
Viral Cutaneous Infections in Swimmers: A Preliminary Study
by
 , and
, and
Eleni Sfyri
1,* ,
,
Vasiliki Kefala
1,
Effie Papageorgiou
1,
Athena Mavridou
1, 
Apostolos Beloukas
1,2 and
and
Efstathios Rallis
1 1
Department of Biomedical Sciences, University of West Attica, Campus I, 12243 Athens, Greece
2
Institute of Infection and Global Health, University of Liverpool, Liverpool L67 7BE, UK
*
Author to whom correspondence should be addressed.
Water 2021, 13(23), 3401; https://doi.org/10.3390/w13233401
Submission received: 20 October 2021
/
Revised: 15 November 2021
/
Accepted: 30 November 2021
/
Published: 2 December 2021
(This article belongs to the Special Issue Healthy Recreational Waters: Sanitation and Safety Issues)
Abstract
:Molluscum contagiosum (MC) and warts are common viral infections of the skin. Data regarding the prevalence of MC and verruca in swimmers are very poor and lacking in the literature. The purpose of this study was to determine the incidence of Molluscum Contagiosum (MC) and warts cases among young competitive swimmers participating in Greek swimming clubs. Of 244 swimmers enrolled in this study, 12.3% reported MC and 43% warts, during their swimming career, diagnosed and treated by dermatologists. There was no difference between sexes for MC but diagnoses of warts were higher in females. Axillae and trunk were the most common sites of primary infection for MC but warts mainly appeared on the soles. The incidence of MC and warts in swimmers who use outdoor facilities was higher. In our study, the incidence of warts and MC in Greek swimmers is considered high. Moist walking surfaces, placing towels on locker room benches, and sharing equipment are behaviors that cause infections. An early diagnosis of warts and MC lesions must be implemented in every swimmer through dermatological examination. Taking proper measures for reducing the risk of warts and MC transmission in Greek swimmers is mandatory.
1. Introduction
Swimming is a sport with fewer injuries compared with other athletic disciplines. Swimmers are less likely to suffer from injuries caused by contact with opponents, surfaces, or equipment. However, the special environment of a swimming pool creates its own special group of skin conditions that are either unique to the sport or shared with other sports [1]. Public swimming pools can be the source of infections due to micro-organisms. Cutaneous diseases and dermatological problems may appertain to the sports medicine field especially for the activity of swimming [1].
Molluscum contagiosum (MC) and warts are common viral infections of the skin. Molluscum contagiosum is a benign, self-limited, self-transmitting, viral infection caused by molluscum contagiosum-virus, poxviridae family affecting the skin and rarely of the mucous membranes [2,3]. The disease is usually seen in children, sexually active individuals, and immunocompromised patients. Transmission occurs from person to person contact, equipment, and autoinoculation. The average time of incubation is 2 to 8 weeks and lesions persist for 2 to 4 months [2,4]. Many epidemiologic studies of MC in the general population confirm an association between swimming pool use and MC [5].
Warts are benign growths of skin and mucosa caused by the human papillomavirus (HPV). Common warts are associated mainly with HPV types 2, 4. Flat warts are caused by types 3, 10, and 28. Deep palmoplantar warts are caused by type 1. Cystic warts are caused by type 60 and focal epithelial hyperplasia is caused by types 13 and 32 [5]. The disease is diffused in the worldwide population. Ιt is transmitted by direct contact with infected skin or indirectly via objects carrying the virus [6,7]. Warts represent one of the most common dermatoses in everyday practice. They are widespread in the general population, especially among primary schoolchildren. The prevalence ranges from 4% to 33% [1,8]. Exposure to HPV in families and school class has been associated with the development of warts. Bruggink et al. claim that the use of public swimming pools showed a low risk [9]. On the other hand, the use of communal showers is considered to be a risk factor for getting plantar warts because damp floors are HPV-friendly surfaces [10].
Incorrect behaviors are rife among swimming pool users and there is little awareness of the importance of pool rules for restricting health risks [11]. According to the Greek swimming pool regulation, swimmers have obligations regarding swimming pool use. Personal hygiene by taking a shower before swimming, the absence of dermatological or other infections, and compliance with safety rules are elements that are mandatory for the proper use of the swimming facility. The facility operator is the person who will take care of the entire facility maintenance, for the cleaning and disinfection program, and the control of swimming pool users’ bathing load. All the above are some basic parameters for the safe operation of a swimming facility and the avoidance of contagious viral dermatological and other infections [12]. Furthermore, WHO indicates that education can encourage swimming pool users to adopt safer behaviors for themselves and other swimmers. Facility operators, swimming clubs, and public health bodies must provide information about the importance of pool rules and signs that can be used to inform swimmers and reinforce previous educational messages [4]. Regardless of the regulation in force and the measures taken in swimming pools, attendance at swimming pools is a significant risk factor for an MC and warts in children [3,7,13]. However, epidemiological data referring to the incidence of Warts and MC among swimmers are lacking.
The purpose of this study was to determine the incidence of MC and warts cases among young competitive swimmers participating in Greek swimming clubs.
2. Materials and Methods
This study was conducted with the approval of the Ethics Committee of the University of West Attica (52645-20 July 2020) and the Hellenic Swimming Federation (787/ε-15 March 2019). Due to COVID-19 pandemic restriction measures, an online survey was conducted, from March 2021 to May 2021. Five swimming clubs from Attica Region with 531 swimmers and five from different Greek province cities (472 swimmers) were chosen to participate in this study. The Attica region swimming clubs were from different municipalities and they were not using the same swimming pool facilities. The swimming clubs were randomly chosen and were based on the willingness of the team coaches and general managers to accept the initial invitation, from the researchers, to participate.
Swimmers’ parents and adult swimmers of these swimming clubs were asked to complete an anonymous questionnaire which was sent via email and swimming clubs’ social media by coaches and general managers of these Greek swimming clubs. The total number of questionnaires’ receivers was 1004 athletes or their parents. Participation in this study was not mandatory.
The questionnaire was created by the researchers and transferred on Google Forms. Before the online survey, a pilot study was provided for the validity and understanding of the questions.
The questionnaire was divided into two parts. The first part concerned general information such as demographics, training routine, behavior in the swimming pool area, and general information about skin health. The second part consisted of questions related to multiple infections, locations of infections, the season of appearances, absence from the training program because of the infections, and dermatologist treatment. In case of recurrent infections, participants were asked to report on the last episode of the infection as it is easier for survey respondents to recall with accuracy.
Statistical Analysis
The categorical variables are presented as absolute (n) and related (%) frequencies. Monde Carlo exact test was applied to test normality between categorical variables. The chi-square test—Fisher’s exact test, was used to investigate the existence of a relationship between two categorical variables. To investigate the existence of a relationship between a categorical and an ordinal variable, the chi-square trend test was used. A binomial test was used to determine if the proportion of dichotomous variables equals a specific claimed value (0.50). Risk Estimate was performed to determine which factors—a type of facility, region of facility, allergies, family history of skin diseases, hygiene habits (sharing equipment and behavior)—might be independently associated with MC and warts, through which the odds ratio (OR) with 95% Confidence Interval was calculated. The two-sided level of statistical significance was set at 0.05. The data analysis was estimated with the statistical package IBM SPSS 26.0 (Statistical Package for Social Sciences).
3. Results
3.1. Demographic Characteristics
Two hundred and forty-four (n: 244) were enrolled in this study. The response rate was 24.3%. 136 were females (55.7%) and 108 were males (44.3%). The enrolled participants were from the junior categories (9–12 years old, n: 86, 35.2%) and the age group categories (13+, n: 158). 146 swimmers (59.8%) were used and an outdoor facility for their training and 98 swimmers (40.2%) an indoor facility. Respondents who swam in the Attica region swimming pools were three times more (n: 181) than those in the Greek province (n: 63). 102 swimmers involved in swimming training for more than 10 years, 69 swimmers for 7 to 9 years, 57 swimmers for 4 to 6 years, and 16 swimmers for less than 3 years. Most of the swimmers (n: 138) were swimming six or more times per week and 169 swimmers (69.3%) were swimming for two or more hours per day (Table 1).
3.2. Molluscum Contagiosum
According to parents’ and swimmers’ responses, 12.3% (n = 30) had MC during their swimming career, diagnosed and treated by dermatologists. Most of the responders with MC were in the 13 to 14 age category (n: 11, 19.3%), but the infection rate was higher among adult swimmers (n: 10, 20.4%), while in younger ages and 15–18 age categories the infection rate was very low. The prevalence did not differ between the sexes. 13% of the respondents who had been infected by MC have used an outdoor facility for their training. The infection rate of MC in the province were higher than in Attica Region. The prevalence of MC increases with years of training—from 6.3% to 17.2%—but without a statistically significant difference (Table 1). Most of the swimmers with MC were infected one time (86.7%), 3.3% two times 10% three times. Twenty-one (n: 21, 70%) of those who had been infected by MC reported that had been infected from warts too. Thus, swimmers with MC showed an increased risk of having warts (OR = 3.611 CI 95% 1.578–8.262 p = 0.001).
Almost all responders, interrupted their attendance of the training program during treatment. The absence period was less than a month for 51.7%. Seven swimmers (n: 7, 24.1%) interrupted their training for 3 months and four swimmers (13.8%) for only one week.
MC infections occurred mainly in wintertime. The proportion of infections in the winter showed a statistically significant difference compared to those who did not infect this season (n: 20, 66.7%, p < 0.001). Spring (33.3%, p < 0.001), autumn (13.3%, p < 0.001) and summertime (10%, p = 0.002) had a reduced reference to the lesion occurrences.
Trunk, axillae (73.3%, p = 0.016), and upper limbs (43.3%), were the most common sites of primary infection. Lower limb (10%) and face (6.7%) had a reduced reference as sites of infections. Swimmers with seasonal allergies had an increased risk of heaving MC (OR = 3.026 CI 95% 1.379–6.640, p = 0.004). Athletes with other types of allergy showed no increased risk of having MC. None of the family skin diseases related to psoriasis, warts, and atopy showed a significant risk of having MC (Table 2).
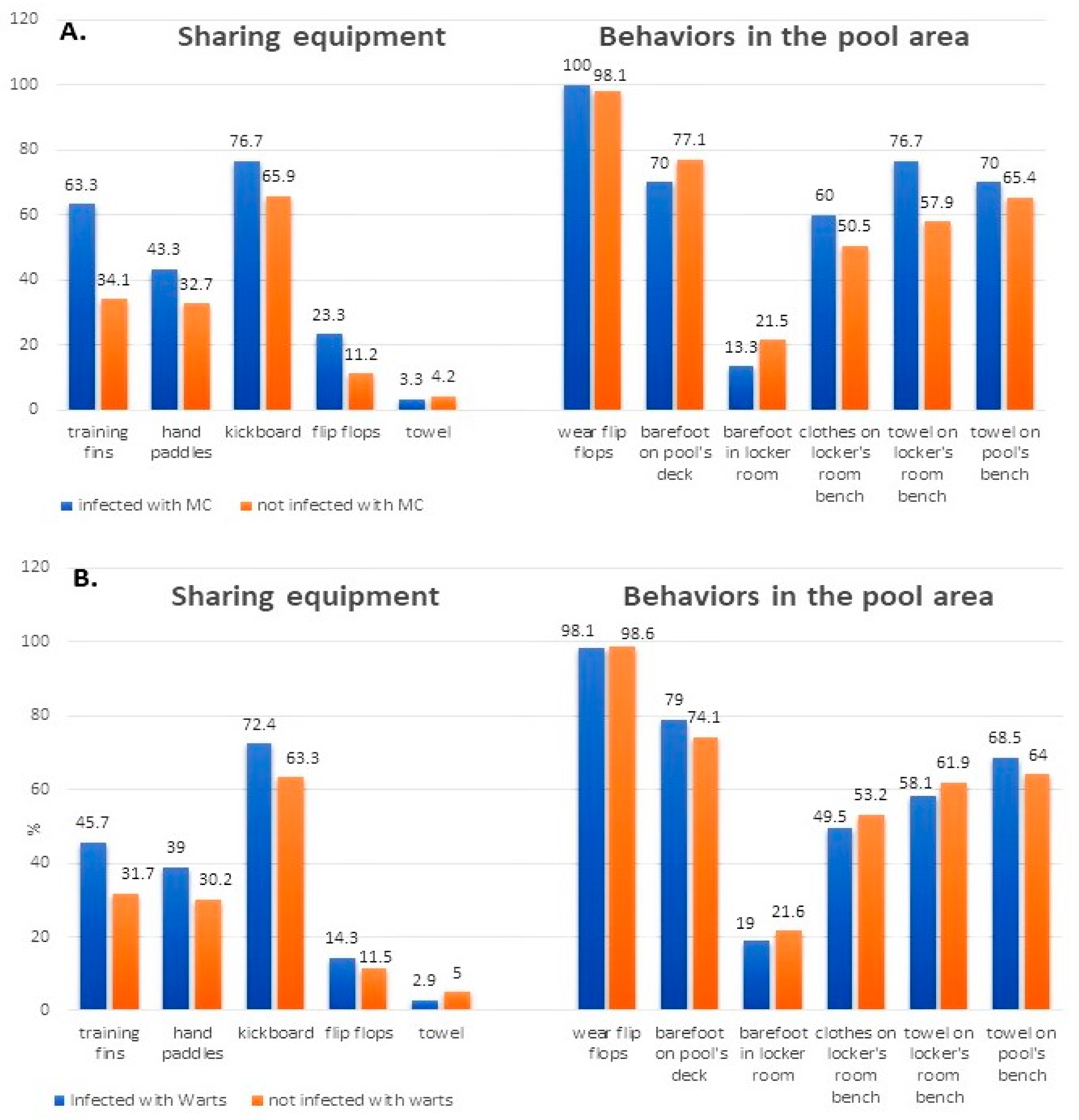
Of the sharing equipment report, only sharing training fins had an increased risk of having MC (OR = 3.336 CI 95% 1.507–7.384 p = 0.002). Wearing flip-flops was a hygiene rule which was observed from almost all the participants. Placing towels and bathrobes on the locker’s room bench had also an increased risk of having MC (OR = 2.385 CI 95% 0.981–5.799 p = 0.05). Factors related to walking barefoot on the pool’s deck or placing clothes on the communal bench had a high rate to all of the swimmers but without a significantly different (Figure 1A).
3.3. Warts
One hundred and five participants (n: 105, 43%) had warts during their swimming career. In all cases, diagnosis and treatment were performed by dermatologists. Infected females were more than males however, the prevalence did not differ between sexes (p = 0.244). Although younger swimmers were more, elder groups were more likely to be infected with warts (60% of 17–18 years old and 49% of adults had warts while 37.2% of 9–12 years old and 40.6% of 15–16 years old). The years and the daily duration of training seem to affect the infection rate of warts. Accordingly, two hours of daily training seems to be the most common duration for swimmers which justifies high warts’ infection rate (Table 1).
The participation in the training program was interrupted in 84.3% (n: 86) of the swimmers during warts’ treatment but for a different time period. Sixteen swimmers (15.7%) continued swimming training during treatment. More than half of the infected swimmers (55.9%) had “less than a month” absence period and 18.6% “less than three months” absence period. Four swimmers interrupted swimming for more than six months because of warts.
Almost half of the warts infections occurred in wintertime and there was not a significant difference with the athletes that were affected other seasons (n: 47, 44.8% p = 0.329). Spring (31.4% p < 0.001), summertime (28.6%, p < 0.001) and autumn (16.2%, p < 0.001) had a significant reduced reference to the lesion occurrences. The soles (45.7%, p < 0.435) were the most common sites of primary infection. The significance of sites infected with warts occurs in lower limb (25.7%, p < 0.001), hands (12.4%, p < 0.001), trunk (9% p < 0.001), upper limb (7% p < 0.001) and face (7%, p < 0.001). Athletes with allergy showed no increased risk of warts. A family history of warts (OR = 2.107 CI 95% 1.557–2.852 p = 0.012) and atopy (OR = 2.729 CI 95%1.111–6.706 p = 0.024) had an increased risk of warts infection (Table 2).
Swimmers who share training fins had an increased risk of having warts (OR = 1.818 CI 95% 1.076–3.072, p = 0.026). Wearing flip-flops was a hygiene rule which was observed from almost all the participants. Walking barefoot on the pool’s deck and placing towels on the pool’s or locker’s room bench were some behaviors that had been observed by more than half of participants in general (Figure 1B).
4. Discussion
Based on our findings the incidence of warts among Greek swimmers has been considered high [14] and MC’s incidence is almost quadrable compared to Kyriakis et al. [2,15]. To our knowledge, this is the first study that exclusively refers to cutaneous viral infections among competitive swimmers and not in the general population [2,10,14,16]. The years and the duration of training may hold an important role in the spread of forgoing viruses. Our findings on the prevalence of warts infections indicate that the rates of infections by age categories are proportional to the years and duration of training. This proportion for the prevalence of MC are not clear, possibly due to the lower number of MC infected swimmers in the 15–18 age categories. Nevertheless, the high percentages of infections of our study, possibly demonstrate what is generally accepted that: both these skin infections are typically caused by moist walking surfaces such as swimming pools, or by sharing items and equipment [4,13].
4.1. Molluscum Contagiosum
In our findings, 12.3% of swimmers were infected with MC in comparison to Mahe et al., who found MC in 3.6% of the general infant population [17]. Kyriakis et al. reported that the incidence of MC in Greece, among children outpatients, was 3.2% [2]. In the past, a 5% attack rate of MC, in an area of Germany, was coincided with a public swimming pool’s opening and declined after the pool was closed [18].
Males and females were equally affected by the MC virus, according to our data. The same results were found in previous studies in Greece and Australia [2,19] but in a Spanish study, boys were double than girls [20]. The majority of our cases were reported at the ages of 9 to 14, but the infections rate was higher in the adult swimmers which was associated with the years and duration of the training and probably the sexual activity. Evidence in young ages was reported by Olsen et al. who showed that 5 to 14 years old children had a high incidence rate [21]. Other studies have reported the high prevalence of MC in younger ages [3,22].
We found no data of a possible association between MC and warts. The co-existence of both viral infections in some participants was reported in our study and is possible due to the impaired epidermal barrier and noncompliance with the hygiene rules. Some studies have correlated MC with a history of atopy, which has been reported as a potential risk factor, in children who shared a bath with other children or swam at a school swimming pool [3,6,13].
Regarding the anatomical distribution of the MC lesions, our findings are similar and support previous relevant findings. They were located on the truck, axillae, and upper limbs in older children while the face was reported only in children aged ≤2 years old [3,15,20]. Niizeki et al., described MC lesions on the extremities, back, and axillae [21]. According to WHO, indirect transmission of MC via water in swimming pools is not considered possible [4]. In agreement with Choong et al., we believe that other behaviors such as direct contact of swimmers, use of bath sponges and towels, or putting clothes and bathrobes on a locker’s room bench, produced infection rates more often than to people who did not share such fomites [13]. Niizeki et al. assumed that the high incidence of lesions on the side of the body is the result of contact with kickboards used in the swimming pool [22]. Other sources of MC transmission may be training fins and hand paddles.
According to our findings, an outdoor facility may have a higher risk of virus transmission. Although the primary source of virus in swimming pool facilities is infected bathers, an outdoor facility needs a demanding hygiene protocol because of the open-air environmental exposure (animals, nature, pollution) [4]. Weismann related 75% of MC cases to the use of an outdoor swimming pool [23]. In Australia, outdoor school swimming pool attendance was found to be a significant risk factor for MC [13]. Regional differences in MC incidence were found in different regions of Holland. There were no differences in the climate, temperatures, or urbanization between the areas [21]. On the other hand, references mentioned the region’s climate for the transmission of MC lesions. A high incidence of MC has been reported in temperate climates. A Dutch study showed an incidence of 17% of MC in children younger than 15 years old [24]. In addition, cool climates facilitate the transmission of MC in children aged 10 to 12 years old, but warm countries favor the transmission at younger ages [25]. Regional differences also were found in North America but there was no explanation of what could attribute the higher prevalence of a region [21]. All reported references focused on the general population. In our study, the swimming pool region seemed to play a role in the potential spread of MC or warts. Due to the numerous responses from the Attica region, the comparison with the province data are not clear. The occurrence of MC among swimmers of different regions in Greece would be of interest.
Wintertime and spring were the seasons with a higher incidence of MC, noting that this is a preparation period for competitive swimmers in Greece. Koning et al. also, found that the incidence was higher between January and June than between July and December [24]. These findings disprove the general belief that warm, humid conditions are more favorable to a viral transmission. Weismann reported that, a seasonal variation in the number of cases of MC, with an increased incidence between February and September, related to the opening of a new outdoor public swimming pool [23].
4.2. Warts
Our findings are not in agreement with Van Haalen et al. who reported 33%, infection of warts in elementary school children [7]. Koning et al. reported 44%, infection of warts but in elementary school children [24]. Plantar warts affect 7–12% of the population with a higher prevalence in school-aged children [7]. Females seem to be more prone to HPV infections than males although Giannaki et al. found no significant difference in the prevalence of warts between sexes [14] or most frequent effect in males [26].
Our findings for the incidence of warts were in relation with Van Haalen et al. The peak age of warts occurring at 9–10 years and common presence in teenagers may relate to school attendance and sports activities [7]. The high incidence rate to 17 and older swimmers in our study is probably associated with the years and duration of training. Vaile et al. noted a positive correlation between the amount of swimming and the incidence of warts [27]. Plantar warts occur most frequently in children and adolescents, although they are rare in patients younger than 5 years [28].
Bruggink et al. mentioned that school class prevalence and having a family member with warts, were important risk factors for the transmission of warts, which is in agreement with our findings [9]. Atopy was mentioned as a risk factor in a Greek study for warts [14]. Another France study showed an association between warts, swimming pool frequentation, and atopy [29]. Seasonal allergy may be associated with the HPV appearance but there are no relevant data in the literature.
The soles are considered the most common site of warts infection among swimmers probably because of their participation in swimming pool training, other sports activities [28], and the use of communal showers [30]. In school children, common warts mainly occurred on hands and feet, confirming that warts are usually spread by direct skin-to-skin inoculation of the virus from one person to another.
Sharing equipment and fomites as training fins and kickboards is a serious risk factor for the transmission of warts [31]. Despite the extensive use of flip flops, a large number of participants walked barefoot on the pool’s deck and placed the towel/bathrobe on the communal bench. Walking barefoot increases the likelihood of contracting HPV, especially if other people walk barefoot as well [30,32]. It is believed that the rough surfaces of a swimming pool promote microtrauma to the sole of the foot, and the warm, moist environment promotes viral infection. The virus can survive several months on any surface until encountering a host [33].
Rates of plantar warts are noted to increase during the winter months [28]. Tamer et al. resulted that warts were mostly detected in summer than wintertime [34]. The competitive swimmers’ training period is from autumn to early summer and the prevalence of warts in winter and springtime is justified considering the daily attendance in the swimming pool.
An outdoor facility may have a higher risk of virus transmission due to the open-air environmental exposure but Vaile et al. reported a greater prevalence of warts in swimmers in covered pools compared to uncovered pools, concluding that this difference was noted in a different period of exposure [27]. For other cutaneous infections, the spreading role of bathing places such as indoor swimming pools or fun parks has been well established [31,35]. Regarding the occurrence of skin infections, further research is required to estimate the role of environmental factors.
To our knowledge, this is the first study assessing the incidence of MC and warts in competitive swimmers, worldwide. However, it includes limitations. Due to COVID-19 pandemic restriction measures, we used an online questionnaire without a clinical examination. Data were all self-reported and the survey required participants to recall past conditions. We thought that this approach was quicker and attractive for the participants because they had time to think about their answers without pressure. The questionnaire concerned a variety of skin infections which was not reported in this study. Thus, it cannot be ensured that the participants responded because they experienced MC or warts infections. Water quality and hygiene measures were not included in our study. In the future, we intend to correlate our findings with water quality measures to determine the risk assessment of the transmission of infectious diseases.
Relying on the data our participants submitted, a correlation between molluscum contagiosum, warts, and swimming pool environment was well documented. Fomites, pool equipment, and pool areas have been suggested as carriers of such viruses but the exact source of infections is not clear. Good practices can minimize the negative health impact of swimmers. The establishment manager is responsible for the proper operation and management of the swimming pool. Poor air and water quality, overcrowding in the facility, and poor maintenance of equipment are some parameters that must be considered for the operation of a swimming facility and the avoidance of contagious viral cutaneous and other infections [4]. The Greek swimming pool regulation includes preventive measures such as limiting the number of swimmers, continuous disinfection of the water, better cleaning of sanitary installations and the facilities, and regular maintenance of the technical equipment such as filters. Furthermore, swimmers have obligations regarding the use of the facility and compliance with safety and hygiene rules. Taking a shower before swimming, excluding swimmers with infectious disease, and using a swimming cup are elements that are mandatory for the proper use of the swimming facility and the avoidance of infections transmission [12]. Recommendations must be made to swimmers such as a visit to the dermatologist every year, to wear flip flops, or not to walk barefoot in public places [11]. Education of the swimmers is necessary for them to adopt proper behaviors. Competent authorities, facility operators, and swimming club managers can provide information on the rules of the facility and the importance of their implementation [4].
5. Conclusions
A high prevalence of MC and warts was observed in competitive swimmers in Greece. An early diagnosis of warts, MC lesions, and other skin viruses must be made for every swimmer through dermatological examination. In this way, possible transmission to other swimmers will be prevented. For skin infections related to swimming pool participation, further research is required on environmental factors such as indoor and outdoor facilities, detailed measures of water quality as well as hygienic control of the swimming pool auxiliary facilities. Taking proper measures for reducing the risk of warts and MC transmissions, such as strict swimming pool rules and recommendations for swimmer’s behavior, is mandatory.
Author Contributions
Conceptualization, E.S. and E.R.; methodology, E.S.; software, E.P.; validation, E.R., E.P. and A.M.; formal analysis, E.S.; investigation, E.S.; resources, V.K.; data curation, A.B.; writing—original draft preparation, E.S.; writing—review and editing, E.R. and A.B.; visualization, E.S.; supervision, E.R.; project administration, A.M.; funding acquisition, V.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the quidelines of the Declaration of Helsinki and approved by the Ethics Committee of Research of the University of West Attica, (52645-20 July 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Basley, R.S.; Basley, G.C.; Palmer, A.H.; Garcia, M.A. Special skin symptoms seen in swimmers. J. Am. Acad. Dermatol. 2000, 43, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Kyriakis, K.P.; Palamaras, I.; Terzoudi, S.; Emmanuelides, S.; Michailides, C. Case detection rates of molluscum contagiosum in childhood. Pediatr. Dermatol. 2007, 24, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Kakourou, T.; Zachariades, A.; Anastasiou, T.; Architectonidou, E.; Georgala, S.; Theodoridou, M. Molluscum contagiosum in Greek children: A case series. Int. J. Dermatol. 2005, 44, 221–223. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guidelines for Safe Recreational-Water Environments Final Draft for Consultation Volume 2: Swimming Pools, Spas and Similar Recreational-Water Environments; World Health Organization: Geneva, Switzerland, 2006; pp. 48–49. [Google Scholar]
- Al Aboud, A.M.; Nigam, P.K. Wart. NCBI e-book StatPearls Publications. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK431047 (accessed on 6 November 2021).
- Braue, A.; Ross, G.; Varigos, G.; Kelly, H. Epidemiology and Impact of Childhood Molluscum Contagiosum: A Case Series and Critical Review of the Literature. Ped. Dermatol. 2005, 22, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Van Haalen, F.M.; Bruggink, S.C.; Gussekloo, J.; Assendelft, W.J.; Eekhof, J.A. Warts in primary school children: Prevalence and relation with environmental factors. Br. J. Dermatol. 2009, 161, 148–152. [Google Scholar] [CrossRef]
- Tlougan, E.B.; Podjasek, O.J.; Adams, B.B. Aquatic sports dermatoses: Part 1. In the Water: Freshwater Dermatoses. Int. J. Dermatol. 2010, 49, 874–885. [Google Scholar] [CrossRef]
- Bruggink, S.C.; Eekhof, J.A.; Egberts, P.F.; Van Blijswijk, S.C.; Assendelft, W.J.; Gussekloo, J. Warts transmitted in families and schools: A prospective cohort. Pediatrics 2013, 131, 928–934. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, J.I.; Silverberg, N.B. The US Prevalence of Common Warts in Childhood: A Population-Based Study. J. Investig. Dermatol. 2013, 133, 2788–2790. [Google Scholar] [CrossRef] [Green Version]
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castaldi, S.; Pasquarella, M.L.; Saccani, E.; Eugenia, M.; Auxilia, F.; Gallè, F.; Di Onofrio, V.; et al. What about Behaviours in Swimming Pools? Results of an Italian Multicentre Study. Microchem. J. 2014, 112, 190–195. [Google Scholar] [CrossRef]
- E-nomothesia.gr. Hygiene Provision C1/443/1973-Law B-87/24-1-1973. Available online: https://www.e-nomothesia.gr/ygeionomikos-kanonismos-diatakseis/kolumbetikes-dexamenes/yd-g1-443-1973.html (accessed on 11 October 2021).
- Choong, K.Y.; Roberts, L.J. Molluscum contagiosum, swimming and bathing: A clinical analysis. Australas. J. Dermatol. 1999, 40, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Giannaki, M.; Kakourou, T.; Theodoridou, M.; Syriopoulou, V.; Kabouris, M.; Louizou, E.; Chrousos, G. Human Papillomavirus (HPV) Genotyping of Cutaneous Warts in Greek Children. Ped. Dermatol. 2013, 30, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Rallis, E.; Sfiri, E.; Tertipi, N.; Kefala, V. Molluscum contagiosum among Greek young competitive swimmers. J. Sports Med. Phys. Fit. 2020, 60, 1307–1308. [Google Scholar] [CrossRef]
- Kilkenny, M.; Merlin, K.; Young, R.; Marks, R. The prevalence of common skin conditions in Australian school students: 1. Common, plane and plantar viral warts. Br. J. Dermatol. 1998, 138, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Mahé, A.; Prual, A.; Konaté, M.; Bobin, P. Skin diseases of children in Mali: A public health problem. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 467–470. [Google Scholar] [CrossRef]
- Bader, R.E. Multiple occurrence of molluscum contagiosum in the zone of a swimming pool. Attempt at an epidemiological analysis. Arch. Hyg. Bakteriol. 1967, 151, 388–402. [Google Scholar] [PubMed]
- Konya, J.; Thompson, C.H. Molluscum contagiosum virus: Antibody responses in persons with clinical lesions and seroepidemiology in a representative Australian population. J. Infect. Dis. 1999, 179, 701–704. [Google Scholar] [CrossRef] [Green Version]
- Castilla, M.T.; Sanzo, J.M.; Fuentes, S. Molluscum contagiosum in children and its relationship to attendance at swimming pools: An epidemiological study. Dermatology 1995, 191, 165. [Google Scholar] [CrossRef] [PubMed]
- Olsena, J.R.; Gallachera, J.; Piguetb, V.; Francisa, N.A. Epidemiology of molluscum contagiosum in children: A systematic review. Fam. Pract. 2013, 31, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niizeki, K.; Kano, O.; Kondo, Y. An epidemic study of molluscum contagiosum. Relationship to swimming. Dermatology 1984, 169, 197–198. [Google Scholar] [CrossRef]
- Weismann, K. An epidemic of molluscum contagiosum originating in an outdoor public swimming-pool. An analysis of 125 consecutive cases. Ugeskr. Laeger 1973, 135, 2151–2156. [Google Scholar]
- Koning, S.; Bruijnzeels, M.A.; van Suijlekom-Smit, L.W.; Van Der Wouden, J.C. Molluscum contagiosum in Dutch general practice. Br. J. Gen. Pract. 1994, 44, 417–419. [Google Scholar]
- Postlethwaite, R.; Watt, J.A.; Hawley, T.G.; Simpson, I.; Adam, H. Features of molluscum contagiosum in the north-east of Scotland and in Fijian village settlements. J. Hyg. 1967, 65, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Al-Mutairi, N.; AlKhalaf, M. Mucocutaneous warts in children: Clinical presentations, risk factors and response to treatment. Acta Dermatovenerol. 2012, 21, 69–72. [Google Scholar]
- Vaile, L.; Finlay, F.; Sharma, S. Should verrucas be covered while swimming? Arch. Dis. Child. 2003, 88, 236–237. [Google Scholar] [CrossRef] [Green Version]
- Witchey, D.J.; Witchey, N.B.; Roth-Kauffman, M.M.; Kauffman, M.K. Plantar Warts: Epidemiology, Pathophysiology, and Clinical Management. J. Am. Osteop. Assoc. 2018, 118, 92–105. [Google Scholar] [CrossRef]
- Penso-Assathiany, D.; Flahault, A.; Roujeau, J.C. Warts, swimming pools and atopy: A case control study conducted in a private dermatology practice. Ann. Dermatol. Venereol. 1999, 126, 696–698. [Google Scholar]
- Johnson, L.W. Communal showers and the risk of plantar warts. J. Fam. Pract. 1995, 40, 136–138. [Google Scholar]
- La Rosa, G.; Della Libera, S.; Petricca, S.; Iaconelli, M.; Briancesco, R.; Paradiso, R.; Semproni, M.; Di Bonito, P.; Bonadonna, L. First detection of papillomaviruses and polyomaviruses in swimming pool waters: Unrecognized recreational water-related pathogens? J. Appl. Microb. 2015, 119, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.V.; Martínez-Campillo, F.; Verdú, M.; Cilleruelo, S.; Roda, J. Risk factors linked to the transmission of papillomavirus in the school environment. Alicante 1999. Aten. Primaria 2003, 31, 415–420. [Google Scholar] [CrossRef]
- Barna, Z.; Kádár, M. The risk of contracting infectious diseases in public swimming pools: A review. Ann. Ist. Super. Sanità 2012, 48, 374–386. [Google Scholar] [CrossRef]
- Tamer, E.; Ilhan, M.N.; Muhterem Polat, M.; Lenk, N.; Alli, N. Prevalence of skin diseases among pediatric patients in Turkey. J. Dermatol. 2008, 35, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Seebacher, C.; Bouchara, J.P.; Mignon, B. Updates on the epidemiology of dermatophyte infections. Mycopathologia 2008, 166, 335–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
(A). Swimmers’ common practices in the pool area and frequencies of those who had or not had infected with Molluscum Contagiosum. (B). Swimmers’ common practices in the pool area and frequencies of those who had or not had infected with Warts.
Figure 1.
(A). Swimmers’ common practices in the pool area and frequencies of those who had or not had infected with Molluscum Contagiosum. (B). Swimmers’ common practices in the pool area and frequencies of those who had or not had infected with Warts.


{kind=link}
Table 1.
Bivariate analyses using molluscum contagiosum and warts as dependent variables.
| Characteristics | Molluscum Contagiosum | p-Value | Warts | |||
|---|---|---|---|---|---|---|
| Yes (%) | No (%) | Yes (%) | No (%) | p-Value | ||
| Total | 30 (12.3) | 214 (87.7) | 105 (43) | 139 (57) | ||
| Gender | 0.499 a | 0.244 a | ||||
| Male | 15 (13.9) | 93 (86.1) | 42 (38.9) | 66 (61.1) | ||
| Female | 15 (11) | 121 (89) | 63 (46.3) | 73 (53.7) | ||
| Age categories | 0.084 b | 0.094 a | ||||
| 9–12 years old | 5 (5.8) | 81 (94.2) | 32 (33.2) | 54 (62.8) | ||
| 13–14 years old | 11 (19.3) | 46 (80.7) | 24 (42.1) | 33 (57.9) | ||
| 15–16 years old | 3 (9.4) | 29 (90.6) | 13 (40.6) | 19 (59.4) | ||
| 17–18 years old | 1 (5) | 19 (95) | 12 (60) | 8 (40) | ||
| Open (Men-Women) | 10 (20.4) | 39 (76.9) | 24 (49) | 25 (51) | ||
| Swimming pool | 0.677 a | 0.567 a | ||||
| Outdoor facility | 19 (13) | 127 (87) | 65 (44.5) | 81 (55.5) | ||
| Indoor facility | 11 (11.2) | 87 (88.8) | 40 (40.8) | 58 (59.2) | ||
| District of facilities | 0.147 a | 0.149 a | ||||
| Capital | 19 (10.5) | 162 (89.5) | 73 (40.3) | 108 (59.7) | ||
| Province | 11 (17.5) | 52 (82.5) | 32 (50.8) | 31 (49.2) | ||
| Training years | 0.077 b | 0.234 b | ||||
| <3 | 1 (6.3) | 15 (93.8) | 5 (31.3) | 11 (68.8) | ||
| 4–6 years | 4 (7) | 53 (93) | 21 (36.8) | 36 (63.2) | ||
| 7–9 years | 9 (13) | 60 (87) | 35 (50.7) | 34 (49.3) | ||
| 10–12 years | 6 (13.6) | 38 (86.4) | 15 (34.1) | 29 (65.9) | ||
| >12 years | 10 (17.2) | 48 (82.8) | 29 (50) | 29 (50) | ||
| Weekly training | 0.966 b | 0.709 b | ||||
| <3 training sessions | 4 (13,3) | 27 (12.6) | 16 (51.6) | 15 (48.4) | ||
| 4–5 trainings sessions | 9 (30) | 66 (30.8) | 29 (38.7) | 46 (61.3) | ||
| <6 trainings sessions | 17 (56.7) | 121 (56.5) | 60 (43.5) | 78 (56.5) | ||
| Hours of daily training | 0.220 b | 0.209 b | ||||
| <1 h/day | 0 (0) | 2 (100) | 0 (0) | 2 (100) | ||
| <1.5 h/day | 5 (6.8) | 68 (93.2) | 28 (38.4) | 45 (61.6) | ||
| 2 h/day | 19 (15.6) | 103 (84.4) | 57 (46.7) | 65 (53.3) | ||
| >3 | 6 (12.8) | 41 (87.2) | 20 (42.6) | 27 (57.4) | ||
Values are expressed as n (%) unless stated otherwise. a n X2 test. b X2 test for trend.
Table 2.
Allergies and family history of skin diseases in relation to Molluscum Contagiosum and Warts.
Table 2.
Allergies and family history of skin diseases in relation to Molluscum Contagiosum and Warts.
| Molluscum Contagiosum | Warts | |||||
|---|---|---|---|---|---|---|
| Yes | No | p-Value | Yes | No | p-Value | |
| Allergies | N (%) | N (%) | N (%) | N (%) | ||
| Dermatological allergy | 0.624 a | 0.155 a | ||||
| Yes | 10 (13.9) | 62 (86.1) | 36 (50) | 36 (50) | ||
| No | 20 (11.6) | 152 (88.4) | 69 (40.1) | 103 (59.9) | ||
| Respiratory allergy | 0.219 b | 0.511 a | ||||
| Yes | 4 (20) | 16 (80) | 10 (50) | 10 (50) | ||
| No | 26 (11.6) | 198 (88.4) | 95 (42) | 129 (57.6) | ||
| Food allergy | 0.077 b | 0.272 a | ||||
| Yes | 4 (28.6) | 10 (71.4) | 8 (57.1) | 6 (42.9) | ||
| No | 26 (11.3) | 204 (88.7) | 97 (42.2) | 133 (57.8) | ||
| Drug allergy | 0.312 b | 0.269 a | ||||
| Yes | 3 (18.8) | 13 (81.3) | 9 (56.3) | 7 (43.8) | ||
| No | 27 (11.8) | 201 (88.2) | 96 (42.1) | 132 (57.9) | ||
| Seasonal allergy | 0.004 a | 0.06 a | ||||
| Yes | 14 (22.6) | 48 (77.4) | 33 (53.2) | 29 (46.8) | ||
| No | 16 (8.8) | 166 (91.2) | 72 (39.6) | 110 (60.4) | ||
| Family history of skin diseases | ||||||
| Psoriasis | 0.208 b | 0.349 b | ||||
| Yes | 2 (28.6) | 5 (71.4) | 4 (57.1) | 3 (42.9) | ||
| No | 28 (11.8) | 209 (97.7) | 101 (96.2) 42.6 | 136 (57.4) | ||
| Warts (HPV) | 0.256 b | 0.012 b | ||||
| Yes | 2 (25) | 6 (75) | 7 (87.5) | 1 (12.5) | ||
| No | 28 (11.9) | 208 (88.1) | 98 (93.3) 41.5 | 138 (58.5) | ||
| Atopy | 0.134 b | 0.024 a | ||||
| Yes | 5 (21.7) | 18 (78.3) | 15 (65.2) | 8 (34.8) | ||
| No | 25 (11.3) | 196 (88.7) | 90 (40.7) | 131 (59.3) | ||
Values are expressed as n (%) unless stated otherwise. a Chi-square. b Fisher’s exact test.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sfyri, E.; Kefala, V.; Papageorgiou, E.; Mavridou, A.; Beloukas, A.; Rallis, E. Viral Cutaneous Infections in Swimmers: A Preliminary Study. Water 2021, 13, 3401. https://0-doi-org.brum.beds.ac.uk/10.3390/w13233401
AMA Style
Sfyri E, Kefala V, Papageorgiou E, Mavridou A, Beloukas A, Rallis E. Viral Cutaneous Infections in Swimmers: A Preliminary Study. Water. 2021; 13(23):3401. https://0-doi-org.brum.beds.ac.uk/10.3390/w13233401
Chicago/Turabian StyleSfyri, Eleni, Vasiliki Kefala, Effie Papageorgiou, Athena Mavridou, Apostolos Beloukas, and Efstathios Rallis. 2021. "Viral Cutaneous Infections in Swimmers: A Preliminary Study" Water 13, no. 23: 3401. https://0-doi-org.brum.beds.ac.uk/10.3390/w13233401
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.