
Real-Time Low-Cost Personal Monitoring for Exposure to PM2.5 among Asthmatic Children: Opportunities and Challenges

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
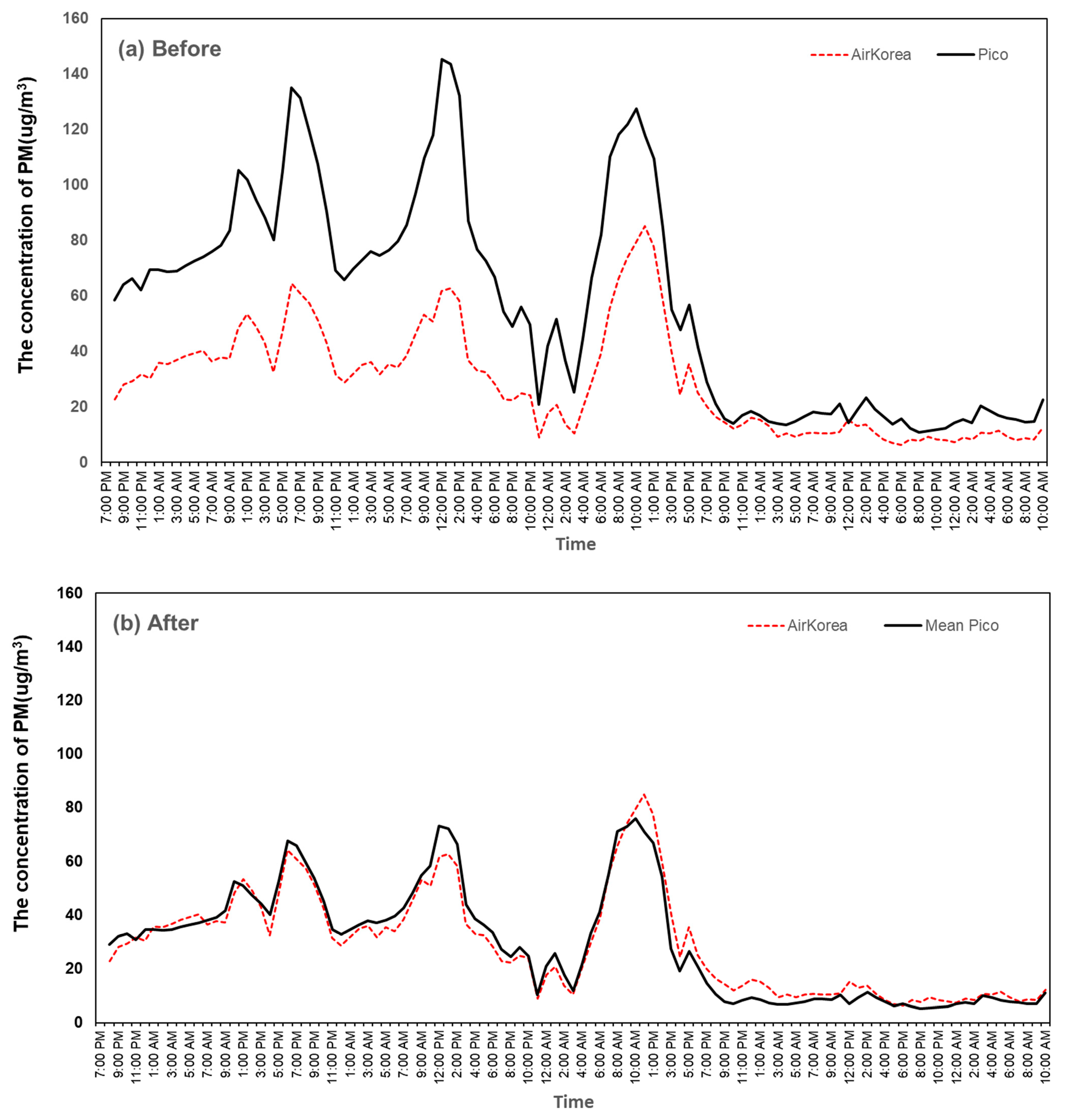
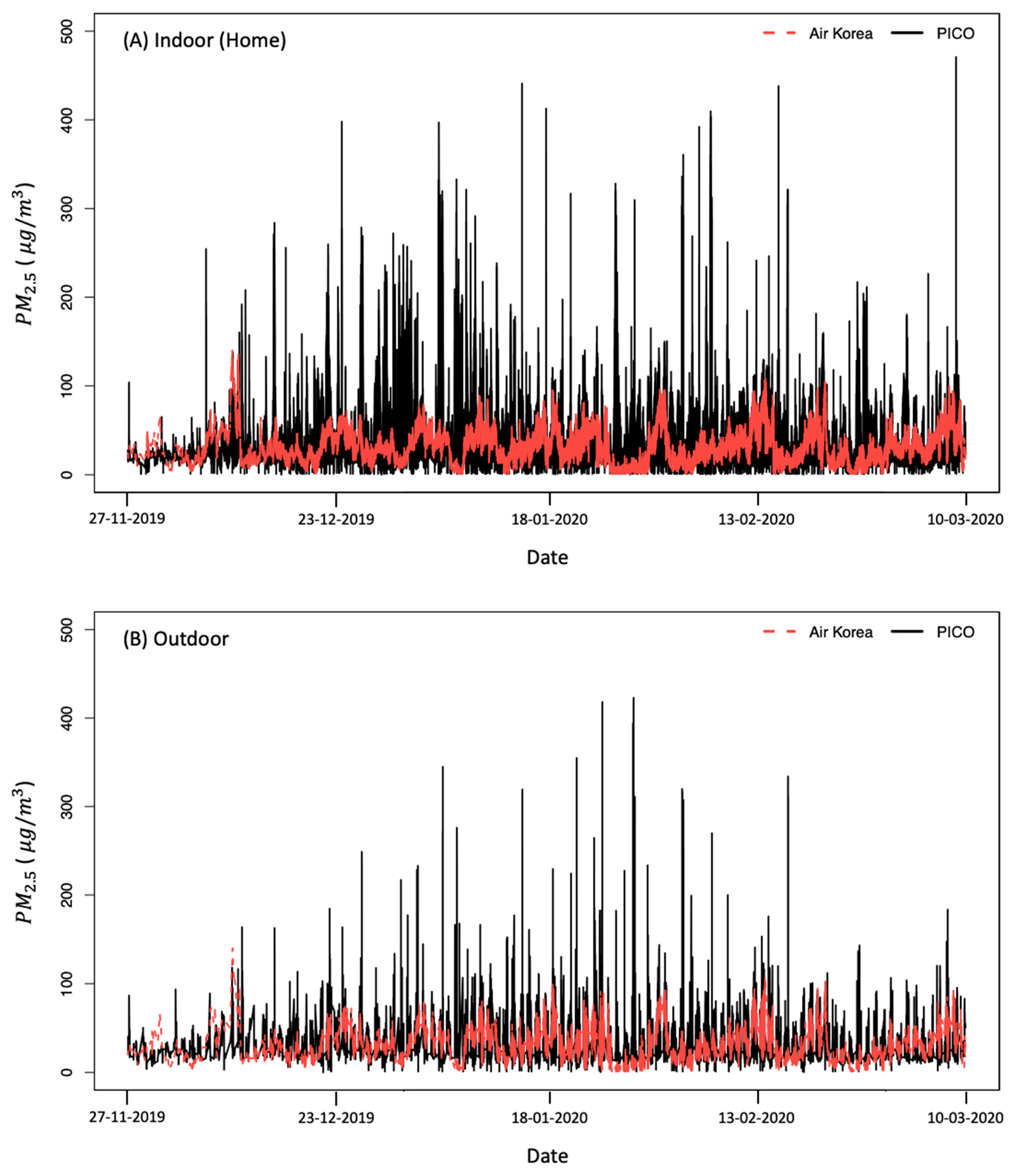
2.2. Station-Based PM Monitoring via Air Korea
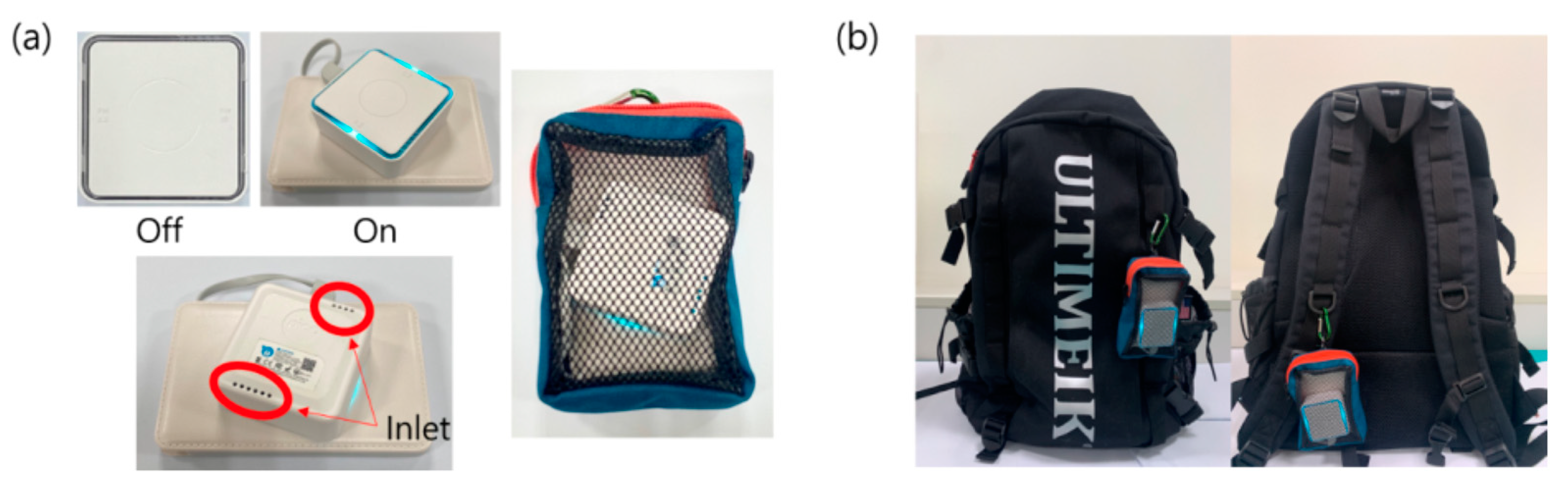
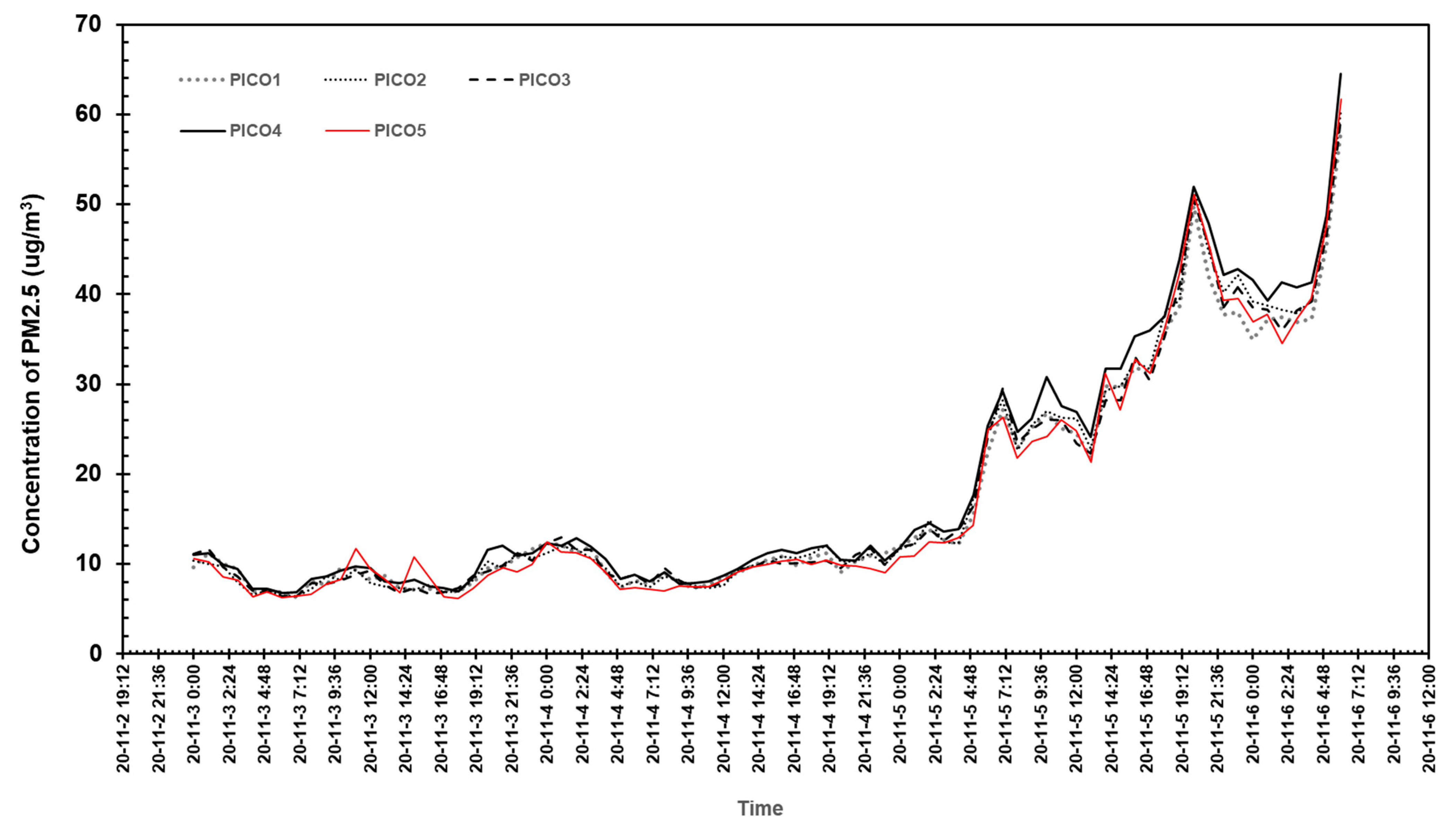
2.3. Personal Real-Time Monitoring via Low-Cost Sensors
2.4. Data Integration and Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Englert, N. Fine particles and human health—A review of epidemiological studies. Toxicolgy Lett. 2004, 149, 235–242. [Google Scholar] [CrossRef]
- Chen, H.; Burnett, R.; Kwong, J.; Vileneuve, P.; Goldberg, M.; Brook, R.; Donkelaar, A.; Jerrett, M.; Martin, R.; Brook, J.; et al. Risk of Incident Diabetes in Relation to Long-term Exposure to Fine Particulate Matter in Ontario, Canada. Environ. Health Perspect. 2013, 121, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Kriit, H.; Forsberg, B.; Astrom, D.; Oudin, A. Annual dementia incidence and monetary burden attributable to fine particulate matter (PM2.5) exposure in Sweden. Environ. Health 2021, 20, 65. [Google Scholar] [CrossRef]
- Peters, A. Particulate matter and heart disease: Evidence from epidemiological studies. Toxicol. Appl. Pharmacol. 2005, 207, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Snyder, E.; Watkins, T.; Solomon, P.; Thoma, E.; Williams, R.; Hagler, G.; Shelow, D.; Hindin, D.; Kilaru, V.; Preuss, P. The Changing Paradigm of Air Pollution Monitoring. Environ. Sci. Technol. 2013, 47, 11369–11377. [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Kauffmann, F.; Pin, I.; Moual, N.; Bousquet, J.; Gormand, F.; Just, J.; Nadif, R.; Pison, C.; Vervloet, D.; et al. Air pollution and asthma control in the Epidemiological study on the Genetics and Environment of Asthma. J. Epidemiol. Community Health 2012, 66, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Choi, H.; Gal, W.; Seo, S. Five Year Trends of Particulate Matter Concentrations in Korean Regions (2015–2019): When to Ventilate? Int. J. Environ. Res. Public Health 2020, 17, 5764. [Google Scholar] [CrossRef]
- Samoli, E.; Peng, R.; Ramsey, T.; Pipikou, M.; Touloumi, G.; Dominici, F.; Burnett, R.; Cohen, A.; Krewski, D.; Samet, J.; et al. Acute Effects of Ambient Particulate Matter on Mortality in Europe and North America: Results from the APHENA Study. Environ. Health Perspect. 2008, 116, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Occhipinti, L.; Oluwasanya, P. articulate Matter Monitoring: Past, Present and Future. Int. J. Earth Environ. Sci. 2017, 2, 144. [Google Scholar] [CrossRef]
- Seo, S.; Kim, D.; Min, S.; Paul, C.; Yoo, Y.; Choung, J.T. GIS-based Association Between PM10 and Allergic Diseases in Seoul: Implications for Health and Environmental Policy. Allergy Asthma Immunol. Res. 2016, 8, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Losser, T.; Yorke, C.; Piltner, R. Fast Inverse Distance Weighting-Based Spatiotemporal Interpolation: A Web-Based Application of Interpolating Daily Fine Particulate Matter PM2.5 in the Contiguous U.S. Using Parallel Programming and k-d Tree. Int. J. Environ. Res. Public Health 2014, 11, 9101–9141. [Google Scholar] [CrossRef]
- Liang, C.; Yu, P. Assessment and Improvement of Two Low-Cost Particulate Matter Sensor Systems by Using Spatial Interpolation Data from Air Quality Monitoring Stations. Atmosphere 2021, 12, 300. [Google Scholar] [CrossRef]
- Yun, J.; Sung, N.; Choi, S.; Kim, J. Real-time PM Monitoring System based on oneM2M IoT Platform and LoRa Networks. In Proceedings of the 2019 IEEE SENSORS, Montreal, QC, Canada, 27–30 October 2019; pp. 1–4. [Google Scholar]
- Steinle, S.; Reis, S.; Sabel, C.E.; Semple, S.; Twigg, M.M.; Braban, C.; Leeson, S.; Heal, M.; Harrison, D.; Lin, C.; et al. Personal exposure monitoring of PM2.5 in indoor and outdoor microenvironments. Sci. Total Environ. 2015, 508, 383–394. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, K.; Brocchieri, L.; Burglin, T.R. A comprehensive classification and evolutionary analysis of plant homeobox genes. Mol. Biol. Evol. 2009, 26, 2775–2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulot, F.; Johnston, S.J.; Basford, P.J.; Easton, N.; Apetroaie-Cristea, M.; Foster, G.; Morris, A.; Cox, S.; Loxham, M. Long-term field comparison of multiple low-cost particulate matter sensors in an outdoor urban environment. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Thai, P.; Liu, X.; Asumadu-Sakyi, A.; Ayoko, G.; Bartonova, A.; Bedini, A.; Chia, F.; Christensen, B.; Dunbabin, M.; et al. Applications of low-cost sensing technologies for air quality monitoring and exposure assessment: How far have they gone? Environ. Int. 2018, 116, 286–299. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Stanton, L.; Graham, A.; Roberts, P. Assessing the Utility of Low-Cost Particulate Matter Sensors over a 12-Week Period in the Cuyama Valley of California. Sensors 2017, 17, 1805. [Google Scholar] [CrossRef] [Green Version]
- Badura, M.; Batog, P.; Drzeniecka-Osiadacz, A.; Modzel, P. Regression methods in the calibration of low-cost sensors for ambient particulate matter measurements. SN Appl. Sci. 2019, 1, 622. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Yang, T.; Kim, T. Mobile-Based Sensing Scheme to Minimize Battery Power Consumption for Urban Monitoring Systems. Electronics 2021, 10, 198. [Google Scholar] [CrossRef]
- Cavaliere, A.; Carotenuto, F.; Gennaro, F.; Gioli, B.; Gualtieri, G.; Martelli, F.; Matese, A.; Toscano, P.; Vagnoli, C.; Zaldei, A. Development of Low-Cost Air Quality Stations for Next Generation Monitoring Networks: Calibration and Validation of PM2.5 and PM10 Sensors. Sensors 2018, 18, 2843. [Google Scholar] [CrossRef] [Green Version]
- Loh, B.; Choi, G. Calibration of Portable Particulate Matter–Monitoring Device using Web Query and Machine Learning. Saf. Health Work 2019, 10, 452–460. [Google Scholar] [CrossRef]
- Wijeratne, L.; Kiv, D.; Aker, A.; Talebi, S.; Lary, D. Using Machine Learning for the Calibration of Airborne Particulate Sensors. Sensors 2020, 20, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, M.; Cho, D.; Shin, K. The Impact of Particulate Matter on Outdoor Activity and Mental Health: A Matching Approach. Int. J. Environ. Res. Public Health 2019, 16, 2983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J. Particulate Matter Mortality Rates and Their Modification by Spatial Synoptic Classification. Int. J. Environ. Res. Public Health 2019, 16, 1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Kim, J.; Seo, S. Real-Time Measurement of Indoor PM Concentrations on Daily Change of Endocrine Disruptors in Urine Samples of New Mothers. Sustainability 2020, 12, 6166. [Google Scholar] [CrossRef]
- Marques, G.; Pitarma, R. Particulate Matter Monitoring and Assessment through Internet of Things: A Health Information System for Enhanced Living Environments. J. Med. Syst. 2020, 44, 207. [Google Scholar] [CrossRef]
- Kim, S.; Park, S.; Lee, J. Evaluation of Performance of Inexpensive Laser Based PM2.5 Sensor Monitors for Typical Indoor and Outdoor Hotspots of South Korea. Appl. Sci. 2019, 9, 1947. [Google Scholar] [CrossRef] [Green Version]
- Lim, C.; Kim, H.; Vilcassim, M.; Thurston, G.; Gordon, T.; Chen, L.; Lee, K.; Heimbinder, M.; Kim, S. Mapping urban air quality using mobile sampling with low-cost sensors and machine learning in Seoul, South Korea. Environ. Int. 2019, 131, 105022. [Google Scholar] [CrossRef]
- Kim, D.; Seo, S.; Min, S.; Simoni, Z.; Kim, S.; Kim, M. A Closer Look at the Bivariate Association between Ambient Air Pollution and Allergic Diseases: The Role of Spatial Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1625. [Google Scholar] [CrossRef] [Green Version]
- Hahm, Y.; Yoon, H. The impact of air pollution alert services on respiratory diseases: Generalized additive modeling study in South Korea. Environ. Res. Lett. 2021, 16, 064048. [Google Scholar] [CrossRef]
- Seo, J.; Kim, J.; Yang, J.; Yun, H.; Roh, M.; Kim, J.; Yu, S.; Jeong, N.; Jeon, H.; Choi, J.; et al. Changes in Air Quality during the COVID-19 Pandemic and Associated Health Benefits in Korea. Appl. Sci. 2020, 10, 8720. [Google Scholar] [CrossRef]
- Choi, Y.; Yoon, H.; Kim, D. Where do people spend their leisure time on dusty days? Application of spatiotemporal behavioral responses to particulate matter pollution. Ann. Reg. Sci. 2019, 63, 317–339. [Google Scholar] [CrossRef]
- Kim, K. Policy Report of Particulate Matters in Korea: Consumer’s Perspectives; KEITI: Seoul, Korea, 2019. [Google Scholar]
- Kwak, K. Relationship between rooftop and on-road concentrations of traffic-related pollutants in a busy street canyon: Ambient wind effects. Environ. Pollut. 2016, 208, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S. Comparative Analysis of Administrative Databases for Particulate Matter Air Pollution Between South Korea and the United States. J. Environ. Policy Adm. 2020, 28, 71–100. [Google Scholar] [CrossRef]
- Wang, Y.; Li, J.; Jing, H.; Zhang, Q.; Jiang, J.; Biswas, P. Laboratory Evaluation and Calibration of Three Low-Cost Particle Sensors for Particulate Matter Measurement. Aerosol Sci. Technol. 2015, 49, 1063–1077. [Google Scholar] [CrossRef]
- Oreskovic, N.; Kinane, B.; Aryee, E.; Kuhlthau, K.; Perrin, J. The Unexpected Risks of COVID-19 on Asthma Control in Children. J. Allergy Clin. Immunol. Pract. 2020, 8, 2489–2491. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Abdulrazzaq, Y.M.; Al-Mutawwa, J.; Debuse, P. Genetic and Environmental Factors Associated with Asthma. Human Biol. 1996, 68, 405–414. [Google Scholar]
- Marinho, S.; Simpson, A.; Custovic, A. Allergen avoidance in the secondary and tertiary prevention of allergic diseases: Does it work? Prim. Care Respir. J. 2006, 15, 152–158. [Google Scholar] [CrossRef]
- Kamp, M.; Thio, B.; De Jongh, F.; Driessen, J. Wearable Home-Monitoring in Asthmatic Children. Am. J. Respir. Crit. Care Med. 2018, 197, A2028. [Google Scholar]
- Fahimi, D.; Mahdavipour, O.; Sabino, J.; White, R.; Paprotny, I. Vertically-stacked MEMS PM2.5 sensor for wearable applications. Sens. Actuators A 2019, 299, 111569. [Google Scholar] [CrossRef]
- Kim, D.; Cho, S.; Tamil, L.; Song, D.; Seo, S. Predicting Asthma Attacks: Effects of Indoor PM Concentrations on Peak Expiratory Flow Rates of Asthmatic Children. IEEE Access 2020, 8, 8791–8797. [Google Scholar] [CrossRef]
- Bhat, G.; Shanka, N.; Kim, D.; Song, D.; Seo, S.; Panahi, I.; Tamil, L. Machine Learning-based Asthma risk prediction using IoT and smartphone applications. IEEE Access 2021, 9, 118708–118715. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Air Korea Mean ± SD | PICO Mean ± SD | Absolute Difference | T (p) | ||
|---|---|---|---|---|---|---|
| Locations of measurements | Indoor (home) | 265,457 | 31.08 ± 18.50 | 27.31 ± 19.30 | 3.77 | <0.01 |
| Indoor (other than home) | 64,533 | 30.71 ± 17.93 | 25.60 ± 19.33 | 5.11 | ||
| Outdoor | 33,880 | 31.34 ± 18.49 | 30.33 ± 20.87 | 1.00 | ||
| Time slots for measurements (outdoors only) | Morning (6 a.m.–noon) | 7695 | 32.27 ± 17.81 | 29.69 ± 16.70 | 2.58 | <0.01 |
| Afternoon (noon–8 p.m.) | 20,044 | 31.21 19.04 | 31.51 22.27 | 0.29 | ||
| Night/overnight (8 p.m.–6 a.m.) | 6141 | 30.58 17.45 | 27.32 20.53 | 3.26 | ||
| Distance from Air Korea station (outdoors only) | Within 500 m | 2220 | 30.52 18.50 | 31.20 22.41 | 0.68 | <0.01 |
| Beyond 500 m | 31,660 | 31.39 18.49 | 30.27 20.76 | 1.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Yum, Y.; George, K.; Kwon, J.-W.; Kim, W.K.; Baek, H.-S.; Suh, D.I.; Yang, H.-J.; Yoo, Y.; Yu, J.; et al. Real-Time Low-Cost Personal Monitoring for Exposure to PM2.5 among Asthmatic Children: Opportunities and Challenges. Atmosphere 2021, 12, 1192. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12091192
Kim D, Yum Y, George K, Kwon J-W, Kim WK, Baek H-S, Suh DI, Yang H-J, Yoo Y, Yu J, et al. Real-Time Low-Cost Personal Monitoring for Exposure to PM2.5 among Asthmatic Children: Opportunities and Challenges. Atmosphere. 2021; 12(9):1192. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12091192
Chicago/Turabian StyleKim, Dohyeong, Yunjin Yum, Kevin George, Ji-Won Kwon, Woo Kyung Kim, Hey-Sung Baek, Dong In Suh, Hyeon-Jong Yang, Young Yoo, Jinho Yu, and et al. 2021. "Real-Time Low-Cost Personal Monitoring for Exposure to PM2.5 among Asthmatic Children: Opportunities and Challenges" Atmosphere 12, no. 9: 1192. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos12091192