
Strain Echocardiography Is a Promising Tool for the Prognostic Assessment of Sarcoidosis

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- TTE, including STE parameters, performed at the Division of Cardiology of Siena University Hospital;
- A medical examination and pulmonary function tests (PFTs), including the diffusing capacity of the lung for carbon monoxide (DLCO) assessment, within three months of TTE;
- No acute event or treatment escalation must have occurred between the execution of the TTE and PFTs.
2.2. Study Design
2.3. Basic and Advanced Echocardiography
2.4. Speckle Tracking Echocardiography
2.5. Lung Function Tests
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Outcome Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| B | HR | CI (95%) | p-Value | |
|---|---|---|---|---|
| Baseline Features | ||||
| Age | 0.063 | 1.065 | 1.023–1.108 | 0.002 |
| Sex | −0.370 | 0.691 | 0.269–1.775 | 0.442 |
| Hypertension | −0.426 | 0.653 | 0.273–1.562 | 0.338 |
| Former smoke habit | −0.322 | 0.725 | 0.245–2.144 | 0.561 |
| Current smoke habit | 3.079 | 21.731 | 0.003–156.170 | 0.497 |
| Diabetes mellitus | −0.234 | 0.791 | 0.185–3.391 | 0.752 |
| ACE | −0.023 | 0.977 | 0.956–0.998 | 0.032 |
| Lysozyme | 0.122 | 1.130 | 0.903–1.413 | 0.286 |
| Chitotriosidase | −0.001 | 0.999 | 0.996–1.002 | 0.415 |
| Urinary calcium | −0.001 | 0.999 | 0.994–1.005 | 0.801 |
| Löfgren syndrome | 0.528 | 1.696 | 0.220–13.058 | 0.612 |
| Extrapulmonary localizations | −0.374 | 0.688 | 0.297–1.593 | 0.383 |
| X-ray stage of disease | −0.095 | 0.909 | 0.679–1.218 | 0.522 |
| Therapy | 0.530 | 1.699 | 0.725–3.984 | 0.223 |
| Spirometry data | ||||
| FVC% predicted value | −0.001 | 0.999 | 0.978–1.021 | 0.922 |
| FVC (mL) | 0.001 | 1.001 | 0.999–1.001 | 0.479 |
| FEV1 % predicted value | −0.007 | 0.993 | 0.972–1.014 | 0.487 |
| FEV1 (mL) | 0.001 | 1.001 | 0.999–1.001 | 0.427 |
| FEV1/FVC | −0.032 | 0.969 | 0.924–1.015 | 0.184 |
| DLCO % predicted value | 0.008 | 1.008 | 0.983–1.035 | 0.526 |
| Echocardiographic data | ||||
| IVS | −0.042 | 0.959 | 0.822–1.119 | 0.596 |
| LV-EDD | 0.059 | 1.060 | 0.982–1.145 | 0.135 |
| EDV | −0.003 | 0.997 | 0.984–1.010 | 0.620 |
| LVEF | −0.021 | 0.979 | 0.924–1.037 | 0.474 |
| Indexed LA volume | 0.023 | 1.023 | 0.985–1.063 | 0.233 |
| E/E′ | −1.698 | 0.183 | 0.034–0.990 | 0.149 |
| Deceleration time | 0.003 | 1.003 | 0.996–1.010 | 0.359 |
| Mitral regurgitation | −0.596 | 0.551 | 0.206–1.472 | 0.235 |
| Right mid-ventricular EDD | −0.016 | 0.984 | 0.891–1.087 | 0.756 |
| RA area | 0.110 | 1.116 | 0.994–1.252 | 0.063 |
| TAPSE | 0.017 | 1.017 | 0.894–1.156 | 0.800 |
| Tricuspid regurgitation | −0.253 | 0.777 | 0.426–1.417 | 0.410 |
| sPAP | −0.005 | 0.995 | 0.931–1.063 | 0.885 |
| Strain echocardiographic data | ||||
| Global LA PALS | −0.050 | 0.952 | 0.907–0.998 | 0.063 |
| Global LA PACS | −0.026 | 0.974 | 0.894–1.061 | 0.551 |
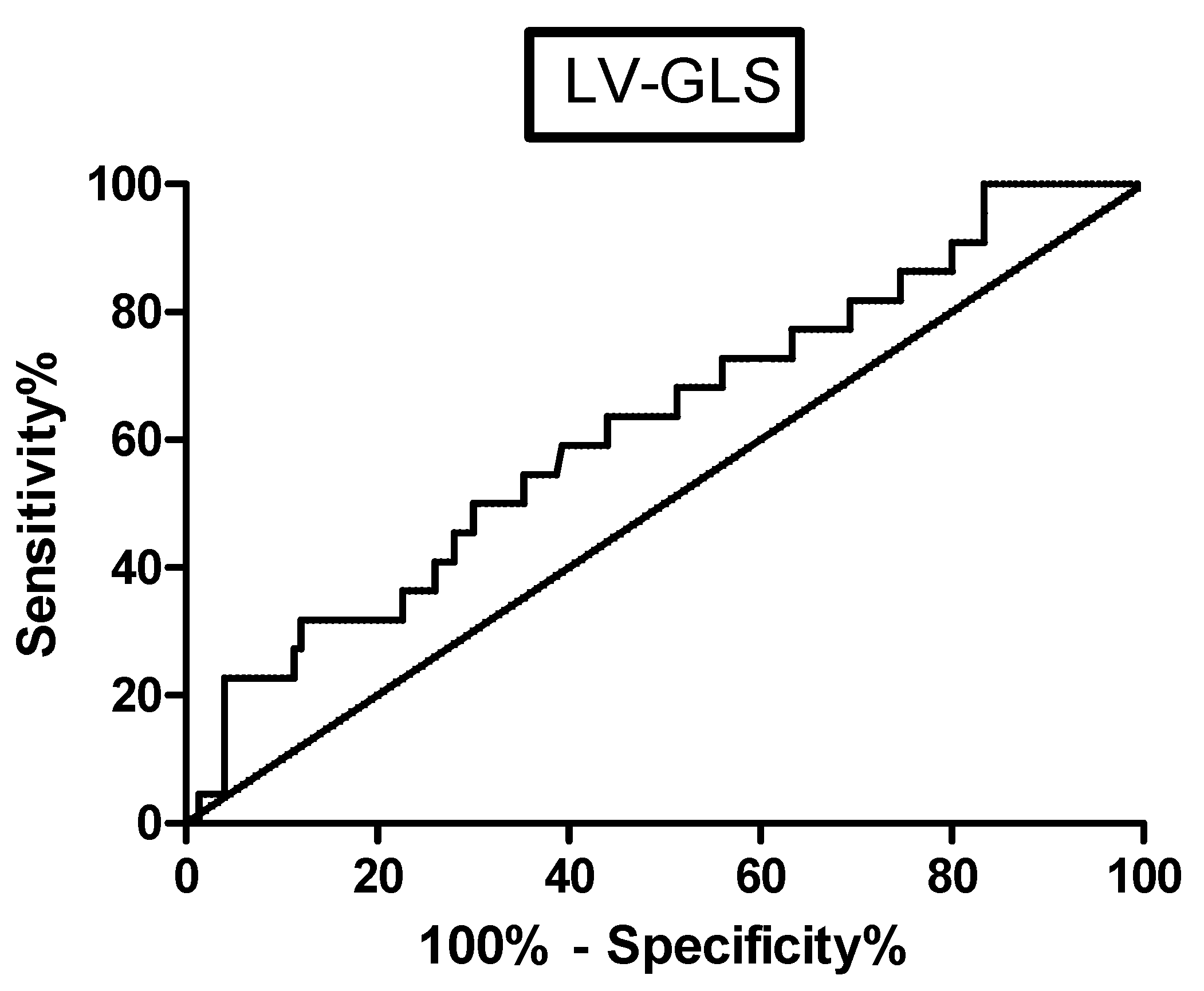
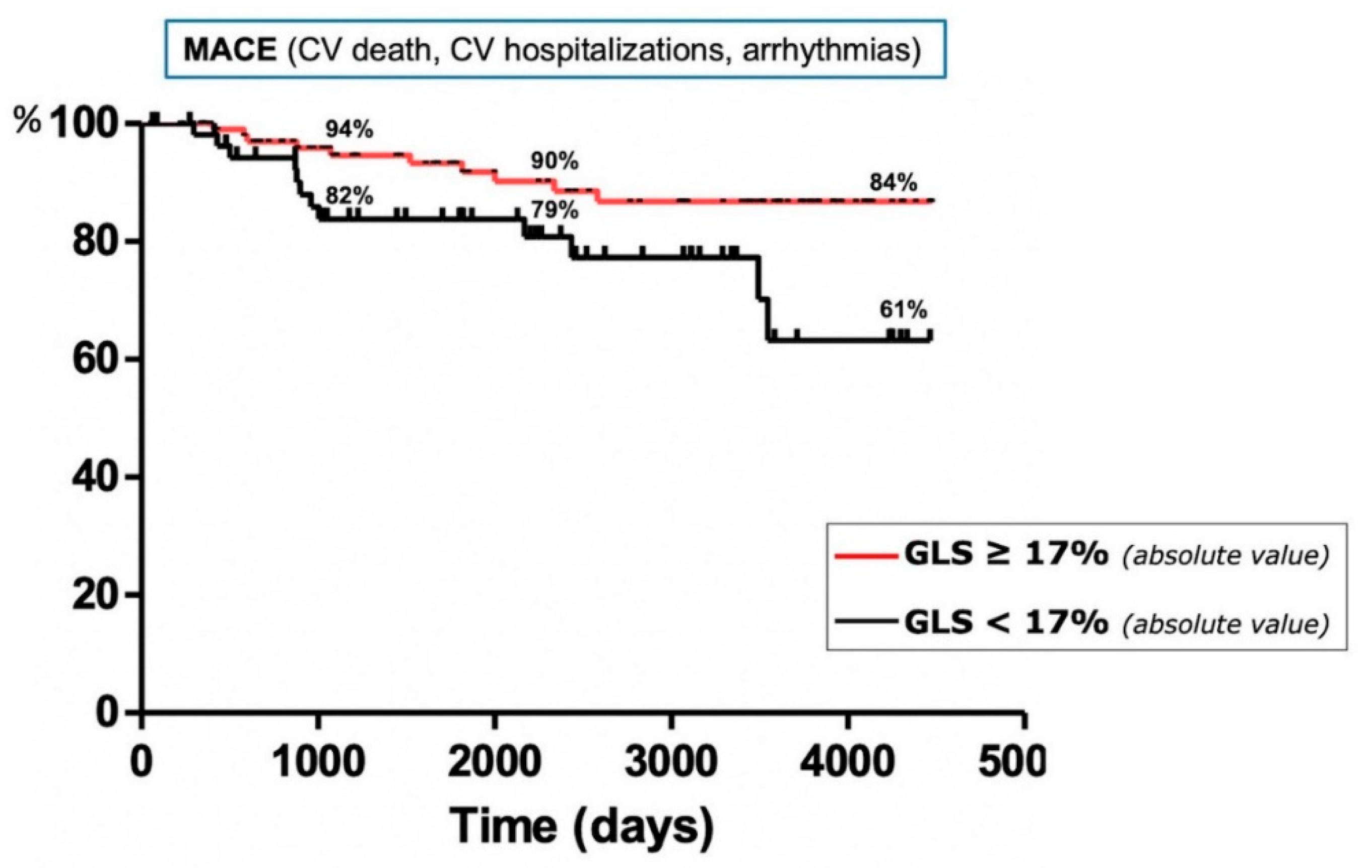
| LV-GLS | −0.141 | 0.869 | 0.774–0.975 | 0.017 |
| TTP LV-GLS | 0.005 | 1.005 | 1.000–1.010 | 0.068 |
| RV-GLS | −0.036 | 0.965 | 0.852–1.093 | 0.574 |
| TTP RV-GLS | −0.002 | 0.998 | 0.991–1.005 | 0.555 |
| Free wall RVLS | −0.012 | 0.988 | 0.904–1.079 | 0.782 |
| B | HR | CI (95%) | p-Value | |
|---|---|---|---|---|
| Baseline Features | ||||
| Age | 0.001 | 1.001 | 1.000–1.003 | 0.664 |
| Female sex | −0.053 | 0.948 | 0.341–2.634 | 0.918 |
| ACE | −0.014 | 0.986 | 0.966–1.007 | 0.195 |
| X-ray stage of disease | −0.094 | 0.910 | 0.658–1.258 | 0.568 |
| Global LA PALS | 0.080 | 1.083 | 0.940–1.248 | 0.270 |
| LV-GLS | −0.156 | 0.855 | 0.756–0.968 | 0.013 |
| B | HR | CI (95%) | p-Value | |
|---|---|---|---|---|
| Baseline Features | ||||
| Age | 0.001 | 1.001 | 1.001–1.006 | 0.955 |
| Sex | −0.073 | 0.929 | 0.464–1.863 | 0.836 |
| Hypertension | 0.264 | 1.302 | 0.592–2.862 | 0.511 |
| Former smoke habit | 0.068 | 1.071 | 0.488–2.352 | 0.865 |
| Current smoke habit | 3.079 | 21.728 | 0.023–209.123 | 0.380 |
| Diabetes mellitus | −0.941 | 0.390 | 0.162–0.941 | 0.036 |
| ACE | 0.011 | 1.011 | 0.996–1.027 | 0.151 |
| Lysozyme | 0.148 | 1.160 | 0.991–1.358 | 0.064 |
| Chitotriosidase | −0.001 | 0.999 | 0.998–1.001 | 0.473 |
| Urinary calcium | 0.001 | 1.001 | 0.996–1.004 | 0.894 |
| Löfgren syndrome | 0.324 | 1.383 | 0.328–5.833 | 0.659 |
| Extrapulmonary localizations | 0.057 | 1.058 | 0.524–2.137 | 0.875 |
| X-ray stage of disease | 0.085 | 1.089 | 0.869–1.365 | 0.459 |
| Therapy | −0.135 | 0.873 | 0.436–1.748 | 0.702 |
| Spirometry data | ||||
| Predicted FVC | 0.001 | 1.001 | 0.983–1.018 | 0.999 |
| FVC (mL) | 0.001 | 1.001 | 1.002–1.004 | 0.623 |
| FEV1 % predicted value | −0.004 | 0.996 | 0.979–1.014 | 0.680 |
| FEV1 (mL) | 0.002 | 1.002 | 1.001–1.005 | 0.589 |
| FEV1/FVC | −0.006 | 0.994 | 0.954–1.037 | 0.786 |
| DLCO % predicted value | −0.002 | 0.998 | 0.977–1.019 | 0.829 |
| Echocardiographic data | ||||
| IVS | −0.022 | 0.978 | 0.885–1.081 | 0.669 |
| LV-EDD | −0.031 | 0.970 | 0.940–1.000 | 0.051 |
| EDV | −0.014 | 0.986 | 0.974–0.998 | 0.220 |
| LVEF | −0.017 | 0.983 | 0.939–1.028 | 0.451 |
| Indexed LA volume | 0.005 | 1.005 | 0.973–1.038 | 0.774 |
| E/E′ | −0.081 | 0.922 | 0.376–2.261 | 0.859 |
| Deceleration time | 0.006 | 1.006 | 1.001–1.012 | 0.200 |
| Mitral regurgitation | −0.676 | 0.509 | 0.234–1.105 | 0.088 |
| Right mid-ventricular EDD | 0.010 | 1.010 | 0.949–1.075 | 0.765 |
| RA area | 0.031 | 1.031 | 0.933–1.140 | 0.548 |
| TAPSE | −0.052 | 0.950 | 0.862–1.045 | 0.292 |
| Tricuspid regurgitation | −0.327 | 0.721 | 0.442–1.175 | 0.190 |
| sPAP | 0.013 | 1.013 | 0.974–1.053 | 0.525 |
| Strain echocardiographic data | ||||
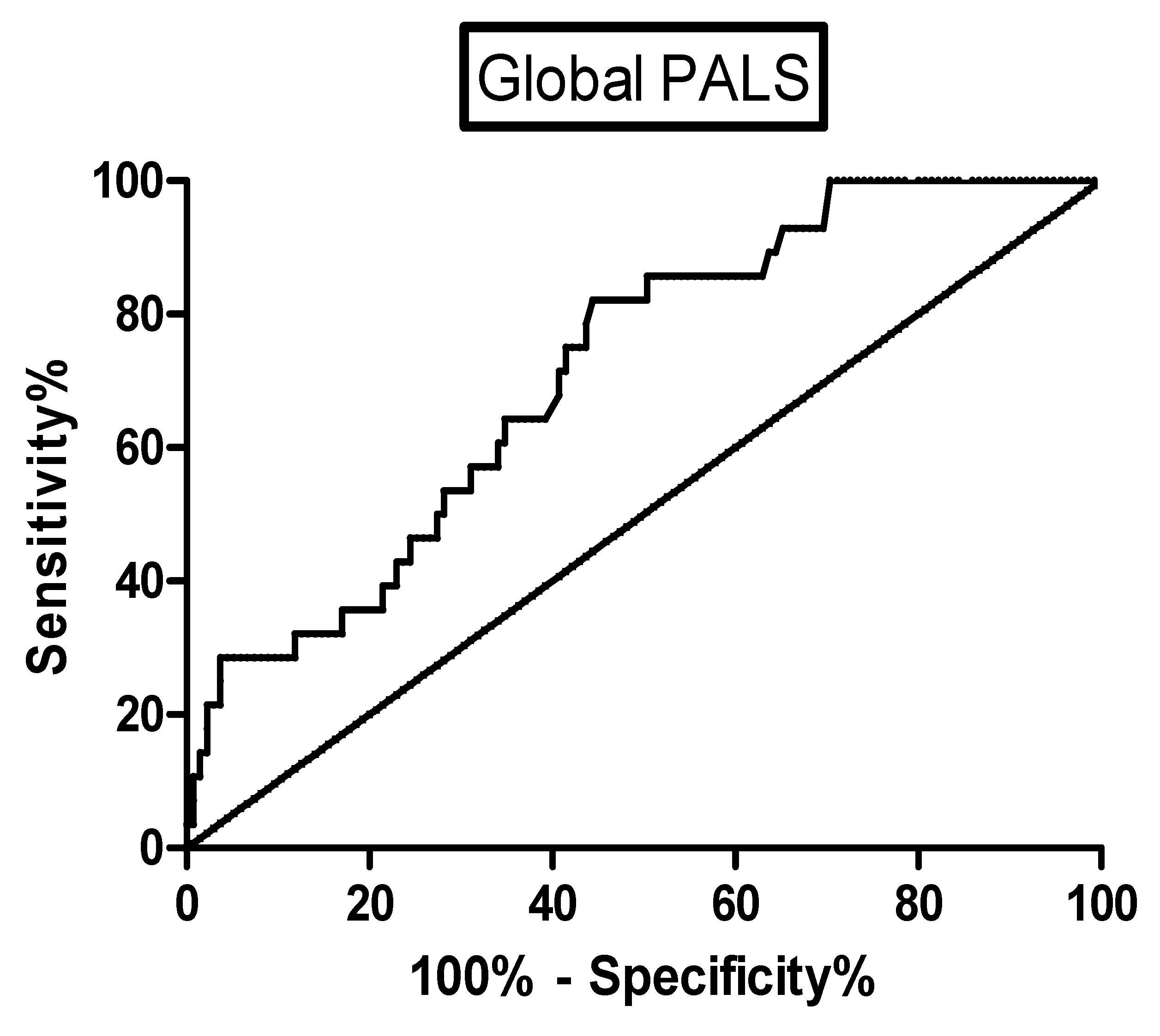
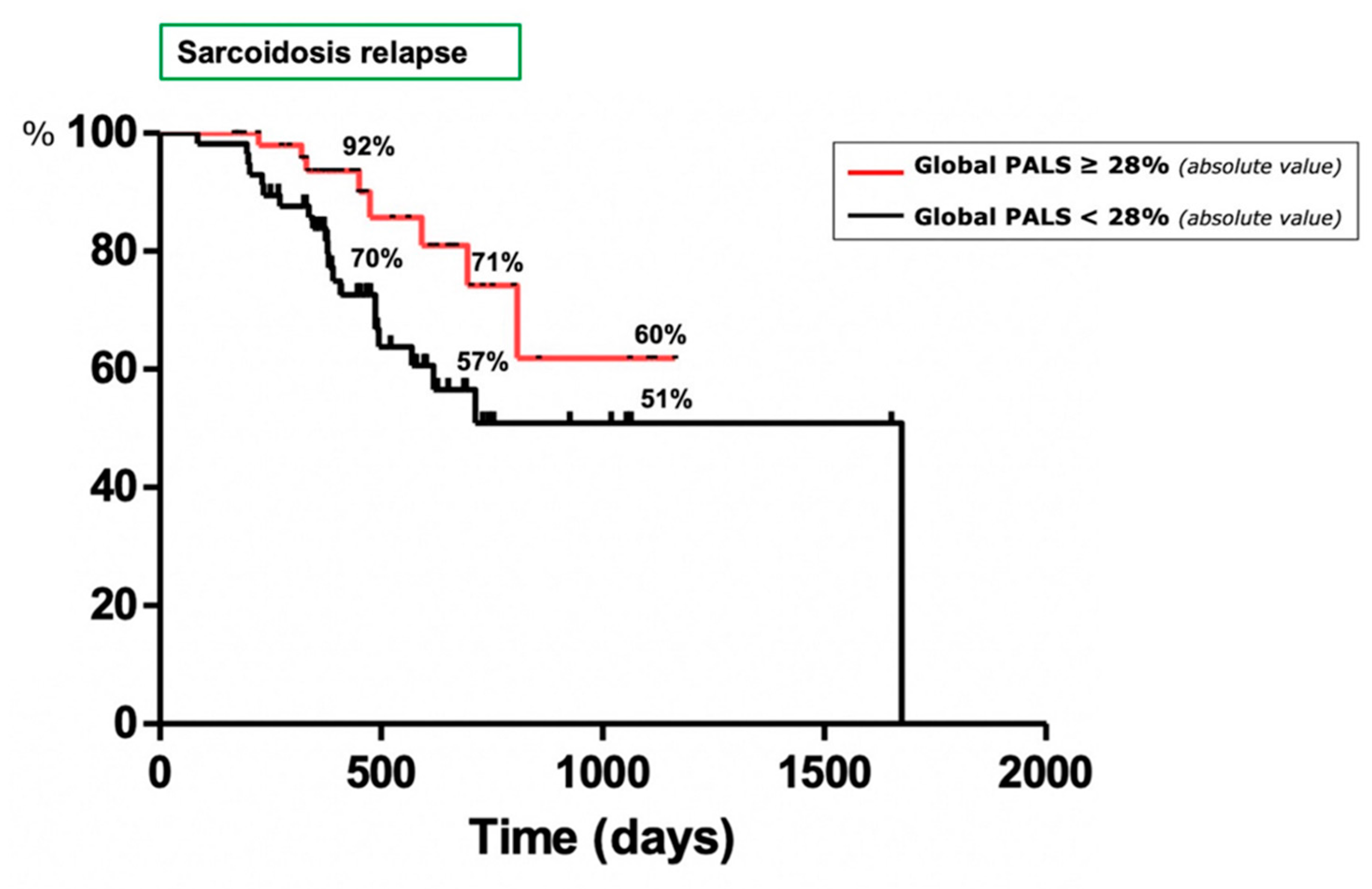
| Global LA PALS | −0.072 | 0.931 | 0.897–0.966 | <0.001 |
| Global LA PACS | −0.098 | 0.907 | 0.850–0.967 | 0.003 |
| LV-GLS | −0.053 | 0.949 | 0.861–1.045 | 0.286 |
| TTP LV-GLS | −0.004 | 0.996 | 0.992–1.001 | 0.093 |
| RV-GLS | −0.051 | 0.951 | 0.866–1.043 | 0.284 |
| TTP RV-GLS | −0.002 | 0.998 | 0.992–1.003 | 0.458 |
| Free wall RVLS | −0.020 | 0.980 | 0.916–1.048 | 0.551 |
| B | HR | CI (95%) | p-Value | |
|---|---|---|---|---|
| Diabetes Mellitus | −0.790 | 0.454 | 0.152–1.357 | 0.157 |
| Age | 0.005 | 1.002 | 1.000–1.008 | 0.985 |
| Global LA PALS | 2.544 | 12.736 | 1.850–87.664 | 0.005 |
| Global LA PACS | 0.149 | 1.161 | 0.880–1.531 | 0.291 |
References
- Spagnolo, P.; Rossi, G.; Trisolini, R.; Sverzellati, N.; Baughman, R.P.; Wells, A.U. Pulmonary sarcoidosis. Lancet Respir. Med. 2018, 6, 389–402. [Google Scholar] [CrossRef]
- Bargagli, E.; Prasse, A. Sarcoidosis: A review for the internist. Intern. Emerg. Med. 2018, 13, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.U. Sarcoidosis: A benign disease or a culture of neglect? Respir. Med. 2018, 144, S1–S2. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Wells, A. Advanced sarcoidosis. Curr. Opin. Pulm. Med. 2019, 25, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Cameli, P.; Caffarelli, C.; Refini, R.M.; Bergantini, L.; D’Alessandro, M.; Armati, M.; Pitinca, M.D.T.; Sestini, P.; Gonnelli, S.; Bargagli, E. Hypercalciuria in sarcoidosis: A specific biomarker with clinical utility. Front. Med. 2020, 7, 568020. [Google Scholar] [CrossRef]
- Bergantini, L.; Bianchi, F.; Cameli, P.; Mazzei, M.A.; Fui, A.; Sestini, P.; Rottoli, P.; Bargagli, E. Prognostic biomarkers of sarcoidosis: A comparative study of serum chitotriosidase, ACE, lysozyme, and KL-6. Dis. Markers 2019, 2019, 8565423. [Google Scholar] [CrossRef] [PubMed]
- Cameli, P.; Gonnelli, S.; Bargagli, E.; d’Alessandro, M.; Bergantini, L.; Favetta, V.; Pitinca, M.D.T.; Lisi, E.; Refini, R.M.; Pieroni, M.; et al. The role of urinary calcium and chitotri-osidase in a cohort of chronic sarcoidosis patients. Respir. Int. Rev. Thorac. Dis. 2020, 99, 207–212. [Google Scholar]
- Eurelings, L.E.M.; Miedema, J.R.; Dalm, V.A.S.H.; van Daele, P.L.A.; van Hagen, P.M.; van Laar, J.A.M.; Dik, W.A. Sensitivity and specificity of serum soluble interleukin-2 receptor for diagnosing sarcoidosis in a population of patients suspected of sarcoidosis. PLoS ONE 2019, 14, e0223897. [Google Scholar] [CrossRef] [Green Version]
- Bennett, D.; Cameli, P.; Lanzarone, N.; Carobene, L.; Bianchi, N.; Fui, A.; Rizzi, L.; Bergantini, L.; Cillis, G.; d’Alessandro, M.; et al. Chitotriosidase: A biomarker of activity and severity in patients with sarcoidosis. Respir. Res. 2020, 21, 6. [Google Scholar] [CrossRef] [Green Version]
- Kiko, T.; Yoshihisa, A.; Kanno, Y.; Yokokawa, T.; Abe, S.; Miyata-Tatsumi, M.; Misaka, T.; Oikawa, M.; Kobayashi, A.; Ishida, T.; et al. A multiple biomarker approach in patients with cardiac sarcoidosis. Int. Hearth J. 2018, 59, 996–1001. [Google Scholar] [CrossRef] [Green Version]
- Schimmelpennink, M.C.; Quanjel, M.; Vorselaars, A.; Wiertz, I.; Veltkamp, M.; Van Moorsel, C.H.M.; Grutters, J.C. Value of serum soluble inter-leukin-2 receptor as a diagnostic and predictive biomarker in sarcoidosis. Exp. Rev. Respir. Med. 2020, 14, 749–756. [Google Scholar] [CrossRef]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and detection of sarcoidosis. An official American Thoracic Society clinical practice guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Barssoum, K.; Altibi, A.M.; Rai, D.; Kumar, A.; Kharsa, A.; Chowdhury, M.; Thakkar, S.; Shahid, S.; Abdelazeem, M.; Abuzaid, A.S.; et al. Speckle tracking echocardiography can predict subclinical myocardial involvement in patients with sarcoidosis: A meta-analysis. Echocardiography 2020, 37, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Joyce, E.; Ninaber, M.K.; Katsanos, S.; Debonnaire, P.; Kamperidis, V.; Bax, J.J.; Taube, C.; Delgado, V.; Marsan, N.A. Subclinical left ventricular dysfunction by echocardiographic speckle-tracking strain analysis relates to outcome in sarcoidosis. Eur. J. Hearth Fail. 2015, 17, 51–62. [Google Scholar] [CrossRef]
- Schouver, E.D.; Moceri, P.; Doyen, D.; Tieulie, N.; Queyrel, V.; Baudouy, D.; Cerboni, P.; Gibelin, P.; Leroy, S.; Fuzibet, J.G.; et al. Early detection of cardiac involvement in sar-coidosis with 2-dimensional speckle-tracking echocardiography. Int. J. Cardiol. 2017, 227, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, C.; Bruno, G.; Arciniegas Calle, M.C.; Acharya, G.A.; Fussner, L.M.; Ungprasert, P.; Cooper, L.T.; Blauwet, L.A.; Ryu, J.H.; Pellikka, P.A.; et al. Diagnostic and predictive value of speckle tracking echocardiography in cardiac sarcoidosis. BMC Cardiovasc. Disord. 2020, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; Du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. ATS/ERS/WASOG statement on sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 1999, 16, 149–173. [Google Scholar]
- Baughman, R.P.; Nagai, S.; Balter, M.; Costabel, U.; Drent, M.; Du Bois, M.; Grutters, J.C.; Judson, M.A.; Lambiri, I.; Lower, E.E.; et al. Defining the clinical outcome status (COS) in sar-coidosis: Results of WASOG task force. Sarcoidosis Vasc. Diffus. Lung Dis. 2011, 28, 56–64. [Google Scholar]
- Schupp, J.C.; Freitag-Wolf, S.; Bargagli, E.; Mihailović-Vučinić, V.; Rottoli, P.; Grubanovic, A.; Müller, A.; Jochens, A.; Tittmann, L.; Schnerch, J.; et al. Phenotypes of organ involvement in sarcoidosis. Eur. Respir. J. 2018, 51, 1700991. [Google Scholar] [CrossRef] [Green Version]
- Scadding, J.G. Prognosis of intrathoracic sarcoidosis in England. A review of 136 cases after five years’ observation. Br. Med. J. 1961, 2, 1165–1172. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quanti-fication by echocardiography in adults: An update from the American Society of Echocardiography and the European Asso-ciation of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2015, 28, 233–271. [Google Scholar]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for noninvasive evaluation of native valvular regurgitation: A report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Cameli, M.; Miglioranza, M.H.; Magne, J.; Mandoli, G.E.; Benfari, G.; Ancona, R.; Sibilio, G.; Reskovic Luksic, V.; Griseli, L.; Van De Heyning, C.M.; et al. Multicentric atrial strain comparison between two different modalities: MASCOT HIT study. Diagnostics 2020, 10, 946. [Google Scholar] [CrossRef]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.M.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameli, M.; Mandoli, G.E.; Lisi, E.; Ibrahim, A.; Incampo, E.; Buccoliero, G.; Rizzo, C.; DeVito, F.; Ciccone, M.M.; Mondillo, S. Left atrial, ventricular and atrio-ventricular strain in patients with subclinical heart dysfunction. Int. J. Cardiovasc. Imaging 2018, 35, 249–258. [Google Scholar] [CrossRef]
- Mandoli, G.E.; Pastore, M.C.; Benfari, G.; Bisleri, G.; Maccherini, M.; Lisi, G.; Cameli, P.; Lisi, M.; Dokollari, A.; Carrucola, C.; et al. Left atrial strain as a pre-operative prognostic marker for patients with severe mitral regurgitation. Int. J. Cardiol. 2021, 324, 139–145. [Google Scholar] [CrossRef]
- Yafasova, A.; Fosbøl, E.L.; Schou, M.; Gustafsson, F.; Rossing, K.; Bundgaard, H.; Lauridsen, M.D.; Kristensen, S.L.; Torp-Pedersen, C.; Gislason, G.H.; et al. Long-term adverse cardiac outcomes in patients with sarcoidosis. J. Am. Coll. Cardiol. 2020, 76, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Okada, D.R.; Smith, J.; Derakhshan, A.; Gowani, Z.; Misra, S.; Berger, R.D.; Calkins, H.; Tandri, H.; Chrispin, J. Ventricular arrhythmias in cardiac sarcoidosis. Circulation 2018, 138, 1253–1264. [Google Scholar] [CrossRef]
- Burstow, D.J.; Tajik, A.J.; Bailey, K.R.; DeRemee, R.A.; Taliercio, C.P. Two-dimensional echocardiographic findings in systemic sarcoidosis. Am. J. Cardiol. 1989, 63, 478–482. [Google Scholar] [CrossRef]
- Mehta, D.; Lubitz, S.A.; Frankel, Z.; Wisnivesky, J.P.; Einstein, A.J.; Goldman, M.; Machac, J.; Teirstein, A. Cardiac involvement in patients with sar-coidosis: Diagnostic and prognostic value of outpatient testing. Chest 2008, 133, 1426–1435. [Google Scholar] [CrossRef]
- Focardi, M.; Picchi, A.; Nikiforakis, N.; Bargagli, E.; Fossi, A.; Maggiorelli, C.; Mondillo, S.; Rottoli, P. Assessment of cardiac involvement in sarcoidosis by echocardiography. Rheumatol. Int. 2009, 29, 1051–1055. [Google Scholar] [CrossRef]
- Felekos, I.; Aggeli, C.; Gialafos, E.; Kouranos, V.; Rapti, A.; Sfikakis, P.; Koulouris, N.; Tousoulis, D. Global longitudinal strain and long-term outcomes in asymptomatic extracardiac sarcoid patients with no apparent cardiovascular disease. Echocardiography 2018, 35, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Judd, R.M.; Kim, R.J.; Kim, H.W.; Klem, I.; Heitner, J.F.; Shah, D.J.; Jue, J.; White, B.E.; Indorkar, R.; et al. Feature-tracking global longitudinal strain predicts death in a multicenter population of patients with ischemic and nonischemic dilated cardiomyopathy incremental to ejection fraction and late gadolinium enhancement. JACC Cardiovasc. Imaging 2018, 11, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Goedemans, L.; Abou, R.; Hoogslag, G.E.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Left ventricular global longitudinal strain and long-term prognosis in patients with chronic obstructive pulmonary disease after acute myocardial infarction. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Stanton, T.; Leano, R.; Marwick, T.H. Prediction of all-cause mortality from global longitudinal speckle strain: Comparison with ejection fraction and wall motion scoring. Circ. Cardiovasc. Imaging 2009, 2, 356–364. [Google Scholar] [CrossRef] [Green Version]
- Cameli, M.; Righini, F.M.; Lisi, M.; Bennati, E.; Navarri, R.; Lunghetti, S.; Padeletti, M.; Cameli, P.; Tsioulpas, C.; Bernazzali, S.; et al. Comparison of right versus left ventricular strain analysis as a predictor of outcome in patients with systolic heart failure referred for heart transplantation. Am. J. Cardiol. 2013, 112, 1778–1784. [Google Scholar] [CrossRef]
- Cameli, M.; Mondillo, S.; Righini, F.M.; Lisi, M.; Dokollari, A.; Lindqvist, P.; Maccherini, M.; Henein, M. Left ventricular deformation and myocardial Fi-brosis in patients with advanced heart failure requiring transplantation. J. Card. Fail. 2016, 22, 901–907. [Google Scholar] [CrossRef]
- Mondillo, S.; Cameli, M.; Caputo, M.L.; Lisi, M.; Palmerini, E.; Padeletti, M.; Ballo, P. Early detection of left atrial strain abnormalities by speckle-tracking in hypertensive and diabetic patients with normal left atrial size. J. Am. Soc. Echocardiogr. 2011, 24, 898–908. [Google Scholar] [CrossRef]
- Yuda, S. Current clinical applications of speckle tracking echocardiography for assessment of left atrial function. J. Echocardiogr. 2021, 19, 129–140. [Google Scholar] [CrossRef]
- Kosmala, W.; Derzhko, R.; Przewlocka-Kosmala, M.; Orda, A.; Mazurek, W. Plasma levels of TNF-α, IL-6, and IL-10 and their relationship with left ventricular diastolic function in patients with stable angina pectoris and preserved left ventricular systolic performance. Coron. Artery Dis. 2008, 19, 375–382. [Google Scholar] [CrossRef] [PubMed]
- El Missiri, A.M.; Alzurfi, A.S.; Keddeas, V.W. The relationship between tumor necrosis factor alpha and left ventricular diastolic function. J. Cardiovasc. Echogr. 2020, 30, 62–67. [Google Scholar] [CrossRef] [PubMed]




| Parameters | Study Population | No MACE | MACE | Deaths |
|---|---|---|---|---|
| N° | 172 | 149 | 23 | 8 |
| Age (years) | 57.4 ± 12.6 | 57.5 ± 15.2 | 65.1 ± 11.1 | 72.3 ± 5.6 |
| Female sex (%) | 111 (64.5) | 95 (63.7) | 16 (69.5) | 3 (37.5) |
| Height (cm) | 166 ± 10 | 165.8 ± 10.4 | 164.9 ± 6.1 | 164.7 ± 7.5 |
| Weight (kg) | 74 ± 16 | 74.3 ± 16.4 | 70.4 ± 12 | 76 ± 13.9 |
| Body surface area (BSA) (m²) | 1.8 ± 0.3 | 1.7 ± 0.3 | 1.7 ± 0.1 | 1.8 ± 0.2 |
| Smokers n (%) | 47 (27.3) | 42 (28.1) | 5 (21.7) | 3 (37.5) |
| - Current | 7 (4) | 7 (4.6) | 0 (0) | 0 (0) |
| - Former | 40 (23.2) | 35 (23.4) | 5 (21.7) | 3 (37.5) |
| Patients with ongoing therapy | 86 (50) | 76 (51) | 10 (43.4) | 4 (50) |
| Time from diagnosis (mo) | 45.6 ± 33.4 | 43.2 ± 28.6 | 55.4.7 ± 30.5 | 74.2 ± 85.5 |
| Clinical features | ||||
| Hypertension (%) | 42 (24.4) | 34 (22.8) | 8 (34.7) | 2 (25) |
| Diabetes (%) | 13 (7.5) | 10 (6.7) | 3 (13) | 2 (25) |
| Ischemic heart disease (%) | 25 (14.5) | 17 (11.4) | 8 (34.7) | 2 (25) |
| Osteopenia/osteoporosis (%) | 57 (33.1) | 53 (35.5) | 4 (17.4) | 3 (37.5) |
| Psychiatric disorders (%) | 11 (6.3) | 9 (6) | 2 (8.6) | 0 (0) |
| GERD (%) | 35 (20.3) | 28 (18.8) | 7 (30.4) | 2 (25) |
| Other (%) | 27 (15.6) | 20 (13.4) | 7 (30.4) | 4 (50) |
| Clinical phenotypes of sarcoidosis | ||||
| Löfgren syndrome (%) | 13 (7.5) | 12 (8) | 1 (4.3) | 0 (0) |
| Extrapulmonary disease (%) | 56 (32.5) | 45 (30.2) | 11 (47.8) | 3 (37.5) |
| GenPhenResA classification | ||||
| - Abdominal (%) | 10 (5.8) | 10 (6.7) | 0 (0) | 0 (0) |
| - OCCC (%) | 8 (4.6) | 6 (4) | 2 (8.6) | 1 (12.5) |
| - Musculoskeletal cutaneous (%) | 27 (15.6) | 21 (14.1) | 6 (26.1) | 1 (12.5) |
| - Isolated pulmonary (%) | 116 (67.4) | 102 (68.4) | 14 (60.8) | 6 (75) |
| - Extrapulmonary (%) | 11 (6.3) | 10 (6.7) | 1 (4.3) | 0 |
| COS scale | ||||
| 1 (%) | 9 (5.2) | 8 (5.3) | 1 (4.3) | 0 (0) |
| 2 (%) | 15 (8.7) | 14 (9.3) | 1 (4.3) | 0 (0) |
| 3 (%) | 13 (7.5) | 11 (7.3) | 2 (8.6) | 0 (0) |
| 4 (%) | 8 (4.6) | 7 (4.6) | 1 (4.3) | 1 (12.5) |
| 5 (%) | 7 (4) | 5 (3.3) | 2 (8.6) | 1 (12.5) |
| 6 (%) | 13 (7.5) | 11 (7.3) | 2 (8.6) | 0 (0) |
| 7 (%) | 38 (22.1) | 34 (22.8) | 4 (17.3) | 2 (25) |
| 8 (%) | 51 (29.6) | 45 (30.2) | 6 (26.1) | 2 (25) |
| 9 (%) | 18 (10.4) | 14 (9.3) | 4 (17.3) | 2 (25) |
| Chest X-ray staging | 156 (90.6) | 133 (89.2) | 23 (100) | 8 (100) |
| Stage 0 n (%) | 67 (42.9) | 57 (38.2) | 10 (43.4) | 5 (62.5) |
| Stage 1 n (%) | 14 (8.9) | 12 (8) | 2 (8.6) | 0 (0) |
| Stage 2 n (%) | 23 (14.7) | 18 (12) | 5 (21.7) | 0 (0) |
| Stage 3 n (%) | 37 (23.7) | 32 (21.4) | 5 (21.7) | 2 (25) |
| Stage 4 n (%) | 15 (9.6) | 14 (9.3) | 1 (4.3) | 1 (12.5) |
| Pulmonary function tests | ||||
| FVC (mL) | 3391 ± 1132 | 3438 ± 1168 | 3119 ± 868 | 2606 ± 479 |
| % FVC predicted | 103 ± 19 | 103.5 ± 19 | 103.5 ± 21.6 | 86.5 ± 22.1 |
| FEV1 (mL) | 2585 ± 966 | 2632 ± 997 | 2328 ± 719 | 1878 ± 445 |
| % FEV1 predicted | 95.6 ± 20 | 96 ± 19.7 | 93 ± 19.6 | 77.7 ± 22.5 |
| FEV1/FVC (%) | 76 ± 7.5 | 76.2 ± 7.6 | 73.3 ± 5.6 | 70.2 ± 7.4 |
| DLCO predicted (%) | 78 ± 17 | 77.2 ± 16.6 | 80.6 ± 17.1 | 77.9 ± 21.6 |
| Urine calcium over 24 h (mg/24 h) |
| Parameters | Study Population | No MACE | MACE | Deaths | p-Value |
|---|---|---|---|---|---|
| N° | 172 | 149 | 23 | 8 | |
| LV end-diastolic volume (mL) | 96.6 ± 32.6 | 96.6 ± 32.7 | 97 ± 33.1 | 101 ± 27.7 | 0.9622 |
| LV end-systolic volume (mL) | 40.8 ± 16 | 40.8 ± 16.1 | 41.2 ± 14.9 | 44.2 ± 16.9 | 0.8946 |
| LV ejection fraction (%) | 57.3 ± 6.7 | 57.5 ± 6.5 | 55.8 ± 7.5 | 56.8 ± 8 | 0.2730 |
| LV mass index (g/m²) | 86.9 ± 29 | 86.1 ± 26.2 | 92.1 ± 44.5 | 97.1 ± 58.8 | 0.5444 |
| Left atrial area (cm²) | 17.1 ± 4.2 | 17.1 ± 4.3 | 17.2 ± 4 | 18.4 ± 5.1 | 0.9082 |
| Left atrial volume index (mL/m²) | 27.4 ± 9.6 | 27.2 ± 9.8 | 28.7 ± 10.4 | 30 ± 13.7 | 0.5314 |
| Mitral regurgitation ≥ moderate n (%) | 37 (21.51) | 34 (22.8) | 3 (13) | 2 (25) | 0.4154 |
| Tricuspid regurgitation ≥ moderate n (%) | 31 (18.02) | 29 (19.4) | 2 (8.6) | 2 (25) | 0.2591 |
| Right atrial area (cm²) | 12.7 ± 3.3 | 12.6 ± 3.3 | 13.2 ± 3.5 | 13.5 ± 4.8 | 0.4661 |
| TDI tricuspid wave (m/sec) | 0.13 ± 0.03 | 0.13 ± 0.031 | 0.13 ± 0.028 | 0.14 ± 0.025 | 0.6082 |
| TAPSE (mm) | 20.9 ± 3.5 | 21 ± 3.5 | 20.8 ± 3.1 | 20.8 ± 3.6 | 0.8047 |
| sPAP (mm/Hg) | 29.4 ± 8.3 | 29.5 ± 8.6 | 28.7 ± 5.3 | 28.7 ± 5.3 | 0.7048 |
| RV medium end-diastolic diameter (mm) | 28.1 ± 5.1 | 28.3 ± 5.3 | 27.1 ± 4.1 | 27.2 ± 3.9 | 0.2148 |
| RV sphericity index | 0.62 ± 0.09 | 0.62 ± 0.11 | 0.61 ± 0.1 | 0.60 ± 0.2 | 0.6018 |
| RV/LV ratio | 0.56 ± 0.07 | 0.56 ± 0.08 | 0.54 ± 0.06 | 0.53 ± 0.08 | 0.1955 |
| RVFAC (%) | 42.9 ± 8.7 | 43 ± 8.4 | 42.6 ± 6.3 | 40.8 ± 7.3 | 0.8267 |
| LV-GLS (%) | 18.3 ± 3.6 | 18.5 ± 3.5 | 16.8 ± 3.7 | 14.6 ± 3.7 | 0.0251 |
| Global PALS (%) | 30.5 ± 9 | 30.8 ± 8.1 | 28.5 ± 10.5 | 26.9 ± 9.2 | 0.2700 |
| Global PACS (%) | 16 ± 12.7 | 16.1 ± 13.4 | 15.2 ± 5 | 15.0 ± 4.8 | 0.5834 |
| PALS-4ch | 30 ± 9.6 | 30.4 ± 9.6 | 27.6 ± 9.8 | 26.2 ±10.3 | 0.1969 |
| PACS-4ch | 14.6 ± 5.4 | 14.5 ± 5.3 | 15 ± 6.4 | 13 ± 5.4 | 0.6741 |
| PALS-2ch | 31.2 ± 9.4 | 31.5 ± 9.7 | 28.9 ± 8.4 | 27.7 ± 9.1 | 0.1554 |
| PACS-2ch | 17.6 ± 23.7 | 17.9 ± 25.3 | 15.4 ± 5 | 14.8 ± 6.3 | 0.6389 |
| LS-4ch | 18.1 ± 3.6 | 18.3 ± 3.6 | 17.8 ± 3.1 | 17.5 ± 2.7 | 0.1638 |
| LS-2ch | 18.7 ± 4.8 | 19.2 ± 3.8 | 17.3 ± 8.1 | 15.9 ± 11.9 | 0.0986 |
| LS-3ch | 18.1 ± 3.7 | 18.3 ± 3.7 | 17 ± 3.3 | 16 ± 3.1 | 0.0619 |
| Global RVLS | 19.5 ± 4.1 | 19.6 ± 4.2 | 18.9 ± 2.8 | 17.6 ± 2.1 | 0.2084 |
| Free wall RVLS | 21.2 ± 5.2 | 21.4 ± 5.3 | 20.6 ± 3.8 | 20.2 ± 3.7 | 0.3661 |
| PALS-4ch RA | 34.1 ± 9.6 | 34.6 ± 9.6 | 31.8 ± 8.7 | 30.2 ± 12.1 | 0.0899 |
| PACS-4ch RA | 15.3 ± 5.4 | 15.4 ± 5.4 | 14.6 ± 5.8 | 15.2 ± 9.1 | 0.5379 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cameli, P.; Pastore, M.C.; Mandoli, G.E.; Vigna, M.; De Carli, G.; Bergantini, L.; d’Alessandro, M.; Ghionzoli, N.; Bargagli, E.; Cameli, M. Strain Echocardiography Is a Promising Tool for the Prognostic Assessment of Sarcoidosis. Life 2021, 11, 1065. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101065
Cameli P, Pastore MC, Mandoli GE, Vigna M, De Carli G, Bergantini L, d’Alessandro M, Ghionzoli N, Bargagli E, Cameli M. Strain Echocardiography Is a Promising Tool for the Prognostic Assessment of Sarcoidosis. Life. 2021; 11(10):1065. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101065
Chicago/Turabian StyleCameli, Paolo, Maria Concetta Pastore, Giulia Elena Mandoli, Mariangela Vigna, Giuseppe De Carli, Laura Bergantini, Miriana d’Alessandro, Nicolò Ghionzoli, Elena Bargagli, and Matteo Cameli. 2021. "Strain Echocardiography Is a Promising Tool for the Prognostic Assessment of Sarcoidosis" Life 11, no. 10: 1065. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101065