
Polymorphisms of the ELANE Gene Promoter Region in End-Stage Chronic Kidney Disease Patients

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
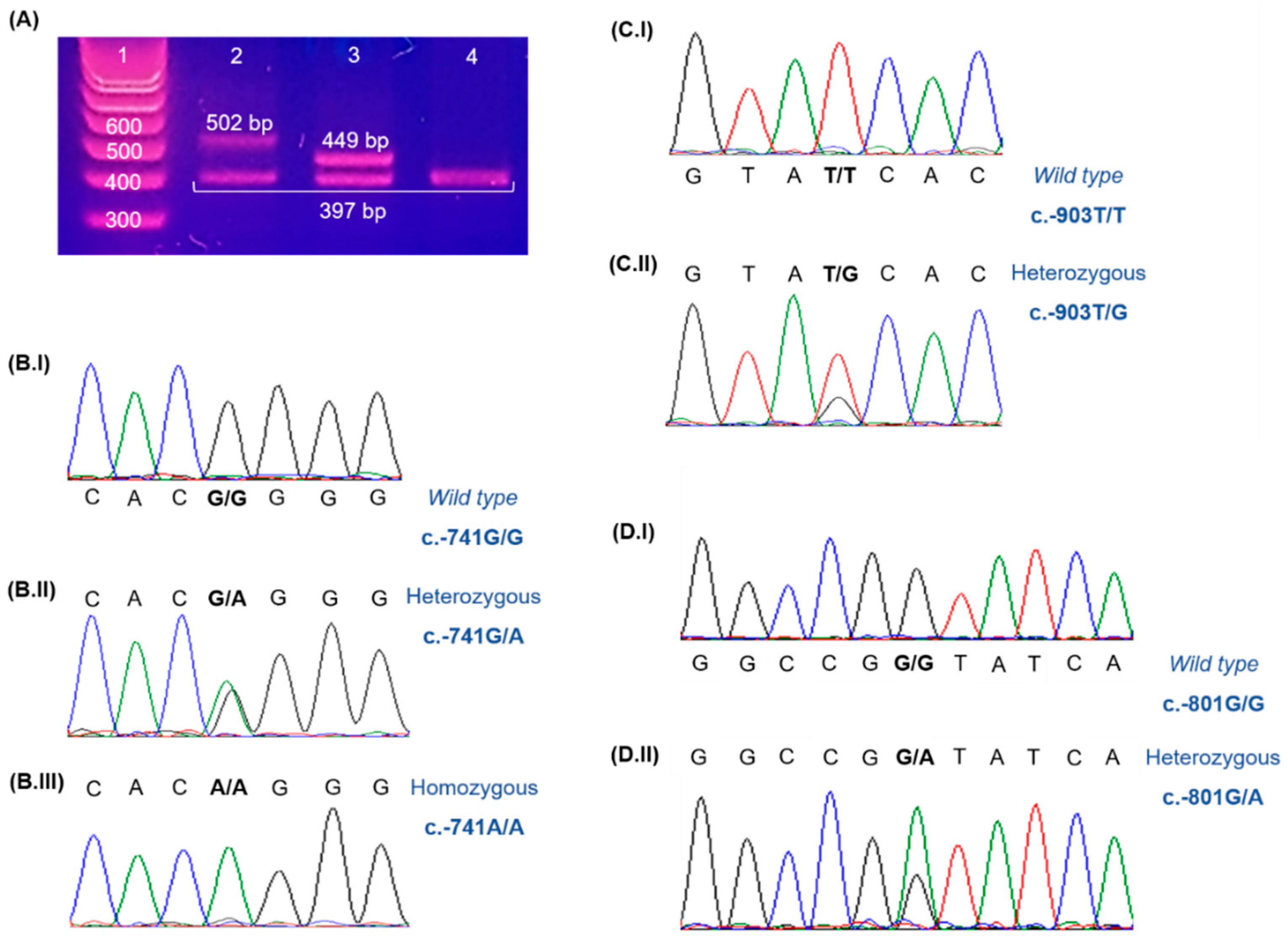
2.2. Methods
3. Results and Discussion
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Costa, E.; Rocha, S.; Rocha-Pereira, P.; Nascimento, H.; Castro, E.; Miranda, V.; Faria, M.S.; Loureiro, A.; Quintanilha, A.; Belo, L.; et al. Neutrophil activation and resistance to recombinant human erythropoietin therapy in hemodialysis patients. Am. J. Nephrol. 2008, 28, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Lindholm, B.; Goldsmith, D.; Fliser, D.; Wiecek, A.; Suleymanlar, G.; Ortiz, A.; Massy, Z.; Martinez-Castelao, A.; Agarwal, R.; et al. Cardiovascular and non-cardiovascular mortality in dialysis patients: Where is the link? Kidney Int. Suppl. 2011, 1, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Costa, E.; Gonçalves, M.; Miranda, V.; do Sameiro Faria, M.; Quintanilha, A.; Belo, L.; Lima, M.; Santos-Silva, A. Neutrophil and monocyte activation in chronic kidney disease patients under hemodialysis and its relationship with resistance to recombinant human erythropoietin and to the hemodialysis procedure. Hemodial. Int. 2010, 14, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Chen, L.; Lee, J.; Sellers, T.; Tockman, M.S. Polymorphisms in the promoter region of neutrophil elastase gene and lung cancer risk. Lung Cancer 2005, 48, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Yang, P.; Jett, J.; Bass, E.; Meyer, R.; Wang, Y.; Deschamps, C.; Liu, W. Polymorphisms in the promoter region of the neutrophil elastase gene are associated with lung cancer development. Clin. Cancer Res. 2002, 8, 1115–1120. [Google Scholar] [PubMed]
- Nikolic, A.; Milosevic, K.; Boskovic, S.; Nestorovic, B. Neutrophil elastase gene polymorphisms: Modulators of response to therapy in childhood bronchiectasis? Lung 2014, 192, 595–599. [Google Scholar] [CrossRef] [PubMed]
- Do Sameiro-Faria, M.; Ribeiro, S.; Rocha-Pereira, P.; Fernandes, J.; Reis, F.; Bronze-da-Rocha, E.; Miranda, V.; Quintanilha, A.; Costa, E.; Belo, L.; et al. Body mass index and resistance to recombinant human erythropoietin therapy in maintenance hemodialysis patients. Renal Fail. 2013, 35, 1392–1398. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Polymorphism | Genotype | Number of Cases | Allelic Frequencies | |||
|---|---|---|---|---|---|---|
| N | % | Allele | % | |||
| Previously Described | c.-903T>G | TT | 111 | 90.2 | T | 95.1 |
| TG | 12 | 9.8 | ||||
| G | 4.9 | |||||
| GG | 0 | 0.0 | ||||
| c.-741G>A | GG | 84 | 68.3 | G | 82.9 | |
| GA | 36 | 29.3 | ||||
| A | 17.1 | |||||
| AA | 3 | 2.4 | ||||
| Extra 52 pb | Wild type | 119 | 96.7 | Wild type | 98.4 | |
| Heterozygous | 4 | 3.3 | ||||
| Extra 52 bp | 1.6 | |||||
| Homozygous | 0 | 0.0 | ||||
| New | c.-801G>A | GG | 122 | 99.2 | G | 99.6 |
| GA | 1 | 0.8 | ||||
| A | 0.4 | |||||
| AA | 0 | 0.0 | ||||
| Extra block | Wild type | 121 | 98.4 | Wild type | 99.2 | |
| Heterozygous | 2 | 1.6 | ||||
| Extra block | 0.8 | |||||
| Homozygous | 0 | 0.0 | ||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, R.; Freitas, B.; Miranda, V.; Costa, E.; Santos-Silva, A.; Bronze-da-Rocha, E. Polymorphisms of the ELANE Gene Promoter Region in End-Stage Chronic Kidney Disease Patients. Genes 2016, 7, 17. https://0-doi-org.brum.beds.ac.uk/10.3390/genes7050017
Fernandes R, Freitas B, Miranda V, Costa E, Santos-Silva A, Bronze-da-Rocha E. Polymorphisms of the ELANE Gene Promoter Region in End-Stage Chronic Kidney Disease Patients. Genes. 2016; 7(5):17. https://0-doi-org.brum.beds.ac.uk/10.3390/genes7050017
Chicago/Turabian StyleFernandes, Rafael, Bruno Freitas, Vasco Miranda, Elísio Costa, Alice Santos-Silva, and Elsa Bronze-da-Rocha. 2016. "Polymorphisms of the ELANE Gene Promoter Region in End-Stage Chronic Kidney Disease Patients" Genes 7, no. 5: 17. https://0-doi-org.brum.beds.ac.uk/10.3390/genes7050017