
Respirable Coal Mine Dust: A Review of Respiratory Deposition, Regulations, and Characterization
by
Younes Shekarian
1,2, 
Elham Rahimi
1,2,
Mohammad Rezaee
2,*,
Wei-Chung Su
3 and
Pedram Roghanchi
1,* 1
Department of Mineral Engineering, New Mexico Institute of Mining and Technology, Socorro, NM 87801, USA
2
Center for Critical Minerals, John and Willie Leone Family Department of Energy and Mineral Engineering, Earth and Mineral Sciences (EMS) Energy Institute, The Pennsylvania State University, University Park, State College, PA 16802, USA
3
Department of Epidemiology, Human Genetics, and Environmental Sciences, School of Public Health, University of Texas Health Science Center at Houston, Houston, TX 77030, USA
*
Authors to whom correspondence should be addressed.
Minerals 2021, 11(7), 696; https://0-doi-org.brum.beds.ac.uk/10.3390/min11070696
Submission received: 14 May 2021
/
Revised: 17 June 2021
/
Accepted: 22 June 2021
/
Published: 28 June 2021
(This article belongs to the Special Issue Mineralogy and Characteristics of Occupational and Environmental Dust Exposures)
Abstract
:In the late 1990s, despite years of efforts to understand and reduce coal worker’s pneumoconiosis (CWP) prevalence from more than 30% in 1970 to less than 4.2%, the level of occurrence among the US coal miners increased unexpectedly. The recent resurgence of lung diseases has raised concerns in the scientific and regulatory communities. In 2014, the United States Mine Safety and Health Administration (MSHA) issued a new dust rule changing the respirable coal mine dust (RCMD) exposure limits, measurement technology, and sampling protocol. The analysis for probable causes for the substantial increase in the CWP incidence rate is rather complicated. This paper aims to conduct a review of RCMD respiratory deposition, health effects, monitoring, regulations, and particle characteristics. The primary sources of RCMD along with the health risks from potential exposure are highlighted, and the current RCMD exposure regulations of the major coal producer countries are compared. A summary of RCMD characterization studies from 1972 to the present is provided. A review of the literature revealed that numerous factors, including geological and mining parameters, advancements in mining practices, particle characteristics, and monitoring approaches are considered to contribute to the recent resurgence of RCMD lung diseases. However, the root causes of the problem are still unknown. The effectiveness of the new dust rules in the United States will probably take years to be correctly assessed. Therefore, future research is needed to understand the relationship between RCMD particle characteristics and lung deposition, and the efficacy of current monitoring practices to measure the true dose of RCMD exposure.
1. Introduction
Dust, as an inherent byproduct of mining, may impose various health and safety issues in mining operations. The term dust is used for solid particles in the air and is defined as airborne particles, usually in a size range of 1 to 100μm [1,2]. Mineral clouds of dust generally occur when collisions, abrasions, cutting, crushing, and explosions break down rocks [3,4,5]. Such mechanical and chemical processes generate dust particles in various sizes, typically formed in irregular shapes [4,6,7]. Generally, the amount of dust generated during excavation is estimated to be approximately 3% of the total mass of the excavated materials [8]. The chance of a dust particle to deposit in the human respiratory system depends significantly on particle size or aerodynamic diameter (defined as the diameter of a unit density particle (1 g/cm3) with the similar settling velocity of the particle) [9,10,11,12]. Respirable dust generally refers to particles having an aerodynamic diameter < 10 μm and a median cut-point (d50) of 4 μm [13,14,15].
The United States Mine Safety and Health Administration (MSHA) states that “Any respirable dust in the mine atmosphere is considered respirable coal mine dust to which miners are exposed and, when measured, is counted for determining compliance with the respirable dust standard” (79 Fed. Reg. 24,866). It is estimated that 40–95% of respirable coal mine dust (RCMD) in the underground coal mine is pure coal and the rest contains particles generated from cutting the roof and floor, diesel equipment, rock dusting practices, etc. [16,17,18]. Dust generation depends on geological parameters and technical factors. Geological parameters include coal thickness, composition, cleavage, compactness, hardness, volatile matter, ash, and coal moisture content. Mining methods, cutting height, cutting equipment, and type and condition of cutting bits are among the contributing technical factors [8,19]. The primary sources of RCMD have been found to be coal seam and surrounded rock strata, intake air, diesel exhaust, mining operations, and rock dusting (Figure 1) [7,20,21,22,23,24,25]. The concentration of dust depends on the number of factors, including types of activity, the number of free surfaces in the cross-section walls, ventilation, and dust control practices.
Cumulative inhalation of RCMD can lead to severe lung diseases, including coal worker’s pneumoconiosis (CWP), silicosis, mixed dust pneumoconiosis, dust-related diffuse fibrosis (DDF), and progressive massive fibrosis (PMF) [27,28,29]. Black lung or CWP has been considered as a main concern among US coal workers since 1962 that followed by regulations to decrease the limits of dust exposure once in a while. In general, the regulations resulted in a significant decrease in the progression of respiratory lung diseases as well as the number of reported CWP cases by the late 1990s [11]. However, an unexpected increase in the number of CWP cases was reported in the late 1990s that were more chronic (Figure 2). Since the time of the disease to manifest is at least five years and can be latent to 10–30 years, the trend for CWP progression in the United States was descending to one-sixth of the earlier percentage in 2000. Since 2000, the trend started to change during mid-2010s, noting that recent CWP cases were more severe.
A considerable amount of research and analysis has investigated the root causes of the increase in lung diseases [7,10,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Nevertheless, identifying the leading causes of this drastic rise seems to be difficult. This paper provides a review of literature on RCMD penetration in the respiratory system and lung deposition, subsequent health problems, exposure limits and regulations, monitoring, and characterization techniques and particle characteristics. The current gaps in knowledge and future research needs are highlighted, and the importance of understanding the relationship between RCMD characterization and lung depositions are discussed.
2. Respirable Dust Deposition in the Human Respiratory System
A simplified schematic of the human respiratory system is shown in Figure 3. When breathing in, air flows through the nostrils and enters the nasal cavity, where, at the entrance, nose hairs coated with mucus are able to trap large particles of dust [43,44]. The main nasal airway (turbinate) assists to warm and moisturize the inhaled air before entering into the lung [43,45,46]. Once passing through the nasal airway, the inhaled air penetrates through the oropharynx, larynx, trachea, and then enters the lungs. The point where the inhaled air splits into the two mainstem bronchi is called the carina [44,45,47]. The right mainstem bronchus is wider and more vertical (and divides into three lobes or bronchi) than the left lung, which divides into two lobes bronchi [48,49,50,51]. The trachea and first three generations of bronchi are large airways, lined mostly by ciliated columnar cells and a handful of goblet cells that secrete mucus, helping to trap particles [44,52]. The ciliated columnar cells beat rhythmically together to move the mucus and any trapped particles from the air towards the pharynx, where they can be either spit out or swallowed, i.e., the mucociliary clearance mechanism [43,52,53].
After the first three generations of bronchi, the air passes through smaller bronchioles for 15–20 generations; the first 16 branching in the tracheobronchial (TB) region and the remaining in the alveolar region [47,48,54]. These conducting bronchioles receive oxygen from the bronchial arteries where the walls are similarly lined by ciliated columnar cells and mucus-secreting goblet cells [52,53]. These cells secrete glycosaminoglycan, a material that protects the bronchiolar or epithelium by helping to regenerate and replace damaged cells [52,53]. Eventually, the respiratory bronchioles end where there are millions of alveoli in the gas exchange region [50,54,55,56,57]. This is the final destination of the inhaled air, in which the wall is lined by thin epithelial cells called pneumocytes [48,52]. If a particle makes it deep into the lungs, there are alveolar macrophages that can swallow and move up the particle to the conducting bronchioles (slow phase of mucociliary clearance) [44,48].
There have been few reports that investigate the effect of physicochemical properties of coal dust including morphology and particle shape, size, composition, and functional groups on CWP [58]. Furthermore, several studies documented that nano-size coal particles are more toxic owing to their special physicochemical properties and ease of absorption by living organisms. These nanosized particles can also be suspected of having a significant contribution to the lung diseases [58,59,60]. In addition to the size of particles, the shape, in another word, angularity and sphericity, will significantly affect the respiratory deposition. For instance, the total deposition of µm-sized fibers and submicron oblate disks was found significantly higher for non-spherical particles compared to spherical particles [61,62]. In general, angular edges increase the inflammation since they can penetrate into the lung tissue. Those particles that contain toxic elements (e.g., Fe, Cd, Hg, Pb) are going to be dangerous if eventually enter into the blood stream. Detailed studies on the relation between particle shape and toxicity revealed that angular particles such as fibers, which have more roughness and sharp edges, have higher risk of toxicity compared to spherical particles [21,58,60].
There are a variety of mechanisms for particle deposition in the respiratory system, some depending on particle size. To illustrate the respiratory deposition of a particle based on its size, the human respiratory system can be simplified in three regions: the head region, the tracheobronchial region (TB), and the alveolar region (gas exchange region) [63,64,65,66,67,68]. Particles with an aerodynamic diameter of less than 100 μm are inhalable through the nasal and oral cavities in the head region. After entering into the respiratory system, large particles with large inertia may be trapped in the upper airways, while smaller particles with small inertia move along with the air and enter the lower airways [1,43,51,55,69,70]. The inhaled particles that fail to deposit in the respiratory system will be exhaled [42,44,48,58,59,60,61,62,63,64,65,66,70]. RCMD particles may include a considerable amount of fine or ultrafine particles from which the most damaging particles are probably those that are small enough to penetrate deep into the lungs. In light of this, diesel particulate matter (DPM) with a diameter of less than 1 µm is considered a concern for underground workers. Submicron particles are not cleared as efficiently as larger particles and have mobility within the respiratory system or beyond via translocation to blood [47,59].
The probability of particle deposition in different regions of the respiratory system as a function of the particle’s aerodynamic diameter is demonstrated in Figure 3. [43]. Almost all small particles (less than 10 nanometers in diameter) and more than 75% of large particles (10 micrometers in diameter) are inhalable, out of which roughly 20% of small particles and nearly all of the large particles are deposited in the head region. Total deposition in the TB region is relatively low. In this region, approximately 25% of small particles and 1.5% of large particles are deposited. The deposition of medium-size particles (300 nanometers in diameter) is higher if not already deposited in the head region. Near 42% of small and about 2% of large particles are deposited in the alveolar region [43,71,72,73]. A summary of lung deposition studies is presented in Table 1.
3. RCMD Exposure Health Risks and Global Disease Distribution
Exposure to RCMD may affect both human internal and external organs. These health effects include eye opacities, hearing loss, contagious illnesses, lung diseases, kidney diseases, cardiovascular problems, nervous system damage, and voice and skin disorders (Figure 4). Despite its effects on other vital organs, cumulative exposure to RCMD is well-known to result in obstructive pulmonary diseases, which are chronic, vulnerable, progressive, and possibly fatal [74,75,76]. In the United States, from 1995 to 2004, pneumoconiosis in coal miners resulted in more than 10,000 mortalities (79 Fed. Reg. 85, 1 May 2014). Pneumoconiosis was first defined by the British National Insurance (Industrial Injuries) Act in 1946 as “fibrosis of the lungs due to silica dust, asbestos dust or other dust and includes the condition known as dust retention.” [77]. The American Lung Association defines pneumoconiosis as a group of interstitial lung disease caused by overly breathing in dust particles that damage lungs tissues by scarring and finally impairing the ability to breath. Pneumoconiosis can be categorized as simple or complicated forms. The simple form called coal workers’ pneumoconiosis, or CWP, causes small scars in the lung tissue, while the complicated form presents with huge amount of scarring tissue known as progressive massive fibrosis, or PMF [78]. Based on the composition of the inhaled dust (i.e., organic and inorganic contaminants with known pro-inflammatory and carcinogenic properties such as coal, silica, iron, cadmium, lead, kaolin, and pyrite), and the exposure duration, different stages of CWP and severity, including pulmonary hypertension, cor pulmonale (defined as an alteration in the structure and function of the right ventricle (RV) of the heart caused by a primary disorder of the respiratory system), and death, may manifest with miscellaneous symptoms [19,38,79]. For either simple or complicated forms of pneumoconiosis, the injury involves the destruction of blood vessels and air sacs in the lungs. The scarring tissue becomes thick and stiff in a way that makes breathing strictly formidable. This is considered an interstitial pulmonary disease that mainly includes asbestosis, silicosis, fibrosis, and black lung or CWP.
Determining the interstitial lung disease (ILD) (i.e., a group of disorders that cause progressive scarring of lung tissue) in coal workers exposed to RCMD seems to be a complicated investigation. Most experiments have shown a robust dose-response in the relationship between RCMD and ILD. However, dose-response for pure coal dust has not been ruled-out [12,79]. Most of the investigations focus on studies that indicate that non-mineral coal dust has an independent impact on ILD progress [12,31,86,87]. Many of those tests were cross-sectional studies, with exposures to quartz to some extent, and a few studies have investigated the effect of smoking and age [12,86,88]. Brown et al. [6] provided an analysis of the thoracic and respirable fractions according to the three variables of age, sex, and activity level (light, moderate, and heavy) that affect the tidal volume (which is the lung volume representing the normal volume of air displaced between normal inhalation and exhalation when extra effort is not applied. In a healthy, young human adult, tidal volume is approximately 500 mL per inspiration or 7 mL/kg of body mass). This study predicted that an increase in activity intensity and airflow causes the impaction of particles with a greater cut-point range of aerodynamic diameter into the ET fraction. In addition to this estimation, [10] presented the thoracic and respirable fractions of ~3 μm in adults (female slightly less than male), while in children, these fractions were estimated as 5 μm and 4 μm, respectively [10].
A summary of lung deposition studies is presented in Table 1.

Table 1.
A summary of recent lung deposition studies for respirable dust [59].
Table 1.
A summary of recent lung deposition studies for respirable dust [59].
| Authors | Proposed Model | Methodology | Results |
|---|---|---|---|
| Brown et al. [10] | Modifications to International Commission on Radiological Protection (ICRP) model | Experimental and mathematical modeling based on the ICRP human respiratory model |
|
| Ghalati et al. [46] | Computational model | Lagrangian and Eulerian models |
|
| Rahimi-Gorji et al. [49] | - | Laminar-to-turbulent airflow, transport and deposition of micro-particles was performed by Eddy Interaction Model (EIM) from the oral cavity up to generation G6 by two-phase flow simulation |
|
| Nemati et al. [59] | A 5-lobe symmetric model | Simulation |
|
| Su et al. [89] | - | Mobile Aerosol Lung Deposition Apparatus (MALDA) |
|
| Choi & Kim [90] | Single-path trumpet model | Numerical method using Weibel’s lung model |
|
| Asgharian, et al. [91] | Multiple-Path Particle Deposition (MPPD) model of lobar deposition | Mathematical formulation using lung structural geometry |
|
Global Distribution of RCMD Lung Diseases
Owing to the lack of reliable statistics, estimation of the global prevalence of lung diseases related to coal mine dust is difficult. In developing nations, where job practices are not well regulated, the incidence rate is expected to be higher. RCMD lung diseases have deteriorated with tightly imposed restrictions on dust control in developed countries [23]. The frequency and intensity of RCMD lung diseases over the last 20 years have resurged in several nations [8,23,92,93]. In the United States, this trend declined to 2.1% in the 1990s, then unexpectedly increased (to 3.2%) in the late 1990s [11,23]. Each year in China, on average, 10,000 patients employed in coal mines are added to the list of pneumoconiosis patients, and over 2500 miners die from this disease [8,94,95]. There were 122,333 new cases of pneumoconiosis reported between 1997 and 2009, ~44% of which were due to CWP, showing that its prevalence remained high (around 6.02%) [93]. In Germany, about 300 new compensated cases per year reported by 1994, which showed severe CWP mostly in retired coal miners [96] Among occupational diseases in Poland, the number of cases reported in coal mining (76.6% of those cases are CWP) is more than three times of other industries [8,34]. By 2017, the total number of pneumoconiosis cases reported was 7340, 80% of which were active and former employees of hard coal mines [8]. In Australia, between 1979 and 2002, 6% of total mining fatalities were classified as CWP, with the number of fatalities decreasing steadily over time [92,97]. Similarly, in India, the resurgence of pneumoconiosis in coal miners is relatively high [19,93]. In the United Kingdom, the incidence of CWP declined dramatically between 2004 and 2008 and has remained relatively stable since then [98].
4. RCMD Exposure Limits and Regulations in the Major Coal Producer Countries
RCMD is mainly regulated by reducing the exposure duration and the total mass of RCMD in the working areas [11,28,37,79]. However, RCMD exposure limits and regulations vary in different countries. While the record of occupational disease recognition goes back to 1706 [99], revealing the first case of CWP in a Scottish coal mine in 1831, stimulating other nations to regulate RCMD concentration in underground coal mines [100], the lack of occupational disease monitoring and medical knowledge and equipment caused the late attention of coal-producing countries to recognize CWP cases. For example, the first case of CWP in the United States was revealed during the 1920s, China in 1949, India in 1956, Poland in 1966, and Germany in 1974 [8,19,23,97,99,101]. The major coal producer countries (shown in Table 2 commenced with setting regulations for RCMD exposure limits (listed in Table 2).
In 2018, China produced approximately 3,500 million tones (Mt) of coal as the top coal producer, of which 90% is extracted from underground mines [23,102,103]. Interestingly, the permissible exposure limits of total dust in China varies between 2 mg/m3 to 20 mg/m3 (1 mg/m3 for coal with 50% silica content to 6 mg/m3 coal with 5% silica content [23,95]). India, in second place, produced 764 Mt with only 10% from underground mines [19,23,102,103]. The maximum exposure limit (MEL) is 3 mg/m3 when respirable crystalline silica (RCS) in respirable dust is less than 5%. However, if free silica is greater than 5%, then MEL should be determined by 15/(% RCS) [23,104]. The regulations in the United States, as the third coal producer, is discussed below in detail. Australia in the fourth place produced 502 Mt, which only 20% of coal mines are underground mines [23,102,103]. The exposure limit in Australia is 1.5 mg/m3 for coal with silica content less than 5% in general [105]. South Africa produced 257 Mt, 50% of which was from underground coal mines. In South Africa, the RCMD concentration limit is set to 2 mg/m3 for coal with less than 5% silica content [23,102,103,106].
In the United States, the setting of regulations on occupational diseases has nearly always led to a prolonged controversy among conflicting interests [23,34,107]. The manifestation of black lung disease was in the 1960s when 30% of workers who had more than 25 years of tenure in underground coal mines were diagnosed with CWP [23]. Since then, considerable medical treatment efforts have been implemented, while no certain cure for CWP has been achieved [28]. Therefore, the effort has been to reduce the number of lung disease incidents by alleviating the exposure of RCMD in working areas. In 1969, the very first RCMD concentration limit of 3.0 mg/m3 coal dust concentration was introduced and was lowered to 2.0 mg/m3 with crystalline silica or quartz less than 5% in 1972. The black lung disease trend from the 1970s to the late 1990s significantly declined. In 1995, the National Institute for Occupational Safety and Health (NIOSH) recommended that the permissible exposure limit (PEL) should be lowered to 1 mg/m3 for RCMD and 0.05 mg/m3 for silica concentration. This was followed by the 2014 (effected on 1 August, 2016) MSHA dust rule, in which the PEL was lowered to 1.5 mg/m3 for RCMD and 0.1 mg/m3 for quartz, along with changes in sampling technique and duration [23].
Previous studies indicated that CWP prevalence is related to the exposure of RCMD to coal workers. CWP can even effectively progress among coal workers after exposure removal [1,2,4,108]. The risk of CWP prevalence is associated with RCMD composition, concentration, and exposure duration [4,22,109]. Doney et al. [74,110] investigated the mass concentrations of RCMD and RCS using the MSHA database between 1982 and 2017. The results of 681,497 RCMD and 210,944 respirable silica dust (RCS) samples in underground mines showed an average of 0.55 mg/m3 and 0.038 mg/m3 for RCMD and RCS concentrations, respectively. However, in surface mines, the average values were 0.17 mg/m3 and 0.02 mg/m3, respectively. The number of RCMD samples exceeding the PEL in underground mines was three times greater than surface mines. The geometric mean of RCMD for different occupational group in underground coal mines was reported as longwall worker (1.02 mg/m3), continuous miner operator and helper (0.73 mg/m3), cutting machine operator and helper (0.67 mg/m3), auger (0.65 mg/m3), roof bolter (0.59 mg/m3), stopping builder/ventilation man/mason (0.57 mg/m3), blaster and helper (0.50 mg/m3), coal drill operator and helper (0.48 mg/m3), beltman/conveyor man/belt cleaner (0.46 mg/m3), and loading machine operator (0.44 mg/m3) [74,110].
Table 2.
Top 10 coal producers in the world with a dust exposure limit.
| Country | Production Ranking (% of World Production) * | Underground/Surface | Seam Properties | Common Underground Mining Method | Regulation Year | Dust Exposure Limits | Sampling | Reference | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Coal Type | Thickness | Coal (mg/m3) | Total Respirable PEL ** (mg/m3) | Silica Content PEL (mg/m3 or %) | |||||||
| China | 1 (45.2%) | 90% U 10% S | 75%bituminous 20% anthracite | Deep thick | LW | 2002 | 2.5 | 4 | <10% | PGS | [23,94,95] |
| India | 2 (9.9%) | 90% S 10% U | anthracite bituminous | thick short deep | R&P 10% LW | 1987 | 2 10/(% silica) | - | <5% >5% | Indian Device | [19,23] |
| United States | 3 (8.9%) | 73% S 27% U | bituminous sub-bituminous | thin | R&P LW | 2016 | 1.5 | - | 0.1 mg/m3 | PGS | [23] |
| Australia | 4 (6.5%) | 80% S 20% U | anthracite bituminous sub-bituminous | thick | 90% LW | 2020 | 1.5 | - | 0.05 mg/m3 | PGS (QL: Monitoring include travel time between mine entrance and coal face, NSW: Miner’s underground work period) | [105] |
| Indonesia | 5 (6.2%) | Not available at the time of the review. | |||||||||
| Russia | 6 (5.4%) | Not available at the time of this review. | |||||||||
| South Africa | 7 (3.3%) | 51% U 49% S | sub-bituminous bituminous anthracite | relatively thin | 90% R&P LW | 1997 | 2 | - | <5% | PGS | [23,106] |
| Germany | 8 (2.2%) | 3% U | bituminous anthracite | thin | LW | 1991 | - | 4 | 0.2–0.15 | AGS | [23,96] |
| Poland | 9 (1.6%) | 53% U | anthracite | thin slanted | LW | 1985 | 0.3 1 | 4 | over 50% 2–50% | PGS | [23,34] |
| Kazakhstan | 10 (1.5%) | -- | -- | -- | -- | -- | 1 2 4 10 | -- | >70% 10–70% 2–10% <2% | -- | [111] |
* Data obtained from [99]. ** The permissible exposure limit (PEL) is a legal limit in the United States for exposure of an employee to a chemical substance or physical agent such as Respirable Coal Mine Dust (RCMD).
5. Progress in RCMD Monitoring
In 1970, the coal mine operators and MSHA started using the “coal mine dust personal sampler unit” (CMDSU) to determine the concentration of respirable dust in the mine environment. This unit was being utilized to test the underground atmosphere by drawing mine air through a filter cassette that collects respirable dust. At the end of a full shift, the cassettes were collected and shipped to a specialized laboratory for analysis. The collected dust on each filter was then weighed under controlled conditions to determine the average concentration of respirable coal dust during the production shifts. An immediate problem with this method was that it takes several days (sometimes weeks) before the mine operators and MSHA to receive the results. Another critical problem with this method was that personal sampling for respirable coal mine dust could be only performed as an average concentration during a full shift. As a result, high transient/short-term concentrations of respirable coal dust events were not captured through the use of the 10-h time-weighted-average (TWA) sampling method [4,23,59,108].
In the 1990s, NIOSH began conducting research and development to produce a new type of personal dust monitoring unit that could provide readings of dust levels in a near-continuous manner. This new device known as the “continuous personal dust monitor” (CPDM) allows the mine operators to promptly identify and respond to dust concentrations exceeding MSHA requirements. Through near real-time readings, the instrument allows the mine operators to determine dust concentrations, trigger dust control systems, and evaluate the effectiveness of the dust control methods [59,108].
Presently, the PDM3700 instrument manufactured by Thermo-Fisher Scientific is used to measure dust concentrations in the production workings in near real-time. During various MSHA–Industry dust partnership meetings and through NIOSH visits to mine sites, mine operators and mine workers have indicated that a second generation CPDM would need to be designed and manufactured to reduce its size, weight, and operating noise. The construction and operating features of this unit are still “mass-based” and “filter-based,” which means that the instrument uses a particulate filter mounted on an oscillating microbalance to measure dust concentrations. As a result, this instrument can only measure the combined mass of respirable coal dust, plus any respirable mineral dust and organic matter that is present in the mine air. The total mass of the RCMD collected by a respirable personal sampler is assumed to all become the miner’s RCMD dose. Nonetheless, the mass concentration does not necessarily represent the true RCMD dose received by the coal miner, especially for RCMD less than 4 μm. Not all of the RCMD inhaled into the miner’s respiratory tract will deposit in the lung to become the RCMD dose. A portion of the inhaled RCMD could be exhaled out of the respiratory tract during exhalation without deposition. This phenomenon is especially significant for submicron RCMD [7,108]. It is also critical to identify different constituents of RCMD in order to have a comprehensive understanding of the health effects. For a thorough chemical analysis, several filter media are needed to collect integrated samples during working shifts. For example, Polycarbonate-membrane (PC) filter is used for morphological and elemental analysis by scanning electron microscopy (SEM). Quartz fiber filter is used for organic analysis of RCMD, or Teflon filter is used for mineralogic analysis by X-ray diffraction (XRD) [112]. The efficiency captured by collector should be maximum for those filters since the total mass of the RCMD collected on a filter is assumed to all become the miner’s exposure dose. The summery of instrument development is presented in Table 3.
6. RCMD Characteristics and Characterization Techniques
To properly understand the characterization of RCMD, a more detailed depiction of the respirable dust is required. Even now, no fundamental approach to systematically and provisionally classify coal mine dust has been proposed [17,21,22,23,109,113,114,115]. Nevertheless, various methods have been used to characterize RCMD, including scanning electron microscopy-energy-dispersive X-ray spectroscopy (SEM-EDX or SEM-EDS), thermogravimetric analysis (TGA), XRD, inductively coupled plasma-mass spectrometry (ICP-MS), Fourier Transform Infra-Red (FTIR) spectroscopy, atomic absorption spectrometry, and X-ray photoelectron spectroscopy (XPS) [5,7,9,17,21,109,116,117,118,119,120,121]. A standard methodology using SEM-EDX was proposed by Sellaro et al. [21] to characterize RCMD particles. Despite being widely used in various metallurgical applications and industrial mineral processing, the SEM-EDX technique was not applied for RCMD characterization before Sellaro et al. [21]. This approach is being progressively used to precisely explain the structure and composition of airborne particles that pose health hazards in industrial and environmental settings. For example, methodologies have been recently developed to study nano-size particles in the field of active welding [89,122]. To accurately describe a particle, different characteristics, including particle size, length, and shape are measured by SEM-EDX. Therefore, this characterization technique can provide a comprehensive array of data in a thorough analysis of RCMD.
The thermogravimetry analysis (TGA) is used to measure the changes in the weight of a dust sample when exposed to temperature [116]. The weight change typically plots as the function of temperature in a thermogram. The data is used to explain chemical changes in the sample when heated [5,116]. For many years, this technique has been used to determine the non-combustible mineral fraction of coal [22,23,123,124]. TGA is a convenient and inexpensive method for obtaining additional knowledge about dust samples. Particularly, the mass percentages of coal and non-coal can be measured by TGA, and the carbonate and non-carbonate mineral fractions can also be estimated [125]. The data obtained by TGA may help researchers better understand how mining activities affect dust composition as well as provide insights into miner health outcomes in terms of dust characteristics. The TGA data for respirable dust samples taken from seven Appalachian mines showed that the carbonate and non-carbonate mass fractions can be very high in the non-coal fraction, while the coal to total mineral mass ration is very low [125].
A summary of RCMD characterization studies from 1972 to the present is provided in Table 4. According to the National Academies of Sciences, Engineering, and Medicine (NAS) [23], the early investigation on dust particle size was presented in 1959 at the Johannesburg conference, in which initial efforts were to measure the size of RCMD particles accumulated in the lungs based on mineral autopsy results. Based on the analyzed pathological samples from the lungs of a former coal miner, dust particles with a diameter less than 5 μm were determined to enter the air exchange region [3,21]. However, a drawback of the analysis was that only a series of particle size deposition values of approximately 3 to 10 μm were covered by the available data [5,10]. Many researchers have suggested that further investigations should address the physical and chemical properties of RCMD and its dependency on the geographic regions [28,97,119]. Morgan et al. [30] suggested that the variations in CWP prevalence cannot be fully explained only by exposure duration, and all contributing factors should be taken into account. For example, the physical and chemical compositions of coal may be responsible for geographical variations in prevalence [30]. A few studies have been conducted to investigate the total RCMD composition and its relationship with the exposure health risks [7,15,20,22,41,126]. The relationship between the CWP prevalence and bioavailable content of coal dust studied by Huang et al. [41] showed a correlation with bioavailable iron and pyritic sulfur, but not with coal rank and silica. Furthermore, a review of several reports revealed that rapid pneumoconiosis cases are likely to be misdiagnosed with silicosis as CWP [36]. Several reasons including high silica content of mines in the southern Appalachian region, thin coal seams containing a high percentage of quartz, small sizes of mines, and an increase in the mines’ shift hours resulting in coal and silica dust accumulation support this claim [7,38].
In the United States, the investigation of RCMD content in the Appalachia region has revealed more details about probable sources of RCMD. A higher concentration of alumino-silicate and carbonate in Appalachian mines is primarily attributed to rock dusting application and cutting or drilling of rock strata [7,22]. Furthermore, particle size analysis based on sampling location showed that samples collected from active cutting or drilling operations and in the return airways have elongated and smaller-sized dust particles than in the intake airways [7,8,19,22,79]. Analysis of the overburden roof and the underlying floor strata of Appalachian basin rock indicated that northern Appalachian mines have a higher percentage of carbonate particles than central and southern Appalachian mines due to higher rock dusting of mines producing from relatively thicker coal seams [7,15,20,22,122,127].
The traditional method of RCMD monitoring based on current regulation relies on the concentration of silica and total mass fraction [23,119,125]. The recent resurgence in rapidly progressing CWP may be localized in the central Appalachian area [23]. Several investigators have proposed a number of potential reasons for the continued prevalence of pneumoconiosis of coal workers, including longer shift times, changes in mining technology, increased mining of higher quartz-bearing coal, and extraction of roof and floor rock strata for mining thin coal seams [11,39,40,79]. The content and characteristics of RCMD particles based on the geographical location of a coal mine requires further studies [7,38,128]. The issue of particle size versus particle mass and total mass or silica content is still in debate [7,23]. Due to the detection limits of instruments, it has been challenging to characterize very fine dust particles in a sample [7,17]. Therefore, there seems to be not enough information about the relative occurrence or impact of submicron (100–1000 nm) particles and their correlation with the exposure health impacts [7,129]. A comprehensive study for both submicron and supra-micron RCMD particles was conducted by Sarver et al. [7] in which the size distribution of RCMD for 76 samples from US coal mines were analyzed. The result showed that RCMD samples are largely submicron rather than supra-micron particles, despite probably ignoring the finest particles. In their experiment, more than 50% of particles accounts for very fine particles (including DPM) and over 75% of total particulates are in the range of submicron. Among different sources of RCMD (i.e., rock strata, rock dusting), diesel particulate is most likely in submicron size, while other sources can be observed in both submicron and supra-micron size ranges [7].
Table 4.
A summary of RCMD characterization studies worldwide.
| Study | Sampling Locations (Sites) | No. of Samples | Instrument | Characteristic Technique | Results |
|---|---|---|---|---|---|
| Corn et al. (1972 & 1973) [109,117] | Western Pennsylvania (Mathies and Robena mines) | 6 | Horizontal Elutriator |
|
|
| Morgan et al. (1973) [30] | Pennsylvania (8 mines), West Virginia (9 mines), Kentucky (3 mines), Virginia (2 mines), Alabama (2 mines), Illinois (2 mines), Utah (2 mines), Ohio (1 mine), Indiana (1 mine), Colorado (1 mine) | 9076 miners | A large field study to determine the prevalence of CWP and Fibrosis |
|
|
| Stein and Corn (1975) [130] | Pennsylvania (Pittsburgh, Lower Freeport, and Lower Kittanning) | 8 | Millipore GS membrane filter |
|
|
| Kriegseis and Scharmann, (1985) [131] | Germany (Ruhr coal field) | 1 | Bergbau-Forschung GmbH, Essen, with BAT II Infrared spectroscopy |
|
|
| Lee (1986) [132] | Pennsylvania (4 mines) West Virginia (1 mine) Ohio (4 mines) | 99 | Cascade impactors |
|
|
| Kim (1989) [113] | Appalachian bituminous coalfield (Upper Freeport, Pittsburgh, Kittanning, Coalburg, and Pocahontas) | 9 | Cascade impactors |
|
|
| Grayson and Peng (1989) [119] | US (1mine) | 10 | Dorr-Oliver 10-mm cyclones and DuPont P2500 |
|
|
| Wallace et al. (1994) [120] | Illinois (1 coal mine) Pennsylvania (6 coal mines and 1 clay mine) West Virginia (1 powdered tunnel quartz rock) | 10 | Not mentioned |
|
|
| Harrison et al. (1997) [121] | Pennsylvania (7 mines) Illinois (2 mines) Colorado (1 mine) | 12 | Cyclone, filter, and impactor |
|
|
| Sapko et al. (2007) [114] | MSHA’s Districts bituminous districts | 163 * | Sieve |
|
|
| Jing et al. (2010) [9] | China (Jining and Shandong) | 4 | Laser particle size instrument(Beckman Coulter LS 13320, the United States) |
|
|
| Sellaro et al. (2015) [21] | Central Appalachia (1 mine) | 3 | MSA Escort ELF pump with a Dorr-Oliver cyclone |
|
|
| Johann-Essex et al. (2017) [22] | Central Appalachia (6 mines) Northern Appalachia (2 mines) | 210 | ELF sampling pumps and cyclones |
|
|
| Sarver et al., (2019) [7] | Central Appalachia (6 mines) Northern Appalachia (2 mines) | 76 (sample sets) | Escort ELF air sampling pumps with 10-mm nylon Dorr-Oliver cyclones |
|
|
| Sarver et al. (2020) [128] | Central Appalachia (15 mines) Northern Appalachia (5 mines) Mid-west/Illinois basin (2 mines) Western basin (2 mines) | 166 | Oliver cyclones |
|
|
* The dust samples collected by mine inspectors for compliance with 30 CFR 75.403. ** The dust samples collected by mine inspectors for compliance with 30 CFR 75.403.
7. Discussion
The analysis for probable reasons for the substantial increase in the CWP incidence rate is rather complicated. Changes in mining practices, technology advancement, thin coal seam mining, rock dusting, and new cutting machinery may each contribute to the occurrence of new CWP cases in the United States [4,5,10,23,133,134]. Further investigations are required to identify the root causes of the resurgence of the lung diseases and the contributing factors [7,10,23]. The majority of disease incidences are reported to be in underground coal miners. Therefore, the vast majority of research studies focus on RCMD monitoring and control in underground mines. However, it is worth mentioning that respiratory lung disease is also a prevalent health issue among surface coal miners.
Generally, the total mass concentration of RCMD and fraction of silica mass are two metrics that are currently used for RCMD monitoring and control [7,23,135]. In the United States, CPDM indicates significant technological progress, as it presents near real-time observations of ambient RCMD concentrations while carrying out operations. In cases that RCMD content in the air exceeds the permitted level, the CPDM alerts miner executives to act immediately, either by changing workers’ location or by implementing mining practices in order to mitigate RCMD content (MSHA, PH89-V-1 (27)) [23,133]. However, the efficacy of the current monitoring approach based on the measurement of RCMD total “mass-concentration” is still unclear. Many have questioned whether reducing the exposure limits will actually target the root cause of the problem. Although the connections between coal miners RCMD exposure and respiratory diseases have been studied for decades, the contributing factors that cause the progression of the disease are not yet identified [7,12,21,22,23,125,129,136].
Several researchers aimed to investigate the health effect of quartz as a major inorganic part of RCMD [115,121]. However, other studies indicated that neither CWP nor PMF could be credited for quartz unless the concentration of quartz reaches 10% [137,138,139,140]. The coal rank is another contributing factor that may play a role in the progression of CWP [33,141]. Several studies confirmed that there is a higher risk of CWP for higher coal rank, even at the same level of RCMD concentrations [38,142]. Gamble et al. [38] proposed higher rank coal as a plausible factor for CWP prevalence within the Appalachian region. In many bituminous coal mines, the higher prevalence of CWP has also been linked to a higher quartz content in respirable dust [143]. Previous studies indicated that an apparent link between the coal rank and CWP may be attributed to the particle surface charge and mineralogical composition of RCMD [127]. However, the causal effects of coal rank have not been exclusively investigated [108]. Moreover, there are research studies suggesting that unlike bioavailable iron and pyritic sulfur, there is no correlation between coal rank and CWP [41,115]. Beer et al. [12] conducted the first systematic review of the coal dust exposure to investigate whether the prevalence of ILD is pure coal or coal mixed with silica minerals. In this review, the author found that the level of evidence is limited for causal links between exposure to pure coal powder and ILD. In order to support the hypothesis, however, further analysis of the data related to miners exposed to none or very small content of mineral particles is required.
It is clear that more research on physical and chemical properties of RCMD is needed to understand the root causes of CWP incidences and its recent resurgence. Characteristics parameters such as particle size distribution (particularly in the smaller fractions enriched with minerals), mineral composition, trace element presence, and particle shape and angularity are all important parameters that need to be examined closely.
The machinery specifications and mineralogical composition of the coal and surrounding rock strata should be considered as contributing factors to the total dust concentration and characteristics of the RCMD [9,115,118,121]. Depending on the coal mining operations and the mining equipment, generated RCMD can be coarse or fine in size. Both coarse and fine coal mine dust can inevitably be inhaled by coal miners while performing their work. Various studies suggest that RCMD concentration varies depending on the locations within underground mines. Miners working between the shearer and the air outlet from the longwall, at the junction of the longwall with the tailgate, loading-shearer, and drilling operators are at the highest risk of occupational lung diseases [7,8,143].
To date, there has been no comprehensive study to investigate the relationship between RCMD characterization and respiratory deposition. Characterization results should be used as guidance for prospective lung deposition and toxicity research that takes into account the differences of RCMD source, particle size distribution, and mineralogical groups to which miners are exposed to cumulative RCMD [141]. Many studies demonstrate that by increasing the tidal volume (whether by increment activity or through the ventilation system), a more considerable amount of dust particles will be deposited in the human respiratory system. Furthermore, size fraction of particle deposition may differ by the breathing scenario, pause fraction, and breathing frequency for adults and young workers. It is crucial to identify different constituents of RCMD in order to have a better understanding of the health effects. Not all of the RCMD particles inhaled into a miner’s respiratory tract will be deposited in the lung. A portion of the inhaled RCMD will be exhaled out of the respiratory tract during exhalation. Therefore, the total amount of RCMD inhaled may not be the representative of the actual RCMD exposure dose. This phenomenon is especially significant for submicron particles [122,144]. Currently, the mine health related RCMD personal sampling is based on the mass concentration, which may not correctly represent the true RCMD dose received by coal miners, especially for particles less than 4 μm in size [23]. Therefore, the correctness of using mass-concentration-based RCMD sampling as an index to protect miner’s RCMD exposure is questionable. The number-concentration-based RCMD samples could be an alternative and ideal index for RCMD dose estimations. There are variety of parameters that affect RCMD characterization (i.e., mineralogy properties, particle size, shape) in mines. For instance, recent findings by Sarver et al. [128] supported the hypothesis that RCMD characterizations among mining regions differ substantially. Mineralogy composition and distributions of the RCMD particle size, which is impacted by geographic location, are essential to understanding the recent CWP resurgence [128].
Overall, the effectiveness of MSHA’s new dust rule (i.e., decreasing the PELs and use of CPDM) will possibly take years to be properly assessed [29]. Nonetheless, the current regulation requires sampling of RCMD mass concentration using CPDM devices (79 Fed. Reg. 84, May 1, 2014) [145]. The gravimetric method is also used to validate CPDM measurements. There are, however, many factors that contribute to the development of lung diseases, including, but not limited to, submicron-size fractions, particle number, DPM, and elemental content. Although time and costs for the characterization of RCMD are likely to be prohibitive for regular monitoring, they offer valuable information to better understand the composition of RCMD and its relationship with the development of lung diseases among coal miners.
8. Conclusions
In the United States, the increase in the rate of CWP in the mid-1990s has renewed the urge among medical and science researchers to investigate the primary root causes of the problem. This paper provided a review of RCMD research studies focusing on characterization, respiratory deposition, and exposure health effects. There have been tremendous efforts to identify the contributing factors in developing lung diseases among coal miners. The analysis of possible explanations for this dramatic increase seems very complicated. Technological development, level of automation, thin coal seam mining, application of rock dusting, and changes in mining practices can all contribute to the increase of lung diseases. No particular medical therapy is useful in controlling and removing the effect of coal mine dust lung diseases such as CWP. Hence, attempts to reduce RCMD exposure along with medical monitoring for early disease diagnosis and elimination from exposure is crucial to protect the health of a miner.
Current MSHA regulation requires the use of a CPDM for the measurement of RCMD mass concentrations in near real-time and determining compliance with the regulatory exposure limit. However, the precision of using mass-concentration-based RCMD sampling as an index to protect miner’s RCMD exposure is questionable. The accuracy of particle number-concentration-based RCMD monitoring systems should be assessed, and their effectiveness should be compared with the mass-based monitoring method. Furthermore, it is crucial to investigate the relationship between the characterization and lung deposition of RCMD in order to understand the true exposure dosage. The distribution of CWPs varies in different US coal regions. Several studies indicated that small mines located in Central Appalachia are at a high risk of CWP prevalence. Therefore, future research studies should focus on identifying the key difference in characteristics of coal dust between underground mines in coal regions in the western and eastern United States.
Author Contributions
Conceptualization, Y.S., E.R., M.R. and P.R.; Methodology, Y.S., E.R.; Investigation, Y.S., E.R., M.R., P.R. and W.-C.S.; Writing-Original Draft Preparation, Y.S., and E.R.; Writing-Review & Editing, M.R., P.R. and W.-C.S.; Visualization, Y.S., E.R. and W.-C.S.; Supervision, M.R. and P.R.; Project Administration, M.R., P.R. and W.-C.S.; Funding Acquisition, P.R., M.R. and W.-C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Institute for Occupational Safety and Health (NIOSH) grant number [75D30119C06390].
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Hazard Prevention and Control in the Work Environment: Airborne Dust; Occupational and Environmental Health, Department of the Protection of the Human Environment: Geneva, Switzerland, 1999; WHO/SDE/OEH/99.14. [Google Scholar]
- Energy Information Administration (EIA). International Energy Statistics: Primary Coal Production. 2018. Available online: https://www.eia.gov/beta/international/rankings/#?pid=7&cy=20141T (accessed on 20 December 2019).
- McPherson, M.J. Subsurface Ventilation and Environmental Engineering; Virginia Polytechnic Institute and State University: Blacksburg, VA, USA, 1993. [Google Scholar]
- Colinet, J.F.; Rider, J.P.; Listak, J.M.; Organiscak, J.A.; Wolfe, A.L. Best Practices for Dust Control in Coal Mining. Department of Health and Human Services; Centers for Disease Control and Prevention National Institute for Occupational Safety and Health Office of Mine Safety and Health Research Pittsburgh: Pittsburgh, PA, USA, 2010. Available online: https://www.cdc.gov/niosh/mining/works/coversheet861.html (accessed on 30 January 2010).
- Scaggs, M.L. Development and Implication of a Standard Methodology for Respirable Coal Mine Dust Characterization with Thermogravimetric Analysis. Master’s Thesis, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA, 2016. [Google Scholar]
- Nousiainen, T. Optical modeling of mineral dust particles: A review. J. Quant. Spectrosc. Radiat. Transf. 2009, 110, 1261–1279. [Google Scholar] [CrossRef]
- Sarver, E.; Kelesa, C.; Rezaee, M. Beyond conventional metrics: Comprehensive characterization of respirable coal mine dust. Int. J. Coal Geol. 2019, 207, 84–95. [Google Scholar] [CrossRef]
- Brondy, J.; Tutak, M. Exposure to harmful dusts on fully powered longwall coal mines in Poland. Int. J. Environ. Res. Public Health 2018, 15, 1846. [Google Scholar] [CrossRef] [Green Version]
- Jing, Y.; Xiukun, W.; Jianguang, G.; Gaiping, L. Surface characteristics and wetting mechanism of respirable coal dust. Min. Sci. Technol. 2010, 20, 365–371. [Google Scholar]
- Brown, J.S.; Gordon, T.; Price, O.; Asgharian, B. Thoracic and Respirable Particle Definitions for Human Health Risk Assessment; National Center for Environmental Assessment, US Environmental Protection Agency: Raleigh, NC, USA, 2013. [Google Scholar] [CrossRef] [Green Version]
- Laney, A.S.; Weissman, D.N. Respiratory diseases caused by coal mine dust. J. Occup. Environ. Med. 2014, 56, 18–22. [Google Scholar] [CrossRef] [Green Version]
- Beer, C.; Kolstad, H.A.; Søndergaard, K.; Bendstrup, E.; Heederik, D.; Olsen, K.E.; Omland, Ø.; Petsonk, E.; Sigsgaard, T.; Sherson, D.L. A systematic review of occupational exposure to coal dust and the risk of interstitial lung diseases. Eur. Clin. Respir. J. 2017, 4, 1264711. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization (ISO). Air Quality-Particle Size Fraction Definitions for Health-Related Sampling; ISO Standard 7708; International Organization for Standardization (ISO): Geneva, Switzerland, 1995. [Google Scholar]
- American Conference of Governmental Industrial Hygienists (ACGIH). Particle Size-Selective Sampling for Health-Related Aerosols; Vincent, J.H., Ed.; Air Sampling Procedures Committee: Cincinnati, OH, USA, 1999; ISBN 1-1882417-30-5. [Google Scholar]
- Occupational Safety and Health Administration. Occupational Exposure to Respirable Crystalline Silica—Review of Health Effects Literature and Preliminary Quantitative Risk Assessment; Occupational Safety and Health Administration: Washington, DC, USA, 2010; OSHA-2010-0034. [Google Scholar]
- Walton, W.H.; Dodgson, J.; Hadden, G.G.; Jacobsen, M. The Effect of Quartz and Other Non-Coal Dusts in Coal Workers’ Pneumoconiosis. In Inhaled Particles IV Part 2, Oxford ed.; Pergamon Press: Oxford, UK, 1977; pp. 669–689. [Google Scholar]
- National Institute for Occupational Safety and Health. Criteria for a Recommended Standard. Occupational Exposure to Respirable Coal Mine Dust; National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 1995. [Google Scholar]
- International Agency for Research on Cancer. Monographs on the Evaluation of Carcinogenic Risks to Humans, Silica, Some Silicates, Coal Dust and Para-Aramid Fibrils; World Health Organization: Geneva, Switzerland, 1997; p. 68. [Google Scholar]
- Pandey, J.K.; Agarwal, D.; Gorain, S.; Dubey, R.K.; Vishwakarma, M.K.; Mishra, K.K.; Pal, A.K. Characterization of respirable dust exposure of different category of workers in Jharia Coalfields. Arab. J. Geosci. 2017, 10, 183. [Google Scholar] [CrossRef]
- Schatzel, S.J.; Stewart, B.W. A provenance study of mineral matter in coal from Appalachian basin coal mining regions and implications regarding the respirable health of underground coal workers: A geochemical and Nd isotope investigation. Int. J. Coal Geol. 2012, 94, 123–136. [Google Scholar] [CrossRef]
- Sellaro, R.; Sarver, E.; Baxter, D. A standard characterization methodology for respirable coal mine dust using SEM-EDX. Resources 2015, 4, 939–957. [Google Scholar] [CrossRef]
- Johann-Essex, V.; Keles, C.; Sarver, E. A computer-controlled SEM-EDX routine for characterizing respirable coal mine dust. Minerals 2017, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- National Academies of Sciences, Engineering, and Medicine. Monitoring and Sampling Approaches to Assess Underground Coal Mine Dust Exposures; The National Academies Press: Washington, DC, USA, 2018; pp. 1–150. [Google Scholar] [CrossRef]
- Watts, W.F.; Cantrell, B.K.; Ambs, J.L.; Rubow, K.L. Diesel Exhaust Aerosol Levels in Underground Coal Mines. In Underground Mines: Measurement and Control of Particulate Emissions, Proceedings of the Bureau of Mines Information and Technology Transfer Seminar, Minneapolis, MN, USA, 29–30 September 1992; US Department of the Interior: Pittsburgh, PA, USA, 1992; pp. 31–39, IC 9324. [Google Scholar]
- Ping, C.; Guang, X. A review of the health effects and exposure-responsible relationship of diesel particulate matter for underground mines. Int. J. Min. Sci. Technol. 2017, 27, 831–838. [Google Scholar]
- Schatzel, S.J. Identifying Sources of Respirable Quartz and Silica Dust in Underground Coal Mines in Southern West Virginia, Western Virginia, and Eastern Kentucky; National Institute for Occupational Safety and Health, Pittsburgh Research Laboratory: Pittsburgh, PA, USA, 2009. [Google Scholar]
- Cullinan, P.; Muñoz, X.; Suojalehto, H.; Agius, R.; Jindal, S.; Sigsgaard, T.; Blomberg, A.; Charpin, D.; Annesi-Maesano, I.; Gulati, M.; et al. Occupational lung diseases: From old to novel exposures to effective preventive strategies. Lancet Respir. Med. 2017, 5, 445–455. [Google Scholar] [CrossRef]
- Almberg, K.S.; Halldin, C.N.; Blackley, D.J.; Laney, A.S.; Storey, E.; Rose, C.S.; Go, L.H.T.; Cohen, R.A. Progressive massive fibrosis resurgence identified in US coal miners filing for black lung benefits, 1970–2016. Ann. Am. Thorac. Soc. 2018, 15, 1420–1426. [Google Scholar] [CrossRef]
- Hall, N.B.; Blackley, D.J.; Halldin, C.N.; Laney, A.S. Current review of pneumoconiosis among US coal miners. Curr. Environ. Health Rep. 2019, 6, 137–147. [Google Scholar] [CrossRef]
- Morgan, W.K.; Burgess, D.B.; Jacobson, G.; O’Brien, R.J.; Pendergrass, E.P.; Reger, R.B.; Shoub, E.P. The prevalence of coal workers’ pneumoconiosis in US coal miners. Arch. Environ. Health Int. J. 1973, 27, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.F.; Burns, J.; Copland, L. Coalworkers’ simple pneumoconiosis and exposure to dust at 10 British coalmines. Br. J. Ind. Med. 1982, 39, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heppleston, A.G. Prevalence and pathogenesis of pneumoconiosis in coal workers. Environ. Health Perspect. 1988, 78, 159–170. [Google Scholar] [CrossRef]
- Attfield, M.D.; Morring, K. An investigation into the relationship between coal workers’ pneumoconiosis and dust exposure in US coal miners. Am. Ind. Hyg. Assoc. 1992, 53, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Marek, K.; Lebecki, K. Occurrence and prevention of coal miners’ pneumoconiosis in Poland. Am. J. Ind. Med. 1999, 36, 610–617. [Google Scholar] [CrossRef]
- Castranova, V.; Vallyathan, V. Silicosis and coal workers’ pneumoconiosis. Environ. Health Perspect. 2000, 108 (Suppl. 4), 675–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.F.; Grayson, R.L.; Metz, E.A. Disease and illness in US mining, 1983–2001. J. Environ. Med. 2004, 46, 1272–1277. [Google Scholar]
- Vallyathan, V.; Landsittel, D.P.; Petsonk, E.L.; Kahn, J.; Parker, J.E.; Oslowy, K.T.; Green, F.H. The influence of dust standards on the prevalence and severity of coal worker’s pneumoconiosis at autopsy in the United States of America. Arch. Pathol. Lab. Med. 2011, 135, 1550–1556. [Google Scholar] [CrossRef] [Green Version]
- Gamble, J.F.; Reger, R.B.; Glenn, R.E. Rapidly progressing coal workers pneumoconiosis as a confounding risk factor in assessing coal mine dust safe exposure levels. J. Clin. Toxicol. 2011, S1, 3. [Google Scholar] [CrossRef] [Green Version]
- Beck, T.W. Coal Workers’ Pneumoconiosis in US Coal Mines; A Review of Exposures, Intervention and Outcomes. Master’s Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2014. [Google Scholar]
- Blackley, D.J.; Halldin, C.N.; Wang, M.L.; Laney, A.S. Small mine size is associated with lung function abnormality and pneumoconiosis among underground coal miners in Kentucky, Virginia and West Virginia. Occup. Environ. Med. 2014, 71, 690–694. [Google Scholar] [CrossRef]
- Huang, X.; Li, W.; Attfield, M.D.; Nadas, A.; Frenkel, K.; Finkelman, R.B. Mapping and prediction of coal workers’ pneumoconiosis with bioavailable iron content in the bituminous coals. Environ. Health Perspect. 2005, 113, 964–968. [Google Scholar] [CrossRef]
- Manojkumar, N.; Srimuruganandam, B.; Shiva Nagendra, S.M. Application of multiple-path particle dosimetry model for quantifying age specified deposition of particulate matter in human airway. Ecotoxicol. Environ. Saf. 2019, 168, 241–248. [Google Scholar] [CrossRef]
- Hinds, W. Aerosol Technology: Properties, Behavior, and Measurement of Airborne Particles; Chapter 11; University of Virginia Library, Interlibrary Services: Charlottesville, VA, USA, 1999. [Google Scholar]
- International Commission on Radiological Protection (ICRP). Human Respiratory Tract Model for Radiological Protection; International Commission on Radiological Protection (ICRP): Ottawa, ON, Canada, 1994; p. 24. ISSN 0146-6453. [Google Scholar]
- Hofmann, W. Modelling inhaled particle deposition in the human lung-a review. J. Aerosol Sci. 2011, 42, 693–724. [Google Scholar] [CrossRef]
- FarhadiGhalati, P.; Keshavarzian, E.; Abouali, O.; Faramarzi, A.; Tu, J.; Shakibafard, A. Numerical analysis of micro-and nano-particle deposition in a realistic human upper airway. Comput. Biol. Med. 2012, 42, 39–49. [Google Scholar] [CrossRef]
- Ahookhosh, K.; Pourmehran, O.; Aminfara, H.; Mohammadpourfard, M.; Sarafraz, M.M.; Hamishehkar, H. Development of human respiratory airway models: A review. Eur. J. Pharm. Sci. 2020, 145, 105233. [Google Scholar] [CrossRef]
- Martonen, T.B.; Schroeter, J.D.; Hwang, D.; Fleming, J.S.; Conway, J.H. Human lung morphology model for particle deposition studies. Inhal. Toxicol. 2000, 12, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Rahimi-Gorji, M.; Gorji, T.B.; Gorji-Bandpy, M. Details of regional particle deposition and airflow structures in a realistic model of human tracheobronchial airways: Two-phase flow simulation. Comput. Biol. Med. 2016, 74, 1–17. [Google Scholar] [CrossRef]
- Rajput, P.; Izhar, S.; Gupta, T. Deposition modeling of ambient aerosols in human respiratory system: Health implication of fine particles penetration into pulmonary region. Atmos. Pollut. Res. 2019, 10, 334–343. [Google Scholar] [CrossRef]
- Islam, M.S.; Paul, G.; Ong, H.X.; Young, P.M.; Gu, Y.T.; Saha, S.C. A review of respiratory anatomical development, air flow characterization and particle deposition. Int. J. Environ. Res. Public Health 2020, 17, 380. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.S.; Zeman, K.L.; Bennett, W.D. Ultrafine particle deposition and clearance in the healthy and obstructed lung. Am. J. Respir. Crit. Care Med. 2002, 166, 1240–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martonen, T.B.; Rosati, J.A.; Isaacs, K.K. Modeling Deposition of Inhaled Particles. In Aerosols Handbook; Chapter 8; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Weibel, E.R. Geometric and Dimensional Airway Models of Conductive, Transitory and Respiratory Zones of the Human Lung. In Morphometry of the Human Lung; Academic Press: Cambridge, UK, 1963; pp. 136–142. [Google Scholar]
- Soni, B.; Arra, N.; Aliabadi, S. Mesh Refinement Study of Flow and Particle Deposition in Human Lung Airway Model. In Proceedings of the 20th American Institute of Aeronautics and Astronautics (AIAA), Computational Fluid Dynamics Conference, Honolulu, HI, USA, 27–30 June 2011. [Google Scholar]
- Nemati, H.; Saidi, M.S.; Hosseini, V. Modeling particle deposition in the respiratory system during successive respiratory cycles. Sci. Iran. Bull. 2020, 27, 215–228. [Google Scholar] [CrossRef]
- Saber, E.M.; Heydari, G. Flow pattern sand deposition fraction of particles in the range of 0.1–10 mm at trachea and the first third generation sunder different breathing conditions. Comput. Biol. Med. 2012, 42, 631–638. [Google Scholar] [CrossRef]
- Liu, T.; Liu, S.H. The impacts of coal dust on miners’ health: A review. Environ. Res. 2020, 190, 109849. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, E. Investigation of Respirable Coal Mine Dust (RCMD) and Respirable Crystalline Silica (RCS) in the U.S. Underground and Surface Coal Mines. No. 28156748. In PROQUESTMS ProQuest Dissertations & Theses A&I; New Mexico Institute of Mining and Technology: Socorro, NM, USA, 2020; Available online: https://0-www-proquest-com.brum.beds.ac.uk/openview/f3c2daa112cb5f32401430d0dc2f6d0f/1?pq-origsite=gscholar&cbl=18750&diss=y (accessed on 30 December 2020).
- Buzea, C.; Pacheco, I.; Robbie, K. Nanomaterials and nanoparticles: Sources and toxicity. Biointerphases 2007, 2, Mr17-71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, R. A Computer Model for the Simulation of Nonspherical Particle Dynamics in the Human Respiratory Tract. Phys. Res. Int. 2012, 2012, 142756. [Google Scholar] [CrossRef] [Green Version]
- Riediker, M.; Zink, D.; Kreyling, W.; Oberdörster, G.; Elder, A.; Graham, U.; Lynch, I.; Duschl, A.; Ichihara, G.; Ichihara, S.; et al. Particle toxicology and health—Where are we? Part. Fibre Toxicol. 2019, 16, 19. [Google Scholar] [CrossRef]
- Lippmann, M.; Albert, R.E. The effect of particle size on the regional deposition of inhaled aerosols in the human respiratory tract. Am. Ind. Hyg. Assoc. J. 1969, 30, 257–275. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, I.S.; Lourenco, R.V. Deposition of aerosols in pulmonary disease. Arch. Intern. Med. 1973, 131, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Landahl, H.D. On the removal of airborne droplets by the human respiratory tract: I The lung. Bull. Math. Biophys. 1950, 12, 43–56. [Google Scholar] [CrossRef]
- Gerrity, T.R.; Lee, P.S.; Hass, F.R.; Marinelli, A.; Werner, P.; Lourenco, R.V. Calculated deposition of inhaled particles in the airway generations of normal subject. J. Appl. Physiol. 1974, 47, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.S.; Zhou, Y.; Su, W.C. Deposition of Particles in Human Mouth–Throat Replicas and a USP induction port. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Heyder, J.; Rudolf, G. Mathematical models of particle deposition in the human respiratory tract. J. Aerosol Sci. 1984, 15, 697–707. [Google Scholar] [CrossRef]
- Su, W.C.; Ku, B.K.; Kulkarni, P.; Cheng, Y.S. Deposition of graphene nanomaterial aerosols in human upper airways. J. Occup. Environ. Hyg. 2016, 13, 48–59. [Google Scholar] [CrossRef] [Green Version]
- Duan, M.; Liu, L.; Da, G.; Géhin, G.; Nielsen, P.V.; Weinreich, U.M.; Lin, B.; Wang, Y.; Zhang, T.; Sun, W. Measuring the Administered Dose of Particles on the Facial Mucosa of a Realistic Human Model; John Wiley & Sons: Hoboken, NJ, USA, 2019; Volume 30, pp. 108–116. [Google Scholar]
- Sturm, R. Particles in the lungs of patients with chronic bronchitis-Part 1: Deposition modeling. J. Public Health Emerg. 2019, 3, 5. [Google Scholar] [CrossRef]
- Ohsaki, S.; Mitani, R.; Fujiwara, S.; Nakamura, H.; Watano, S. Effect of particle-wall interaction and particle shape on particle deposition behavior in human respiratory system. Pharm. Soc. Jpn. Chem. Pharm. Bull. 2019, 67, 1328–1336. [Google Scholar] [CrossRef] [Green Version]
- Khac, V.; Bui, H.; Moon, J.Y.; Chae, M.; Park, D.; Lee, Y.C. Prediction of aerosol deposition in the human respiratory tract via computational models: A review with recent updates. Atmosphere 2020, 11, 137. [Google Scholar] [CrossRef] [Green Version]
- Doney, B.C.; Blackley, D.; Hale, J.M.; Halldin, C.; Kurth, L.; Syamlal, G.; Laney, A.S. Respirable coal mine dust in underground mines, United States, 1982–2017. Am. J. Ind. Med. 2019, 62, 478–485. [Google Scholar] [CrossRef]
- Morgan, W.K. Industrial bronchitis. Br. J. Ind. Med. 1978, 35, 285–291. [Google Scholar] [CrossRef]
- Perret, J.L.; Plush, B.; Lachapelle, P.; Hinks, T.S.C.; Walter, C.; Clarke, P.; Irving, L.; Brady, P.; Dharmage, S.C.; Stewart, A. Coal mine dust lung disease in the modern era. Asian Pac. Soc. Respirol. 2017, 22, 662–670. [Google Scholar] [CrossRef]
- Sutherland, C.L. Pneumoconiosis—Its effects and complications. Occup. Med. 1959, 10, 4–15. [Google Scholar] [CrossRef]
- Douglas, A.N.; Robertson, A.; Chapman, J.S.; Ruckley, V.A. Dust exposure, dust recovered from the lung, and associated pathology in a group of British coalminers. Br. J. Ind. Med. 1986, 43, 795–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zosky, G.R.; Hoy, R.F.; Silverstone, E.J.; Brims, F.J.; Miles, S.; Johnson, A.R.; Gibson, P.G.; Yates, D.H. Coal workers’ pneumoconiosis Australian prospective. Med. J. Aust. 2016, 204, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Ruckley, V.A.; Gauld, S.J.; Chapman, J.S.; Davis, J.M.; Douglas, A.N.; Fernie, J.M.; Jacobsen, M.; Lamb, D. Emphysema and dust exposure in a group of coal workers. Am. Rev. Respir. Dis. 1983, 129, 528–532. [Google Scholar]
- Morfeld, P.; Lampert, K.; Ziegler, H.; Stegmaier, C.; Dhom, G.; Piekarski, C. Overall mortality and cancer mortality of coal miners: Attempts to adjust for healthy worker selection effects. Ann. Occup. Hyg. 1997, 41, 346–351. [Google Scholar] [CrossRef]
- Naidoo, R.; Robins, T.; Seixas, N. Respiratory Diseases Among South African Coal Miners. Safety in Mines Research Advisory Committee; Final Project Report; University of Natal (SA); University of Michigan: Ann Arbor, MI, USA, 2002. [Google Scholar]
- Cohn, C.A.; Laffers, R.; Simon, S.R.; O’Riordan, T.; Schoonen, M. Role of pyrite in formation of hydroxyl radicals in coal: Possible implications for human health. Part. Fiber Toxicol. 2006, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hendryx, M. Mortality from heart, respiratory, and kidney disease in coal mining areas of Appalachia. Int. Arch. Occup. Environ. Health 2009, 82, 243–249. [Google Scholar] [CrossRef]
- Petsonk, E.L.; Rose, C.; Cohen, R. Coal mine dust lung disease- new lessons from an old exposure. Am. J. Respir. Crit. Care Med. 2013, 187, 1178–1185. [Google Scholar] [CrossRef]
- Graber, J.M.; Stayner, L.T.; Cohen, R.A.; Conroy, L.M.; Attfield, M.D. Respiratory disease mortality among US coal miners; results after 37years of follow-up. Occup. Environ. Med. 2014, 71, 30–39. [Google Scholar] [CrossRef]
- Buchanan, D.; Miller, B.G.; Soutar, C.A. Quantitative relations between exposure to respirable quartz and risk of silicosis. Occup. Environ. Med. 2003, 60, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Casswell, C.; Bergman, I.; Rossiter, C.E. The relation of radiological appearance in simple pneumoconiosis of coal workers to the content and composition of the lung. Inhaled Part. 1970, 2, 713–726. [Google Scholar]
- Su, W.C.; Chen, Y.; Bezerra, M.; Wang, J. Respiratory deposition of ultrafine welding fume particles. J. Occup. Environ. Hyg. 2019, 16, 694–706. [Google Scholar] [CrossRef]
- Choi, J.; Kim, C.S. Mathematical Analysis of Particle Deposition in Human Lungs: An Improved Single Path Transport Model. Inhal. Toxicol. 2007, 19, 925–939. [Google Scholar] [CrossRef] [PubMed]
- Asgharian, B.; Hofmann, W.; Bergmann, R. Particle deposition in a multiple-path model of the human lung. Aerosol Sci. Technol. 2001, 34, 332–339. [Google Scholar] [CrossRef]
- Plush, B.; Ren, T.; Aziz, N. A Critical Evaluation of Dust Sampling Methodologies in Longwall Mining in Australia and the USA. In Proceedings of the 12th Coal Operators’ Conference, University of Wollongong & the Australasian Institute of Mining and Metallurgy, Wollongong, NSW, Australia, 16–17 February 2012; pp. 193–201. [Google Scholar]
- Schroedl, C.J.; Go, L.H.T.; Cohen, R.A. Coal Mine Dust Lung Disease: The Silent Coal Mining Disaster. Curr. Respir. Med. Rev. 2016, 12, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Pneumoconiosis in China—Advances in prevention and control. National Institute of Occupational Health and Poison Control, Chinese CDC. 2005. Available online: http://www.ilo.int/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/policy/wcms_110489.pdf (accessed on 30 November 2020).
- Yinlin, J.; Ting, R.; Peter, W.; Zhijun, W.; Zhaoyang, M.; Zhimin, W. A comparative study of dust control practices in Chinese and Australian longwall coal mines. Int. J. Min. Sci. Technol. 2016, 26, 199–208. [Google Scholar] [CrossRef]
- Morfeld, P.; Vautrin, H.J.; Kösters, A.; Lampert, K.; Piekarski, C. Components of coal mine dust exposure and the occurrence of prestages of pneumoconiosis. Appl. Occup. Environ. Hyg. 2011, 12, 973–979. [Google Scholar] [CrossRef]
- Zhao, J.Q.; Li, J.G.; Zhao, C.X. Prevalence of pneumoconiosis among young adults aged 24–44 years in a heavily industrialized province of China. J. Occup. Health 2019, 61, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Kingdom Health and Safety Executive. Silicosis and Coal Workers’ Pneumoconiosis Statistics in Great Britain. Annual Statistics. 2019. Available online: www.hse.gov.uk/statistics/ (accessed on 28 November 2020).
- Pendergrass, E.P.; Lainhart, W.S.; Bristol, L.J.; Felson, B.; Jacobson, G. Historical perspectives of coal workers’pneumoconiosis in the united states. Ann. N. Y. Acad. Sci. 1972, 200, 835–854. [Google Scholar] [CrossRef]
- Gregory, J.C. Case of Peculiar Black Infiltration of the Whole Lungs, Resembling Melanosis. Edinb. Med. Surg. J. 1831, 36, 389–394. [Google Scholar] [PubMed]
- Liang, Y.X.; Wong, O.; Fu, H.; Hu, T.X.; Xue, S.Z. The economic burden of pneumoconiosis in China. Occup. Environ. Med. 2003, 60, 383–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Petrolium (BP). Statistical Review of World Energy. 2019. Available online: https://www.bp.com/en/global/corporate/energy-economics/statistical-review-of-world-energy.html (accessed on 30 February 2020).
- Ener Data. Coal and Lignite Production. 2019. Available online: https://yearbook.enerdata.net/coal-lignite/coal-production-data.html (accessed on 30 March 2020).
- DGMS (Directorate General of Mines Safety, Government of India). Respirable Dust Measurements and Control to Prevent Pneumoconiosis in Mines. DGME (Tech.) (S&T) Circular. 2010. Available online: https://elibrarywcl.files.wordpress.com/2015/02/dgms-tech-st-circular-no-01-of-2010-respirable-dust.pdf1T (accessed on 8 February 2018).
- NSW Government. Resources Regulator in NSW. Revision to Coal and Silica Exposure Standard. Available online: https://www.resourcesregulator.nsw.gov.au/safety-and-health/topics/airborne-contaminants-and-dust (accessed on 31 July 2020).
- Belle, B.K.; Plessis, J.D. Recent Advances in Dust Control Technology on South African Underground Coal Mines. Mine Ventilation Society of South Africa. 2002. Available online: http://hdl.handle.net/2263/59517 (accessed on 30 October 2002).
- Stansbury, R.C. Progressive massive fibrosis and coal mine dust lung disease: The continued resurgence of a preventable disease. Ann. Am. Thorac. Soc. 2018, 15, 1394–1396. [Google Scholar] [CrossRef]
- Shekarian, Y. An Investigation of the Effects of Mining Parameters on the Prevalence of Coal Worker’s Pneumoconiosis (CWP) Risks among the US Coal Miners. Master’s Thesis, New Mexico Institute of Mining and Technology, Socorro, NM, USA, 2020. [Google Scholar] [CrossRef]
- Corn, M.; Stein, F.; Hammad, Y.; Manekshaw, S.; Bell, W.; Penkala, S.J. Physical and chemical characteristics of respirable coal mine dust. Ann. NY Acad. Sci. 1972, 200, 17–36. [Google Scholar] [CrossRef]
- Doney, B.C.; Blackley, D.; Hale, J.M.; Halldin, C.; Kurth, L.; Syamlal, G.; Laney, A.S. Respirable coal mine dust at surface mines, United States, 1982–2017. Am. J. Ind. Med. 2020, 63, 232–239. [Google Scholar] [CrossRef]
- Decree of the Government of the Republic of Kazakhstan (DGRK). Technical Regulation: Requirements for the Safety of Coal and Production Processes for Their Extraction, processing, storage and transport thereof. FAOLEX Database 2010, 731. (In Russian) [Google Scholar]
- Abbasi, B.; Wang, X.; Chow, J.C.; Watson, J.G.; Peik, B.; Nasiri, V.; Riemenschnitter, K.B.; Elahifard, M. Review of Respirable Coal Mine Dust Characterization for Mass Concentration, Size Distribution and Chemical Composition. Minerals 2021, 11, 426. [Google Scholar] [CrossRef]
- Kim, H. Characteristics of Airborne Coal Mine Dust and Its Implication to Coal Workers’ Pneumoconiosis. Ph.D. Thesis, West Virginia University, Morgantown, WV, USA, 1989. [Google Scholar]
- Sapko, M.J.; Cashdollar, K.L.; Green, G.M. Coal dust particle size survey of US mines. J. Loss Prev. Process. Ind. 2007, 20, 616–620. [Google Scholar] [CrossRef]
- Thakur, P. Advanced Mine Ventilation: Respirable Coal Dust, Combustible Gas and Mine Fire Control. In Advanced Mine Ventilation, 1st ed.; Elsevier Science: Amsterdam, The Netherlands, 2019; pp. 105–136. [Google Scholar] [CrossRef]
- Coats, A.W.; Redfern, J.P. Thermogravimetyric Analysis: A Review. Analyst 1963, 88, 906–924. [Google Scholar] [CrossRef]
- Corn, M.; Stein, F.; Hammad, Y.; Manekshaw, S.; Freedman, R.; Hartstein, A.M. Physical and chemical properties of respirable coal dust from two United States mines. Am. Ind. Hyg. Assoc. J. 1973, 34, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Freedman, R.W.; Toma, S.Z.; Lang, H.W. On-filter Analysis of Quartz in Respirable Coal Dust by Infrared Absorption and X-ray Diffraction. Am. Ind. Hyg. Assoc. J. 1974, 35, 411–418. [Google Scholar] [CrossRef]
- Grayson, R.L.; Peng, S.S. Characterization of Respirable Dust on a Longwall Panel—A Case Study; The National Institute for Occupational Safety and Health (NIOSH): Washington, DC, USA, 1989; pp. 328–345. [Google Scholar]
- Wallace, W.E.; Harrison, J.C.; Grayson, R.L.; Keane, M.J.; Bolsaitis, P.; Kennedy, R.D.; Wearden, A.Q.; Attfield, M.D. Aluminosilicate surface contamination of respirable quartz particles from coal mine dusts and from clay works dusts. Ann. Occup. Hyg. 1994, 38, 439–445. [Google Scholar]
- Harrison, J.C.; Brower, P.S.; Attfield, M.D.; Doak, C.B.; Keane, M.J.; Grayson, R.L.; Wallace, W.E. Surface composition of respirable silica particles in a set of US anthracite and bituminous coal mine dusts. J. Aerosol Sci. 1997, 28, 689–696. [Google Scholar] [CrossRef]
- Su, W.C.; Chen, Y.; Xi, J. A new approach to estimate ultrafine particle respiratory deposition. Inhal. Toxicol. Int. Forum Respir. Res. 2019, 31, 35–43. [Google Scholar] [CrossRef]
- Mayoral, M.C.; Izquierdo, M.T.; Andrés, J.M.; Rubio, B. Different approaches to proximate analysis by thermogravimetry analysis. Thermochim. Acta 2001, 370, 91–97. [Google Scholar] [CrossRef]
- Zhang, W.; Jiang, S.; Hardacre, C.; Goodrich, P. A combined raman spectroscopic and thermogravimetric analysis study on oxidation of coal with different ranks. J. Anal. Methods Chem. 2015, 2015, 306874. [Google Scholar] [CrossRef] [Green Version]
- Phillips, K.; Keles, C.; Scaggs, M.; Johann, V.; Rezaee, M.; Sarver, E.A. Comparison of Coal vs. Mineral Mass Fractions in Respirable Dust in Appalachian Coal Mines. In Proceedings of the 16th North American Mine Ventilation Symposium, Golden, CO, USA, 17–22 June 2017. [Google Scholar]
- National Institute for Occupational Safety and Health. Rock Dust Partnership Meeting: Attributes of Rock Dust to Prevent Coal Dust Explosions; Pittsburgh Mining Research Division: Pittsburgh, PA, USA, 2016. [Google Scholar]
- Sellaro, R.; Sarver, E. Characterization of respirable dust in an underground coal mine in central Appalachia. Trans. Soc. Min. Metall. Explor. 2014, 336, 457–466. [Google Scholar]
- Sarver, E.; Keles, C.; Lowers, H.; Zulfikar, R.; Zell-Baran, L.; Vorajee, N.; Sanyal, S.; Rose, C.S.; Petsonk, E.L.; Murray, J.; et al. Analysis of Respirable Dust from 24 Underground Coal Mines in Four Geographic Regions of the United States. Am. J. Respir. Crit. Care Med. 2020, 201, A2635. [Google Scholar]
- Phillips, K.; Keles, C.; Sarver, E.; Scaggs-Witte, M. Coal and mineral mass fractions in personal respirable dust samples collected by central Appalachian miners. Miner. Eng. 2018, 70, 16–30. [Google Scholar]
- Stein, F.; Corn, M. Shape factors of narrow size range samples of respirable coal mine dust. Powder Technol. 1975, 13, 133–141. [Google Scholar] [CrossRef]
- Kriegseis, W.; Scharmann, A. Determination of free quartz surfaces in coal mine dust. Ann. Occup. Hyg. 1985, 29, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.W. Statistical Analysis of the Size and Elemental Composition of Airborne Coal Mine Dust. Ph.D. Thesis, PB 90-161647. Pennsylvania State University, State College, PA, USA, 1986. [Google Scholar]
- Volkwein, J.C.; Vinson, R.P.; Page, S.J.; McWilliams, L.J.; Joy, G.J.; Mischler, S.E.; Tuchman, D.P. Laboratory and Field Performance of a Continuously Measuring Personal Respirable Dust Monitor; National Institute for Occupational Safety and Health, Pittsburgh Research Laboratory: Pittsburgh, PA, USA, 2006. [Google Scholar]
- Colinet, J.F.; Listak, J.M. Silica and Respirable Content in Rock Dust Sample; National Institute for Occupational Safety and Health Office of Mine Safety and Health, Office of Mine Safety and Health Research: Pittsburgh, PA, USA, 2012. Available online: https://www.cdc.gov/Niosh/mining/UserFiles/works/pdfs/aotsp.pdf (accessed on 20 September 2020).
- Rider, J.P.; Colinet, J.F. An Overview of Fundamental and Emerging Technologies to Monitor and Control. Respirable Dust in Underground Coal Mines in The United States; National Institute for Occupational Safety and Health, Pittsburgh Research Laboratory: Pittsburgh, PA, USA, 2015. [Google Scholar]
- Kittelson, D.B. Engines and nanoparticles: A review. J. Aerosol Sci. 1998, 29, 575–588. [Google Scholar] [CrossRef]
- Jacobsen, M. New data on the relationship between simple pneumoconiosis and exposure to coal mine dust. Chest 1980, 78, 408–410. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.F.; Alexander, W.P.; Hazledine, D.J.; Jacobsen, M.; Maclaren, W.M. Exposure to respirable coal mine dust and incidence of progressive massive fibrosis. Br. J. Ind. Med. 1987, 44, 661–672. [Google Scholar] [PubMed] [Green Version]
- McCunney, R.J.; Morfeld, P.; Payne, S. What component of coal causes coal workers’ pneumoconiosis? J. Occup. Environ. Med. 2009, 51, 462–471. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.A.; Petsonk, E.L.; Rose, C.; Young, B.; Regier, M.; Najmuddin, A.; Abraham, J.L.; Churg, A.; Green, F.H.Y. Lung Pathology in US Coal Workers with Rapidly Progressive Pneumoconiosis Implicates Silica and Silicates. Am. J. Respir. Crit. Care Med. 2016, 193, 673–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maclaren, W.M.; Hurley, J.F.; Collins, H.P.; Cowie, A.J. Factors associated with the development of progressive massive fibrosis in British coalminers: A case-control study. Br. J. Ind. Med. 1989, 46, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Antao, V.C.; Petsonk, E.L.; Sokolow, L.Z.; Wolfe, A.L.; Pinheiro, G.A.; Attfield, M.D. Rapidly progressive coal workers’ pneumoconiosis in the United States: Geographic clustering and other factors. Occup. Environ. Med. 2005, 62, 670–674. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, A.K.; Bhattacharya, S.K.; Sayed, H.N. Assessment of respirable dust and its freesilica contents in different Indian coalmines. Ind. Health 2005, 43, 277–284. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/15895842 (accessed on 20 May 2018).
- Voliotis, A.; Samara, C. Submicron particle number doses in the human respiratory tract: Implications for urban traffic and background environments. Environ. Sci. Pollut. Res. 2018, 25, 33724–33735. [Google Scholar] [CrossRef] [PubMed]
- Mine Safety and Health Administration. Federal Register, Rules and Regulations; Mine Safety and Health Administration: Arlington, VA, USA, 2014.

Figure 2.
Number of reported CWP in the United States underground coal mines from 1983–2018 (Data is extracted from Accident/Injury/Illness Files of MSHA, see https://arlweb.msha.gov/OpenGovernmentData/OGIMSHA.asp (accessed on 27 June 2021)).
Figure 2.
Number of reported CWP in the United States underground coal mines from 1983–2018 (Data is extracted from Accident/Injury/Illness Files of MSHA, see https://arlweb.msha.gov/OpenGovernmentData/OGIMSHA.asp (accessed on 27 June 2021)).

Figure 3.
Probability of deposition of particles in three regions of the head, tracheobronchial, alveolar, and total deposition in the respiratory tract based on particle size after [43].
Figure 3.
Probability of deposition of particles in three regions of the head, tracheobronchial, alveolar, and total deposition in the respiratory tract based on particle size after [43].


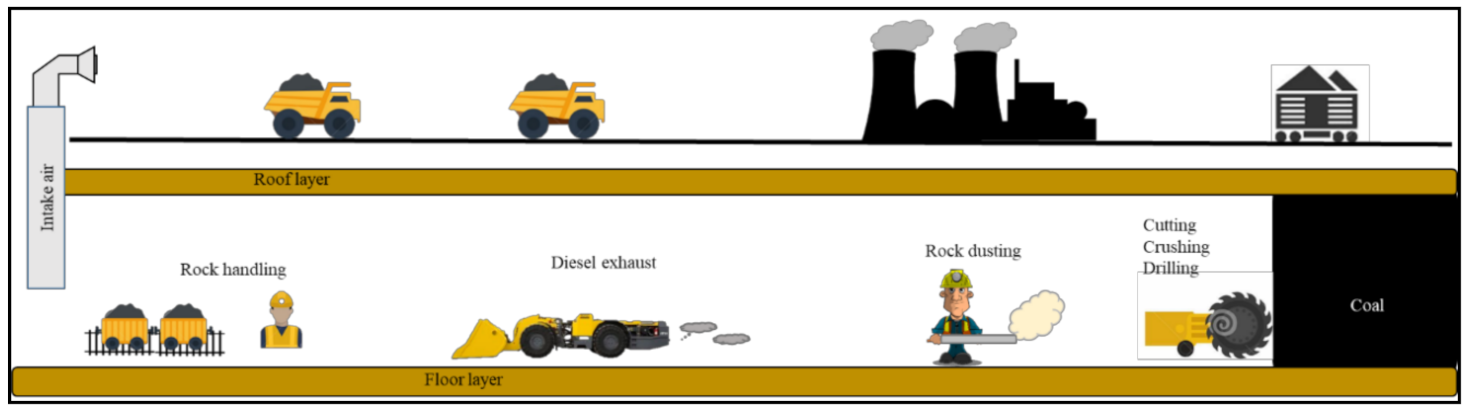{kind=link}
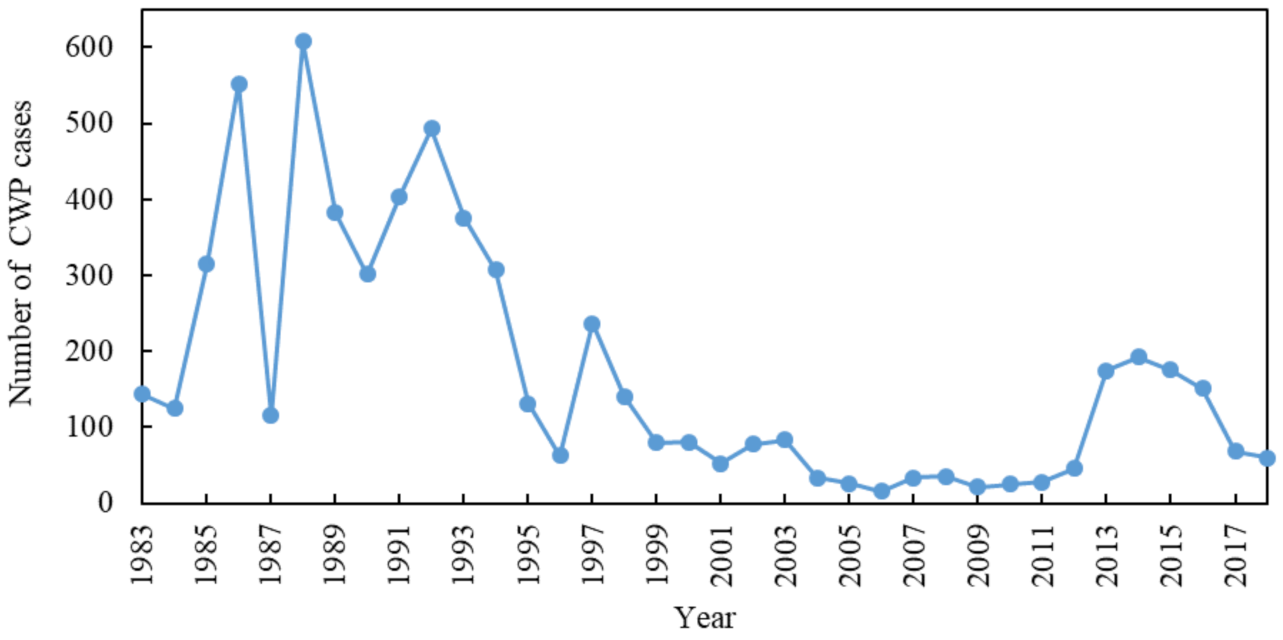{kind=link}
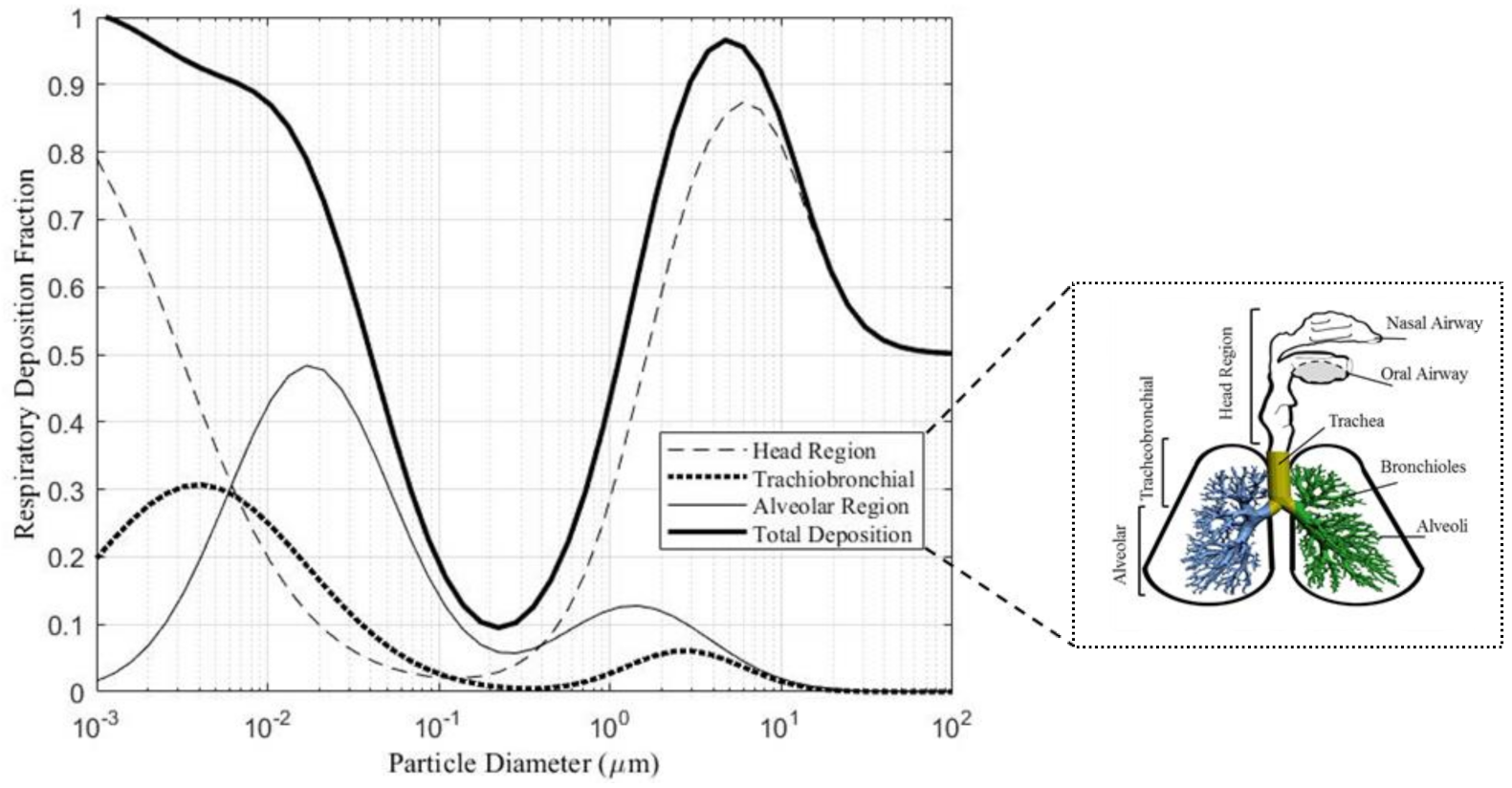{kind=link}
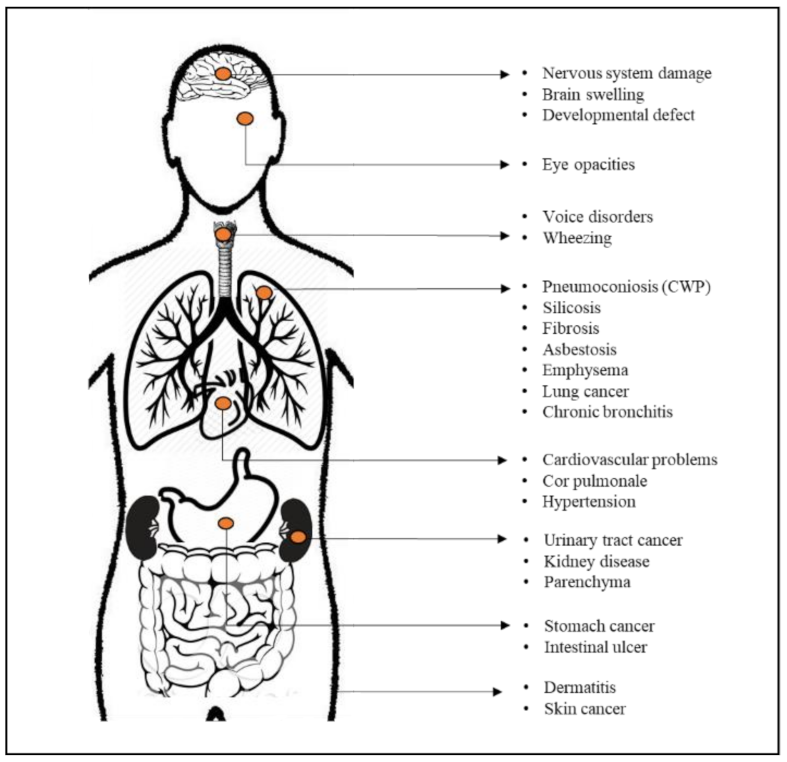{kind=link}
Table 3.
Development of permissible dust sampling devices for measuring respirable dust [59].
Table 3.
Development of permissible dust sampling devices for measuring respirable dust [59].
| Device Name | Country/ Association | Description of the Sampling Operation | Sampling Positioning |
|---|---|---|---|
| Midget Impinger (1937) | U.S. Bureau of Mines | A hand-wrapped pump pulled the air into the impinger. Inside the device, the air emerged from a small orifice at high velocity and impinged on the bottom of a liquid-filled container. Then, particulate matters above one micrometer in size were trapped in the liquid and then counted. | Area sampling |
| Gravimetric Sampler (1964) | United Kingdom (MRE) | This device first removed particles beyond the respirable sizes, and small particles under 7 µm in size were collected on an elutriator. The elutriator is required to be held in a steady horizontal position to work correctly. | Used as fixed-location in the return airway |
| Personal Sampler (1969) | U.S. Atomic Energy Commission | Particles over 7 µm removed by 10-mm nylon cyclone. The cyclone is attached to a filter that collects respirable dust up to a few ounces. | Pinned to lapel and a pump mounted on belt |
| CMDPSU (1970) | U.S. Department of Labor, MSHA | The air is drawn through a filter cassette that collects RCMD particles. Then at the end of each shift, filter cassettes are analyzed to measure the weight of dust. Polyvinyl chloride (PVC) filter with pore sizes less than 5 µm is usually used in this method. The total measurement of RCMD weight is averaged as an average concentration of RCMD for the shift. | Personal sampling instrument |
| Tyndallometer and SIMSLIN * (1981) | U.S. Department of Labor, MSHA | The principles employed in Tyndallometer included light scattering, real-time aerosol monitor. The principles employed in SIMSLIN is beta-ray attenuation and the change in the resonant frequency of a piezoelectric crystal. | Adjustments to personal dust sampling tool |
| CPDM (1991) | NIOSH | NIOSH began conducting research and development to produce a new type of personal dust monitoring unit using a Tapered Element Oscillating Microbalance (TEOM-based) personal dust monitor to provide readings of dust levels in a near-continuous manner by the PDM3700 instrument. | Personal Dust Monitor |
| PDM3700 (2016) | Thermo-Fisher Scientific | This device is designed explicitly for MSHA’s rule for underground coal mine applications. PDM provides three primary current mass concentration, primary cumulative mass concentration, and percent of the limit. | Personal Dust Monitor |
* Safety in Mines Scattered Light Instrument.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shekarian, Y.; Rahimi, E.; Rezaee, M.; Su, W.-C.; Roghanchi, P. Respirable Coal Mine Dust: A Review of Respiratory Deposition, Regulations, and Characterization. Minerals 2021, 11, 696. https://0-doi-org.brum.beds.ac.uk/10.3390/min11070696
AMA Style
Shekarian Y, Rahimi E, Rezaee M, Su W-C, Roghanchi P. Respirable Coal Mine Dust: A Review of Respiratory Deposition, Regulations, and Characterization. Minerals. 2021; 11(7):696. https://0-doi-org.brum.beds.ac.uk/10.3390/min11070696
Chicago/Turabian StyleShekarian, Younes, Elham Rahimi, Mohammad Rezaee, Wei-Chung Su, and Pedram Roghanchi. 2021. "Respirable Coal Mine Dust: A Review of Respiratory Deposition, Regulations, and Characterization" Minerals 11, no. 7: 696. https://0-doi-org.brum.beds.ac.uk/10.3390/min11070696
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.