
Clinical Case: Patient with Mixed Graft Rejection Four Days after Kidney Transplantation Developed Specific Antibodies against Donor Bw4 Specificities

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. HLA Typing
2.2. LABScreen™ Single Antigen HLA Class I and Class II
2.3. C1qScreen™ Single Antigen HLA Class I and Class II
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Eikmans, M.; Gielis, E.M.; Ledeganck, K.J.; Yang, J.; Abramowicz, D.; Claas, F.F.J. Non-invasive Biomarkers of Acute Rejection in Kidney Transplantation: Novel Targets and Strategies. Front. Med. 2018, 5, 358. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Alexander, S.I. Rejection of the kidney allograft. N. Engl. J. Med. 2010, 363, 1451–1462. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.K.; Bedi, D.S.; Denecke, C.; Ge, X.; Tullius, S.G. Impact of innate and adaptive immunity on rejection and tolerance. Transplantation 2008, 86, 889–894. [Google Scholar] [CrossRef]
- Terasaki, P.I.; Cecka, J.M.; Gjertson, D.W.; Takemoto, S. High survival rates of kidney transplants from spousal and living unrelated donors. N. Engl. J. Med. 1995, 333, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Colvin, R.B. Antibody-mediated renal allograft rejection: Diagnosis and pathogenesis. J. Am. Soc. Nephrol. 2007, 18, 1046–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Karpinski, M.; Ho, J.; Storsley, L.J.; Goldberg, A.; Birk, P.E.; Rush, D.N.; Nickerson, P.W. Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2012, 12, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Lutz, C.T. Human leukocyte antigen Bw4 and Bw6 epitopes recognized by antibodies and natural killer cells. Curr. Opin. Organ Transplant. 2014, 19, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Leffell, M.S.; Kraus, E.; Racusen, L.C.; Ratner, L.E.; Charney, D.; Zachary, A.A. Effect of Bw4 and Bw6 epitope mismatches on antibody production, acute and chronic rejection, and graft survival in renal allografts. Transplantation 2001, 72, 433–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2018, 18, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Randhawa, P. T-cell-mediated rejection of the kidney in the era of donor-specific antibodies: Diagnostic challenges and clinical significance. Curr. Opin. Organ Transplant. 2015, 20, 325–332. [Google Scholar] [CrossRef]
- Hagerty, D.T.; Allen, P.M. Processing and presentation of self and foreign antigens by the renal proximal tubule. J. Immunol. 1992, 148, 2324–2330. [Google Scholar]
- Phillips, B.L.; Callaghan, C. The immunology of organ transplantation. Surgery 2017, 35, 333–340. [Google Scholar] [CrossRef]
- Knight, S.R.; Alasadi, A.; Clancy, M. The immunology of solid organ transplantation. Anaesth. Intensive Care Med. 2018, 19, 579–582. [Google Scholar] [CrossRef]
- Actor, J.K. Transplantation Immunology. Introd. Immunol. 2019, 133–142. [Google Scholar] [CrossRef]
- Loupy, A.; Lefaucheur, C. Antibody-Mediated Rejection of Solid-Organ Allografts. N. Engl. J. Med. 2018, 379, 1150–1160. [Google Scholar] [CrossRef]
- Voora, S.; Adey, D.B. Management of Kidney Transplant Recipients by General Nephrologists: Core Curriculum 2019. Am. J. kidney Dis. Off. J. Natl. Kidney Found. 2019, 73, 866–879. [Google Scholar] [CrossRef] [PubMed]
- Thurman, J.M.; Panzer, S.E.; Le Quintrec, M. The role of complement in antibody mediated transplant rejection. Mol. Immunol. 2019, 112, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Baranwal, A.K.; Bhat, D.K.; Goswami, S.; Agarwal, S.K.; Kaur, G.; Kaur, J.; Mehra, N. Comparative analysis of Luminex-based donor-specific antibody mean fluorescence intensity values with complement-dependent cytotoxicity & flow crossmatch results in live donor renal transplantation. Indian J. Med. Res. 2017, 145, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Gutiérrez, A.; Morales-Buenrostro, L.E.; Vilatobá-Chapa, M.; Mendoza-De-la-Garza, Á.; Vega-Vega, O.; Gabilondo-Pliego, B.; Alberú, J. Factores de riesgo para el desarrollo de función retardada del injerto en receptores de trasplante renal de donante fallecido y su impacto en la supervivencia de paciente e injerto. Rev. Investig. Clín. 2013, 65, 109–115. [Google Scholar]
- Lim, W.H.; Wong, G.; Heidt, S.; Claas, F.H.J. Novel aspects of epitope matching and practical application in kidney transplantation. Kidney Int. 2018, 93, 314–324. [Google Scholar] [CrossRef]
- Hiraiwa, M.; Yamamoto, J.; Matsumoto, K.; Karaki, S.; Nagao, T.; Kano, K.; Takiguchi, M. T cell can recognize the allospecificities formed by the substitution of amino acids associated with HLA-Bw4/Bw6 public epitopes. Hum. Immunol. 1991, 32, 41–45. [Google Scholar] [CrossRef]
- Kumru Sahin, G.; Unterrainer, C.; Süsal, C. Critical evaluation of a possible role of HLA epitope matching in kidney transplantation. Transplant. Rev. 2020, 34, 100533. [Google Scholar] [CrossRef] [PubMed]
- Nainani, N.; Singh, N.; Shanahan, T.; Damodar, A.; Parimoo, N.; Ummadi, S.; Qazi, Y.; Murray, B.M.; Tornatore, K.M.; Ciccirella, J.C.; et al. Cross Reactive Epitope Group antibodies in sensitized kidneys transplant recipients was associated with early acute Antibody Mediated Rejection. Transpl. Immunol. 2009, 20, 113–117. [Google Scholar] [CrossRef]
- Gorbacheva, V.; Fan, R.; Fairchild, R.L.; Baldwin, W.M.; Valujskikh, A. Memory CD4 T cells induce antibody-mediated rejection of renal allografts. J. Am. Soc. Nephrol. 2016, 27, 3299–3307. [Google Scholar] [CrossRef] [PubMed]
- Visentin, J.; Vigata, M.; Daburon, S.; Contin-Bordes, C.; Fremeaux-Bacchi, V.; Dromer, C.; Billes, M.-A.; Neau-Cransac, M.; Guidicelli, G.; Taupin, J.-L. Deciphering complement interference in anti-human leukocyte antigen antibody detection with flow beads assays. Transplantation 2014, 98, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Gareau, A.J.; Pochinco, D.; Gibson, I.W.; Ho, J.; Birk, P.E.; Blydt-Hansen, T.; Karpinski, M.; Goldberg, A.; Storsley, L.; et al. Evaluation of C1q Status and Titer of De Novo Donor-Specific Antibodies as Predictors of Allograft Survival. Am. J. Transplant. 2017, 17, 703–711. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anti-HLA Antibodies Analysis Date | Anti-HLA CLASS I Antibodies | Anti-HLA CLASS II Antibodies |
|---|---|---|
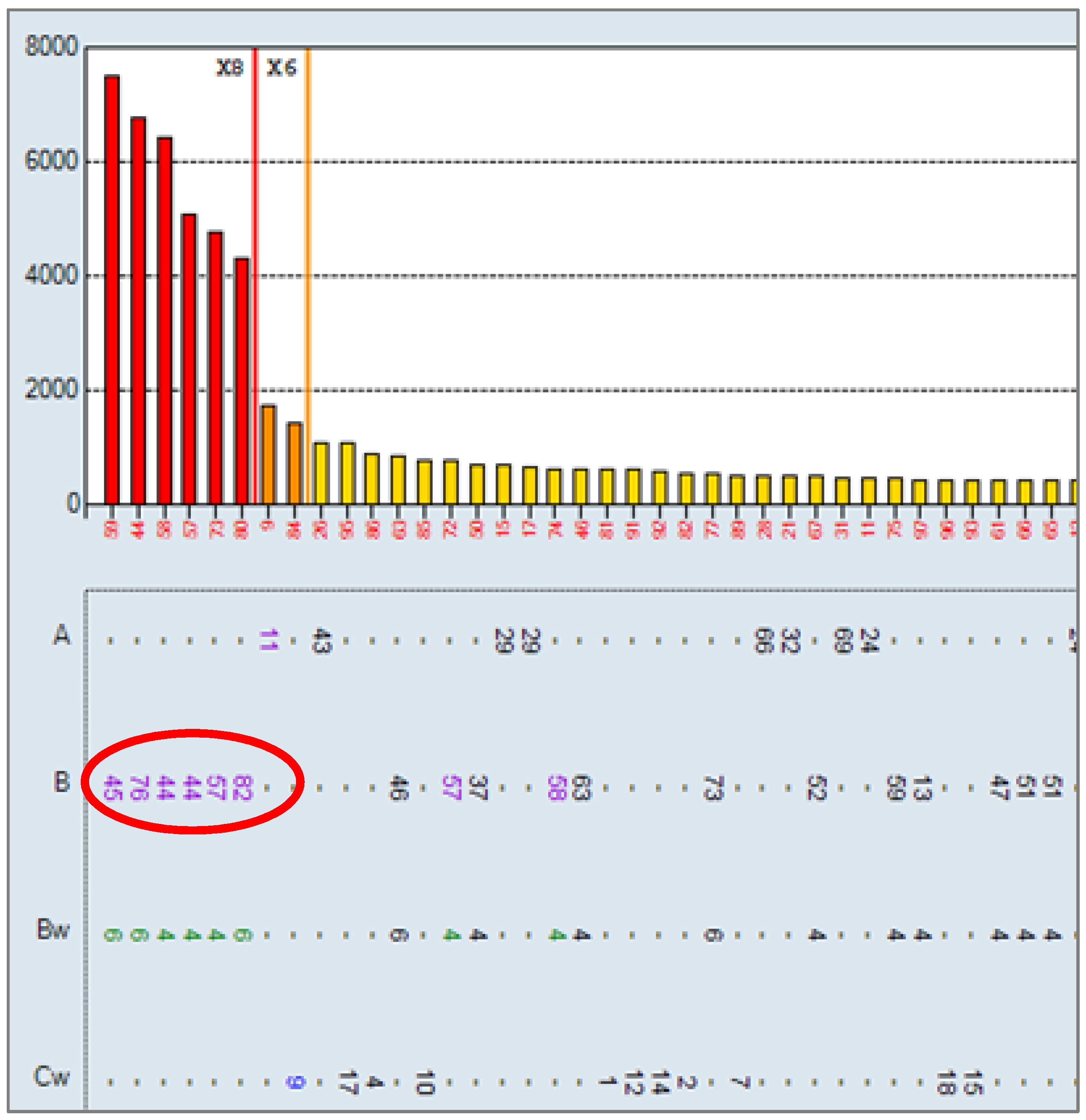
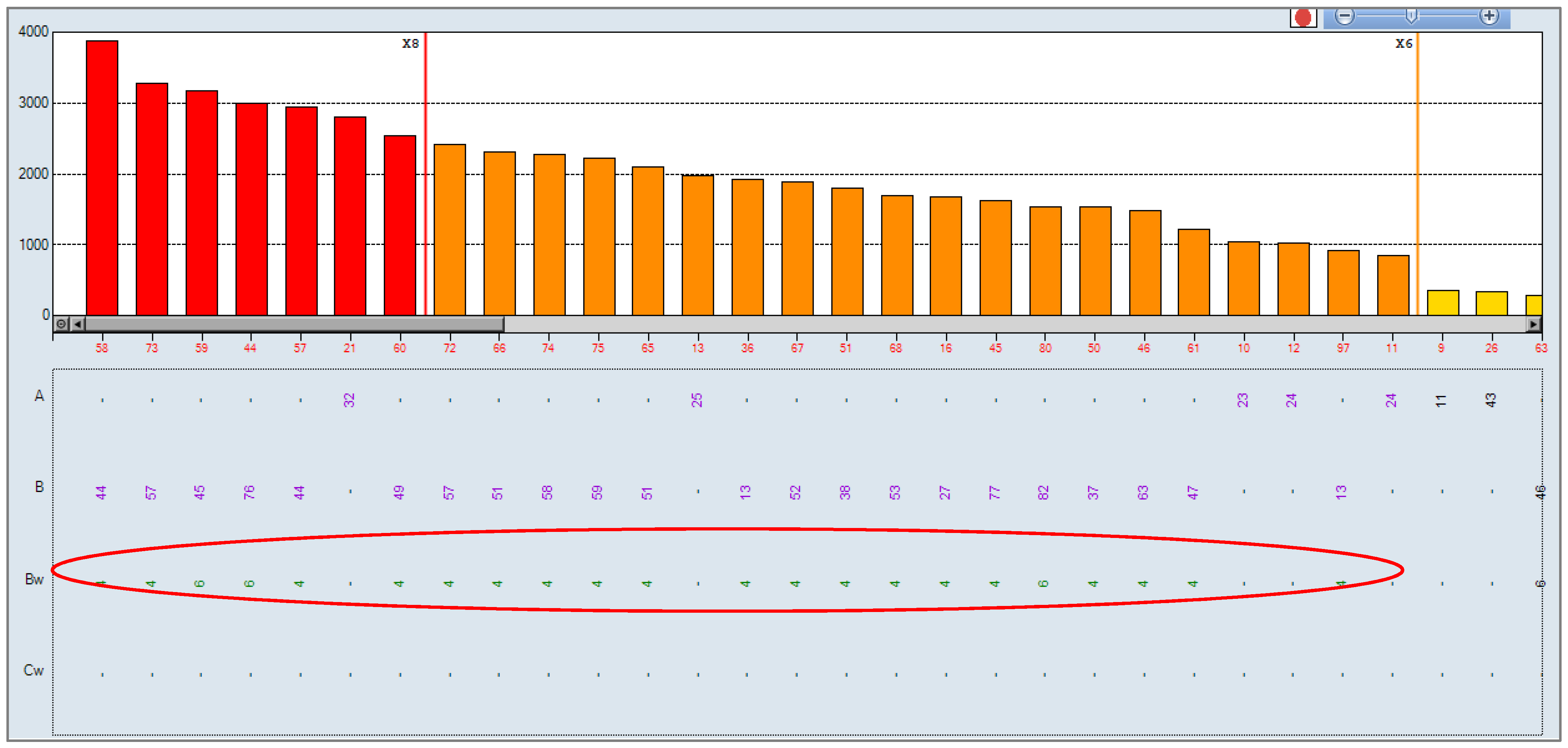
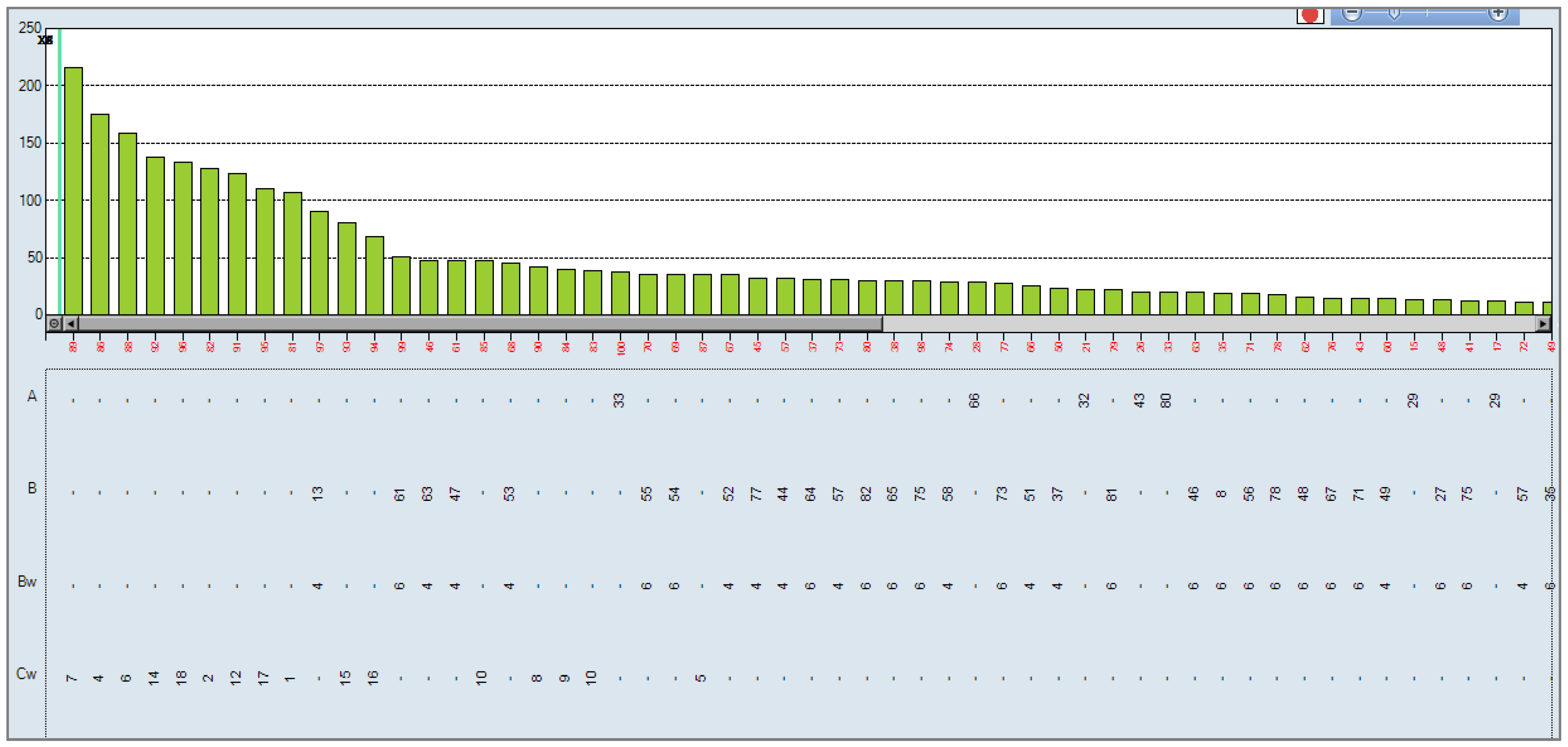
| 14 March 2017 | B45, B44, B76, B82 | Negative |
| 6 April 2017 | Negative | Negative |
| 7 July 2017 | Negative | Negative |
| 9 October 2017 | Negative | Negative |
| 10 January 2018 | B45, B44, B76, B57, B82, A11, Cw9 | Negative |
| A * | A * | B * | B * | Bw | Bw | C * | C * | DRB1 * | DRB1 * | DQB1 * | DQB1 * | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HLA recipient | 01 | 30 | 18 | 40 | Bw6 | - | 02 | 06 | 11 | - | 03 | - |
| HLA donor | 03 | 30 | 38 | - | Bw4 | - | 12 | - | 01 | 13 | 05 | 06 |
| Creatinine | Diuresis | Blood Pressure | |
|---|---|---|---|
| Day 1 post-transplant | 3.44 mg/dL | 3480 cc | 137/94 mmHg |
| Day 2 post-transplant | 2.46 mg/dL | 5260 cc | 141/92 mmHg |
| Day 3 post-transplant | 2.28 mg/dL | 8910 cc | 145/90 mmHg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Herrera, C.M.; Gutiérrez-Bautista, J.F.; López-Nevot, M.Á. Clinical Case: Patient with Mixed Graft Rejection Four Days after Kidney Transplantation Developed Specific Antibodies against Donor Bw4 Specificities. Antibodies 2021, 10, 28. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030028
Muñoz-Herrera CM, Gutiérrez-Bautista JF, López-Nevot MÁ. Clinical Case: Patient with Mixed Graft Rejection Four Days after Kidney Transplantation Developed Specific Antibodies against Donor Bw4 Specificities. Antibodies. 2021; 10(3):28. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030028
Chicago/Turabian StyleMuñoz-Herrera, Claudia M., Juan Francisco Gutiérrez-Bautista, and Miguel Ángel López-Nevot. 2021. "Clinical Case: Patient with Mixed Graft Rejection Four Days after Kidney Transplantation Developed Specific Antibodies against Donor Bw4 Specificities" Antibodies 10, no. 3: 28. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030028