Comparison of Body Composition Monitor and InBody 720 Bioimpedance Devices for Body Composition Estimation in Hemodialysis Patients and Healthy Controls




Abstract
:1. Introduction
2. Materials and Methods
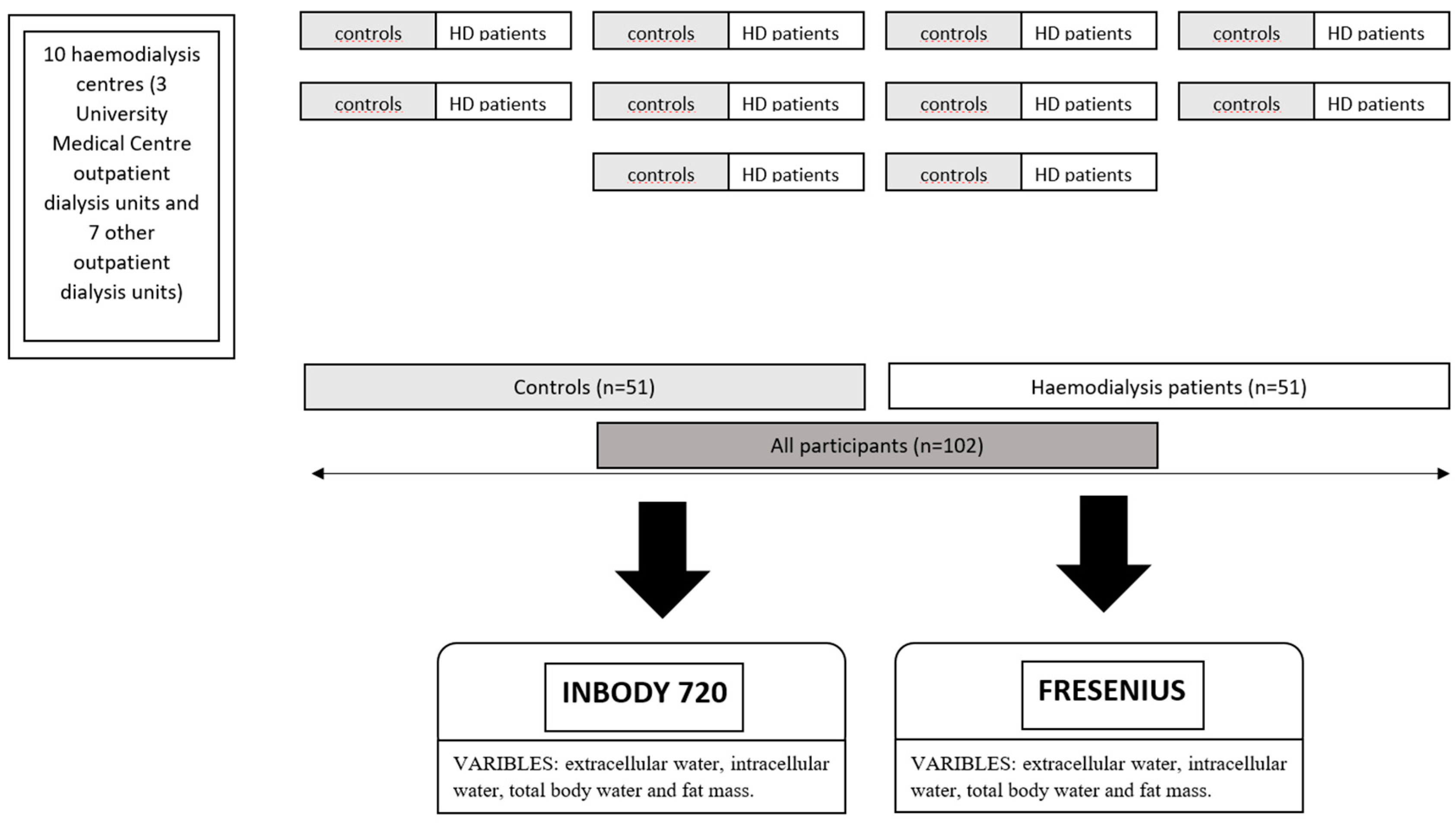
2.1. Participants
2.2. Procedures
2.3. Statistical Analyses
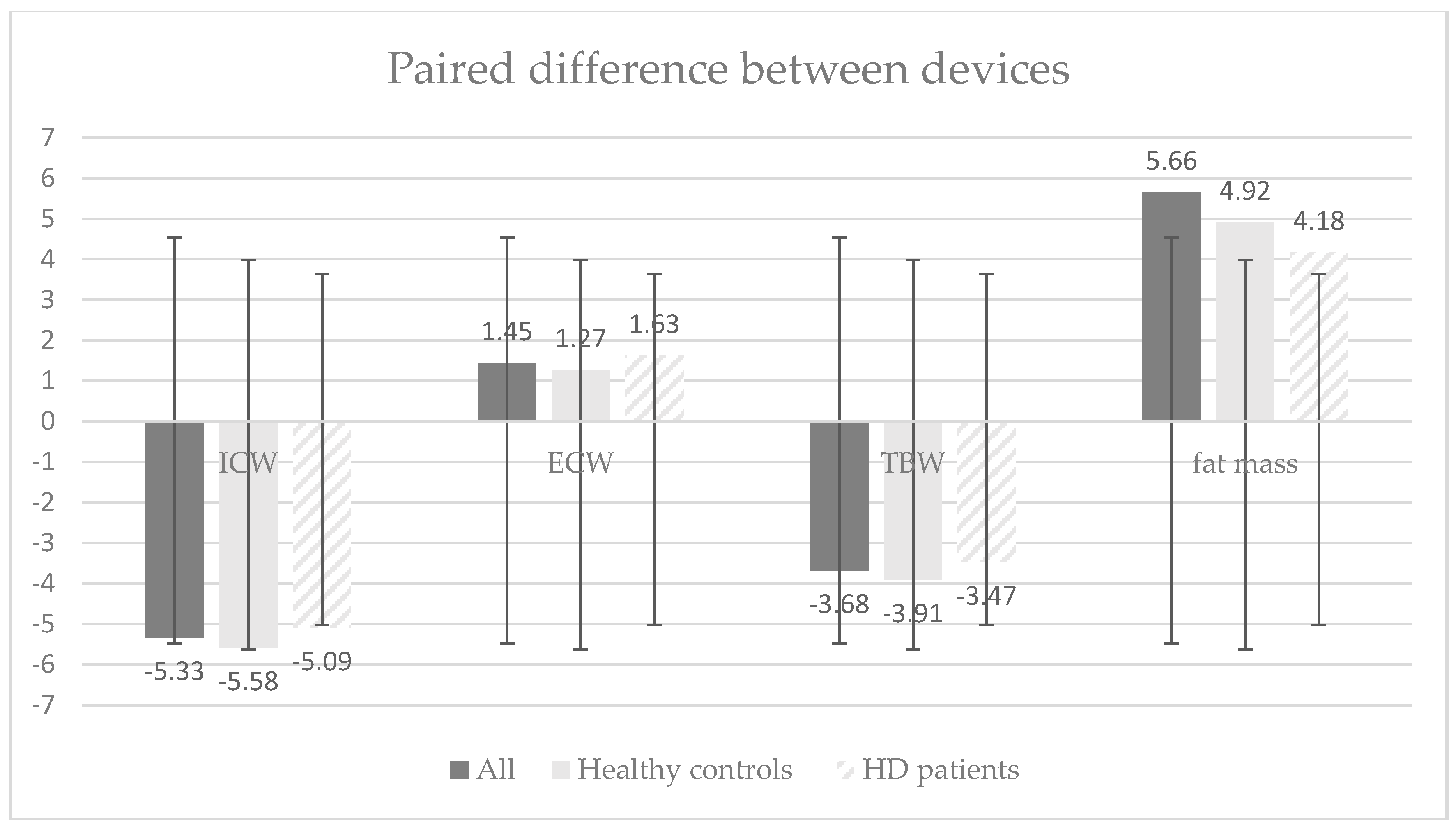
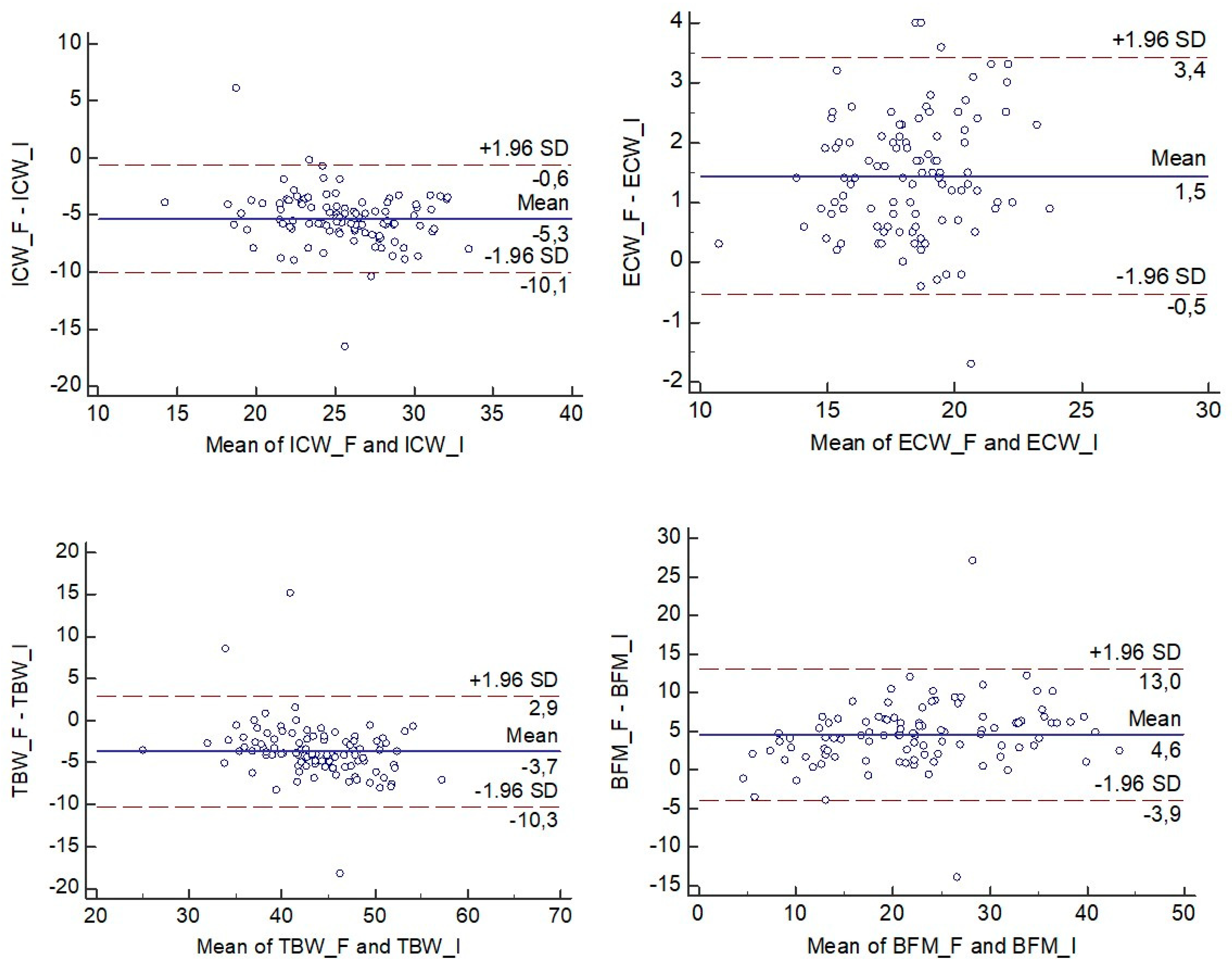
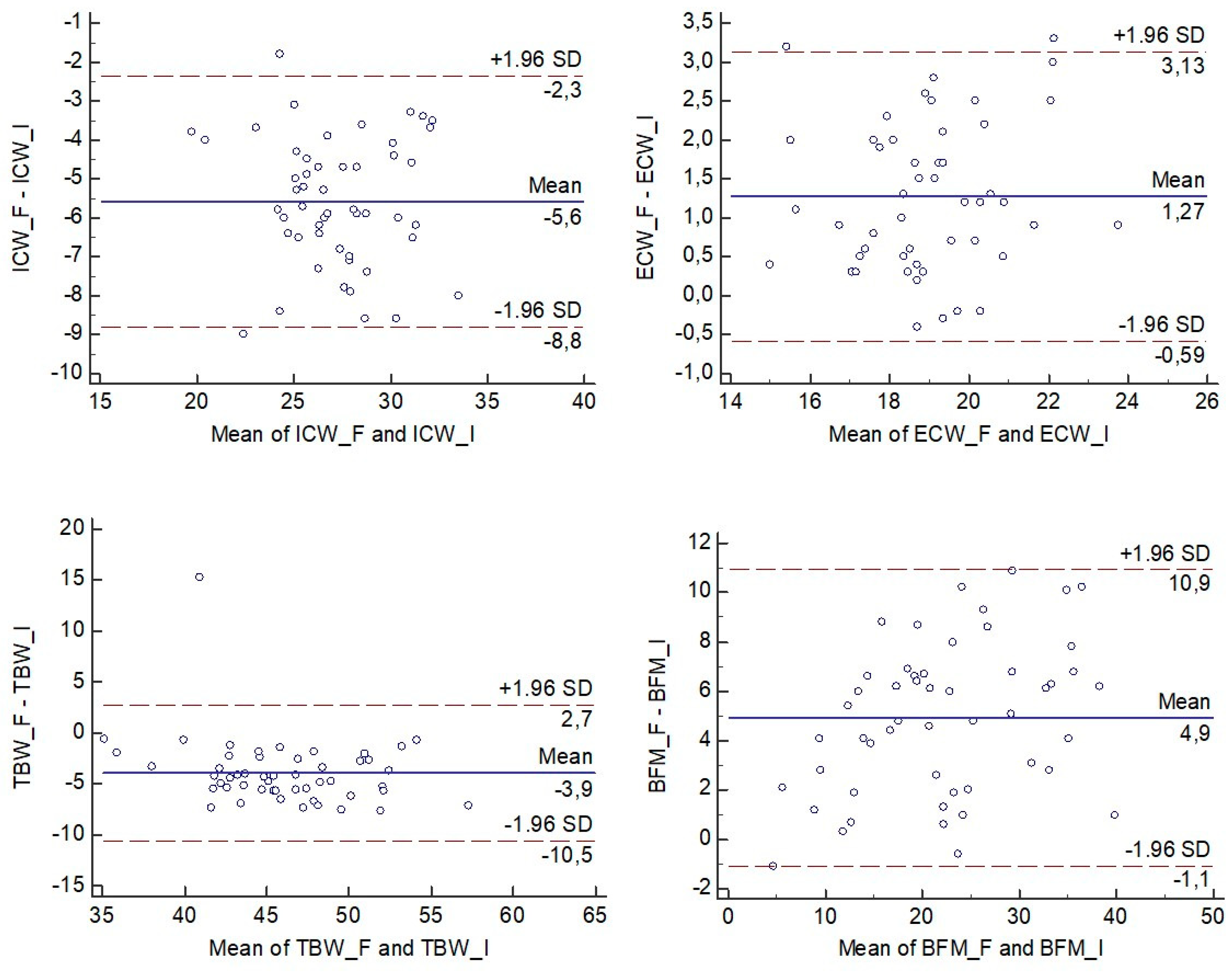
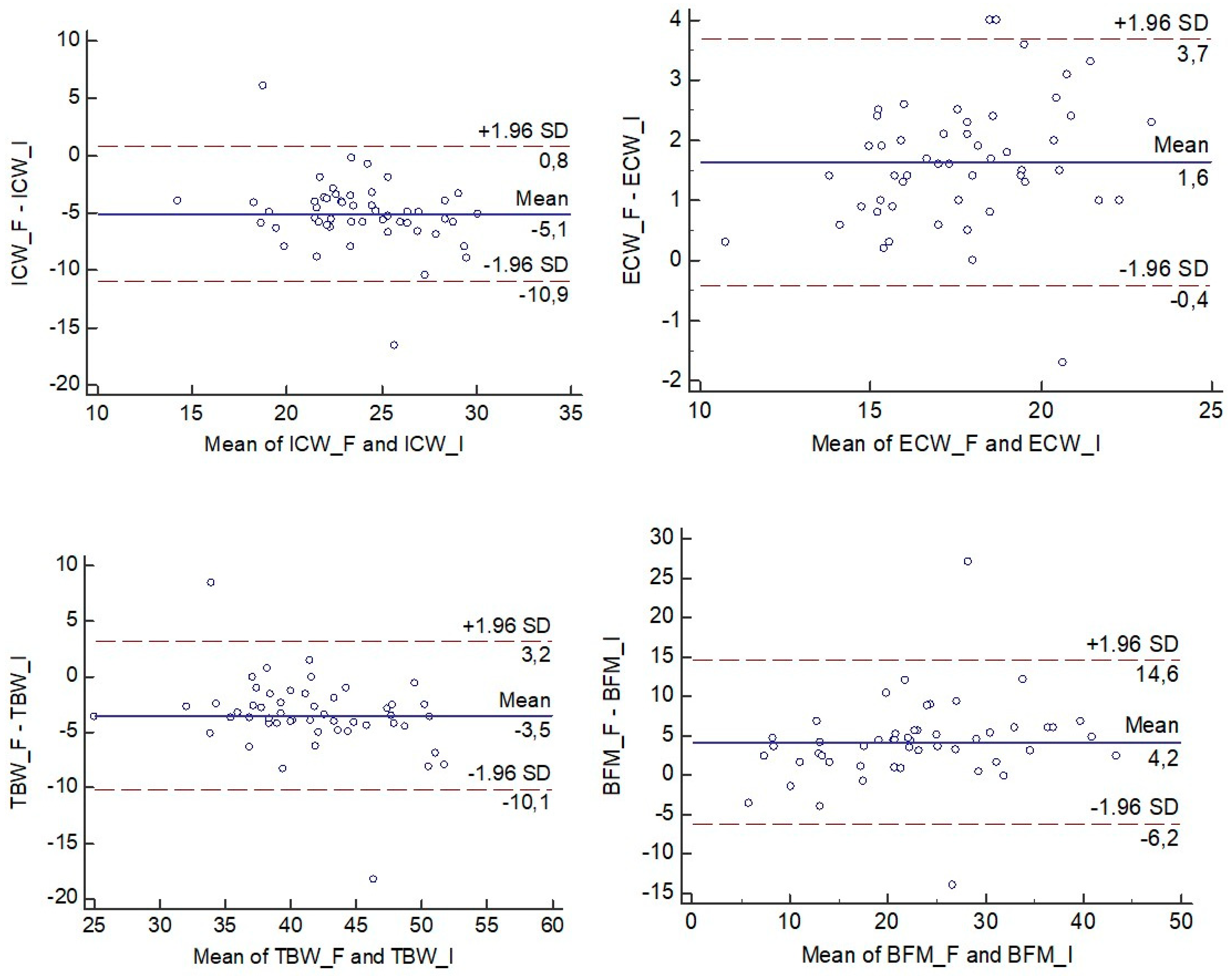
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dziubek, W.; Bulińska, K.; Kusztal, M.; Kowalska, J.; Rogowski, Ł.; Zembroń-Łacny, A.; Gołębiowski, T.; Ochmann, B.; Pawlaczyk, W.; Klinger, M.; et al. Evaluation of Exercise Tolerance in Dialysis Patients Performing Tai Chi Training: Preliminary Study. Evid. Based Complementary Altern. Med. 2016, 2016, 5672580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leavey, S.F.; McCullough, K.; Hecking, E.; Goodkin, D.; Port, F.K.; Young, E.W. Body mass index and mortality in ‘healthier’ as compared with ‘sicker’ haemodialysis patients: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transpl. 2001, 16, 2386–2394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K.; Abbott, K.C.; Salahudeen, A.K.; Kilpatrick, R.D.; Horwich, T.B. Survival advantages of obesity in dialysis patients. Am. J. Clin. Nutr. 2005, 81, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Shinaberger, C.S.; Kilpatrick, R.D.; Regidor, D.L.; McAllister, C.J.; Greenland, S.; Kopple, J.D.; Kalantar-Zadeh, K. Longitudinal Associations Between Dietary Protein Intake and Survival in Hemodialysis Patients. Am. J. Kidney Dis. 2016, 48, 37–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noguchi, M.; Yamaguchi, S.; Koshino, Y.; Kimura, A.; Miyagi, S. Validity of body impedance analysis for evaluating body composition in patients undergoing long-term hemodialysis. J. Phys. Ther. Sci. 2015, 27, 1649–1652. [Google Scholar] [CrossRef] [Green Version]
- Paudel, K.; Visser, A.; Burke, S.; Samad, N.; Fan, S.L. Can Bioimpedance Measurements of Lean and Fat Tissue Mass Replace Subjective Global Assessments in Peritoneal Dialysis Patients? J. Ren. Nutr. 2015, 25, 480–487. [Google Scholar] [CrossRef]
- Huang, C.X.; Tighiouart, H.; Beddhu, S.; Cheung, A.K.; Dwyer, J.T.; Eknoyan, G.; Beck, G.J.; Levey, A.S.; Sarnak, M.J. Both low muscle mass and low fat are associated with higher all-cause mortality in hemodialysis patients. Kidney Int. 2010, 77, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Savalle, M.; Gillaizeau, F.; Maruani, G.; Puymirat, E.; Bellenfant, F.; Houillier, P.; Fagon, J.-Y.; Faisy, C. Assessment of body cell mass at bedside in critically ill patients. AJP Endocrinol. Metab. 2012, 303, E389–E396. [Google Scholar] [CrossRef]
- Talluri, A.; Liedtke, R.; Mohamed, E.I.; Maiolo, C.; Martinoli, R.; De Lorenzo, A. The application of body cell mass index for studying muscle mass changes in health and disease conditions. Acta Diabetol. 2003, 40, S286–S289. [Google Scholar] [CrossRef]
- Kakiya, R.; Shoji, T.; Tsujimoto, Y.; Tatsumi, N.; Hatsuda, S.; Shinohara, K.; Kimoto, E.; Tahara, H.; Koyama, H.; Emoto, M.; et al. Body fat mass and lean mass as predictors of survival in hemodialysis patients. Kidney Int. 2006, 70, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Broers, N.J.H.; Usvyat, L.A.; Marcelli, D.; Bayh, I.; Scatizzi, L.; Canaud, B.; van der Sande, F.M.; Kotanko, P.; Moissl, U.; Kooman, J.P. Season affects body composition and estimation of fluid overload in haemodialysis patients: Variations in body composition; a survey from the European MONDO database. Nephrol. Dial. Transpl. 2014, 30, 678–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Kutáč, P.; Kopecký, M. Comparison of body fat using various bioelectrical impedance analyzers in university students. Acta Gymnica 2015, 45, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Reddan, D.N.; Szczech, L.A.; Hasselblad, V.; Lowrie, E.G.; Lindsay, R.M.; Himmelfarb, J.; Owen, W.F. Intradialytic blood volume monitoring in ambulatory hemodialysis patients: A randomized trial. J. Am. Soc. Nephrol. 2005, 16, 2162–2169. [Google Scholar] [CrossRef] [Green Version]
- Chamney, P.W.; Kramer, M.; Rode, C.; Kleinekofort, W.; Wizemann, V. A new technique for establishing dry weight in hemodialysis patients via whole body bioimpedance. Kidney Int. 2002, 61, 2250–2258. [Google Scholar] [CrossRef] [Green Version]
- Kaysen, G.A.; Zhu, F.; Sarkar, S.; Heymsfield, S.B.; Wong, J.; Kaitwatcharachai, C.; Kuhlmann, M.K.; Levin, N.W. Estimation of total-body and limb muscle mass in hemodialysis patients by using multifrequency bioimpedance spectroscopy. Am. J. Clin. Nutr. 2005, 82, 988–995. [Google Scholar] [CrossRef] [Green Version]
- Devolder, I.; Verleysen, A.; Vijt, D.; Vanholder, R.; Van Biesen, W. Body composition, hydration, and related parameters in hemodialysis versus peritoneal dialysis patients. Perit. Dial. Int. 2010, 30, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Davenport, A. Effect of Intra-abdominal Dialysate on Bioimpedance-Derived Fluid Volume Status and Body Composition Measurements in Peritoneal Dialysis Patients. Perit. Dial. Int. 2013, 33, 578–579. [Google Scholar] [CrossRef] [Green Version]
- Guo, Q.; Yi, C.; Li, J.; Wu, X.; Yang, X.; Yu, X. Prevalence and Risk Factors of Fluid Overload in Southern Chinese Continuous Ambulatory Peritoneal Dialysis Patients. PLoS ONE 2013, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Panorchan, K.; Nongnuch, A.; El-Kateb, S.; Goodlad, C.; Davenport, A. Changes in muscle and fat mass with haemodialysis detected by multi-frequency bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2015, 69, 1109–1112. [Google Scholar] [CrossRef] [Green Version]
- Fürstenberg, A.; Davenport, A. Assessment of Body Composition in Peritoneal Dialysis Patients Using Bioelectrical Impedance and Dual-Energy X-Ray Absorptiometry. Am. J. Nephrol. 2011, 33, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Khosravi, M.; Massart, A.; Potluri, M.; Davenport, A. Are serum to dialysate sodium gradient and segmental bioimpedance volumes associated with the fall in blood pressure with hemodialysis? Int. J. Artif. Organs 2014, 37, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Kandouz, S.; Mohamed, A.S.; Zheng, Y.; Sandeman, S.; Davenport, A. Reduced protein bound uraemic toxins in vegetarian kidney failure patients treated by haemodiafiltration. Hemodial. Int. 2016, 20, 610–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oei, E.; Paudel, K.; Visser, A.; Finney, H.; Fan, S.L. Is overhydration in peritoneal dialysis patients associated with cardiac mortality that might be reversible? World J. Nephrol. 2016, 5, 448–454. [Google Scholar] [CrossRef]
- Moissl, U.; Arias-Guillén, M.; Wabel, P.; Fontseré, N.; Carrera, M.; Campistol, J.M.; Maduell, F. Bioimpedance-Guided Fluid Management in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 1575–1582. [Google Scholar] [CrossRef] [Green Version]
- Wabel, P.; Chamney, P.; Moissl, U.; Jirka, T. Importance of whole-body bioimpedance spectroscopy for the management of fluid balance. Blood Purif. 2009, 27, 75–80. [Google Scholar] [CrossRef]
- Grangé, S.; Hanoy, M.; Le Roy, F.; Guerrot, D.; Godin, M. Monitoring of hemodialysis quality-of-care indicators: Why is it important? BMC Nephrol. 2013, 14, 109. [Google Scholar] [CrossRef] [Green Version]
- Passauer, J.; Petrov, H.; Schleser, A.; Leicht, J.; Pucalka, K. Evaluation of clinical dry weight assessment in haemodialysis patients using bioimpedance spectroscopy: A cross-sectional study. Nephrol. Dial. Transpl. 2010, 25, 545–551. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. The BCM—Body Composition Monitor for Managing Fluid in People Ha Having Ving Dialysis; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- Medrano, G.; Leonhardt, S.; Zhang, P. Modeling the Influence of Body Position in Bioimpedance Measurements. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 3934–3937. [Google Scholar]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Chamney, P.W.; Wabel, P.; Moissl, U.M.; Müller, M.J.; Bosy-Westphal, A.; Korth, O.; Fuller, N.J. A whole-body model to distinguish excess fluid from the hydration of major body tissues. Am. J. Clin. Nutr. 2007, 85, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Davenport, A.; Hussain Sayed, R.; Fan, S. The effect of racial origin on total body water volume in peritoneal dialysis patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 2492–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, S.; Davenport, A. Does Loss of Residual Renal Function Lead to Increased Volume Overload and Hypertension in Peritoneal Dialysis Patients? Perit. Dial. Int. 2015, 35, 753–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, S.; Davenport, A. Does increased glucose exposure lead to increased body fat and reduced lean body mass in anuric peritoneal dialysis patients? Eur. J. Clin. Nutr. 2014, 68, 1253–1254. [Google Scholar] [CrossRef] [PubMed]
- McCafferty, K.; Fan, S.; Davenport, A. Extracellular volume expansion, measured by multifrequency bioimpedance, does not help preserve residual renal function in peritoneal dialysis patients. Kidney Int. 2014, 85, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, C.H.Y.; de Craen, A.J.M.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.M.; Westendorp, R.G.J.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Pelle, G.; Branche, I.; Kossari, N.; Tricot, L.; Delahousse, M.; Dreyfus, J.-F. Is 3-compartment bioimpedance spectroscopy useful to assess body composition in renal transplant patients? J. Ren. Nutr. 2013, 23, 363–366. [Google Scholar] [CrossRef]
- Bučar Pajek, M.; Čuk, I.; Leskošek, B.; Mlinšek, G.; Buturović Ponikvar, J.; Pajek, J. Six-minute walk test in renal failure patients: Representative results, performance analysis and perceived dyspnea predictors. PLoS ONE 2016, 11, e0150414. [Google Scholar] [CrossRef] [Green Version]
- Tabinor, M.; Davies, S.J. The use of bioimpedance spectroscopy to guide fluid management in patients receiving dialysis. Curr. Opin. Nephrol. Hypertens. 2018, 27, 406–412. [Google Scholar] [CrossRef]
- Ponce, P.; Pham, J.; Gligoric-Fuerer, O.; Kreuzberg, U. Fluid management in haemodialysis: Conventional versus body composition monitoring (BCM) supported management of overhydrated patients. Port. J. Nephrol. Hypertens. 2014, 28, 239–248. [Google Scholar]
- Huan-Sheng, C.; Yeong-Chang, C.; Ming-Hsing, H.; Fan-Lieh, T.; Chu-Cheng, L.; Tsai-Kun, W.; Hung-Ping, C.; Sze-Hung, H.; Hsien-Chang, C.; Chia-Chen, L. Application of bioimpedance spectroscopy in Asian dialysis patients (ABISAD-III): A randomized controlled trial for clinical outcomes. Int. Urol. Nephrol. 2016, 48, 1897–1909. [Google Scholar] [CrossRef]
- Lara, D.M. Comparação da Pressão Arterial, Aferida por Mapa, Após Sessão de Hemodiálise, em Pacientes Submetidos à Avaliação Clínica ou Bioimpedância, Para Determinação de Peso Seco. Master’s Thesis, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil, 2010. [Google Scholar]
- Onofriescu, M.; Hogas, S.; Voroneanu, L.; Apetrii, M.; Nistor, I.; Kanbay, M.; Covic, A.C. Bioimpedance-guided fluid management in maintenance hemodialysis: A pilot randomized controlled trial. Am. J. Kidney Dis. 2014, 64, 111–118. [Google Scholar] [CrossRef]
- Vermeiren, E.; Ysebaert, M.; Van Hoorenbeeck, K.; Bruyndonckx, L.; Van Dessel, K.; Van Helvoirt, M.; De Guchtenaere, A.; De Winter, B.; Verhulst, S.; Van Eyck, A. Comparison of bioimpedance spectroscopy and dual energy X-ray absorptiometry for assessing body composition changes in obese children during weight loss. Eur. J. Clin. Nutr. 2020, 1–12. [Google Scholar] [CrossRef]
- Rymarz, A.; Szamotulska, K.; Niemczyk, S. Comparison of skinfold thicknesses and bioimpedance spectroscopy to dual-energy x-ray absorptiometry for the body fat measurement in patients with chronic kidney disease. Nutr. Clin. Pract. 2017, 32, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Jaffrin, M.Y.; Morel, H. Body fluid volumes measurements by impedance: A review of bioimpedance spectroscopy (BIS) and bioimpedance analysis (BIA) methods. Med. Eng. Phys. 2008, 30, 1257–1269. [Google Scholar] [CrossRef]
- Mager, J.R.; Sibley, S.D.; Beckman, T.R.; Kellogg, T.A.; Earthman, C.P. Multifrequency bioelectrical impedance analysis and bioimpedance spectroscopy for monitoring fluid and body cell mass changes after gastric bypass surgery. Clin. Nutr. 2008, 27, 832–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.W.Y.; Ngoh, C.L.Y.; Chua, H.R.; Haroon, S.; Wong, W.K.; Lee, E.J.C.; Lau, T.W.L.; Sethi, S.; Teo, B.W. Evaluation of different bioimpedance methods for assessing body composition in Asian non-dialysis chronic kidney disease patients. Kidney Res. Clin. Pract. 2019, 38, 71. [Google Scholar] [CrossRef] [Green Version]
- Keane, D.F.; Baxter, P.; Lindley, E.; Moissl, U.; Pavitt, S.; Rhodes, L.; Wieskotten, S. The Body Composition Monitor: A flexible tool for routine fluid management across the haemodialysis population. Biomed. Phys. Eng. Express 2017, 3, 35017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mialich, M.S.; Sicchieri, J.M.F.; Junior, A.A.J. Analysis of body composition: A critical review of the use of bioelectrical impedance analysis. Int. J. Clin. Nutr. 2014, 2, 1–10. [Google Scholar]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Variable | Mean ± SD | SE | CV | r | Mean. Diff | Cronbach Alpha | Average Rel. Error |
|---|---|---|---|---|---|---|---|---|
| All | ICW_F | 22.87 ± 3.49 | 0.36 | 0.15 | 0.80 | −5.33 * | 0.89 | 0.24 |
| ICW_I | 28.20 ± 4.01 | 0.40 | 0.14 | |||||
| ECW_F | 19.06 ± 2.38 | 0.24 | 0.12 | 0.91 | 1.45 * | 0.95 | −0.07 | |
| ECW_I | 17.60 ± 2.24 | 0.22 | 0.13 | |||||
| TBW_F | 41.92 ± 5.33 | 0.53 | 0.13 | 0.84 | −3.68 * | 0.91 | 0.08 | |
| TBW_I | 45.61 ± 6.25 | 0.62 | 0.14 | |||||
| FTM_F | 24.90 ± 9.82 | 0.97 | 0.39 | 0.90 | 4.55 * | 0.94 | −0.17 | |
| BFM_I | 20.35 ± 8.67 | 0.86 | 0.43 | |||||
| OH_F | 0.67 ± 1.21 | 0.08 | 1.80 | |||||
| Healthy controls | ICW_F | 24.42 ± 3.03 | 0.42 | 0.10 | 0.86 | −5.58 * | 0.92 | 0.23 |
| ICW_I | 30.00 ± 3.13 | 0.43 | 0.13 | |||||
| ECW_F | 19.62 ± 1.91 | 0.26 | 0.10 | 0.87 | 1.27 * | 0.93 | −0.06 | |
| ECW_I | 18.37 ± 1.79 | 0.25 | 0.10 | |||||
| TBW_F | 44.05 ± 4.44 | 0.62 | 0.10 | 0.77 | −3.91 * | 0.86 | 0.09 | |
| TBW_I | 47.97 ± 5.26 | 0.73 | 0.11 | |||||
| FTM_F | 24.70 ± 9.60 | 1.34 | 0.49 | 0.95 | 4.92 * | 0.97 | −0.19 | |
| BFM_I | 19.77 ± 8.50 | 1.19 | 0.34 | |||||
| OH_F | 0.63 ± 1.21 | 0.08 | 1.93 | |||||
| HD patients | ICW_F | 21.30 ± 3.25 | 0.45 | 0.15 | 0.68 | −5.09 * | 0.80 | 0.24 |
| ICW_I | 26.39 ± 4.01 | 0.56 | 0.15 | |||||
| ECW_F | 18.48 ± 2.65 | 0.37 | 0.14 | 0.92 | 1.63 * | 0.96 | −0.08 | |
| ECW_I | 16.85 ± 2.39 | 0.33 | 0.14 | |||||
| TBW_F | 39.79 ± 5.32 | 0.74 | 0.13 | 0.84 | −3.47 * | 0.91 | 0.08 | |
| TBW_I | 43.24 ± 6.31 | 0.88 | 0.15 | |||||
| FTM_F | 25.10 ± 10.14 | 1.41 | 0.40 | 0.85 | 4.18 * | 0.91 | −0.13 | |
| BFM_I | 20.91 ± 8.88 | 1.24 | 0.35 | |||||
| OH_F | 0.64 ± 1.22 | 0.08 | 1.89 |
| Mean Difference | Sig. | |
|---|---|---|
| Diff. ICW | −0.49020 | 0.307 |
| Diff. ECW | −0.35882 | 0.072 |
| Diff. TBW | −0.45490 | 0.499 |
| Diff. FM | 0.74118 | 0.389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pajek, M.; Sember, V.; Čuk, I.; Šimenko, J.; Pajek, J. Comparison of Body Composition Monitor and InBody 720 Bioimpedance Devices for Body Composition Estimation in Hemodialysis Patients and Healthy Controls. Symmetry 2021, 13, 150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13010150
Pajek M, Sember V, Čuk I, Šimenko J, Pajek J. Comparison of Body Composition Monitor and InBody 720 Bioimpedance Devices for Body Composition Estimation in Hemodialysis Patients and Healthy Controls. Symmetry. 2021; 13(1):150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13010150
Chicago/Turabian StylePajek, Maja, Vedrana Sember, Ivan Čuk, Jožef Šimenko, and Jernej Pajek. 2021. "Comparison of Body Composition Monitor and InBody 720 Bioimpedance Devices for Body Composition Estimation in Hemodialysis Patients and Healthy Controls" Symmetry 13, no. 1: 150. https://0-doi-org.brum.beds.ac.uk/10.3390/sym13010150