Assessment of the incorporation of CNV surveillance into gene panel next-generation sequencing testing for inherited retinal diseases. J. Med. Genet. 2017, 55, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Consugar, M.B.; Navarro-Gomez, D.; Place, E.M.; Bujakowska, K.M.; Sousa, M.E.; Fonseca-Kelly, Z.D.; Taub, D.; Janessian, M.; Wang, D.Y.; Au, E.D.; et al. Panel-based genetic diagnostic testing for inherited eye diseases is highly accurate and reproducible, and more sensitive for variant detection, than exome sequencing. Genet. Med. 2015, 17, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Loeber, G.; Maurer-Fogy, I.; Schwendenwein, R. Purification, cDNA cloning and heterologous expression of the human mitochondrial NADP+-dependent malic enzyme. Biochem. J. 1994, 304, 687–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyakoshi, K.; Murphy, M.J.; Yeoman, R.R.; Mitra, S.; Dubay, C.J.; Hennebold, J.D. The Identification of Novel Ovarian Proteases Through the Use of Genomic and Bioinformatic Methodologies1. Biol. Reprod. 2006, 75, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Scheideler, M.; Elabd, C.; Zaragosi, L.-E.; Chiellini, C.; Hackl, H.; Sanchez-Cabo, F.; Yadav, S.; Duszka, K.; Friedl, G.; Papak, C.; et al. Comparative transcriptomics of human multipotent stem cells during adipogenesis and osteoblastogenesis. BMC Genom. 2008, 9, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Family ID | XDW248 | DX1344 | DX1561 | DX1988 | |
|---|---|---|---|---|---|
| Sex | Female | Male | Female | Male | |
| At diagnosis | Age (yrs.) | 12 | 4 | 1 | 1 |
| Stage (OD/OS) † | 1/4 | 1/4 | 1/4 | 1/4 | |
| Retinal folds (OD/OS) | no/yes | no/yes | no/yes | no/yes | |
| At last follow-up | Age (yrs.) | 14 | 36 | 4 | 3 |
| Stage (OD/OS) | 4/4 | 1/4 | 1/4 | 1/4 | |
| Refractive Error (Spherical Equivalent, OD/OS) | −13.38; NLP § | NA | +0.25; −16.75 | NA/NA | |
| BCVA ‡ | 0.2/NLP | 0.2/NLP | NA/NA | NA/NA | |
| Others | OD retinal detachment | OS glaucoma | NO | NO | |
| Inherited from | Paternal | Paternal | paternal | paternal | |
| Stage of affected parent (OD/OS) | 2/2 | NA/NA | 1/1 | 1/1 |
| Mutations | CNVs | Missense | p |
|---|---|---|---|
| Age (yrs. M ± SD) | 5.00 ± 6.16 | 9.14 ± 12.50 | 0.857 |
| Gender (Male: female) | 2:2 | 22:8 | 0.564 |
| Stage * | 1.000 | ||
| 1 | 0 | 2 | |
| 2 | 0 | 4 | |
| 3 | 0 | 4 | |
| 4 | 4 | 17 | |
| 5 | 0 | 3 | |
| Total patients | 4 | 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.; Lu, J.; Zhang, L.; Zhang, Z.; Sun, L.; Li, S.; Zhang, T.; Chen, L.; Cao, L.; Ding, X. Whole-Gene Deletions of FZD4 Cause Familial Exudative Vitreoretinopathy. Genes 2021, 12, 980. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070980
Huang L, Lu J, Zhang L, Zhang Z, Sun L, Li S, Zhang T, Chen L, Cao L, Ding X. Whole-Gene Deletions of FZD4 Cause Familial Exudative Vitreoretinopathy. Genes. 2021; 12(7):980. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070980
Chicago/Turabian StyleHuang, Li, Jinglin Lu, Linyan Zhang, Zhaotian Zhang, Limei Sun, Songshan Li, Ting Zhang, Limei Chen, Liming Cao, and Xiaoyan Ding. 2021. "Whole-Gene Deletions of FZD4 Cause Familial Exudative Vitreoretinopathy" Genes 12, no. 7: 980. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12070980