
Long-Term Survival and Value of 18F-FDG PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors Treated with Second Peptide Receptor Radionuclide Therapy Course with 177Lu-DOTATATE

Abstract
:1. Introduction
2. Results
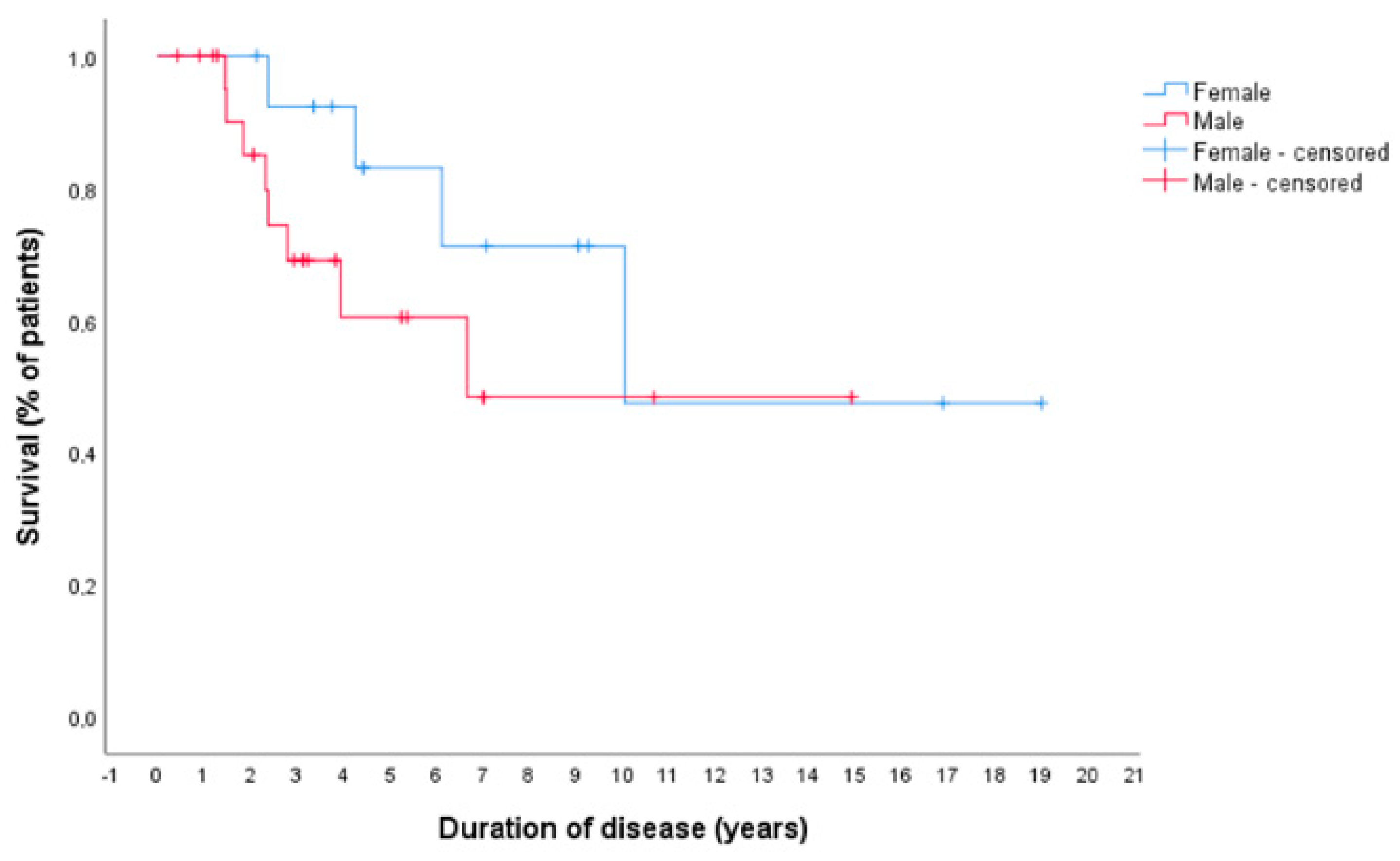
2.1. Survival
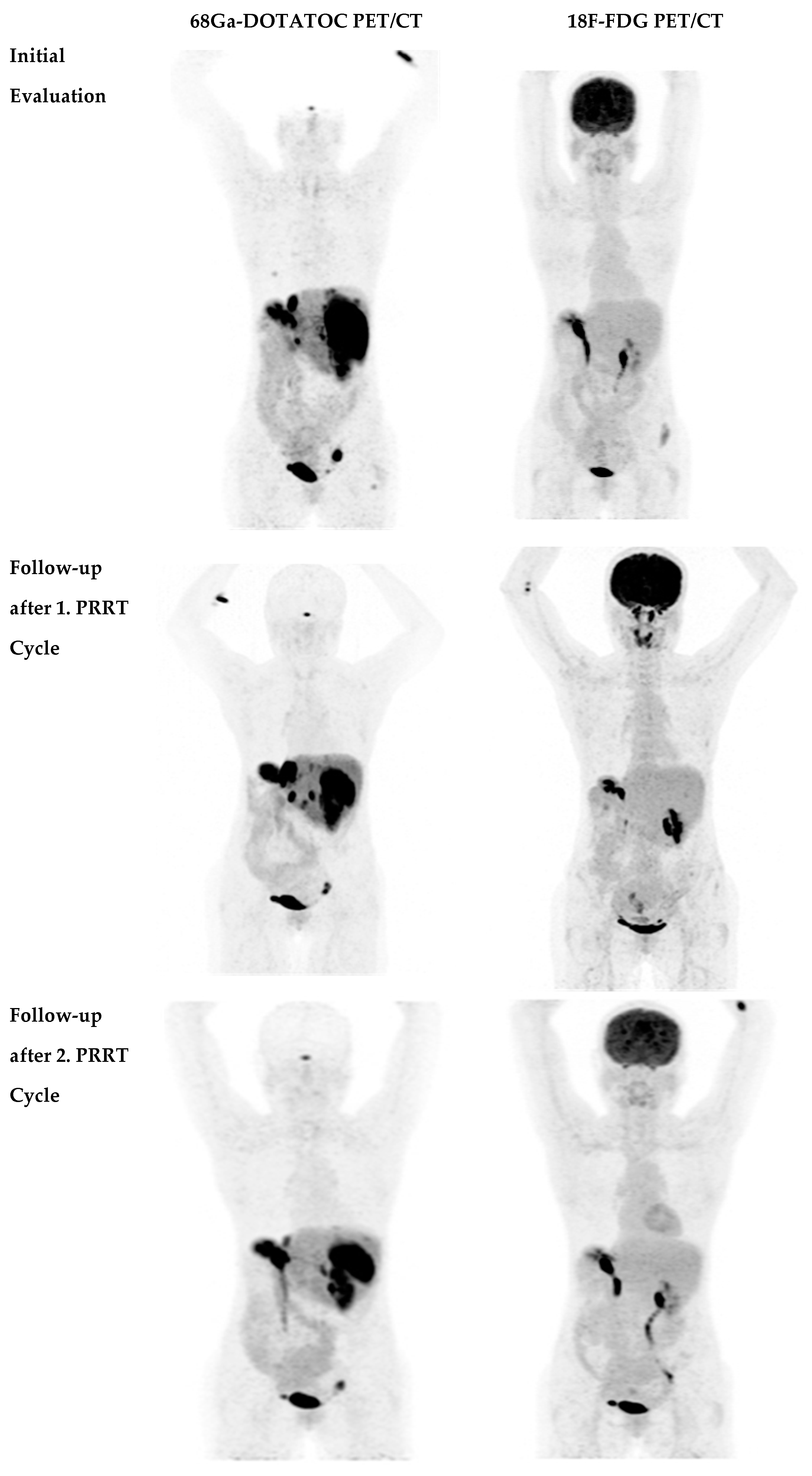
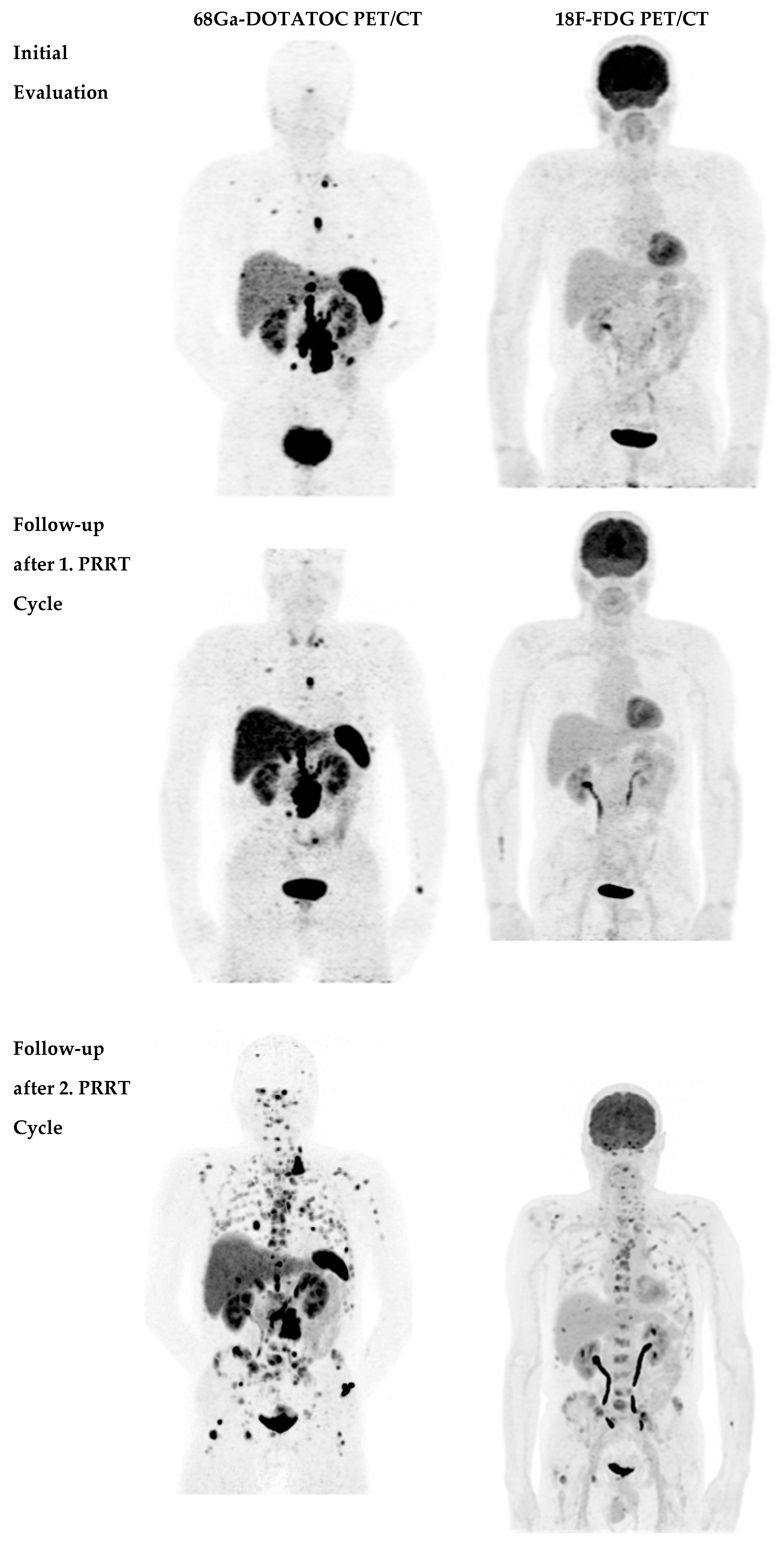
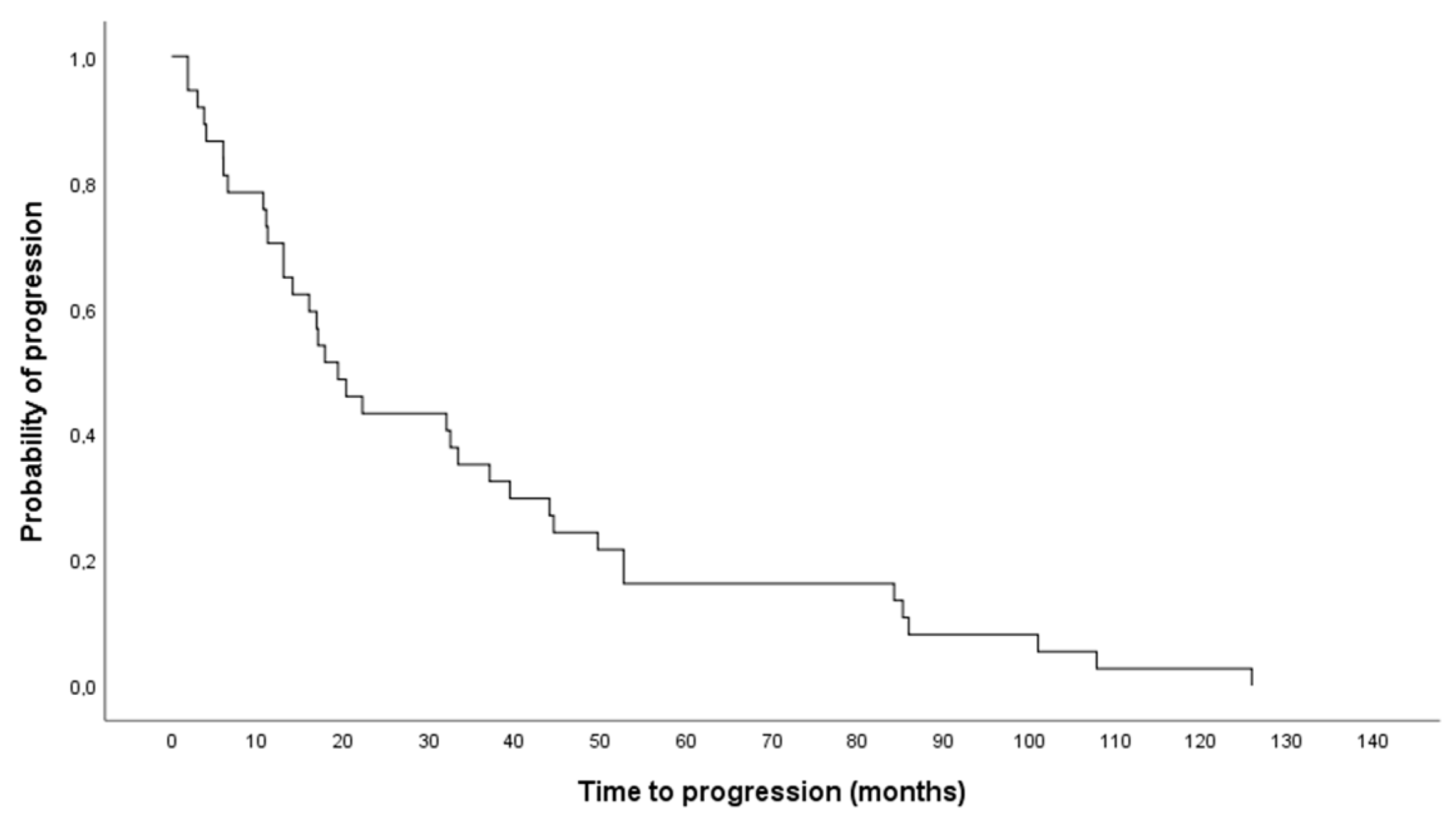
2.2. Disease Course after Second PRRT Course
2.3. 18F-FDG Uptake Status Related to Survival
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Peptide Receptor Radionuclide Therapy (PRRT) Regimen
4.3. Positron Emission Tomography (PET)
4.3.1. 68Ga-DOTA-TOC
4.3.2. 18F-FDG
4.3.3. CT
4.3.4. Image Review
4.3.5. Statistical Data Analysis and Data Collection
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Reubi, J.C. Peptide Receptors as Molecular Targets for Cancer Diagnosis and Therapy. Endocr. Rev. 2003, 24, 389–427. [Google Scholar] [CrossRef] [Green Version]
- Reubi, J.C.; Schär, J.-C.; Waser, B.; Wenger, S.; Heppeler, A.; Schmitt, J.S.; Mäcke, H.R. Affinity profiles for human somatostatin receptor subtypes SST1-SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. Eur. J. Nucl. Med. Mol. Imaging 2000, 27, 273–282. [Google Scholar] [CrossRef]
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Fave, G.D.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, M.K.; Carneiro, F.; Cree, I.A. The WHO Classification of Tumours Editorial Board The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, M.; Breeman, W.A.; Kwekkeboom, D.J.; Valkema, R.; Krenning, E.P. Tumor imaging and therapy using radiolabeled somatostatin analogues. Acc. Chem. Res. 2009, 42, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Ramage, J.K.; Ahmed, A.; Ardill, J.; Bax, N.; Breen, D.J.; Caplin, M.E.; Corrie, P.; Davar, J.; Davies, A.H.; Lewington, V.; et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut 2011, 61, 6–32. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; Von Guggenberg, E.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-Octreotide PET in Neuroendocrine Tumors: Comparison with Somatostatin Receptor Scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Putzer, D.; Gabriel, M.; Henninger, B.; Kendler, D.; Uprimny, C.; Dobrozemsky, G.; Decristoforo, C.; Bale, R.J.; Jaschke, W.; Virgolini, I.J. Bone Metastases in Patients with Neuroendocrine Tumor: 68Ga-DOTA-Tyr3-Octreotide PET in Comparison to CT and Bone Scintigraphy. J. Nucl. Med. 2009, 50, 1214–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilica, B.; Waitz, D.; Stevanovic, V.; Uprimny, C.; Kendler, D.; Buxbaum, S.; Warwitz, B.; Gerardo, L.; Henninger, B.; Virgolini, I.; et al. Direct comparison of 68Ga-DOTA-TOC and 18F-FDG PET/CT in the follow-up of patients with neuroendocrine tumour treated with the first full peptide receptor radionuclide therapy cycle. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1585–1592. [Google Scholar] [CrossRef] [Green Version]
- Kwee, T.C.; Basu, S.; Saboury, B.; Ambrosini, V.; Torigian, E.A.; Alavi, A. A new dimension of FDG-PET interpretation: Assessment of tumor biology. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1158–1170. [Google Scholar] [CrossRef]
- Kayani, I.; Bomanji, J.B.; Groves, A.; Conway, G.; Gacinovic, S.; Win, T.; Dickson, J.; Caplin, M.; Ell, P.J. Functional imaging of neuroendocrine tumors with combined PET/CT using68Ga-DOTATATE (DOTA-DPhe1,Tyr3-octreotate) and18F-FDG. Cancer 2008, 112, 2447–2455. [Google Scholar] [CrossRef]
- Adams, S.; Baum, R.; Rink, T.; Schumm-Dräger, P.-M.; Usadel, K.-H.; Hör, G. Limited value of fluorine-18 fluorodeoxyglucose positron emission tomography for the imaging of neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 1997, 25, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Binderup, T.; Knigge, U.; Loft, A.; Federspiel, B.; Kjaer, A. 18F-Fluorodeoxyglucose Positron Emission Tomography Predicts Survival of Patients with Neuroendocrine Tumors. Clin. Cancer Res. 2010, 16, 978–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, M.; Andergassen, U.; Putzer, D.; Kroiss, A.; Waitz, D.; Von Guggenberg, E.; Kendler, D.; Virgolini, I.J. Individualized peptide-related-radionuclide-therapy concept using different radiolabelled somatostatin analogs in advanced cancer patients. Q. J. Nucl. Med. Mol. Imaging 2010, 54, 92–99. [Google Scholar] [PubMed]
- Kwekkeboom, D.J.; de Herder, W.W.; Kam, B.L.; van Eijck, C.H.; van Essen, M.; Kooij, P.P.; Feelders, R.A.; van Aken, M.O.; Krenning, E.P. Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: Toxicity, efficacy, and survival. J. Clin. Oncol. 2008, 26, 2124–2130. [Google Scholar] [CrossRef] [Green Version]
- Oberg, K.; Knigge, U.; Kwekkeboom, D.J.; Perren, A. Neuroendocrine gastro-entero-pancreatic tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23, vii124–vii130. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Prasad, V.; Lee, D.S.; Baum, R.P. Effect of Peptide Receptor Radionuclide Therapy on Somatostatin Receptor Status and Glucose Metabolism in Neuroendocrine Tumors: Intraindividual Comparison of Ga-68 DOTANOC PET/CT and F-18 FDG PET/CT. Int. J. Mol. Imaging 2011, 2011, 1–7. [Google Scholar] [CrossRef]
- Gabriel, M.; Nilica, B.; Kaiser, B.; Virgolini, I.J. Twelve-Year Follow-up After Peptide Receptor Radionuclide Therapy. J. Nucl. Med. 2018, 60, 524–529. [Google Scholar] [CrossRef] [Green Version]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Brabander, T.; Van Der Zwan, W.A.; Teunissen, J.J.; Kam, B.L.; Feelders, R.A.; De Herder, W.W.; Van Eijck, C.H.; Franssen, G.J.; Krenning, E.P.; Kwekkeboom, D.J. Long-Term Efficacy, Survival, and Safety of [177Lu-DOTA0,Tyr3]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin. Cancer Res. 2017, 23, 4617–4624. [Google Scholar] [CrossRef] [Green Version]
- Cwikla, J.B.; Sankowski, A.; Seklecka, N.; Buscombe, J.R.; Nasierowska-Guttmejer, A.; Jeziorski, K.G.; Mikolajczak, R.; Pawlak, D.; Stepien, K.; Walecki, J. Efficacy of radionuclide treatment DOTATATE Y-90 in patients with progressive metastatic gastroenteropancreatic neuroendocrine carcinomas (GEP-NETs): A phase II study. Ann. Oncol. 2009, 21, 787–794. [Google Scholar] [CrossRef]
- Vaughan, E.; Machta, J.; Walker, M.; Toumpanakis, C.; Caplin, M.; Navalkissoor, S. Retreatment with peptide receptor radionuclide therapy in patients with progressing neuroendocrine tumours: Efficacy and prognostic factors for response. Br. J. Radiol. 2018, 91, 20180041. [Google Scholar] [CrossRef]
- Hallet, J.; Law, C.H.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising. incidence of neuroendocrine tumors: A population-based analysis of epidemiology,. metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, Q.; Singh, A.; Schuchardt, C.; Kulkarni, H.R.; Baum, R.P. Prognostic Value of (18)F-FDG PET/CT in a large cohort of 495 patients with advanced metastatic neuroendocrine neoplasms (NEN) treated with peptide receptor radionuclide therapy (PRRT). J. Nucl. Med. 2020, 61, 1560–1569. [Google Scholar] [CrossRef]
- Pavel, M.; Baudin, E.; Couvelard, A.; Krenning, E.; Öberg, K.; Steinmüller, T.; Anlauf, M.; Wiedenmann, B.; Salazar, R. ENETS Consensus Guidelines for the Management of Patients with Liver and Other Distant Metastases from Neuroendocrine Neoplasms of Foregut, Midgut, Hindgut, and Unknown Primary. Neuroendocr 2012, 95, 157–176. [Google Scholar] [CrossRef] [PubMed]
- Heetfeld, M.; Chougnet, C.N.; Olsen, I.H.; Rinke, A.; Borbath, I.; Crespo, G.; Barriuso, J.; Pavel, M.; O’Toole, D.; Walter, T. Characteristics and treatment of patients with G3 gastroenteropancreatic neuroendocrine neoplasms. Endocr. Relat. Cancer 2015, 22, 657–664. [Google Scholar] [CrossRef] [Green Version]
- Raj, N.; Valentino, E.; Capanu, M.; Tang, L.H.; Basturk, O.; Untch, B.R. Treatment response and outcomes of grade 3 pancreatic neuroendocrine neoplasms based on morphology: Well differentiated versus poorly differentiated. Pancreas 2017, 46, 296–301. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Oberauer, A.; Dobrozemsky, G.; Decristoforo, C.; Putzer, D.; Kendler, D.; Uprimny, C.; Kovacs, P.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-Octreotide PET for Assessing Response to Somatostatin-Receptor-Mediated Radionuclide Therapy. J. Nucl. Med. 2009, 50, 1427–1434. [Google Scholar] [CrossRef] [Green Version]
- Sorbye, H.; Kong, G.; Grozinsky-Glasberg, S. PRRT in high-grade gastroenteropancreatic neuroendocrine neoplasms (WHO G3). Endocr. Relat. Cancer 2020, 27, R67–R77. [Google Scholar] [CrossRef]
- Moertel, C.G.; Kvols, L.K.; O’Connell, M.J.; Rubin, J. Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin. Evidence of major therapeutic activity in the anaplastic variants of these neoplasms. Cancer 1991, 68, 227–232. [Google Scholar] [CrossRef]
- Decristoforo, C.; Knopp, R.; Von Guggenberg, E.; Rupprich, M.; Dreger, T.; Hess, A.; Virgolini, I.; Haubner, R. A fully automated synthesis for the preparation of 68Ga-labelled peptides. Nucl. Med. Commun. 2007, 28, 870–875. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Partial Remission | Stable Disease | Progressive Disease | Total | ||
|---|---|---|---|---|---|
| Sex | Female | 0 | 7 | 7 | 14 |
| Male | 2 | 14 | 10 | 26 | |
| Total | 2 | 21 | 17 | 40 |
| Before PRRT | After First PRRT Course | After Second PRRT Course | |
|---|---|---|---|
| Negative | 33 | 30 | 26 |
| Positive | 7 | 10 | 14 |
| Total | 40 | 40 | 40 |
| Characteristic | Number (n) | Percentage (%) |
|---|---|---|
| Total number of patients | 40 | |
| Age at initial diagnosis (years) Mean ± standard deviation Range | 54.63 ± 12.85 29–83 | |
| Gender Male Female | 26 14 | 65.0 35.0 |
| Primary tumor site Pancreas Stomach Small bowel Colon Rectum | 18 2 18 1 1 | 45.0 5.0 45.0 2.5 2.5 |
| Sites of metastases Liver Lymph nodes Bone Lung Peritoneum Small bowel Spleen Suprarenal gland | 36 15 7 1 6 1 2 1 | 90.0 37.5 17.5 2.5 15.0 2.5 5.0 2.5 |
| Grade 1 2 3 Unknown | 2 29 8 1 | 5.0 72.5 20.0 2.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, M.; Winkler, K.-K.; Svirydenka, H.; Nilica, B.; Uprimny, C.; Virgolini, I. Long-Term Survival and Value of 18F-FDG PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors Treated with Second Peptide Receptor Radionuclide Therapy Course with 177Lu-DOTATATE. Life 2021, 11, 198. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030198
Rodrigues M, Winkler K-K, Svirydenka H, Nilica B, Uprimny C, Virgolini I. Long-Term Survival and Value of 18F-FDG PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors Treated with Second Peptide Receptor Radionuclide Therapy Course with 177Lu-DOTATATE. Life. 2021; 11(3):198. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030198
Chicago/Turabian StyleRodrigues, Margarida, Kevin-Klaus Winkler, Hanna Svirydenka, Bernhard Nilica, Christian Uprimny, and Irene Virgolini. 2021. "Long-Term Survival and Value of 18F-FDG PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors Treated with Second Peptide Receptor Radionuclide Therapy Course with 177Lu-DOTATATE" Life 11, no. 3: 198. https://0-doi-org.brum.beds.ac.uk/10.3390/life11030198