
Hearing Loss and Cognitive Impairment: Epidemiology, Common Pathophysiological Findings, and Treatment Considerations

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
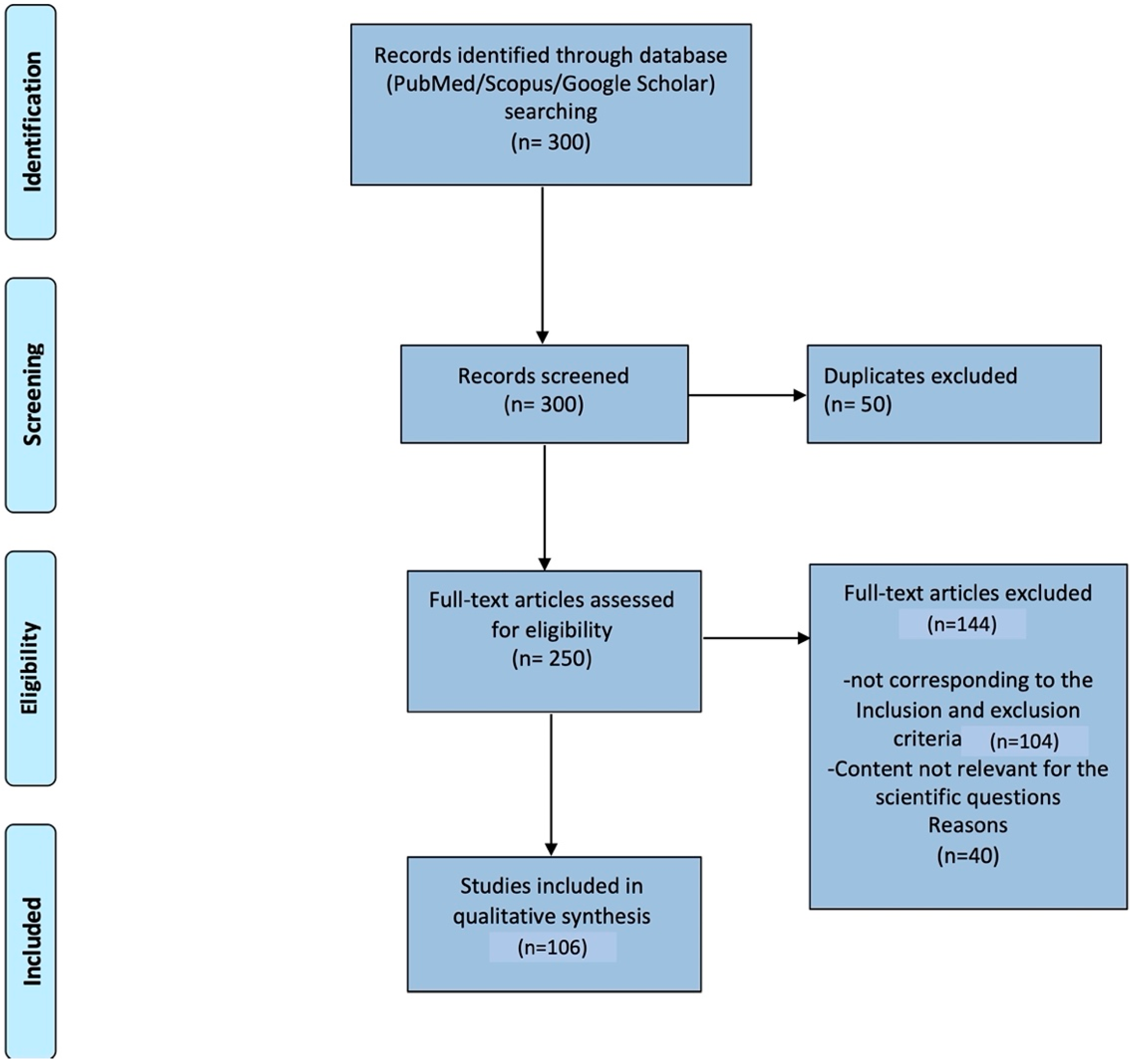
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Analysis of the Articles
3. Epidemiology
4. Definition of Hearing Loss and Cognitive Deficit in Elderly Population
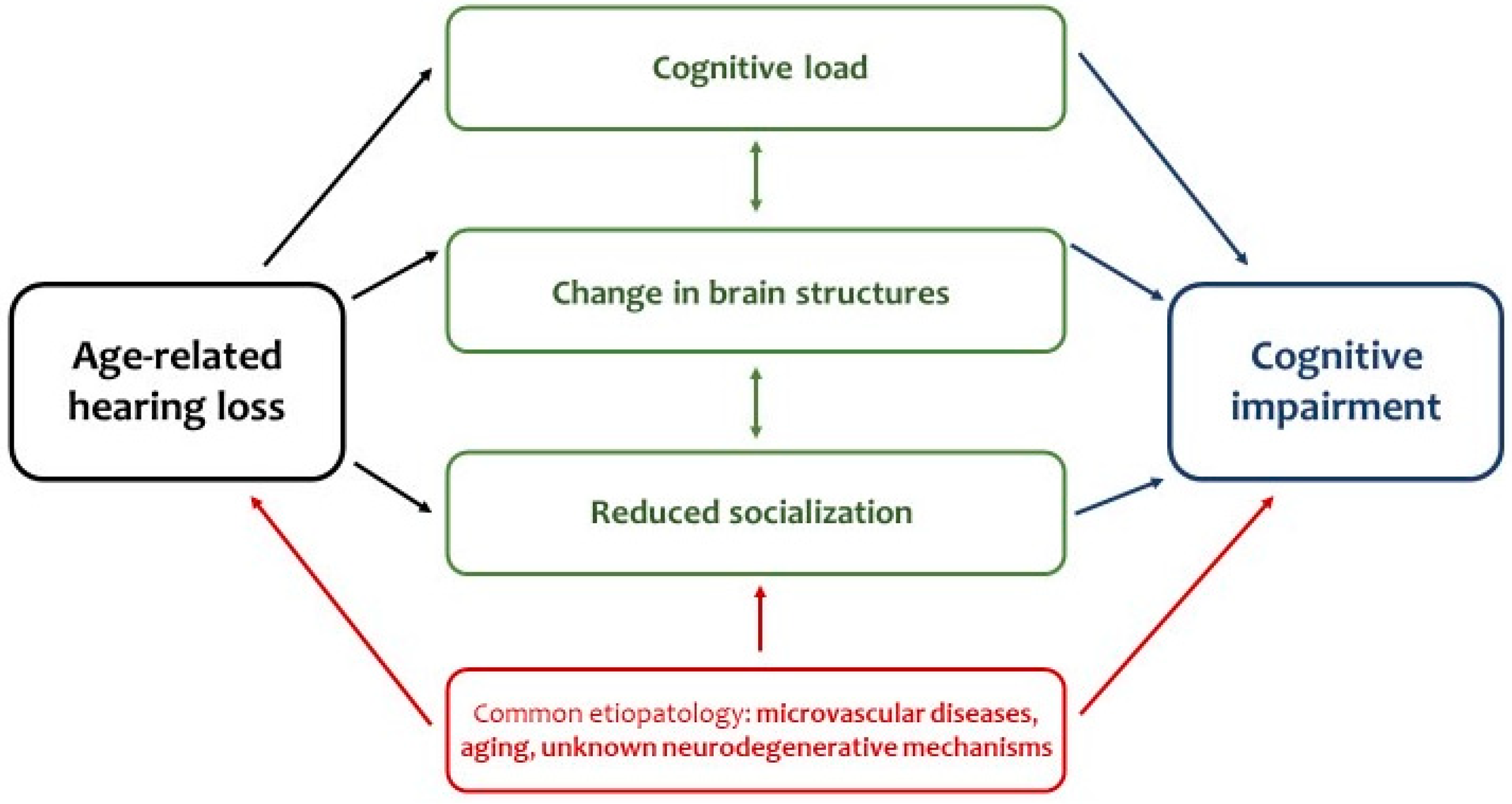
5. Common Pathophysiological Mechanisms
5.1. Increased Cognitive Load
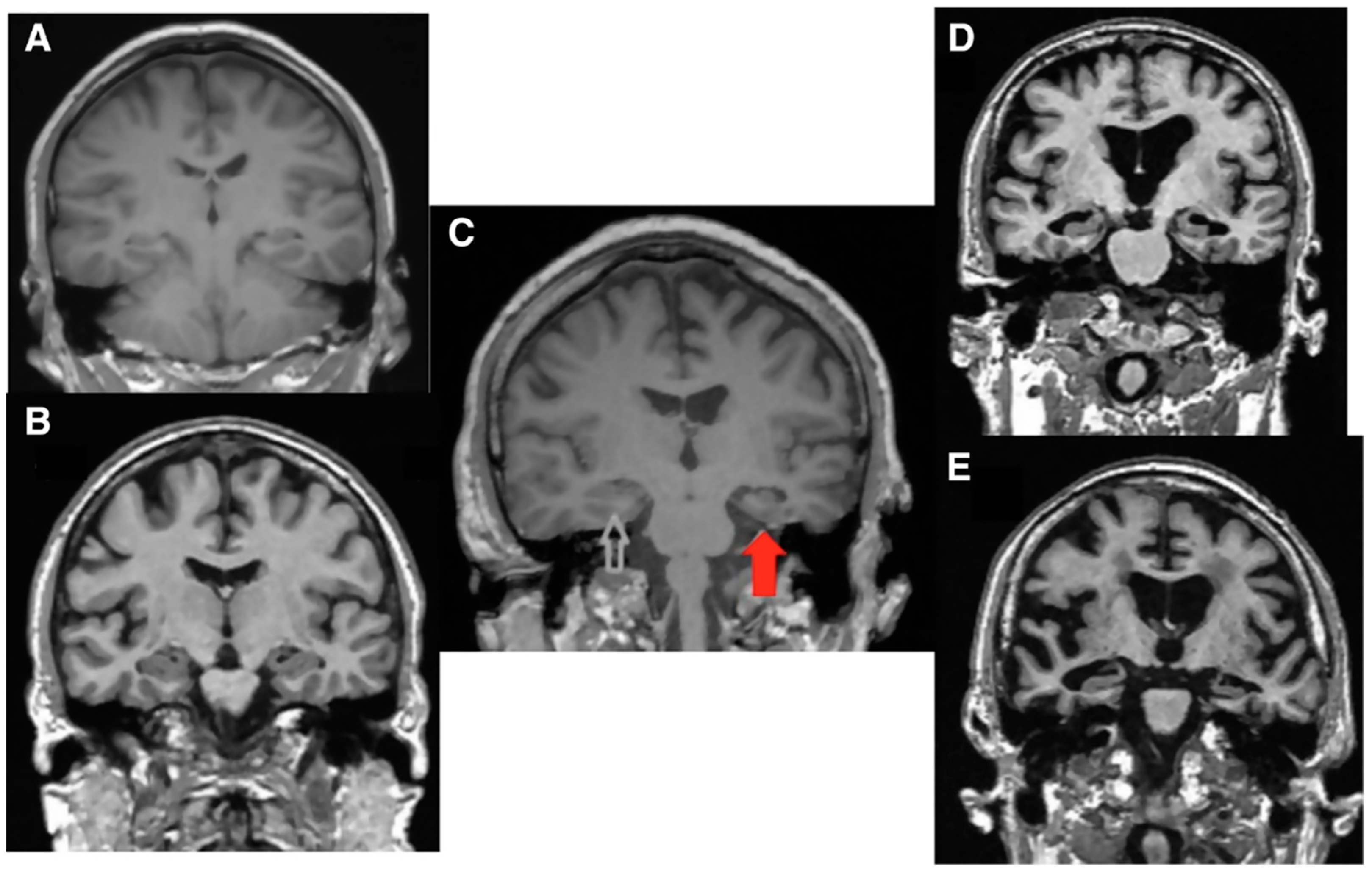
5.2. Changes in Brain Structure and Function
5.3. Common Pathological Conditions
5.4. Social Disengagement
6. Evaluation of Hearing Loss in Patients with Cognitive Impairment
7. Treatment of Hearing Loss in Patients with Cognitive Impairment
7.1. Hearing Aids
7.2. Hearing Amplification Devices
7.3. Cochlear Implant
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, Y.; Fan, S.; Liao, W.; Fang, W.; Xiao, S.; Liu, J. Hearing impairment and risk of Alzheimer’s disease: A meta-analysis of prospective cohort studies. Neurol. Sci. 2017, 38, 233–239. [Google Scholar] [CrossRef]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Simonsick, E.M.; et al. Hearing loss and cognitive decline in older adults. JAMA Intern. Med. 2013, 173, 293–299. [Google Scholar] [CrossRef]
- Ralli, M.; Gilardi, A.; Stadio, A.D.; Severini, C.; Salzano, F.A.; Greco, A.; Vincentiis, M. Hearing loss and Alzheimer’s disease: A Review. Int. Tinnitus J. 2019, 23, 79–85. [Google Scholar] [CrossRef]
- Golub, J.S. Brain changes associated with age-related hearing loss. Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Ferrucci, L.; An, Y.; Goh, J.O.; Doshi, J.; Metter, E.J.; Davatzikos, C.; Kraut, M.A.; Resnick, S.M. Association of hearing impairment with brain volume changes in older adults. Neuroimage 2014, 90, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlmann, R.F.; Larson, E.B.; Rees, T.S.; Koepsell, T.D.; Duckert, L.G. Relationship of hearing impairment to dementia and cognitive dysfunction in older adults. JAMA 1989, 261, 1916–1919. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Metter, E.J.; O’Brien, R.J.; Resnick, S.M.; Zonderman, A.B.; Ferrucci, L. Hearing loss and incident dementia. Arch. Neurol. 2011, 68, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Gallacher, J.; Ilubaera, V.; Ben-Shlomo, Y.; Bayer, A.; Fish, M.; Babisch, W.; Elwood, P. Auditory threshold, phonologic demand, and incident dementia. Neurology 2012, 79, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Meusy, A. Presbycusis and Dementia: Results from 8 years of follow-up in the three-city Montpellier study. J. Alzheimer’s Assoc. 2016, 1, 12–175. [Google Scholar] [CrossRef]
- Fritze, T.; Teipel, S.; Ovari, A.; Kilimann, I.; Witt, G.; Doblhammer, G. Hearing Impairment Affects Dementia Incidence. An Analysis Based on Longitudinal Health Claims Data in Germany. PLoS ONE 2016, 11, e0156876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amieva, H.; Ouvrard, C.; Giulioli, C.; Meillon, C.; Rullier, L.; Dartigues, J.F. Self-Reported Hearing Loss, Hearing Aids, and Cognitive Decline in Elderly Adults: A 25-Year Study. J. Am. Geriatr. Soc. 2015, 63, 2099–2104. [Google Scholar] [CrossRef]
- Dawes, P.; Emsley, R.; Cruickshanks, K.J.; Moore, D.R.; Fortnum, H.; Edmondson-Jones, M.; McCormack, A.; Munro, K.J. Hearing loss and cognition: The role of hearing AIDS, social isolation and depression. PLoS ONE 2015, 10, e0119616. [Google Scholar] [CrossRef] [Green Version]
- Dawes, P.; Cruickshanks, K.J.; Fischer, M.E.; Klein, B.E.; Klein, R.; Nondahl, D.M. Hearing-aid use and long-term health outcomes: Hearing handicap, mental health, social engagement, cognitive function, physical health, and mortality. Int. J. Audiol. 2015, 54, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Deal, J.A.; Reed, N.S.; Kravetz, A.D.; Weinreich, H.; Yeh, C.; Lin, F.R.; Altan, A. Incident Hearing Loss and Comorbidity: A Longitudinal Administrative Claims Study. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 36–43. [Google Scholar] [CrossRef]
- Fong, T.G.; Davis, D.; Growdon, M.E.; Albuquerque, A.; Inouye, S.K. The interface between delirium and dementia in elderly adults. Lancet Neurol. 2015, 14, 823–832. [Google Scholar] [CrossRef] [Green Version]
- Linszen, M.M.; Brouwer, R.M.; Heringa, S.M.; Sommer, I.E. Increased risk of psychosis in patients with hearing impairment: Review and meta-analyses. Neurosci. Biobehav. Rev. 2016, 62, 1–20. [Google Scholar] [CrossRef]
- El Haj, M.; Roche, J.; Jardri, R.; Kapogiannis, D.; Gallouj, K.; Antoine, P. Clinical and neurocognitive aspects of hallucinations in Alzheimer’s disease. Neurosci. Biobehav. Rev. 2017, 83, 713–720. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Costs of Unaddressed Hearing Loss and Cost-Effectiveness of Interventions: A Who Report. Deafness Prevention. 2017. Available online: https://www.who.int/deafness/en/ (accessed on 28 September 2021).
- Alzheimer’s Disease International. World Alzheimer’s Report. 2018. Available online: https://www.alz.co.uk/research/world-report-2018 (accessed on 28 September 2021).
- Gordon, A.L.; Franklin, M.; Bradshaw, L.; Logan, P.; Elliott, R.; Gladman, J.R. Health status of UK care home residents: A cohort study. Age Ageing 2014, 43, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernabei, R.; Bonuccelli, U.; Maggi, S.; Marengoni, A.; Martini, A.; Memo, M.; Pecorelli, S.; Peracino, A.P.; Quaranta, N.; Stella, R.; et al. Hearing loss and cognitive decline in older adults: Questions and answers. Aging Clin. Exp. Res. 2014, 26, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.Y. Pathophysiology of age-related hearing loss (peripheral and central). Korean J. Audiol. 2013, 17, 45–49. [Google Scholar] [CrossRef] [Green Version]
- Sardone, R.; Castellana, F.; Bortone, I.; Lampignano, L.; Zupo, R.; Lozupone, M.; Griseta, C.; Dibello, V.; Seripa, D.; Guerra, V.; et al. Association Between Central and Peripheral Age-Related Hearing Loss and Different Frailty Phenotypes in an Older Population in Southern Italy. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Di Stadio, A.; Ralli, M.; Roccamatisi, D.; Scarpa, A.; Della Volpe, A.; Cassandro, C.; Ricci, G.; Greco, A.; Bernitsas, E. Hearing loss and dementia: Radiologic and biomolecular basis of their shared characteristics. A systematic review. Neurol. Sci. 2021, 42, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Ohlemiller, K.K. Age-related hearing loss: The status of Schuknecht’s typology. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Di Stadio, A. Which factors to induce hearing loss in professional musicians? Extensive literature review and histopathology findings can answer it. Hear. Balance Commun. 2017, 15, 63–71. [Google Scholar] [CrossRef]
- Elangovan, S.; Spankovich, C. Diabetes and Auditory-Vestibular Pathology. Semin. Hear. 2019, 40, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, S.G.; Liberman, M.C. Synaptopathy in the noise-exposed and aging cochlea: Primary neural degeneration in acquired sensorineural hearing loss. Hear. Res. 2015, 330, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Di Stadio, A.D.V.; Della Volpe, A.; Ralli, M.; Ricci, G.; Greco, A. Spiral ganglions and speech perception in the elderly. Which turn of the cochlea is the more relevant? A preliminary study on human temporal bones. J. Adv. Otol. 2020, 16, 318. [Google Scholar] [CrossRef]
- Roth, T.N. Aging of the auditory system. Handb. Clin. Neurol. 2015, 129, 357–373. [Google Scholar] [CrossRef]
- Di Stadio, A.; Messineo, D.; Ralli, M.; Roccamatisi, D.; Musacchio, A.; Ricci, G.; Greco, A. The impact of white matter hyperintensities on speech perception. Neurol. Sci. 2020, 41, 1891–1898. [Google Scholar] [CrossRef]
- Fusconi, M.; Attanasio, G.; Capitani, F.; Di Porto, E.; Diacinti, D.; Musy, I.; Ralli, M.; Ralli, G.; Greco, A.; de Vincentiis, M.; et al. Is there a relation between sudden sensorineural hearing loss and white matter lesions? Eur. Arch. Otorhinolaryngol. 2019, 276, 3043–3049. [Google Scholar] [CrossRef] [PubMed]
- Sardone, R.; Battista, P.; Donghia, R.; Lozupone, M.; Tortelli, R.; Guerra, V.; Grasso, A.; Griseta, C.; Castellana, F.; Zupo, R.; et al. Age-Related Central Auditory Processing Disorder, MCI, and Dementia in an Older Population of Southern Italy. Otolaryngol. Head Neck Surg. 2020, 163, 348–355. [Google Scholar] [CrossRef]
- Kirova, A.M.; Bays, R.B.; Lagalwar, S. Working memory and executive function decline across normal aging, mild cognitive impairment, and Alzheimer’s disease. Biomed. Res. Int. 2015, 2015, 748212. [Google Scholar] [CrossRef] [Green Version]
- Severini, C.; Barbato, C.; Di Certo, M.G.; Gabanella, F.; Petrella, C.; Di Stadio, A.; de Vincentiis, M.; Polimeni, A.; Ralli, M.; Greco, A. Alzheimer’s disease: New concepts on the role of autoimmunity and of NLRP3 inflammasome in the pathogenesis of the disease. Curr. Neuropharmacol. 2020, 19, 498–512. [Google Scholar] [CrossRef]
- Lozupone, M.; Sardone, R.; Donghia, R.; D’Urso, F.; Piccininni, C.; Battista, P.; Di Gioia, I.; Resta, E.; Castellana, F.; Lampignano, L.; et al. Late-onset depression is associated to age-related central auditory processing disorder in an older population in Southern Italy. Geroscience 2021, 43, 1003–1014. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Uchida, Y.; Sugiura, S.; Nishita, Y.; Saji, N.; Sone, M.; Ueda, H. Age-related hearing loss and cognitive decline—The potential mechanisms linking the two. Auris Nasus Larynx 2019, 46, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, A.S.; Jin, P.; Sweller, J. Cognitive Load and Learner Expertise: Split-Attention and Redundancy Effects in Reading with Explanatory Notes. Contemp. Educ. Psychol. 1998, 23, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Sweller, J. Measuring cognitive load. Perspect. Med. Educ. 2018, 7, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panza, F.; Solfrizzi, V.; Seripa, D.; Imbimbo, B.P.; Capozzo, R.; Quaranta, N.; Pilotto, A.; Logroscino, G. Age-related hearing impairment and frailty in Alzheimer’s disease: Interconnected associations and mechanisms. Front. Aging Neurosci. 2015, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Ohlenforst, B.; Zekveld, A.A.; Jansma, E.P.; Wang, Y.; Naylor, G.; Lorens, A.; Lunner, T.; Kramer, S.E. Effects of Hearing Impairment and Hearing Aid Amplification on Listening Effort: A Systematic Review. Ear Hear. 2017, 38, 267–281. [Google Scholar] [CrossRef] [Green Version]
- Van Engen, K.J.; McLaughlin, D.J. Eyes and ears: Using eye tracking and pupillometry to understand challenges to speech recognition. Hear. Res. 2018, 369, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Ponticorvo, S.; Manara, R.; Pfeuffer, J.; Cappiello, A.; Cuoco, S.; Pellecchia, M.T.; Saponiero, R.; Troisi, D.; Cassandro, C.; John, M.; et al. Cortical pattern of reduced perfusion in hearing loss revealed by ASL-MRI. Hum. Brain Mapp. 2019, 40, 2475–2487. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, A.; Fuccillo, E.; Martorana, A.; Ricci, M.; Giacomini, P.G.; Schillaci, O.; Di Girolamo, S. Hearing and cognitive impairment: A functional evaluation of associative brain areas in patients affected by Alzheimer’s disease. Funct. Neurol. 2019, 34, 15–20. [Google Scholar]
- Rutherford, B.R.; Brewster, K.; Golub, J.S.; Kim, A.H.; Roose, S.P. Sensation and Psychiatry: Linking Age-Related Hearing Loss to Late-Life Depression and Cognitive Decline. Am. J. Psychiatry 2018, 175, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Uchida, Y.; Nishita, Y.; Kato, T.; Iwata, K.; Sugiura, S.; Suzuki, H.; Sone, M.; Tange, C.; Otsuka, R.; Ando, F.; et al. Smaller Hippocampal Volume and Degraded Peripheral Hearing Among Japanese Community Dwellers. Front. Aging Neurosci. 2018, 10, 319. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Glick, H.; Campbell, J.; Torres, J.; Dorman, M.; Zeitler, D.M. Cortical Plasticity and Reorganization in Pediatric Single-sided Deafness Pre- and Postcochlear Implantation: A Case Study. Otol. Neurotol. 2016, 37, e26–e34. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.M. Does treating hearing loss prevent or slow the progress of dementia? Hearing is not all in the ears, but who’s listening? CNS Spectr. 2017, 22, 247–250. [Google Scholar] [CrossRef]
- Wayne, R.V.; Johnsrude, I.S. A review of causal mechanisms underlying the link between age-related hearing loss and cognitive decline. Ageing Res. Rev. 2015, 23, 154–166. [Google Scholar] [CrossRef]
- Lin, F.R.; Albert, M. Hearing loss and dementia—Who is listening? Aging Ment. Health 2014, 18, 671–673. [Google Scholar] [CrossRef] [Green Version]
- Petrella, C.; Di Certo, M.G.; Barbato, C.; Gabanella, F.; Ralli, M.; Greco, A.; Possenti, R.; Severini, C. Neuropeptides in Alzheimer’s Disease: An Update. Curr. Alzheimer Res. 2019, 16, 544–558. [Google Scholar] [CrossRef]
- Ciafre, S.; Ferraguti, G.; Tirassa, P.; Iannitelli, A.; Ralli, M.; Greco, A.; Chaldakov, G.N.; Rosso, P.; Fico, E.; Messina, M.P.; et al. Nerve growth factor in the psychiatric brain. Riv. Psichiatr. 2020, 55, 4–15. [Google Scholar] [CrossRef]
- Tavanai, E.; Mohammadkhani, G. Role of antioxidants in prevention of age-related hearing loss: A review of literature. Eur. Arch. Otorhinolaryngol. 2017, 274, 1821–1834. [Google Scholar] [CrossRef]
- Wolters, F.J.; Segufa, R.A.; Darweesh, S.K.L.; Bos, D.; Ikram, M.A.; Sabayan, B.; Hofman, A.; Sedaghat, S. Coronary heart disease, heart failure, and the risk of dementia: A systematic review and meta-analysis. Alzheimer’s Dement. 2018, 14, 1493–1504. [Google Scholar] [CrossRef]
- Lourenco, J.; Serrano, A.; Santos-Silva, A.; Gomes, M.; Afonso, C.; Freitas, P.; Paul, C.; Costa, E. Cardiovascular Risk Factors Are Correlated with Low Cognitive Function among Older Adults Across Europe Based on The SHARE Database. Aging Dis. 2018, 9, 90–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Ryou, N.; Jun, H.J.; Hwang, S.Y.; Song, J.J.; Chae, S.W. Effect of Cigarette Smoking and Passive Smoking on Hearing Impairment: Data from a Population-Based Study. PLoS ONE 2016, 11, e0146608. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Sugiura, S.; Ando, F.; Nakashima, T.; Shimokata, H. Diabetes reduces auditory sensitivity in middle-aged listeners more than in elderly listeners: A population- based study of age-related hearing loss. Med. Sci. Monit. 2010, 16, PH63–PH68. [Google Scholar] [PubMed]
- Attanasio, G.; Califano, L.; Bruno, A.; Giugliano, V.; Ralli, M.; Martellucci, S.; Milella, C.; de Vincentiis, M.; Russo, F.Y.; Greco, A. Chronic cerebrospinal venous insufficiency and meniere’s disease: Interventional versus medical therapy. Laryngoscope 2019, 130, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, M.; De Luca, P.; Scarpa, A.; Ralli, M.; Bottiglieri, P.; Cassandro, E.; Iemma, M. SCORE risk scale as a prognostic factor after sudden sensorineural hearing loss. Eur. Arch. Otorhinolaryngol. 2019, 276, 2739–2745. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Zhang, Y.; Li, M.; Wu, J.H.; Mai, L.; Li, J.; Yang, Y.; Hu, Y.; Huang, Y. Association between prediabetes and risk of all cause mortality and cardiovascular disease: Updated meta-analysis. BMJ 2020, 370, m2297. [Google Scholar] [CrossRef]
- Gopinath, B.; Schneider, J.; Rochtchina, E.; Leeder, S.R.; Mitchell, P. Association between age-related hearing loss and stroke in an older population. Stroke 2009, 40, 1496–1498. [Google Scholar] [CrossRef] [PubMed]
- Sarant, J.Z.; Bowe, S.J.; McEvoy, M.; Attia, J. The Apolipoprotein Allele and Sensorineural Hearing Loss in Older Community-Dwelling Adults in Australia. Ear Hear. 2019, 41, 622–629. [Google Scholar] [CrossRef]
- Dawes, P.; Platt, H.; Horan, M.; Ollier, W.; Munro, K.; Pendleton, N.; Payton, A. No association between apolipoprotein E or N-acetyltransferase 2 gene polymorphisms and age-related hearing loss. Laryngoscope 2015, 125, E33–E38. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, C.; Westendorp, R.G.; de Craen, A.J.; Gussekloo, J.; de Laat, J.; van Exel, E. Gene dose of apolipoprotein E and age-related hearing loss. Neurobiol. Aging 2012, 33, 2230 e2237–2230 e2212. [Google Scholar] [CrossRef]
- Shen, Y.; Ye, B.; Chen, P.; Wang, Q.; Fan, C.; Shu, Y.; Xiang, M. Cognitive Decline, Dementia, Alzheimer’s Disease and Presbycusis: Examination of the Possible Molecular Mechanism. Front. Neurosci. 2018, 12, 394. [Google Scholar] [CrossRef]
- Hardy, C.J.; Marshall, C.R.; Golden, H.L.; Clark, C.N.; Mummery, C.J.; Griffiths, T.D.; Bamiou, D.E.; Warren, J.D. Hearing and dementia. J. Neurol. 2016, 263, 2339–2354. [Google Scholar] [CrossRef] [Green Version]
- Ray, M.; Dening, T.; Crosbie, B. Dementia and hearing loss: A narrative review. Maturitas 2019, 128, 64–69. [Google Scholar] [CrossRef]
- Mick, P.; Kawachi, I.; Lin, F.R. The association between hearing loss and social isolation in older adults. Otolaryngol. Head Neck Surg. 2014, 150, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Resnick, H.E.; Fries, B.E.; Verbrugge, L.M. Windows to their world: The effect of sensory impairments on social engagement and activity time in nursing home residents. J. Gerontol. B Psychol. Sci. Soc. Sci. 1997, 52, S135–S144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, S.W.; Hawkley, L.C.; Arevalo, J.M.; Cacioppo, J.T. Transcript origin analysis identifies antigen-presenting cells as primary targets of socially regulated gene expression in leukocytes. Proc. Natl. Acad. Sci. USA 2011, 108, 3080–3085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, S.W.; Hawkley, L.C.; Arevalo, J.M.; Sung, C.Y.; Rose, R.M.; Cacioppo, J.T. Social regulation of gene expression in human leukocytes. Genome Biol. 2007, 8, R189. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, L.E.; Palmer, C.V.; Pratt, S.; Erickson, K.I.; Moncrieff, D. The Effect of Decreased Audibility on MMSE Performance: A Measure Commonly Used for Diagnosing Dementia. J. Am. Acad. Audiol. 2016, 27, 311–323. [Google Scholar] [CrossRef]
- Dupuis, K.; Pichora-Fuller, M.K.; Chasteen, A.L.; Marchuk, V.; Singh, G.; Smith, S.L. Effects of hearing and vision impairments on the Montreal Cognitive Assessment. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2015, 22, 413–437. [Google Scholar] [CrossRef] [PubMed]
- NICE. Hearing Loss in Adults: Assessment and Management. 2018. Available online: https://www.nice.org.uk/guidance/ng98 (accessed on 26 September 2021).
- Swords, G.M.; Nguyen, L.T.; Mudar, R.A.; Llano, D.A. Auditory system dysfunction in Alzheimer disease and its prodromal states: A review. Ageing Res. Rev. 2018, 44, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Gates, G.A.; Anderson, M.L.; McCurry, S.M.; Feeney, M.P.; Larson, E.B. Central auditory dysfunction as a harbinger of Alzheimer dementia. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 390–395. [Google Scholar] [CrossRef] [Green Version]
- Idrizbegovic, E.; Hederstierna, C.; Dahlquist, M.; Kampfe Nordstrom, C.; Jelic, V.; Rosenhall, U. Central auditory function in early Alzheimer’s disease and in mild cognitive impairment. Age Ageing 2011, 40, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, G.A. Central presbycusis: An emerging view. Otolaryngol. Head Neck Surg. 2012, 147, 1–2. [Google Scholar] [CrossRef]
- Quaranta, N.; Coppola, F.; Casulli, M.; Barulli, M.R.; Panza, F.; Tortelli, R.; Capozzo, R.; Leo, A.; Tursi, M.; Grasso, A.; et al. The prevalence of peripheral and central hearing impairment and its relation to cognition in older adults. Audiol. Neurootol. 2014, 19, 10–14. [Google Scholar] [CrossRef]
- Ralli, M.; Greco, A.; De Vincentiis, M.; Sheppard, A.; Cappelli, G.; Neri, I.; Salvi, R. Tone-in-noise detection deficits in elderly patients with clinically normal hearing. Am. J. Otolaryngol. 2019, 40, 1–9. [Google Scholar] [CrossRef]
- Salvi, R.; Ding, D.; Jiang, H.; Chen, G.D.; Greco, A.; Manohar, S.; Sun, W.; Ralli, M. Hidden Age-Related Hearing Loss and Hearing Disorders: Current Knowledge and Future Directions. Hear. Balance Commun. 2018, 16, 74–82. [Google Scholar] [CrossRef]
- Sergeyenko, Y.; Lall, K.; Liberman, M.C.; Kujawa, S.G. Age-related cochlear synaptopathy: An early-onset contributor to auditory functional decline. J. Neurosci. 2013, 33, 13686–13694. [Google Scholar] [CrossRef]
- Liberman, M.C.; Kujawa, S.G. Cochlear synaptopathy in acquired sensorineural hearing loss: Manifestations and mechanisms. Hear. Res. 2017, 349, 138–147. [Google Scholar] [CrossRef]
- Viana, L.M.; O’Malley, J.T.; Burgess, B.J.; Jones, D.D.; Oliveira, C.A.; Santos, F.; Merchant, S.N.; Liberman, L.D.; Liberman, M.C. Cochlear neuropathy in human presbycusis: Confocal analysis of hidden hearing loss in post-mortem tissue. Hear. Res. 2015, 327, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loughrey, D.G.; Kelly, M.E.; Kelley, G.A.; Brennan, S.; Lawlor, B.A. Association of Age-Related Hearing Loss with Cognitive Function, Cognitive Impairment, and Dementia: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Jayakody, D.M.P.; Friedland, P.L.; Martins, R.N.; Sohrabi, H.R. Impact of Aging on the Auditory System and Related Cognitive Functions: A Narrative Review. Front. Neurosci. 2018, 12, 125. [Google Scholar] [CrossRef] [PubMed]
- Fetoni, A.R.; Ralli, M.; Sergi, B.; Parrilla, C.; Troiani, D.; Paludetti, G. Protective properties of antioxidant drugs in noise-induced hearing loss in the guinea pig. Audiol. Med. 2009, 6, 271–277. [Google Scholar] [CrossRef]
- Ralli, M.; Lobarinas, E.; Fetoni, A.R.; Stolzberg, D.; Paludetti, G.; Salvi, R. Comparison of salicylate- and quinine-induced tinnitus in rats: Development, time course, and evaluation of audiologic correlates. Otol. Neurotol. 2010, 31, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Ralli, M.; Troiani, D.; Podda, M.V.; Paciello, F.; Eramo, S.L.; de Corso, E.; Salvi, R.; Paludetti, G.; Fetoni, A.R. The effect of the NMDA channel blocker memantine on salicylate-induced tinnitus in rats. Acta Otorhinolaryngol. Ital. 2014, 34, 198–204. [Google Scholar]
- Amazan, D.; Cordero, G.; Lopez-Bote, C.J.; Lauridsen, C.; Rey, A.I. Effects of oral micellized natural vitamin E (D-alpha-tocopherol) v. synthetic vitamin E (DL-alpha-tocopherol) in feed on alpha-tocopherol levels, stereoisomer distribution, oxidative stress and the immune response in piglets. Animal 2014, 8, 410–419. [Google Scholar] [CrossRef] [Green Version]
- Gul, F.; Muderris, T.; Yalciner, G.; Sevil, E.; Bercin, S.; Ergin, M.; Babademez, M.A.; Kiris, M. A comprehensive study of oxidative stress in sudden hearing loss. Eur. Arch. Otorhinolaryngol. 2017, 274, 1301–1308. [Google Scholar] [CrossRef]
- Henderson, D.; Bielefeld, E.C.; Harris, K.C.; Hu, B.H. The role of oxidative stress in noise-induced hearing loss. Ear Hear. 2006, 27, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Sha, S.H.; Schacht, J. Emerging therapeutic interventions against noise-induced hearing loss. Expert Opin. Investig. Drugs 2017, 26, 85–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralli, M.G.; Greco, A.; De Vincentiis, M. Hearing loss following unsafe listening practices in children, teenagers and young adults: An underestimated public health threat? Int. J. High Risk Behav. 2018, 7, e65873. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.L.; Sheppard, A.; Ralli, M.; Liu, X.; Salvi, R. Prolonged low-level noise exposure reduces rat distortion product otoacoustic emissions above a critical level. Hear. Res. 2018, 370, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Moberly, A.C.; Doerfer, K.; Harris, M.S. Does Cochlear Implantation Improve Cognitive Function? Laryngoscope 2019, 129, 2208–2209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulrow, C.D.; Aguilar, C.; Endicott, J.E.; Tuley, M.R.; Velez, R.; Charlip, W.S.; Rhodes, M.C.; Hill, J.A.; DeNino, L.A. Quality-of-life changes and hearing impairment. A randomized trial. Ann. Intern. Med. 1990, 113, 188–194. [Google Scholar] [CrossRef]
- Maharani, A.; Dawes, P.; Nazroo, J.; Tampubolon, G.; Pendleton, N.; group, S.E.-C.W. Longitudinal Relationship Between Hearing Aid Use and Cognitive Function in Older Americans. J. Am. Geriatr. Soc. 2018, 66, 1130–1136. [Google Scholar] [CrossRef] [Green Version]
- Deal, J.A.; Sharrett, A.R.; Albert, M.S.; Coresh, J.; Mosley, T.H.; Knopman, D.; Wruck, L.M.; Lin, F.R. Hearing impairment and cognitive decline: A pilot study conducted within the atherosclerosis risk in communities neurocognitive study. Am. J. Epidemiol. 2015, 181, 680–690. [Google Scholar] [CrossRef] [Green Version]
- Shukla, A.; Nieman, C.L.; Price, C.; Harper, M.; Lin, F.R.; Reed, N.S. Impact of Hearing Loss on Patient-Provider Communication Among Hospitalized Patients: A Systematic Review. Am. J. Med. Qual. 2019, 34, 284–292. [Google Scholar] [CrossRef]
- Mamo, S.K.; Nirmalasari, O.; Nieman, C.L.; McNabney, M.K.; Simpson, A.; Oh, E.S.; Lin, F.R. Hearing Care Intervention for Persons with Dementia: A Pilot Study. Am. J. Geriatr. Psychiatry 2017, 25, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Dawes, P. Hearing interventions to prevent dementia. HNO 2019, 67, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Volter, C.; Gotze, L.; Dazert, S.; Falkenstein, M.; Thomas, J.P. Can cochlear implantation improve neurocognition in the aging population? Clin. Interv. Aging 2018, 13, 701–712. [Google Scholar] [CrossRef] [Green Version]
- Jayakody, D.M.P.; Friedland, P.L.; Nel, E.; Martins, R.N.; Atlas, M.D.; Sohrabi, H.R. Impact of Cochlear Implantation on Cognitive Functions of Older Adults: Pilot Test Results. Otol. Neurotol. 2017, 38, e289–e295. [Google Scholar] [CrossRef]
- Cosetti, M.K.; Pinkston, J.B.; Flores, J.M.; Friedmann, D.R.; Jones, C.B.; Roland, J.T., Jr.; Waltzman, S.B. Neurocognitive testing and cochlear implantation: Insights into performance in older adults. Clin. Interv. Aging 2016, 11, 603–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosnier, I.; Bebear, J.P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artieres, F.; Bordure, P.; Robier, A.; et al. Predictive factors of cochlear implant outcomes in the elderly. Audiol. Neurootol. 2014, 19, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Mosnier, I.; Bebear, J.P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artieres, F.; Bordure, P.; Robier, A.; et al. Improvement of cognitive function after cochlear implantation in elderly patients. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 442–450. [Google Scholar] [CrossRef]
- Della Volpe, A.; Ippolito, V.; Roccamatisi, D.; Garofalo, S.; De Lucia, A.; Gambacorta, V.; Longari, F.; Ricci, G.; Di Stadio, A. Does Unilateral Hearing Loss Impair Working Memory? An Italian Clinical Study Comparing Patients with and Without Hearing Aids. Front. Neurosci. 2020, 14, 905. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author and Year | Population Studied | Results |
|---|---|---|
| Uhlmann, 1989 [6] | 100 cases with Alzheimer’s dementia and 100 nondemented controls | Hearing loss of 30 dB or greater significantly higher in cases than in controls. Greater hearing loss associated with a more severe dementia. |
| Lin, 2011 [7] | 639 older adults without dementia | Mild, moderate or severe hearing loss associated with a risk of cognitive decline, respectively, two, three and five-fold higher than in normal-hearing population |
| Gallacher, 2012 [8] | 1057 men | Risk of developing dementia 2.7-fold higher for every 10 dB of hearing loss |
| Amieva, 2015 [11] | 3670 people aged 65 and older | Worse hearing associated with lower cognitive efficiency scores and with greater decline in cerebral activity |
| Dawes, 2015 [13] | 164,770 adults aged 40–69 | Frail hearing associated with higher levels of cognitive impairment |
| Meusy, 2016 [9] | 600 men and women without dementia | Hearing loss in 77% of dementia population. ARHL associated with an over 3-fold increase in the probability of manifesting dementia |
| Fritze, 2016 [10] | 154,783 people aged 65 and older, including 14,602 cases of dementia | Bilateral hearing loss associated with a 43% increase in the probability of developing dementia; unilateral hearing loss with a 20% increase |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bisogno, A.; Scarpa, A.; Di Girolamo, S.; De Luca, P.; Cassandro, C.; Viola, P.; Ricciardiello, F.; Greco, A.; De Vincentiis, M.; Ralli, M.; et al. Hearing Loss and Cognitive Impairment: Epidemiology, Common Pathophysiological Findings, and Treatment Considerations. Life 2021, 11, 1102. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101102
Bisogno A, Scarpa A, Di Girolamo S, De Luca P, Cassandro C, Viola P, Ricciardiello F, Greco A, De Vincentiis M, Ralli M, et al. Hearing Loss and Cognitive Impairment: Epidemiology, Common Pathophysiological Findings, and Treatment Considerations. Life. 2021; 11(10):1102. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101102
Chicago/Turabian StyleBisogno, Antonella, Alfonso Scarpa, Stefano Di Girolamo, Pietro De Luca, Claudia Cassandro, Pasquale Viola, Filippo Ricciardiello, Antonio Greco, Marco De Vincentiis, Massimo Ralli, and et al. 2021. "Hearing Loss and Cognitive Impairment: Epidemiology, Common Pathophysiological Findings, and Treatment Considerations" Life 11, no. 10: 1102. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101102