
Role of Oxidative Stress and Inflammatory Cytokines (TNF-α and IL-6) in Acetic Acid-Induced Ulcerative Colitis in Rats: Ameliorated by Otostegia fruticosa

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Plant Collection and Extraction
2.3. Animals
2.4. Acute Toxicity Study
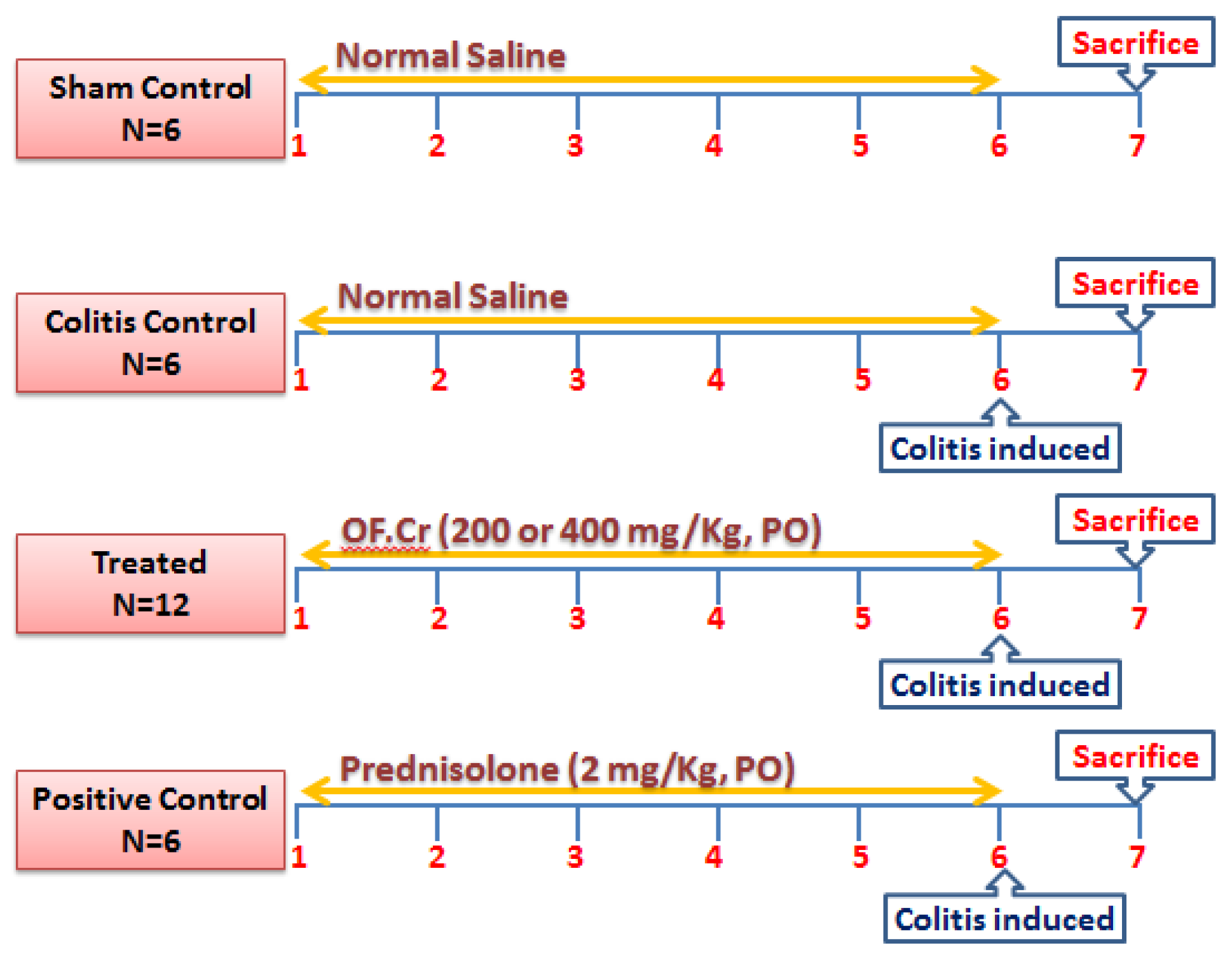
2.5. Study Design
2.6. Induction of Colitis
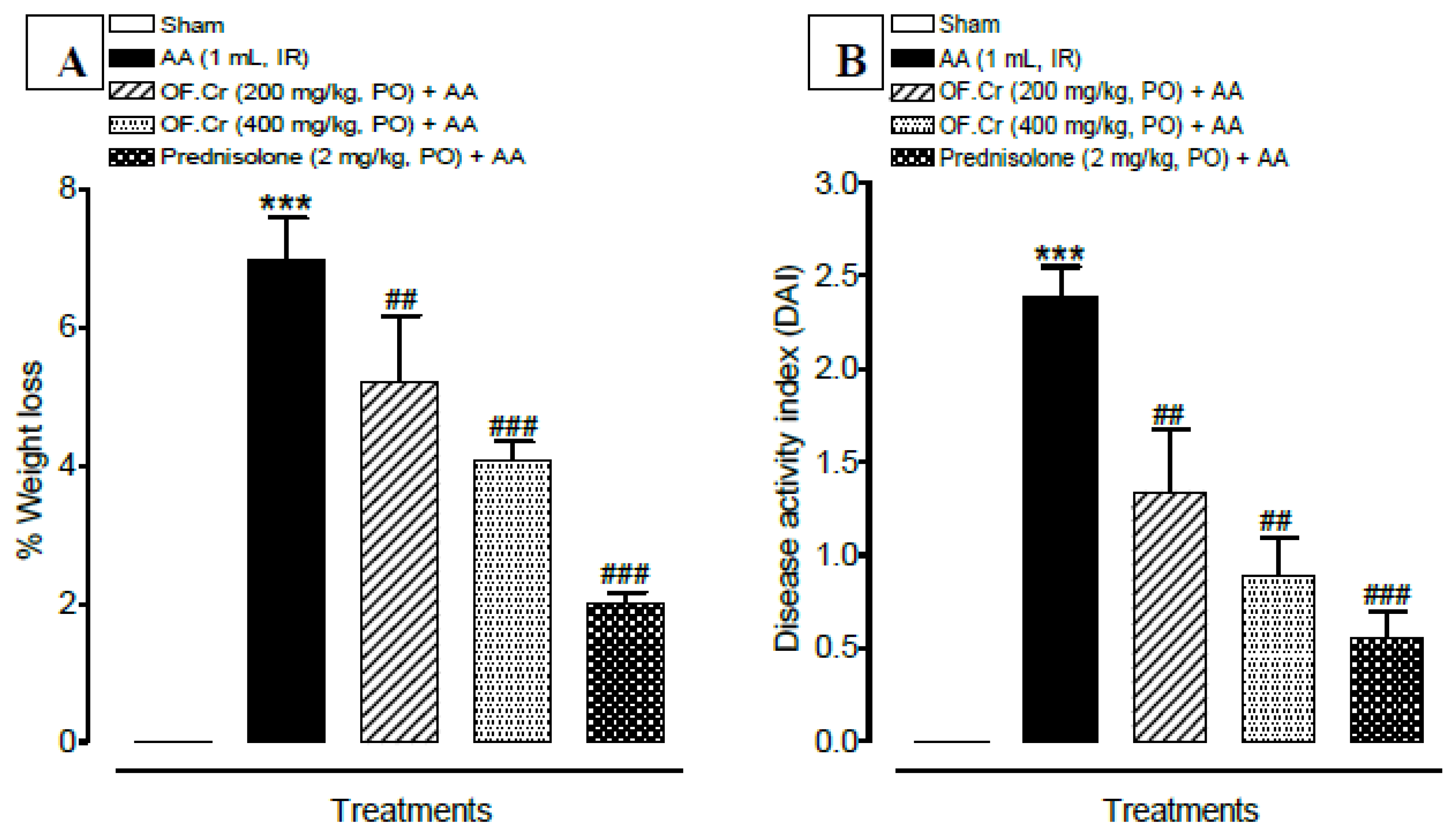
2.7. Assessment of Disease Activity Index (DAI)
2.8. Assessment of Macroscopic Damage
2.9. Preparation of Tissue Homogenate
2.10. Assessment of Lipid Peroxidation Activity
2.11. Assessment of Antioxidant Levels
2.12. Assessment of Cytokine Levels (IL-6 and TNFα)
2.13. Microscopic Assessment of UC
2.14. Statistical Analysis
3. Results
3.1. Effect of O. fruticosa Extract on the Disease Activity Index
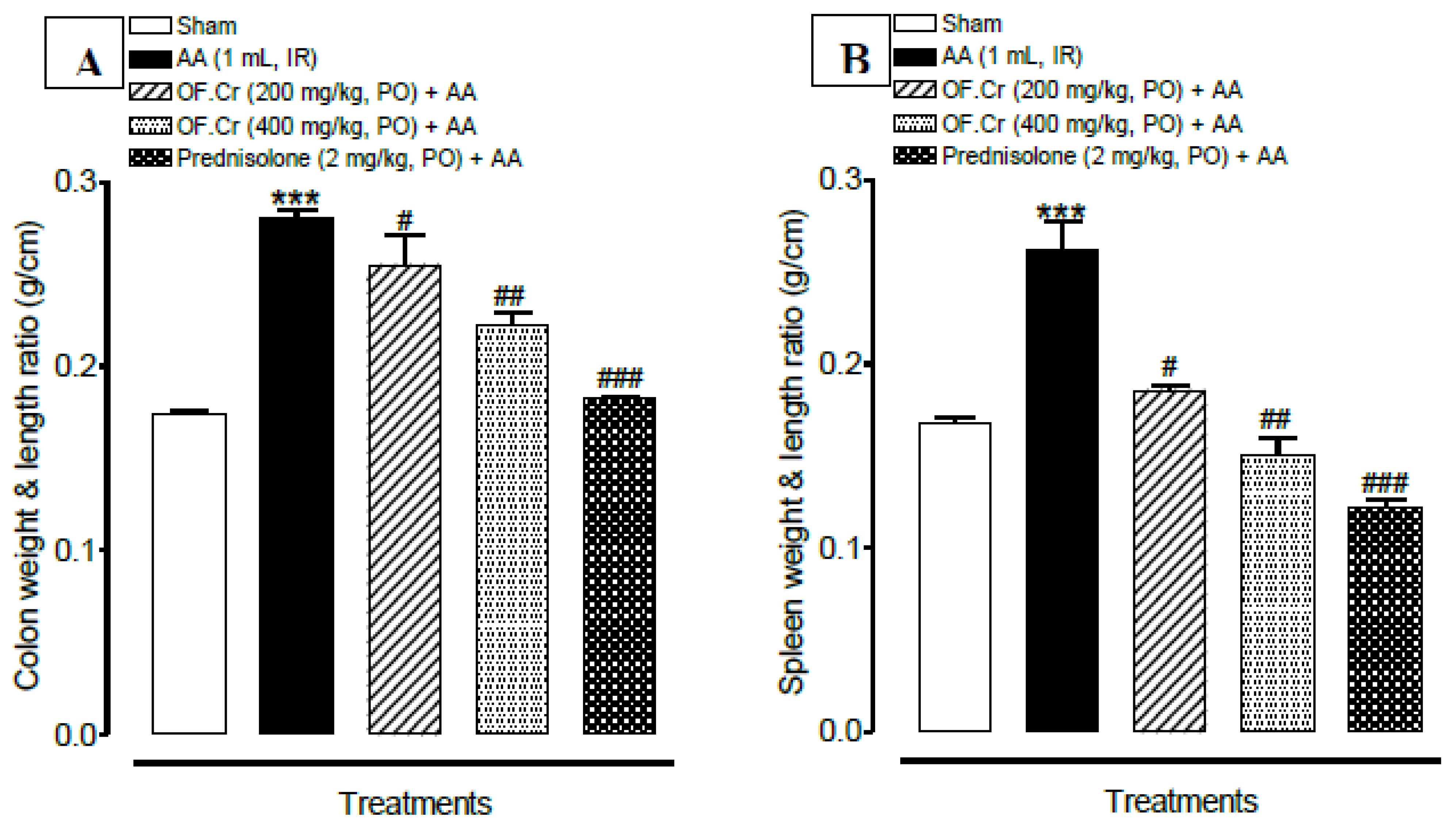
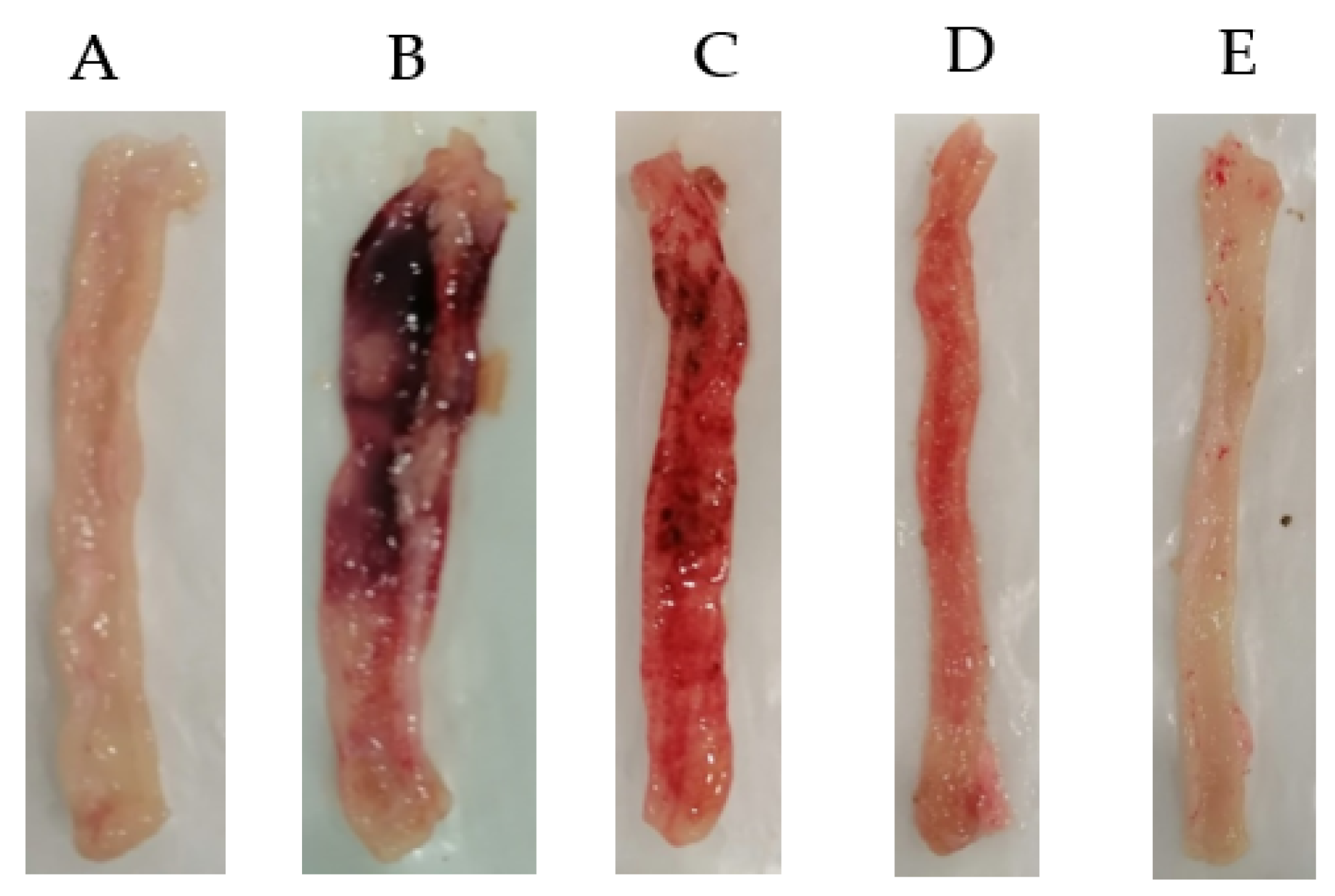
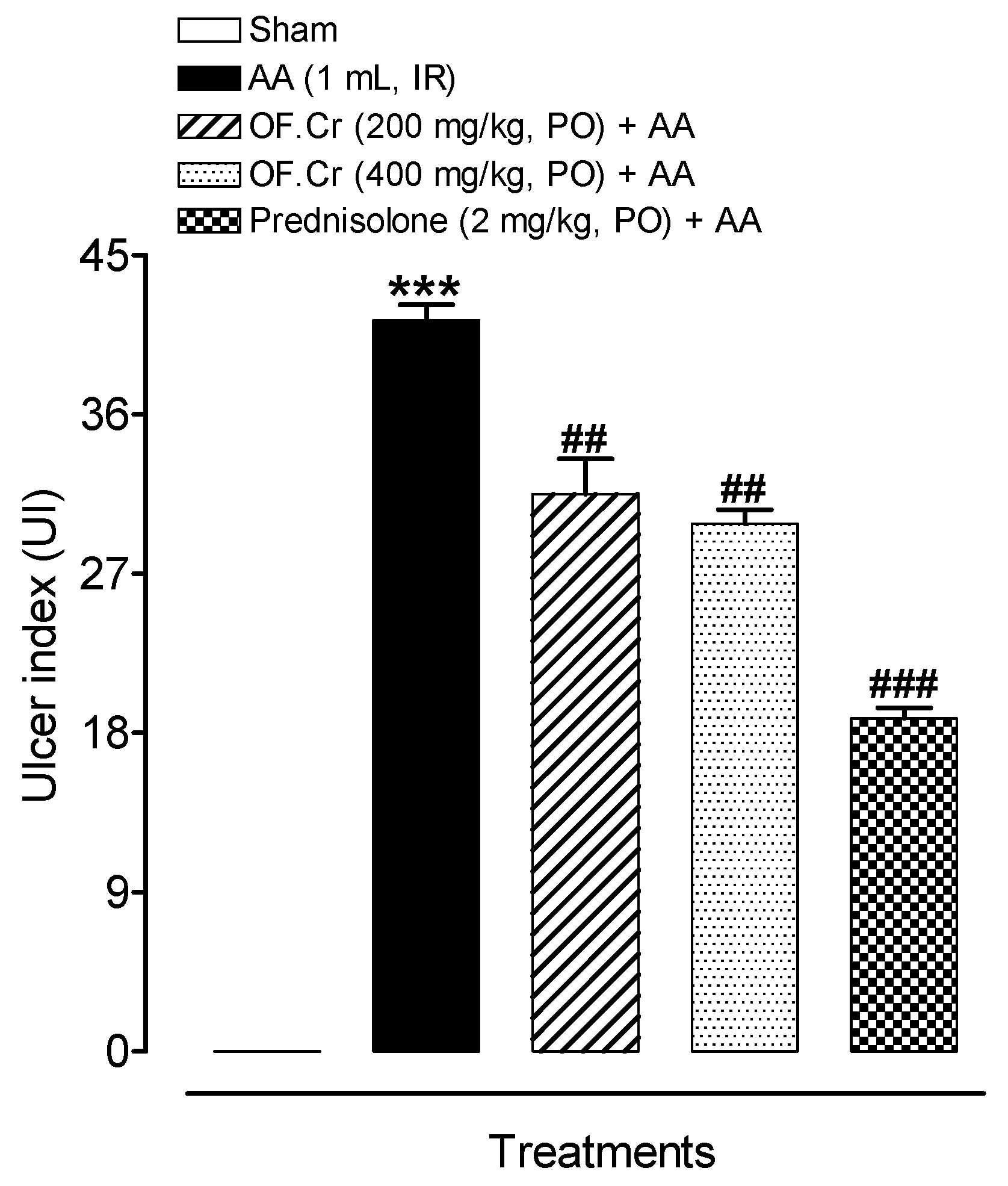
3.2. Effect of O. fruticosa Extract on Macroscopic Anatomy
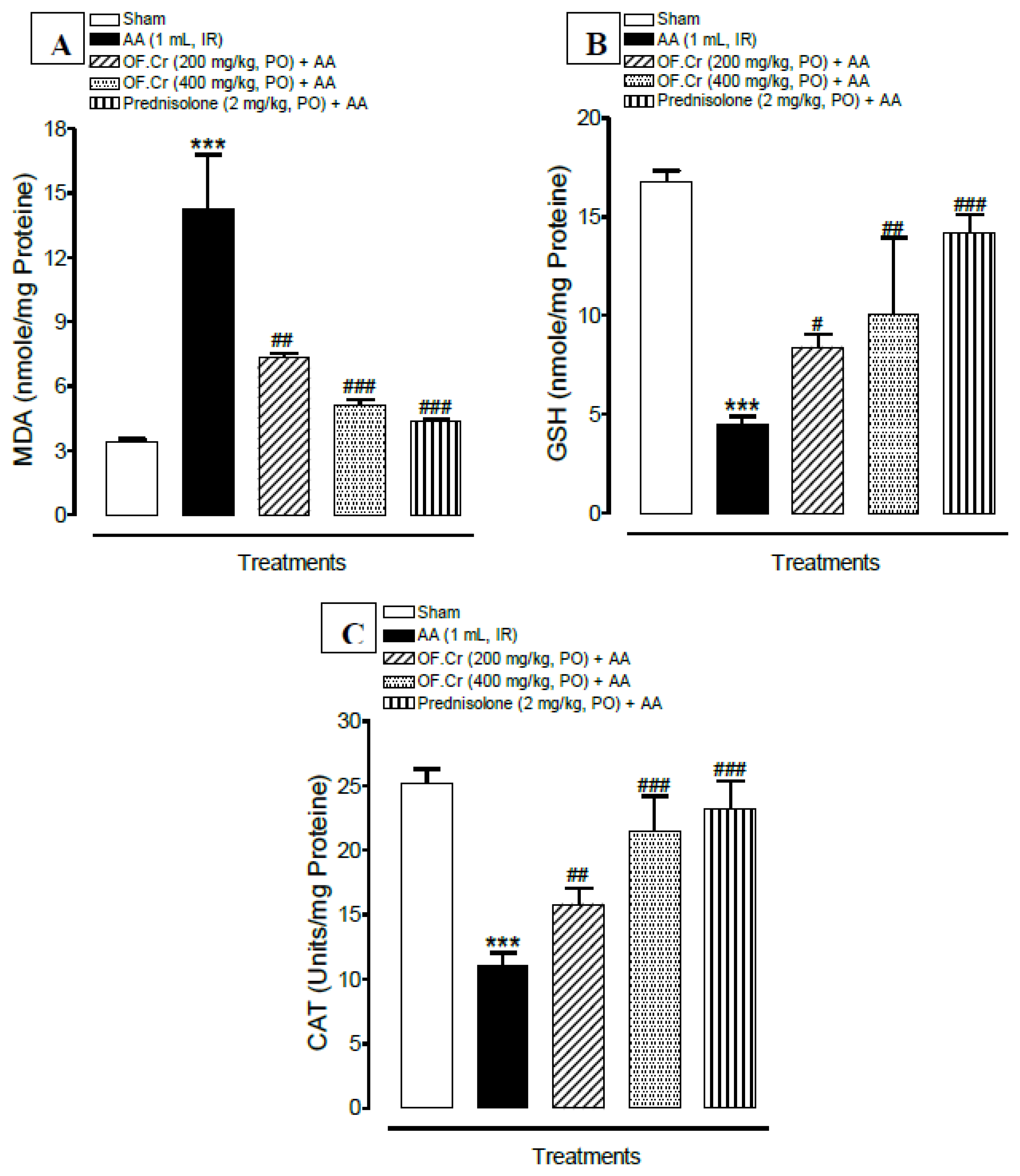
3.3. Effect of O. fruticosa Extract on Lipid Peroxidation
3.4. Effect of O. fruticosa Extract on Antioxidant Activity
3.5. Effect of O. fruticosa Extract on IL-6 and TNFα
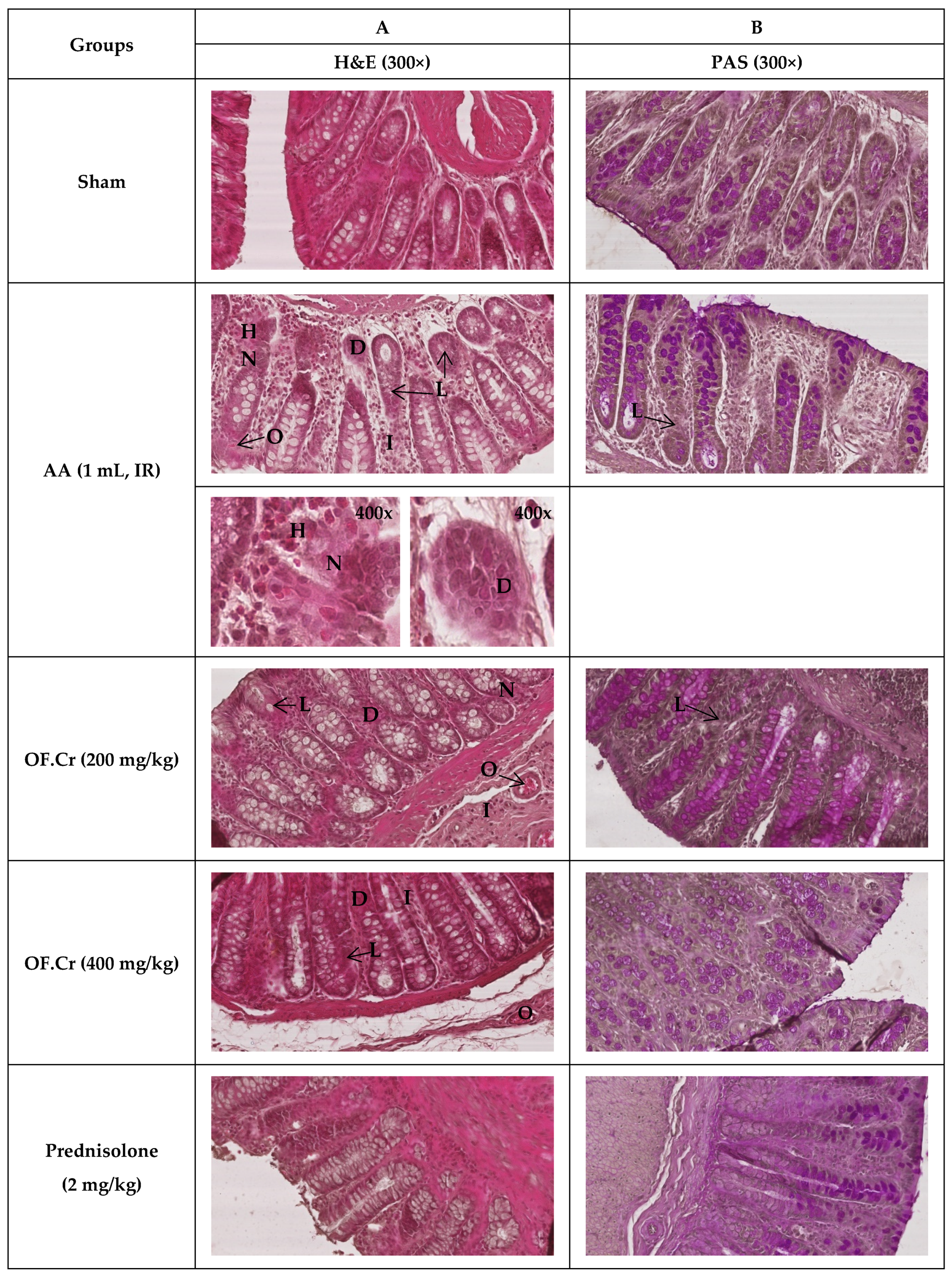
3.6. Effect of O. fruticosa Extract on Microscopic Damage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. European Crohn’s and Colitis Organisation [ECCO]. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: Definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J. Crohns. Colitis. 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Eisenstein, M. Ulcerative colitis: Towards remission. Nature 2018, 563, S33. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, P.; Mytton, J.; Evison, F.; Kamarajah, S.K.; Reece, J.; Iqbal, T.; Cooney, R.; Thompson, F.; Walmsley, M.; Ferguson, J.; et al. A nationwide population-based evaluation of mortality and cancer-risk in patients with ulcerative colitis/primary sclerosing cholangitis—young age at diagnosis and the unmet need to reduce mortality. J. Hepatol. 2018, 68, S220–S221. [Google Scholar] [CrossRef]
- Ooi, C.J.; Hilmi, I.; Banerjee, R.; Chuah, S.W.; Ng, S.C.; Wei, S.C.; Makharia, G.K.; Pisespongsa, P.; Chen, M.H.; Ran, Z.H.; et al. Best practices on immunomodulators and biologic agents for ulcerative colitis and Crohn’s disease in Asia. Intest. Res. 2019, 17, 285–310. [Google Scholar] [CrossRef] [PubMed]
- Mizoguchi, E.; Nguyen, D.; Low, D. Animal models of ulcerative colitis and their application in drug research. Drug Des. Devel. Ther. 2013, 7, 1341–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, X.; Zhang, H.; Li, W.; Wang, Y.; Mu, Q.; Wang, X.; He, Z.; Yao, H. Protective effect of cavidine on acetic acid-induced murine colitis via regulating antioxidant, cytokine profile and NF-κB signal transduction pathways. Chem. Biol. Interact. 2015, 239, 34–45. [Google Scholar] [CrossRef]
- Molodecky, N.A.; Kaplan, G.G. Environmental risk factors for inflammatory bowel disease. Gastroenterol. Hepatol. 2010, 6, 339–346. [Google Scholar]
- Yasukawa, K.; Hirago, A.; Yamada, K.; Tun, X.; Ohkuma, K.; Utsumi, H. In vivo redox imaging of dextran sodium sulfate-induced colitis in mice using Overhauser-enhanced magnetic resonance imaging. Free Radic. Biol. Med. 2019, 136, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sales-Campos, H.; Basso, P.J.; Alves, V.B.F.; Fonseca, M.T.C.; Bonfá, G.; Nardini, V.; Cardoso, C.R. Classical and recent advances in the treatment of inflammatory bowel diseases. Braz. J. Med. Biol. Res. 2015, 48, 96–107. [Google Scholar] [CrossRef]
- Jeong, D.Y.; Kim, S.; Son, M.J.; Son, C.Y.; Kim, J.Y. Kronbichler A Induction and maintenance treatment of inflammatory bowel disease: A comprehensive review. Autoimmun. Rev. 2019, 18, 439–454. [Google Scholar] [CrossRef]
- Ardizzone, S.; Cassinotti, A.; Manes, G.; Porro, G.B. Immunomodulators for all patients with inflammatory bowel disease? Therap. Adv. Gastroenterol. 2010, 3, 31–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oka, A.; Sartor, R.B. Microbial-based and microbial-targeted therapies for inflammatory bowel diseases. Dig. Dis. Sci. 2020, 65, 757–788. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.; Ma, Q.; Ye, L.; Piao, G. The traditional medicine and modern medicine from natural products. Molecules 2016, 21, 559. [Google Scholar] [CrossRef] [Green Version]
- Langmead, L.; Feakins, R.M.; Goldthorpe, S.; Holt, H.; Tsironi, E.; De Silva, A.; Jewell, D.P.; Rampton, D.S. Randomized, double-blind, placebo-controlled trial of oral aloe vera gel for active ulcerative colitis. Aliment. Pharmacol. Ther. 2004, 19, 739–747. [Google Scholar] [CrossRef]
- Zhou, Y.H.; Yu, J.P.; Liu, Y.F.; Teng, X.J.; Ming, M.; Lv, P.; An, P.; Liu, S.Q.; Yu, H.G. Effects of Ginkgo biloba extract on inflammatory mediators (SOD, MDA, TNF-alpha, NF-kappaBp65, IL-6) in TNBS-induced colitis in rats. Mediat. Inflamm. 2006, 2006, 92642. [Google Scholar] [CrossRef] [Green Version]
- Kudo, T.; Okamura, S.; Zhang, Y.; Masuo, T.; Mori, M. Topical application of glycyrrhizin preparation ameliorates experimentally induced colitis in rats. World J. Gastroenterol. 2011, 17, 2223–2228. [Google Scholar] [CrossRef] [PubMed]
- Langmead, L.; Rampton, D.S. Review article: Complementary and alternative therapies for inflammatory bowel disease. Aliment. Pharmacol. Ther. 2006, 23, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Iida, T.; Takeuchi, K.; Watanabe, F.; Maruyama, Y.; Andoh, A.; Tsujikawa, T.; Fujiyama, Y.; Mitsuyama, K.; Sata, M.; et al. Curcumin maintenance therapy for ulcerative colitis: Randomized, multicenter, double-blind, placebo-controlled trial. Clin. Gastroenterol. Hepatol. 2006, 4, 1502–1506. [Google Scholar] [CrossRef] [PubMed]
- El-Abhar, H.S.; Hammad, L.N.; Gawad, H.S. Modulating effect of ginger extract on rats with ulcerative colitis. J. Ethnopharmacol. 2008, 118, 367–372. [Google Scholar] [CrossRef]
- Mazzon, E.; Muià, C.; Paola, R.D.; Genovese, T.; Menegazzi, M.; De Sarro, A.; Suzuki, H.; Cuzzocrea, S. Green tea polyphenol extract attenuates colon injury induced by experimental colitis. Free Radic. Res. 2005, 39, 1017–1025. [Google Scholar] [CrossRef]
- Enyew, A.; Asfaw, Z.; Kelbessa, E.; Nagappan, R. Status of medico-cultural commercial plants at Fiche town market Ethiopia. Int. J. Pharm. Health Care Res. 2013, 1, 227–236. [Google Scholar]
- Getaneh, S.; Girma, Z. An ethnobotanical study of medicinal plants in Debre Libanos Wereda, Central Ethiopia. Afr. J. Plant Sci. 2014, 8, 366–379. [Google Scholar] [CrossRef] [Green Version]
- D’avigdor, E.; Wohlmuth, H.; Asfaw, Z.; Awas, T. The current status of knowledge of herbal medicine and medicinal plants in Fiche, Ethiopia. J. Ethnobiol. Ethnomed. 2014, 10. [Google Scholar] [CrossRef] [Green Version]
- Andemariam, W.S. Legislative regulation of traditional medicinal knowledge in Eritrea vis-à-vis Eritrea’s commitments under the convention on biological diversity: Issues and alternatives. Law Environ. Dev. J. 2010, 6, 130–162. [Google Scholar]
- Rahman, M.A.; Mossa, J.S.; Al-Said, M.S.; Al-Yahya, M.A. Medicinal plant diversity in the flora of Saudi Arabia: A report on seven plant families. Fitoterapia 2004, 75, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.N.; Rehman, N.U.; Karim, A.; Bahta, T.; Abujheisha, K.Y.; Ahamad, S.R.; Imam, F. Evaluation of Bronchodilator and antimicrobial activities of Otostegia fruticose: A multi-mechanistic approach. Saudi Pharm. J. 2020, 28, 281–289. [Google Scholar] [CrossRef]
- Bahta, T.; Karim, A.; Periasamy, G.; Gebremedhin, G.; Ur-Rehman, N.; Bitew, H.; Hagazi, K. Analgesic, Anti-inflammatory and In-vitro Hyaluronidase Inhibitory Properties of the Leaf Extract and Solvent Fractions of Otostegia Fruticosa (Forssk.) Schweinf. ex Penzig. Iran. J. Pharm. Res. 2020, 19, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Meragiaw, M.; Asfaw, Z.; Argaw, M. The Status of Ethnobotanical Knowledge of Medicinal Plants and the Impacts of Resettlement in Delanta, Northwestern Wello, Northern Ethiopia. Evid. Based Complement. Alternat. Med. 2016, 2016, 5060247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mothana, R.A.A.; Kriegisch, S.; Harms, M.; Wende, K.; Lindequist, U. Assessment of selected Yemeni medicinal plants for their in vitro antimicrobial, anticancer, and antioxidant activities. Pharm. Biol. 2011, 49, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Al-Jumayi, H.A.R.O. Amelioration of gentamicin-induced nephrotoxicity using essential oil extract from Otostegia fruticosa leaves in albino rats. Plant Cell Biotechnol. Mol. Biol. 2020, 21, 90–106. [Google Scholar]
- National Research Council. Guide for the Care and Use of Laboratory Animals; National Academy Press: Washington, DC, USA, 1996; pp. 1–7. [Google Scholar]
- Organization for Economic Cooperation and Development. The OECD 423 Guideline for Testing of Chemicals Acute Oral Toxicity; Organization for Economic Co-operation and Development: Paris, France, 2001. [Google Scholar]
- MacPherson, B.R.; Pfeiffer, C.J. Experimental production of diffuse colitis in rats. Digestion 1978, 17, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, S.; Popp, V.; Kindermann, M.; Gerlach, K.; Weigmann, B.; Fichtner-Feigl, S.; Neurath, M.F. Chemically induced mouse models of intestinal inflammation. Nat. Protoc. 2017, 12, 1295–1309. [Google Scholar] [CrossRef] [PubMed]
- Palla, A.H.; Iqbal, N.T.; Minhas, K.; Gilani, A.H. Flaxseed extract exhibits mucosal protective effect in acetic acid induced colitis in mice by modulating cytokines, antioxidant and antiinflammatory mechanisms. Int. Immunopharmacol. 2016, 38, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.P.; Beck, P.L.; Herridge, M.S.; Depew, W.T.; Szewczuk, M.R.; Wallace, J.L. Hapten-induced model of chronic inflammation and ulceration in the rat colon. Gastroenterology 1989, 96, 795–803. [Google Scholar] [CrossRef]
- Imam, F.; Al-Harbi, N.O.; Al-Harbi, M.M.; Ansari, M.A.; Almutairi, M.M.; Alshammari, M.; Almukhlafi, T.S.; Ansari, M.N.; Aljerian, K.; Ahmad, S.F. Apremilast reversed carfilzomib-induced cardiotoxicity through inhibition of oxidative stress, NF-κB and MAPK signaling in rats. Toxicol. Mech. Methods 2016, 26, 700–708. [Google Scholar] [CrossRef]
- Esterbauer, H.; Cheeseman, K.H. Determination of aldehydic lipid peroxidation products: Malonaldehyde and 4-hydroxynonenal. Methods Enzymol. 1990, 186, 407–421. [Google Scholar] [CrossRef]
- Jollow, D.J.; Mitchell, J.R.; Zampaglione, N.; Gillette, J.R. Bromobenzene induced liver necrosis: Protective role of glutathione and evidence for 3,4-bromobenzene as the hepatic metabolite. Pharmacology 1974, 11, 151–169. [Google Scholar] [CrossRef]
- Claiborne, A.L. Assay of catalase. In Handbook of Methods of Oxygen Radical Research; Greenwald, R.A., Ed.; CRC Press: Boca Raton, FL, USA, 1985; pp. 283–285. [Google Scholar]
- Neurath, M.F.; Fuss, I.; Kelsall, B.L.; Stüber, E.; Strober, W. Antibodies to interleukin-12 abrogate established experimental colitis in mice. J. Exp. Med. 1995, 182, 1281–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiela, P.R.; Midura, A.J.; Kuscuoglu, N.; Jolad, S.D.; Sólyom, A.M.; Besselsen, D.G.; Timmermann, B.N.; Ghishan, F.K. Effects of Boswellia serrata in mouse models of chemically induced colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2005, 288, G798–G808. [Google Scholar] [CrossRef] [Green Version]
- Dorofeyev, A.E.; Vasilenko, I.V.; Rassokhina, O.A.; Kondratiuk, R.B. Mucosal barrier in ulcerative colitis and Crohn’s disease. Gastroenterol. Res. Pract. 2013, 2013, 431231. [Google Scholar] [CrossRef] [PubMed]
- Soliman, G.A.; Gabr, G.A.; Al-Saikhan, F.I.; Ansari, M.N.; Khan, T.H.; Ganaie, M.A.; Abdulaziz, S.S.; Alankus-Calıskan, Ö. Protective effects of two Astragalus species on ulcerative colitis in rats. Trop. J. Pharm. Res. 2016, 15, 2155–2163. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez–Rey, E.; Chorny, A.; Delgado, M. Terapeutic action of ghrelin in a mouse model of colitis. Gastroenterology 2006, 130, 1707–1720. [Google Scholar] [CrossRef] [PubMed]
- Hunschede, S.; Kubant, R.; Akilen, R.; Thomas, S.; Anderson, G.H. Decreased appetite after high-intensity exercise correlates with increased plasma interleukin-6 in normal-weight and overweight/obese boys. Curr. Dev. Nutr. 2017, 1, e000398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harputluoglu, M.M.; Demirel, U.; Yücel, N.; Karadağ, N.; Temel, I.; Firat, S.; Ara, C.; Aladağ, M.; Karincaoğlu, M.; Hilmioğlu, F. The effects of Gingko biloba extract on acetic acid-induced colitis in rats. Turk. J. Gastroenterol. 2006, 17, 177–182. [Google Scholar] [PubMed]
- Bhattacharyya, A.; Chattopadhyay, R.; Mitra, S.; Crowe, S.E. Oxidative stress: An essential factor in the pathogenesis of gastrointestinal mucosal diseases. Physiol. Rev. 2014, 94, 329–354. [Google Scholar] [CrossRef] [Green Version]
- Baumgart, D.C.; Carding, S.R. Inflammatory bowel disease: Cause and immunobiology. Lancet 2007, 369, 1627–1640. [Google Scholar] [CrossRef]
- Ran, Z.H.; Chen, C.; Xiao, S.D. Epigallocatechin-3-gallate ameliorates rats colitis induced by acetic acid. Biomed. Pharmacother. 2008, 62, 189–196. [Google Scholar] [CrossRef]
- Nakhai, L.A.; Mohammadirad, A.; Yasa, N.; Minaie, B.; Nikfar, S.; Ghazanfari, G.; Zamani, M.J.; Dehghan, G.; Jamshidi, H.; Boushehri, V.S.; et al. Benefits of zataria multiflora boiss in experimental model of mouse inflammatory bowel disease. Evid. Based Complement. Alternat. Med. 2007, 4, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Fournier, B.M.; Parkos, C.A. The role of neutrophils during intestinal inflammation. Mucosal Immunol. 2012, 5, 354–366. [Google Scholar] [CrossRef]
- Murch, S.H.; Lamkin, V.A.; Savage, M.O.; Walker-Smith, J.A.; MacDonald, T.T. Serum concentrations of tumour necrosis factor alpha in childhood chronic infl ammatory bowel disease. Gut 1991, 32, 913–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braegger, C.P.; Nicholls, S.; Murch, S.H.; Stephens, S.; MacDonald, T.T. Tumour necrosis factor alpha in stool as a marker of intestinal infl ammation. Lancet 1992, 339, 89–91. [Google Scholar] [CrossRef]
- Neurath, M.F. Cytokines in inflammatory bowel disease. Nat. Rev. Immunol. 2014, 14, 329–342. [Google Scholar] [CrossRef]
- Xavier, R.J.; Podolsky, D.K. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007, 448, 427–434. [Google Scholar] [CrossRef]
- Fawzy, S.A.; Abo-Elnou, R.K.E.D.; el-Deeb, D.F.A.E.M.; Abd-Elkader, M.M.Y. The possible role of mesenchymal stem cells therapy in the repair of experimentally induced colitis in male albino rats. Int. J. Stem. Cells 2013, 6, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Bertevello, P.L.; Logullo, Ã.F.; Nonogaki, S.; Campos, F.M.; Chiferi, V.; Alves, C.C.; Torrinhas, R.S.; Gama-Rodrigues, J.J.; Waitzberg, D.L. Immunohistochemical assessment of mucosal cytokine profile in acetic acid experimental colitis. Clinics 2005, 60, 277–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.; Levenson, C.; Bell, R.H.; Anderson, S.A.; Hudson, J.B.; Collins, C.C.; Cox, M.E. Suppression of lipopolysaccharide-stimulated cytokine/chemokine production in skin cells by sandalwood oils and purified alpha-santalol and beta-santalol. Phytother. Res. 2014, 28, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Lenfeld, J.; Motl, O.; Trka, A. Anti-inflammatory activity of extracts from Conyza canadensis. Die Pharm. 1986, 41, 268–269. [Google Scholar] [PubMed]
- Singh, G.; Kapoor, I.P.; Singh, P.; de Heluani, C.S.; de Lampasona, M.P.; Catalan, C.A. Comparative study of chemical composition and antioxidant activity of fresh and dry rhizomes of turmeric (Curcuma longa Linn.). Food Chem. Toxicol. 2010, 48, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, Y.H.; Kim, Y.; Lee, S.J. Aromatic-turmerone attenuates invasion and expression of MMP-9 and COX-2 through inhibition of NF-kappaB activation in TPA-induced breast cancer cells. J. Cell Biochem. 2012, 113, 3653–3662. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Lu, B.; Lü, C.; Bai, Q.; Yan, D.; Wu, Y.; Hong, Z.; Xu, H. Solanesol induces the expression of hemeoxygenase-1 via p38 and Akt and suppresses the production of proinflammatory cytokines in RAW264.7cells. Food Funct. 2017, 8, 132–141. [Google Scholar] [CrossRef]
- Pichersky, E.; Raguso, R.A. Why do plants produce so many terpenoid compounds? New Phytol. 2018, 220, 692–702. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Neurath Score (Maximum Score = 4) | Kiela Score (Maximum Score = 3) | Mucin Score (Maximum Score = 3) |
|---|---|---|---|
| AA | 3.75 | 2.75 | 1.25 |
| OF.Cr (200 mg/kg) | 2.75 | 2.25 | 2.00 |
| OF.Cr (400 mg/kg) | 1.75 ** | 2.00 * | 2.00 |
| Prednisolone (2 mg/kg) | 1.25 *** | 1.00 *** | 2.75 *** |
| KW p value | 0.0004 | 0.0007 | 0.0029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansari, M.N.; Rehman, N.U.; Karim, A.; Soliman, G.A.; Ganaie, M.A.; Raish, M.; Hamad, A.M. Role of Oxidative Stress and Inflammatory Cytokines (TNF-α and IL-6) in Acetic Acid-Induced Ulcerative Colitis in Rats: Ameliorated by Otostegia fruticosa. Life 2021, 11, 195. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030195
Ansari MN, Rehman NU, Karim A, Soliman GA, Ganaie MA, Raish M, Hamad AM. Role of Oxidative Stress and Inflammatory Cytokines (TNF-α and IL-6) in Acetic Acid-Induced Ulcerative Colitis in Rats: Ameliorated by Otostegia fruticosa. Life. 2021; 11(3):195. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030195
Chicago/Turabian StyleAnsari, Mohd Nazam, Najeeb Ur Rehman, Aman Karim, Gamal A. Soliman, Majid A. Ganaie, Mohammad Raish, and Abubaker M. Hamad. 2021. "Role of Oxidative Stress and Inflammatory Cytokines (TNF-α and IL-6) in Acetic Acid-Induced Ulcerative Colitis in Rats: Ameliorated by Otostegia fruticosa" Life 11, no. 3: 195. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030195