
Oncogenic Role of Connective Tissue Growth Factor Is Associated with Canonical TGF-β Cascade in Colorectal Cancer

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Clinicopathological Data
2.3. RNA Isolation and cDNA Synthesis
2.4. Real Time PCR Analysis
2.5. Immunohistochemistry and Evaluation of Staining
2.6. Statistical Analysis
3. Results
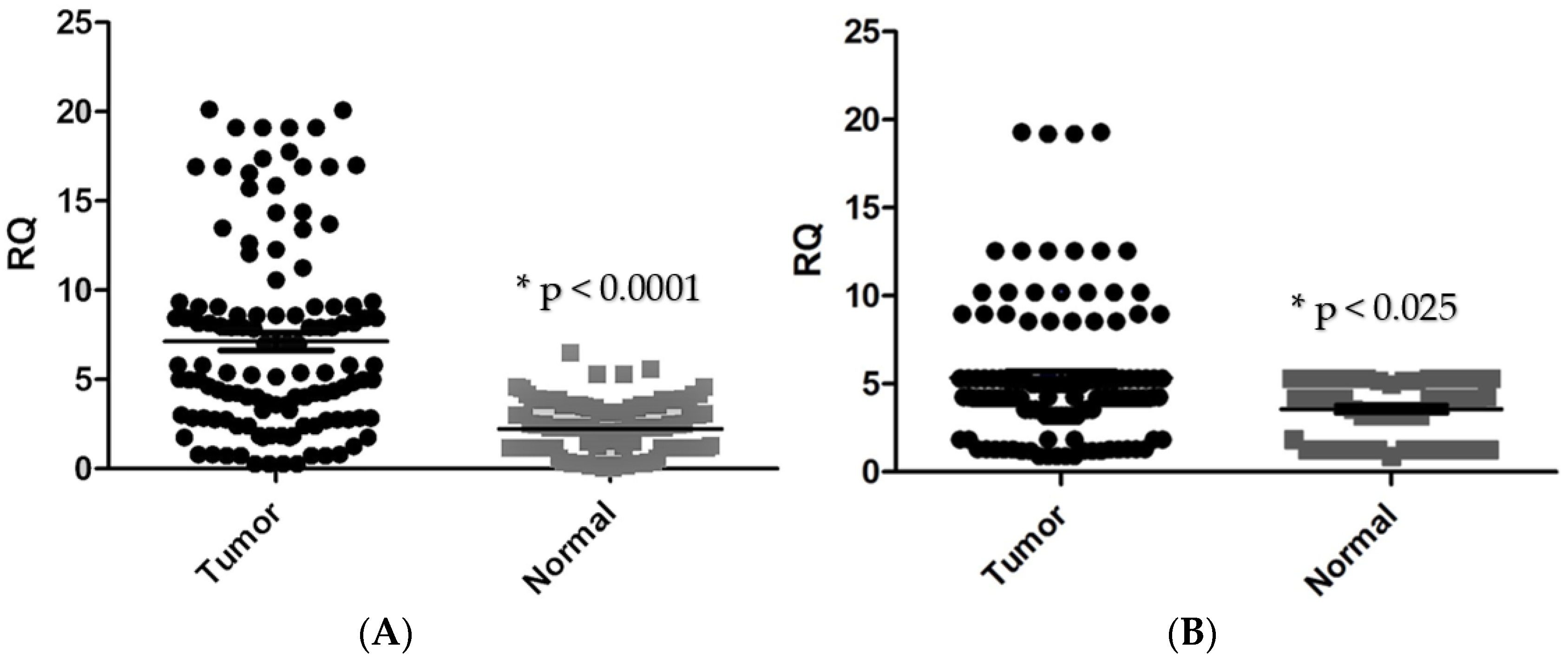
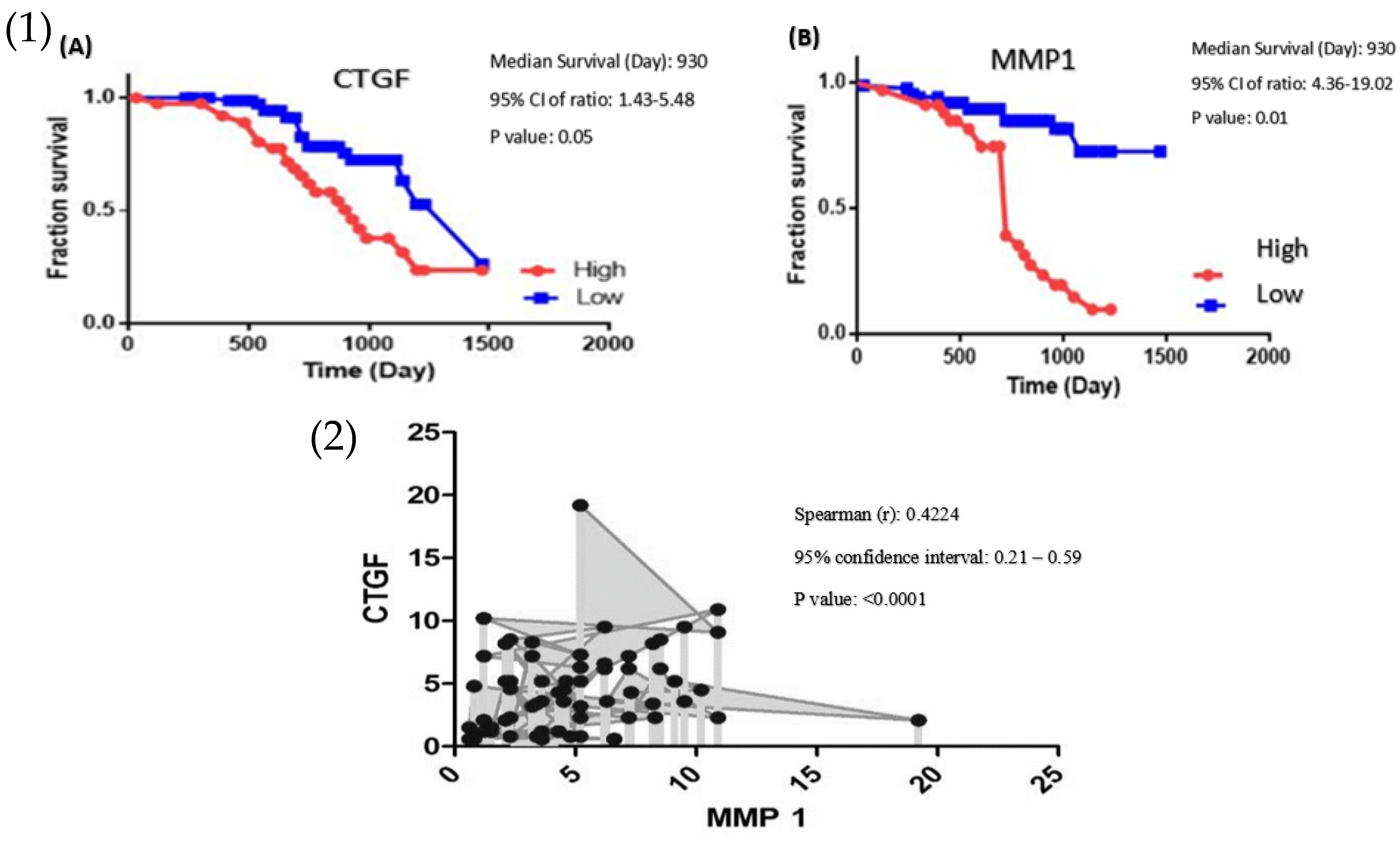
3.1. High Expression of CTGF Contributes to Poor Prognosis in Colorectal Cancer Patients
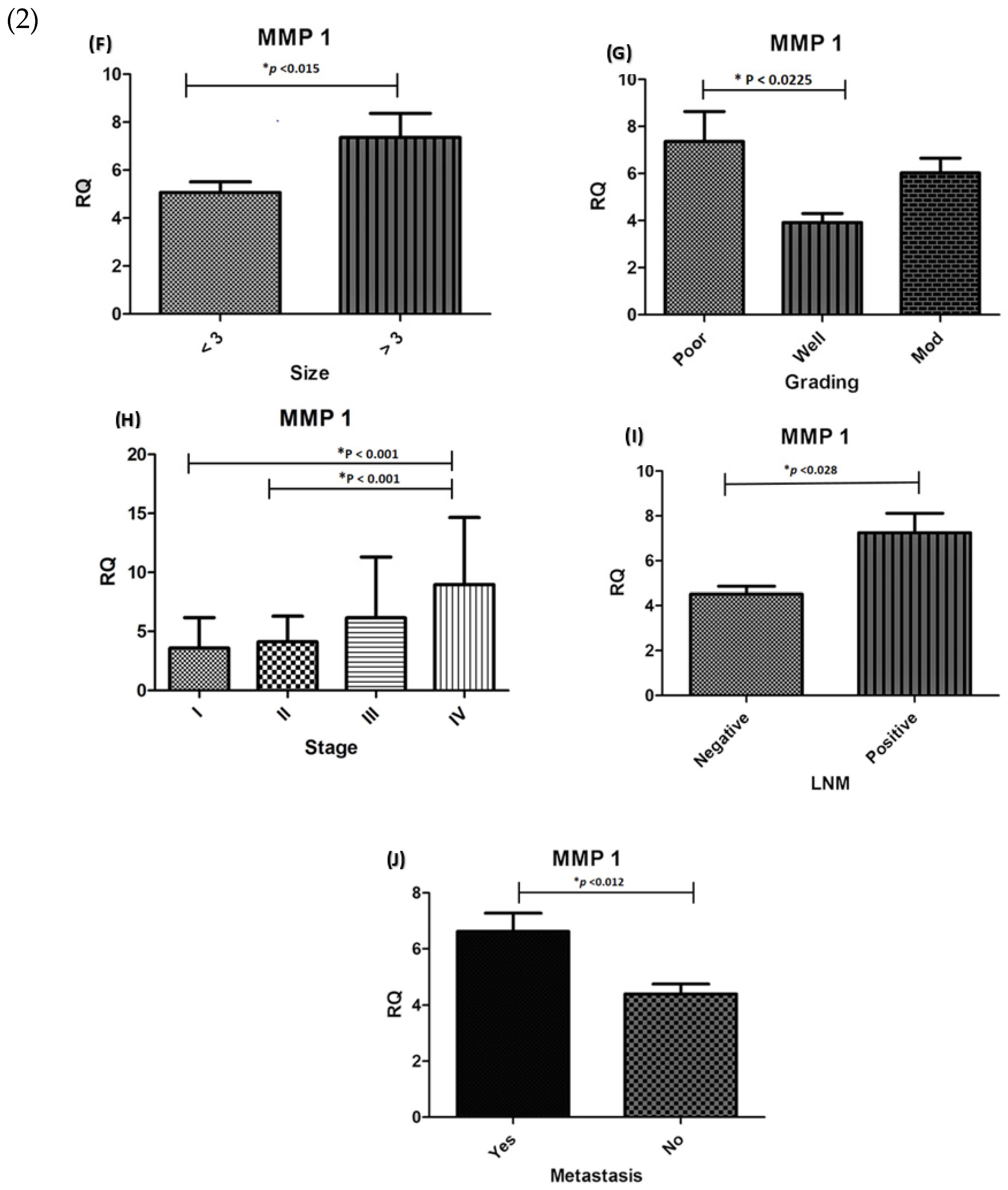
3.2. MMP-1 Is Overexpressed in Colorectal Carcinoma Samples and Is Related to Poor Prognosis in CRC Patients
3.3. CTGF Increases MMP-1 Expression in Colorectal Carcinomas
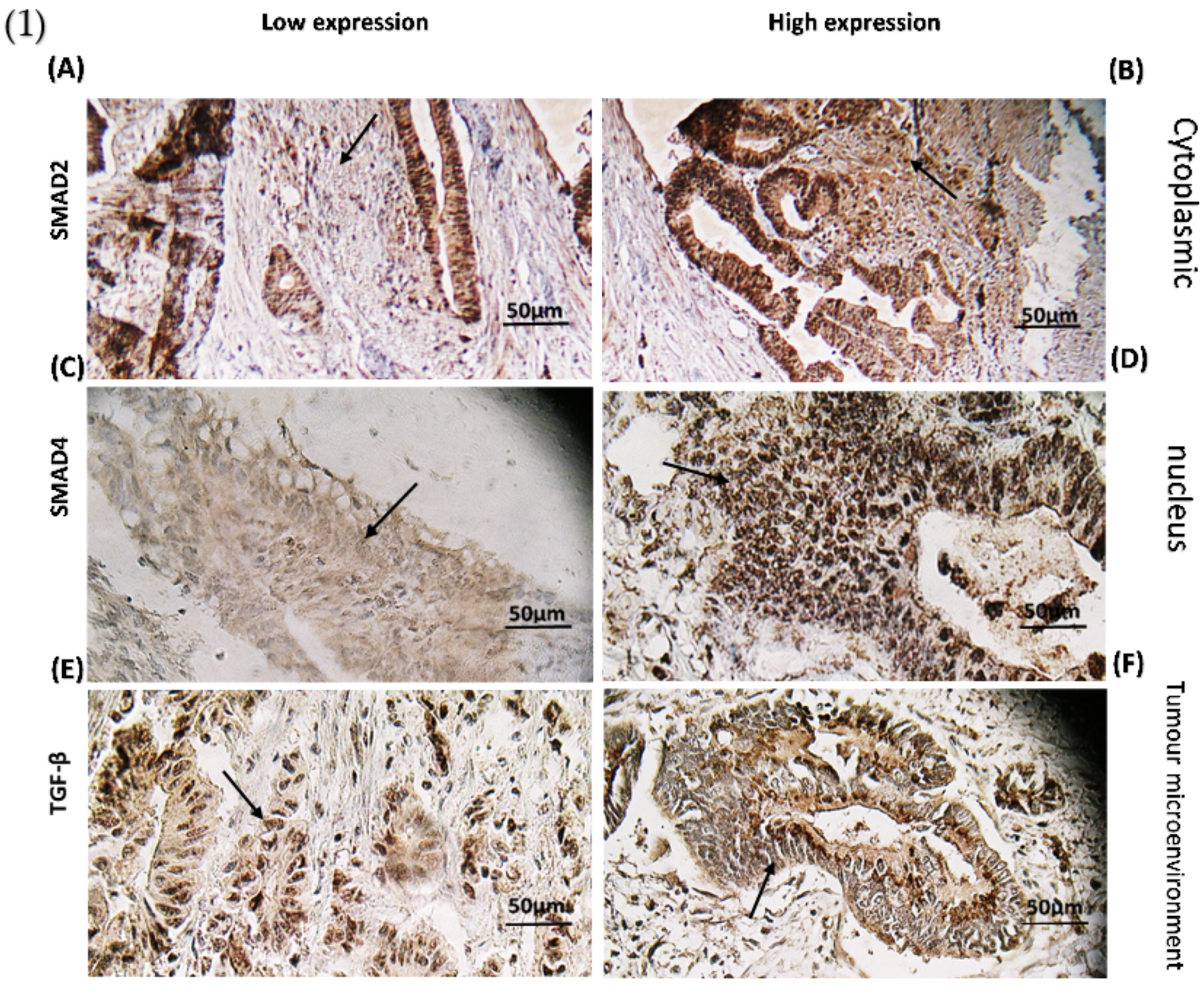
3.4. TGF-β Signalling Pathway Has a Multifaceted Role in Colorectal Cancer
3.5. The Effect of CTGF and MMP-1 mRNA Expression on TGF-β Protein Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Prz. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, A.; Woodhouse, M.; Gupta, S. Colorectal cancer is a leading cause of cancer incidence and mortality among adults younger than 50 years in the USA: A SEER-based analysis with comparison to other young-onset cancers. J. Investig. Med. 2017, 65, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, V. TGF-β Signaling in Cancer. J. Cell. Biochem. 2016, 117, 1279–1287. [Google Scholar] [CrossRef]
- Ji, Q.; Liu, X.; Han, Z.; Zhou, L.; Sui, H.; Yan, L.; Jiang, H.; Ren, J.; Cai, J.; Li, Q. Resveratrol suppresses epithelial-to-mesenchymal transition in colorectal cancer through TGF-β1/Smads signaling pathway mediated Snail/E-cadherin expression. BMC Cancer 2015, 15, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soleimani, A.; Pashirzad, M.; Avan, A.; Ferns, G.A.; Khazaei, M.; Hassanian, S.M. Role of the transforming growth factor-β signaling pathway in the pathogenesis of colorectal cancer. J. Cell. Biochem. 2019, 120, 8899–8907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, L.H.; Likhter, M.; Jogunoori, W.; Belkin, M.; Ohshiro, K.; Mishra, L. TGF-β signaling in liver and gastrointestinal cancers. Cancer Lett. 2016, 379, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheruku, H.; Mohamedali, A.; Cantor, D.; Tan, S.H.; Nice, E.; Baker, M. Transforming Growth Factor-β, MAPK and Wnt Signaling Interactions in Colorectal Cancer. EuPA Open Proteom. 2015, 8, 104–115. [Google Scholar] [CrossRef] [Green Version]
- Wells, J.E.; Howlett, M.; Cole, C.H.; Kees, U.R. Deregulated expression of connective tissue growth factor (CTGF/CCN2) is linked to poor outcome in human cancer. Int. J. Cancer 2015, 137, 504–511. [Google Scholar] [CrossRef]
- Inman, G.J. Switching TGFβ from a tumor suppressor to a tumor promoter. Curr. Opin. Genet. Dev. 2011, 21, 93–99. [Google Scholar] [CrossRef]
- Ubink, I.; Verhaar, E.R.; Kranenburg, O.; Goldschmeding, R. A potential role for CCN2/CTGF in aggressive colorectal cancer. J. Cell Commun. Signal. 2016, 10, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Shirin, M.; Madadi, S.; Peyravian, N.; Pezeshkian, Z.; Rejali, L.; Hosseini, M.; Moradi, A.; Khanabadi, B.; Sherkat, G.; Aghdaei, H.A.; et al. A linkage between effectual genes in progression of CRC through canonical and non-canonical TGF-β signaling pathways. Med. Oncol. 2022, 39, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Conlon, G.A.; Murray, G.I. Recent advances in understanding the roles of matrix metalloproteinases in tumour invasion and metastasis. J. Pathol. 2019, 247, 629–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, A.H.; Raufman, J.-P.; Xie, G. The role of matrix metalloproteinases in colorectal cancer. Cancers 2014, 6, 366–375. [Google Scholar] [CrossRef]
- Bendardaf, R.; Buhmeida, A.; Ristamäki, R.; Syrjänen, K.; Pyrhönen, S. MMP-1 (collagenase-1) expression in primary colorectal cancer and its metastases. Scand. J. Gastroenterol. 2007, 42, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zheng, J.; Yu, J.; Wu, Y.; Guo, J.; Xu, Z.; Sun, X. Knockdown of MMP-1 inhibits the progression of colorectal cancer by suppressing the PI3K/Akt/c-myc signaling pathway and EMT. Oncol. Rep. 2020, 43, 1103–1112. [Google Scholar] [CrossRef]
- Lyall, M.S.; Dundas, S.R.; Curran, S.; Murray, G.I. Profiling markers of prognosis in colorectal cancer. Clin. Cancer Res. 2006, 12, 1184–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.W.; Ko, Y.T.; Kim, N.K.; Chung, H.C.; Min, B.S.; Lee, K.Y.; Park, J.-P.; Kim, H. A comparative study of protein expression in primary colorectal cancer and synchronous hepatic metastases: The significance of matrix metalloproteinase-1 expression as a predictor of liver metastasis. Scand. J. Gastroenterol. 2010, 45, 217–225. [Google Scholar] [CrossRef]
- Wagenaar-Miller, R.A.; Gorden, L.; Matrisian, L.M. Matrix metalloproteinases in colorectal cancer: Is it worth talking about? Cancer Metastasis Rev. 2004, 23, 119–135. [Google Scholar] [CrossRef]
- Peyravian, N.; Larki, P.; Gharib, E.; Nazemalhosseini-Mojarad, E.; Anaraki, F.; Young, C.; McClellan, J.; Bonab, M.A.; Asadzadeh-Aghdaei, H.; Zali, M.R. The Application of Gene Expression Profiling in Predictions of Occult Lymph Node Metastasis in Colorectal Cancer Patients. Biomedicines 2018, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, N.M.; Upton, M.; Rojas, A.; Washington, M.K.; Lin, L.; Chytil, A.; Sozmen, E.G.; Madison, B.B.; Pozzi, A.; Moon, R.T.; et al. Transforming growth factor beta receptor type II inactivation induces the malignant transformation of intestinal neoplasms initiated by Apc mutation. Cancer Res. 2006, 66, 9837–9844. [Google Scholar] [CrossRef] [Green Version]
- Itatani, Y.; Kawada, K.; Fujishita, T.; Kakizaki, F.; Hirai, H.; Matsumoto, T.; Iwamoto, M.; Inamoto, S.; Hatano, E.; Hasegawa, S.; et al. Loss of SMAD4 from colorectal cancer cells promotes CCL15 expression to recruit CCR1+ myeloid cells and facilitate liver metastasis. Gastroenterology 2013, 145, 1064–1075.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramamoorthi, G.; Sivalingam, N. Molecular mechanism of TGF-β signaling pathway in colon carcinogenesis and status of curcumin as chemopreventive strategy. Tumor Biol. 2014, 35, 7295–7305. [Google Scholar] [CrossRef] [PubMed]
- Kumar Pandurangan, A.; Divya, T.; Kumar, K.; Dineshbabu, V.; Velavan, B.; Sudhandiran, G. Colorectal carcinogenesis: Insights into the cell death and signal transduction pathways: A review. World J. Gastrointest. Oncol. 2018, 10, 244. [Google Scholar]
- Zhao, M.; Mishra, L.; Deng, C.X. The role of TGF-β/SMAD4 signaling in cancer. Int. J. Biol. Sci. 2018, 14, 111–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samanta, D.; Datta, P.K. Alterations in the Smad pathway in human cancers. Front. Biosci. 2012, 17, 1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sameer, A.S.; Abdullah, S.; Syeed, N.; Siddiqi, M.A. Colorectal cancer, TGF-signaling and SMADs. Int. J. Genet. Mol. Biol. 2010, 2, 101–111. [Google Scholar]
- Jung, B.; Staudacher, J.J.; Beauchamp, D. Transforming Growth Factor β Superfamily Signaling in Development of Colorectal Cancer. Gastroenterology 2017, 152, 36–52. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.X.; Cao, Z.B.; He, T.T.; Huang, T.; Xiang, C.L.; Liu, Y. TGFβ1 is essential for MSCs-CAFs differentiation and promotes HCT116 cells migration and invasion via JAK/STAT3 signaling. Onco Targets Ther. 2019, 12, 5323–5334. [Google Scholar] [CrossRef] [Green Version]
- Otegbeye, F.; Ojo, E.; Moreton, S.; Mackowski, N.; Lee, D.A.; de Lima, M.; Wald, D.N. Inhibiting TGF-beta signaling preserves the function of highly activated, in vitro expanded natural killer cells in AML and colon cancer models. PLoS ONE. 2018, 13, e0191358. [Google Scholar]
- Huynh, L.K.; Hipolito, C.J.; Ten Dijke, P. A Perspective on the Development of TGF-β Inhibitors for Cancer Treatment. Biomolecules 2019, 9, 743. [Google Scholar] [CrossRef] [Green Version]
- Gachpazan, M.; Kashani, H.; Hassanian, S.M.; Khazaei, M.; Khorrami, S.; Ferns, G.A.; Avan, A. Therapeutic potential of targeting transforming growth factor-beta in colorectal cancer: Rational and progress. Curr. Pharm. Des. 2019, 25, 4085–4089. [Google Scholar] [CrossRef] [PubMed]
- Lampropoulos, P.; Zizi-Sermpetzoglou, A.; Rizos, S.; Kostakis, A.; Nikiteas, N.; Papavassiliou, A.G. Prognostic significance of transforming growth factor beta (TGF-β) signaling axis molecules and E-cadherin in colorectal cancer. Tumour Biol. 2012, 33, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Liu, Z.; Tan, J.; Dong, H.; Zhang, X. Multispectral imaging reveals hyperactive TGF-β signaling in colorectal cancer. Cancer Biol. Ther. 2018, 19, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fessler, E.; Drost, J.; Van Hooff, S.R.; Linnekamp, J.F.; Wang, X.; Jansen, M.; De Sousa E Melo, F.; Prasetyanti, P.R.; Ijspeert, J.E.; Franitza, M.; et al. TGFβ signaling directs serrated adenomas to the mesenchymal colorectal cancer subtype. EMBO Mol. Med. 2016, 8, 745–760. [Google Scholar] [CrossRef]
- Parada, C.; Li, J.; Iwata, J.; Suzuki, A.; Chai, Y. CTGF mediates Smad-dependent transforming growth factor β signaling to regulate mesenchymal cell proliferation during palate development. Mol. Cell. Biol. 2013, 33, 3482–3493. [Google Scholar] [CrossRef] [Green Version]
- Ihn, H. Pathogenesis of fibrosis: Role of TGF-beta and CTGF. Curr. Opin. Rheumatol. 2002, 14, 681–685. [Google Scholar] [CrossRef]
- Zhang, S.D.; McCrudden, C.M.; Yuen, H.F.; Leung, K.L.; Hong, W.J.; Kwok, H.F. Association between the expression levels of TAZ, AXL and CTGF and clinicopathological parameters in patients with colon cancer. Oncol. Lett. 2016, 11, 1223–1229. [Google Scholar] [CrossRef] [Green Version]
- Lau, L.F.; Lam, S.C. The CCN family of angiogenic regulators: The integrin connection. Exp. Cell Res. 1999, 248, 44–57. [Google Scholar] [CrossRef]
- Ladwa, R.; Pringle, H.; Kumar, R.; West, K. Expression of CTGF and Cyr61 in colorectal cancer. J. Clin. Pathol. 2011, 64, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Sunami, E.; Tsuno, N.; Osada, T.; Saito, S.; Kitayama, J.; Tomozawa, S.; Tsuruo, T.; Shibata, Y.; Muto, T.; Nagawa, H. MMP-1 is a prognostic marker for hematogenous metastasis of colorectal cancer. Oncology 2000, 5, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.Y.; Chang, C.C.; Prakash, E.; Kuo, M.L. Connective tissue growth factor (CTGF) and cancer progression. J. Biomed. Sci. 2008, 15, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.; O’Kelly, J.; Lu, D.; Leiter, A.; Sohn, J.; Yin, D.; Karlan, B.; Vadgama, J.; Lyons, K.M.; Koeffler, H.P. Expression of connective tissue growth factor (CTGF/CCN2) in breast cancer cells is associated with increased migration and angiogenesis. Int. J. Oncol. 2011, 38, 1741–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, S.J.; Doecke, J.D.; Ghazawi, I.; Yang, J.; Griffiths, L.R.; Spring, K.; Ralph, S.J.; Mellick, A.S. Novel STAT binding elements mediate IL-6 regulation of MMP-1 and MMP-3. Sci. Rep. 2017, 7, 8526. [Google Scholar] [CrossRef]
- Quintero-Fabián, S.; Arreola, R.; Becerril-Villanueva, E.; Torres-Romero, J.C.; Arana-Argáez, V.; Lara-Riegos, J.; Ramírez-Camacho, M.A.; Alvarez-Sánchez, M.E. Role of Matrix Metalloproteinases in Angiogenesis and Cancer. Front. Oncol. 2019, 9, 1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, Y.-C.; Sheu, B.-S. Matrix metalloproteinases and their inhibitors in the gastrointestinal cancers: Current knowledge and clinical potential. Met. Med. 2014, 1, 3–13. [Google Scholar]
- Langenskiöld, M.; Ivarsson, M.L.; Holmdahl, L.; Falk, P.; Kåbjörn-Gustafsson, C.; Angenete, E. Intestinal mucosal MMP-1—A prognostic factor in colon cancer. Scand. J. Gastroenterol. 2013, 48, 563–569. [Google Scholar] [CrossRef]
- Shiozawa, J.; Ito, M.; Nakayama, T.; Nakashima, M.; Kohno, S.; Sekine, I. Expression of matrix metalloproteinase-1 in human colorectal carcinoma. Mod. Pathol. 2000, 13, 925–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsson, A.; Falk, P.; Angenete, E.; Hjalmarsson, C.; Ivarsson, M.-L. Plasma MMP-1 Expression as a Prognostic Factor in Colon Cancer. J. Surg. Res. 2021, 266, 254–260. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Cases | % |
|---|---|---|
| Gender: | ||
| Male | 77 | (63.1) |
| Female | 45 | (36.9) |
| Age (years): | ||
| ≤60 years | 55 | (45.1) |
| >60 years | 67 | (54.9) |
| Histological grade: | ||
| Grade I (well differentiated) | 35 | (28.67) |
| Grade II (moderately differentiated) | 70 | (57.40) |
| Grade III (poorly differentiated) | 17 | (13.93) |
| Pathological stage: | ||
| Stage I | 23 | (18.9) |
| Stage II | 47 | (38.5) |
| Stage III | 41 | (33.6) |
| Stage VI | 11 | (9.0) |
| Lymph node involvement: | ||
| No | 48 | (39.3) |
| Yes | 74 | (60.7) |
| Tumor size (cm) | ||
| ≤3 cm | 93 | (76.2) |
| >3 cm | 29 | (23.8) |
| Localization: | ||
| Right colon | 31 | (25.4) |
| Left colon | 91 | (74.6) |
| Status of patient: | ||
| Alive | 83 | (68.0) |
| Dead | 39 | (32.0) |
| Chemotherapy (After Surgery) | ||
| Yes | 97 | (79.5) |
| No | 25 | (20.5) |
| Gene ID | Primer | Sequence |
|---|---|---|
| 1490 | CTGF | 5′-CTGGAAGAGAACATTAAGAAGGGC-3′ 5′-CGGTATGTCTTCATGCTGGTGC-3′ |
| 4312 | MMP1 | 5′-GGGAATAAGTACTGGGCTGTTC-3′ 5′-GTCCTTGGGGTATCCGTGTAG-3′ |
| 567 | β2-micro globulin(B2M) | 5′-TGCTGTCTCCATGTTTAGTGTATCT-3′ 5′-TCTCTGCTCCCCACCTCTAAGT-3′ |
| Clinicopathological Features | TGF-β Signalling Pathway (%) | p-Value | ||
|---|---|---|---|---|
| Low | High | |||
| Gender: | Male | 51 (60.7) | 26 (68.4) | 0.544 |
| Female | 33 (39.3) | 45 (36.9) | ||
| Age | ≤60 years | 36 (42.9) | 19 (50.0) | 0.544 |
| >60 years | 48 (57.1) | 19 (50.0) | ||
| Tumour size | ≤3 cm | 65 (77.4) | 28 (73.3) | 0.653 |
| >3 cm | 19 (22.6) | 10 (26.3) | ||
| Location | Right colon | 22 (26.2) | 9 (23.7) | 0.826 |
| Left colon | 62 (73.8) | 29 (76.3) | ||
| Differentiation: | Well | 28 (33.3) | 12 (31.6) | 0.847 |
| Moderate | 47 (56.0) | 23 (60.5) | ||
| Poor | 9 (10.7) | 3 (2.5) | ||
| Pathological stage: | Stage I | 19 (22.6) | 4 (10.5) | <0.001 * |
| Stage II | 41 (48.8) | 6 (15.8) | ||
| Stage III | 19 (22.6) | 22 (57.9) | ||
| Stage VI | 5 (6.0) | 6 (15.8) | ||
| Lymph node metastasis | No | 23 (27.4) | 25 (65.8) | <0.001 * |
| Yes | 61 (72.6) | 13 (34.2) | ||
| Metastasis | Yes | 19 (22.6) | 33 (86.8) | <0.001 * |
| No | 65 (77.4) | 5 (13.2) | ||
| Family History | Yes | 29 (34.5) | 12 (31.6) | 0.837 |
| No | 55 (65.5) | 26 (68.4) | ||
| Recurrence | Yes | 11 (13.1) | 17 (44.7) | <0.001 * |
| No | 73 (86.9) | 21 (55.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini, S.; Rejali, L.; Pezeshkian, Z.; Malekian, M.; Fatemi, N.; Peyravian, N.; Hadizadeh, M.; Mohsenifar, Z.; Khanabadi, B.; Farzam, M.; et al. Oncogenic Role of Connective Tissue Growth Factor Is Associated with Canonical TGF-β Cascade in Colorectal Cancer. Genes 2022, 13, 689. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13040689
Hosseini S, Rejali L, Pezeshkian Z, Malekian M, Fatemi N, Peyravian N, Hadizadeh M, Mohsenifar Z, Khanabadi B, Farzam M, et al. Oncogenic Role of Connective Tissue Growth Factor Is Associated with Canonical TGF-β Cascade in Colorectal Cancer. Genes. 2022; 13(4):689. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13040689
Chicago/Turabian StyleHosseini, Shaghayegh, Leili Rejali, Zahra Pezeshkian, Mahtash Malekian, Nayeralsadat Fatemi, Noshad Peyravian, Mahrooyeh Hadizadeh, Zhaleh Mohsenifar, Binazir Khanabadi, Maral Farzam, and et al. 2022. "Oncogenic Role of Connective Tissue Growth Factor Is Associated with Canonical TGF-β Cascade in Colorectal Cancer" Genes 13, no. 4: 689. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13040689