
Exploratory Study of the Association between the Severity of Idiopathic Intracranial Hypertension and Electroretinogram Photopic Negative Response Amplitude Obtained Using a Handheld Device

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
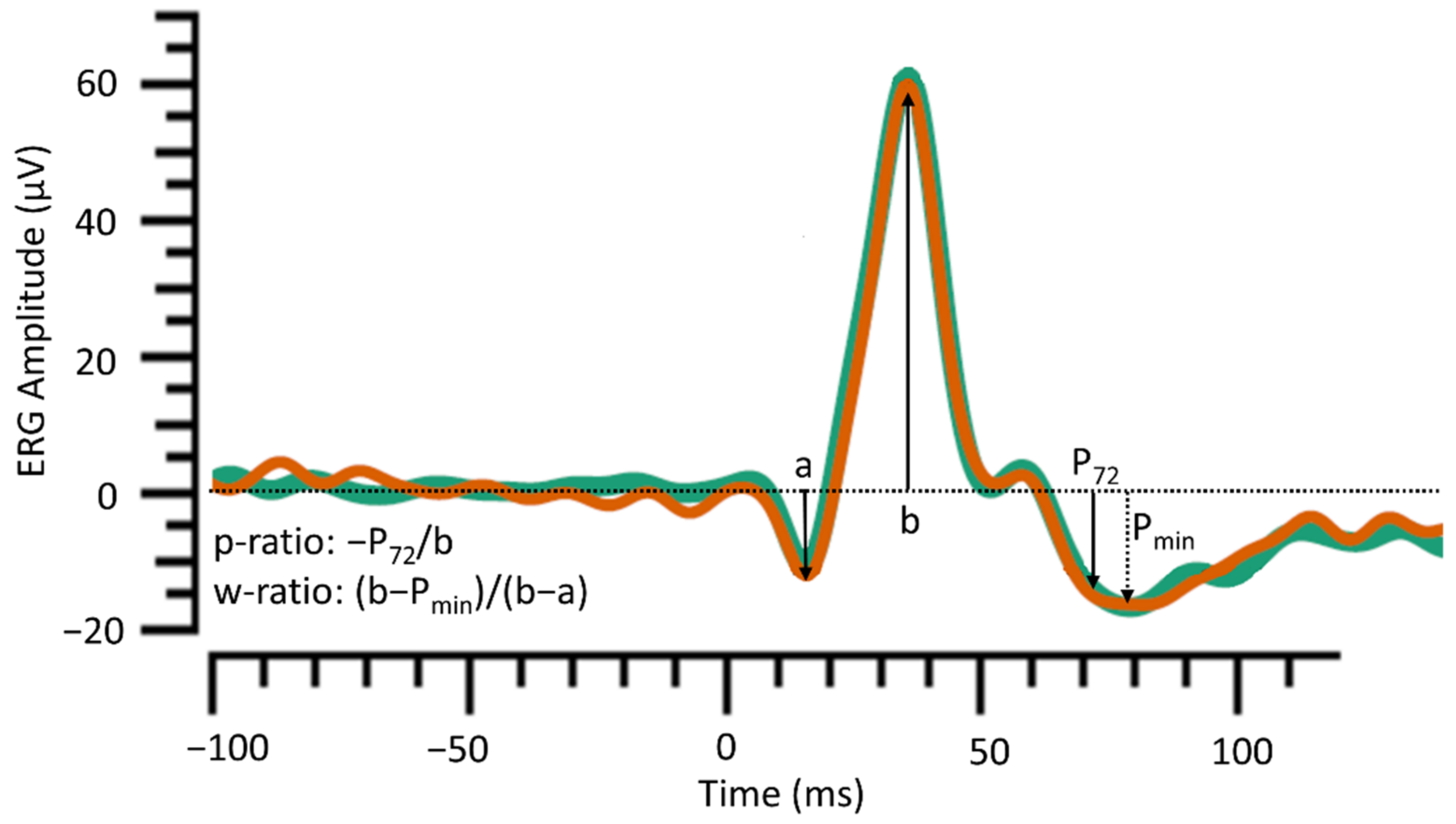
2.2. Electroretinogram Recordings Using a Handheld Device
2.3. Clinical Characteristics and Other Parameters of Visual Structure and Function
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
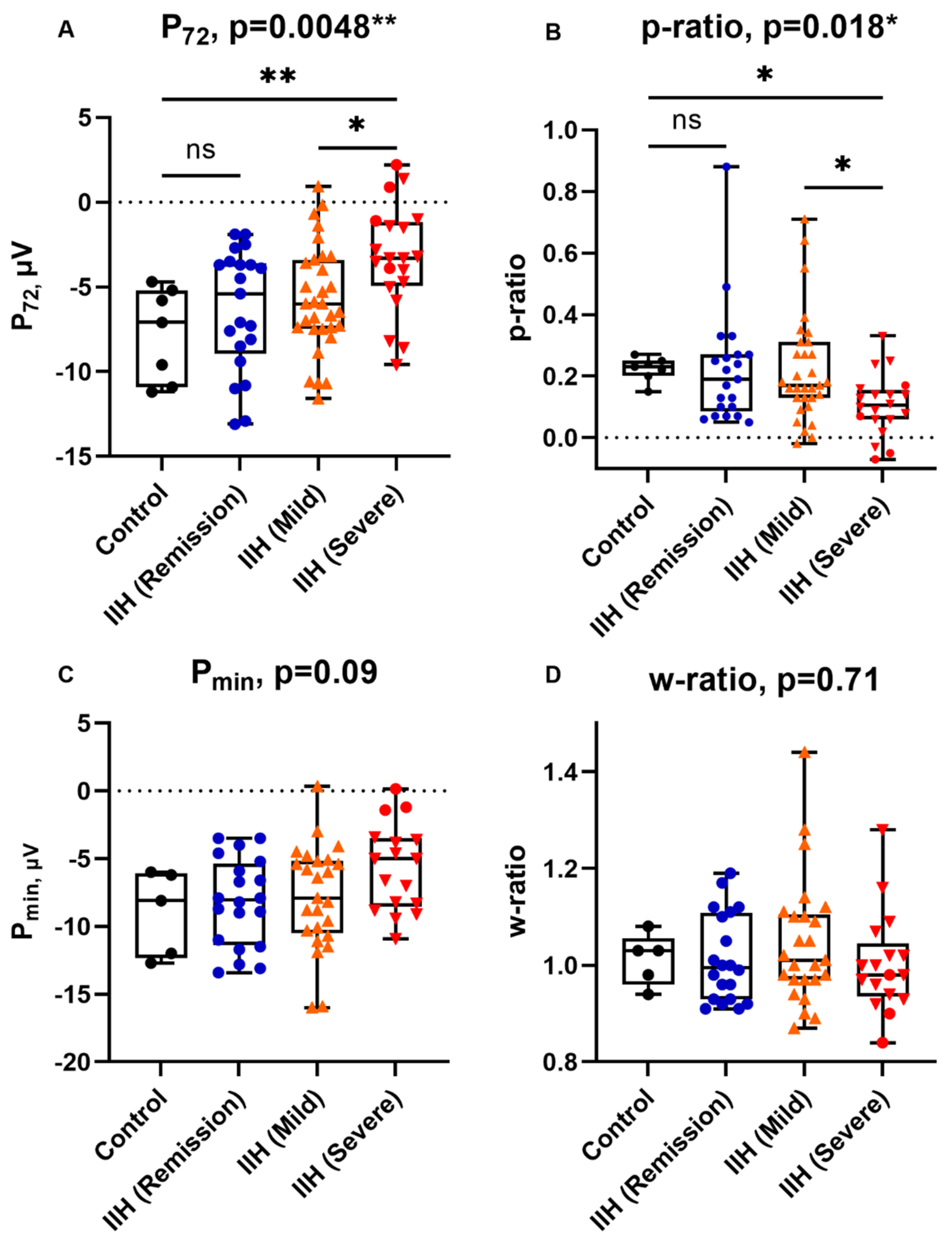
3.2. Electroretinographic Findings and IIH Severity
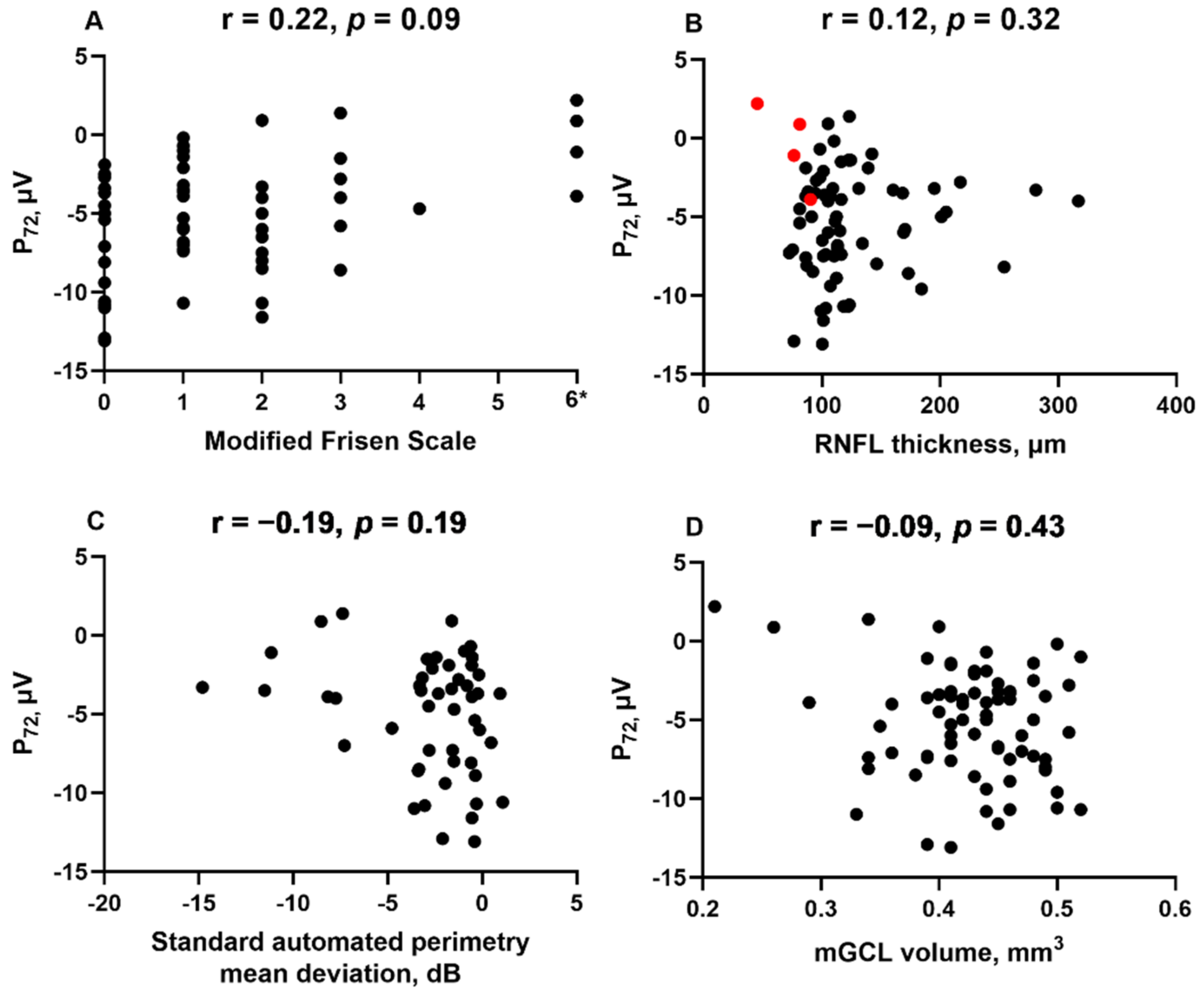
3.3. Correlation between PhNR and Parameters of Visual Structure and Function
3.4. Correlation between PhNR and Clinical Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayreh, S.S. Pathogenesis of optic disc edema in raised intracranial pressure. Prog. Retin. Eye Res. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollan, S.P.; Aguiar, M.; Evison, F.; Frew, E.; Sinclair, A.J. The expanding burden of idiopathic intracranial hypertension. Eye 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miah, L.; Strafford, H.; Fonferko-Shadrach, B.; Hollinghurst, J.; Sawhney, I.M.S.; Hadjikoutis, S.; Rees, M.I.; Powell, R.; Lacey, A.; Pickrell, W.O. Incidence, Prevalence, and Health Care Outcomes in Idiopathic Intracranial Hypertension. Neurology 2021, 96, e1251–e1261. [Google Scholar] [CrossRef] [PubMed]
- Best, J.; Silvestri, G.; Burton, B.; Foot, B.; Acheson, J. The Incidence of Blindness Due to Idiopathic Intracranial Hypertension in the UK. Open Ophthalmol. J. 2013. [Google Scholar] [CrossRef] [Green Version]
- Orcutt, J.C.; Page, N.G.R.; Sanders, M.D. Factors Affecting Visual Loss in Benign Intracranial Hypertension. Ophthalmology 1984. [Google Scholar] [CrossRef]
- Mollan, S.P.; Davies, B.; Silver, N.C.; Shaw, S.; Mallucci, C.L.; Wakerley, B.R.; Krishnan, A.; Chavda, S.V.; Ramalingam, S.; Edwards, J.; et al. Idiopathic intracranial hypertension: Consensus guidelines on management. J. Neurol. Neurosurg. Psychiatry 2018. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, S.; Frishman, L.J.; Robson, J.G.; Harwerth, R.S.; Smith, E.L. The photopic negative response of the macaque electroretinogram: Reduction by experimental glaucoma. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1124–1136. [Google Scholar]
- Elgohary, A.A.; Elshazly, L.H.M. Photopic negative response in diagnosis of glaucoma: An experimental study in glaucomatous rabbit model. Int. J. Ophthalmol. 2015. [Google Scholar] [CrossRef]
- Viswanathan, S.; Frishman, L.J.; Robson, J.G.; Walters, J.W. The photopic negative response of the flash electroretinogram in primary open angle glaucoma. Investig. Ophthalmol. Vis. Sci. 2001, 42, 514–522. [Google Scholar]
- Gotoh, Y.; Machida, S.; Tazawa, Y. Selective Loss of the Photopic Negative Response in Patients with Optic Nerve Atrophy. Arch. Ophthalmol. 2004. [Google Scholar] [CrossRef] [Green Version]
- Preiser, D.; Lagrèze, W.A.; Bach, M.; Poloschek, C.M. Photopic negative response versus pattern electroretinogram in early glaucoma. Investig. Ophthalmol. Vis. Sci. 2013. [Google Scholar] [CrossRef] [Green Version]
- Moss, H.E.; Park, J.C.; McAnany, J.J. The photopic negative response in idiopathic intracranial hypertension. Investig. Ophthalmol. Vis. Sci. 2015. [Google Scholar] [CrossRef] [Green Version]
- Park, J.C.; Moss, H.E.; McAnany, J.J. Electroretinography in idiopathic intracranial hypertension: Comparison of the pattern ERG and the photopic negative response. Doc. Ophthalmol. 2018. [Google Scholar] [CrossRef]
- Mortlock, K.E.; Binns, A.M.; Aldebasi, Y.H.; North, R.V. Inter-subject, inter-ocular and inter-session repeatability of the photopic negative response of the electroretinogram recorded using DTL and skin electrodes. Doc. Ophthalmol. 2010. [Google Scholar] [CrossRef]
- Sieving, P.A.; Murayama, K.; Naarendorp, F. Push-pull model of the primate photopic electroretinogram: A role for hyperpolarizing neurons in shaping the b-wave. Vis. Neurosci. 1994. [Google Scholar] [CrossRef]
- Scott, C.J.; Kardon, R.H.; Lee, A.G.; Frisén, L.; Wall, M. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs. clinical expert assessment using a clinical staging scale. Arch. Ophthalmol. 2010. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Feng, C.; Zhao, G.; Chen, W.; Wang, M.; Sun, X.; Sha, Y.; Li, Z.; Tian, G. Pseudotumour Cerebri Syndrome in China: A Cohort Study. Sci. Rep. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wall, M.; Kupersmith, M.J.; Kieburtz, K.D.; Corbett, J.J.; Feldon, S.E.; Friedman, D.I.; Katz, D.M.; Keltner, J.L.; Schron, E.B.; McDermott, M.P. The idiopathic intracranial hypertension treatment trial clinical profile at baseline. JAMA Neurol. 2014. [Google Scholar] [CrossRef]
- Tang, J.; Hui, F.; Coote, M.; Crowston, J.G.; Hadoux, X. Baseline detrending for the photopic negative response. Transl. Vis. Sci. Technol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Miyamoto, K.; Yokota, S.; Ogino, K.; Yoshimura, N. Focal macular photopic negative response in patients with optic neuritis. Eye 2011. [Google Scholar] [CrossRef] [Green Version]
- Niyadurupola, N.; Luu, C.D.; Nguyen, D.Q.; Geddes, K.; Tan, G.X.V.; Wong, C.C.W.; Tran, T.; Coote, M.A.; Crowston, J.G. Intraocular pressure lowering is associated with an increase in the photopic negative response (PhNR) amplitude in glaucoma and ocular hypertensive eyes. Investig. Ophthalmol. Vis. Sci. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machida, S.; Gotoh, Y.; Toba, Y.; Ohtaki, A.; Kaneko, M.; Kurosaka, D. Correlation between photopic negative response and retinal nerve fiber layer thickness and optic disc topography in glaucomatous eyes. Investig. Ophthalmol. Vis. Sci. 2008. [Google Scholar] [CrossRef] [PubMed]
- Szewka, A.J.; Bruce, B.B.; Newman, N.J.; Biousse, V. Idiopathic intracranial hypertension: Relation between obesity and visual outcomes. J. Neuro Ophthalmol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Sugawara, A.; Nagashima, R.; Ikesugi, K.; Sugimoto, M.; Kondo, M. Factors affecting photopic negative response recorded with reteval system: Study of young healthy subjects. Transl. Vis. Sci. Technol. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control, n = 7 | IIH, n = 72 | p-Value | |||
|---|---|---|---|---|---|
| Remission, n = 21 | Mild, n = 31 | Severe, n = 20 | |||
| White | 2/5 (40) | 11/20 (55) | 7/21 (33) | 7/16 (44) | 0.99 |
| Female | 6/7 (86) | 20/21 (95) | 28/31(90) | 17/20 (85) | 0.54 |
| Age, years | 53.0 (32.0–65.0) | 36.0 (28.5–55.5) | 33.0 (26.0–38.0) | 30.0 (27.0–37.8) | 0.036 |
| Body mass index, Kg/m2 | 34.5 (32.3–42.2) | 35.3 (32.0–41.9) | 34.2 (31.3–39.3) | 33.2 (28.2–40.0) | 0.68 |
| Duration of symptoms, months | N/A | 28 (12–60) | 18 (5.3–36) | 24 (7.0–78) | 0.58 |
| SAP-MD, db | NA | −1.8 (−3.1, −0.41) | −1.2 (−2.6, −0.34) | −5.4 (−9.2, −1.4) | 0.0038 |
| −2 ≤ SAP-MD < −5 | NA | 8/19 (42) | 4/16 (25) | 3/14 (21) | |
| SAP-MD ≤ −5 | NA | 0/19 (0) | 1/16 (6.3) | 7/14 (50) | |
| RNFL thickness, μm | 99 (91, 114) | 94 (84, 103) | 111 (102, 119) | 179 (147, 214) | < 0.0001 |
| MFS 1–2 | 0/7 (0) | 0/19 (0) | 25/25 (100) | 2/16 (12.5) | |
| MFS ≥ 3 or atrophic papilloedema | 0/7 (0) | 0/19 (0) | 0/25 (0) | 10/16 (62.5) | |
| Atrophic papilloedema | 0/7 (0) | 0/19 (0) | 0/25 (0) | 4/16 (25) | |
| mGCL volume, mm3 | 0.43 (0.39, 0.45) | 0.41 (0.39, 0.44) | 0.44 (0.41, 0.47) | 0.45 (0.37, 0.49) | 0.16 |
| CSF opening pressure, cmCSF | NA | 30 (25, 36) | 33 (28, 40) | 33 (29, 40) | 0.23 |
| Control, n = 7 | IIH, n = 72 | p-Value | |||
|---|---|---|---|---|---|
| Remission, n = 21 | Mild, n = 31 | Severe, n = 20 | |||
| Photopic flash a-wave | |||||
| Amplitude (μV) | −8.3 (−11.1, −4.8) | −8.4 (−10.2, 6.3) | −6.8 (−8.4, −4.7) | −5.8 (−8.4, −4.2) | 0.070 |
| Peak time (ms) | 13.5 (13.2, 14.0) | 13.2 (13.1, 14.0) | 13.3 (12.5, 13.7) | 13.2 (12.7, 13.7) | 0.53 |
| Photopic flash b-wave | |||||
| Amplitude (μV) | 40.5 (33.7, 52.7) | 40.2 (33.7, 52.3) | 38.8 (30.2, 45.9) | 36.5 (26.7, 49.8) | 0.77 |
| Peak time (ms) | 30.4 (29.9, 31.0) | 29.7 (27.9, 31.4) | 29.2 (27.8, 29.9) | 29.2 (28.3, 30.0) | 0.29 |
| PhNR | |||||
| Amplitude, at 72 ms, P72 (μV) | −7.1 (−10.9, −5.2) | −5.4 (−9.0, −3.6) | −6.0 (−7.5, −3.4) | −3.3 (−4.9, −1.2) | 0.0048 |
| p-ratio | 0.23 (0.20, 0.25) | 0.19 (0.09, 0.27) | 0.17 (0.13, 0.31) | 0.11 (0.06, 0.16) | 0.018 |
| Amplitude at trough, Pmin (μV) | −8.1 (−12.4, −6.1) | −8.1 (−11.4, −5.4) | −7.9 (−10.5, −5.2) | −5.0 (−8.6, −3.5) | 0.09 |
| w-ratio | 1.03 (0.96, 1.06) | 1.00 (0.93, 1.11) | 1.01 (0.97, 1.11) | 0.98 (0.94, 1.05) | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raharja, A.; Leo, S.M.; Chow, I.; Indusegaran, M.; Hammond, C.J.; Mahroo, O.A.; Wong, S.H. Exploratory Study of the Association between the Severity of Idiopathic Intracranial Hypertension and Electroretinogram Photopic Negative Response Amplitude Obtained Using a Handheld Device. Life 2021, 11, 437. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050437
Raharja A, Leo SM, Chow I, Indusegaran M, Hammond CJ, Mahroo OA, Wong SH. Exploratory Study of the Association between the Severity of Idiopathic Intracranial Hypertension and Electroretinogram Photopic Negative Response Amplitude Obtained Using a Handheld Device. Life. 2021; 11(5):437. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050437
Chicago/Turabian StyleRaharja, Antony, Shaun M. Leo, Isabelle Chow, Mathura Indusegaran, Christopher J. Hammond, Omar A. Mahroo, and Sui H. Wong. 2021. "Exploratory Study of the Association between the Severity of Idiopathic Intracranial Hypertension and Electroretinogram Photopic Negative Response Amplitude Obtained Using a Handheld Device" Life 11, no. 5: 437. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050437