
Evaluation of Blood Coagulation Parameters and ADMA, NO, IL-6, and IL-18 Serum Levels in Patients with Neovascular AMD before, during, and after the Initial Loading Phase of Intravitreal Aflibercept

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
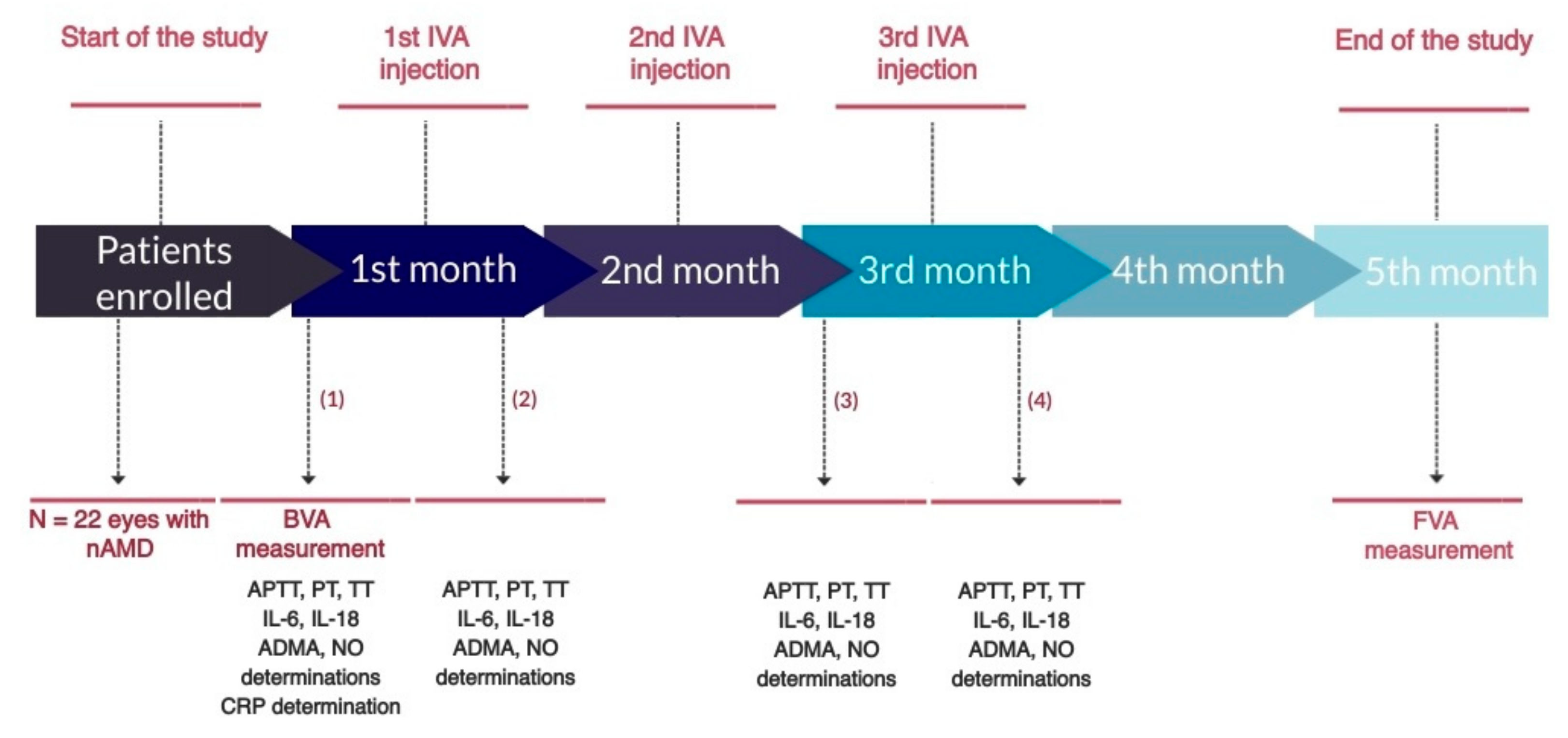
2.2. Study Design
2.3. Sample Collection
2.4. Statistical Analysis
3. Results
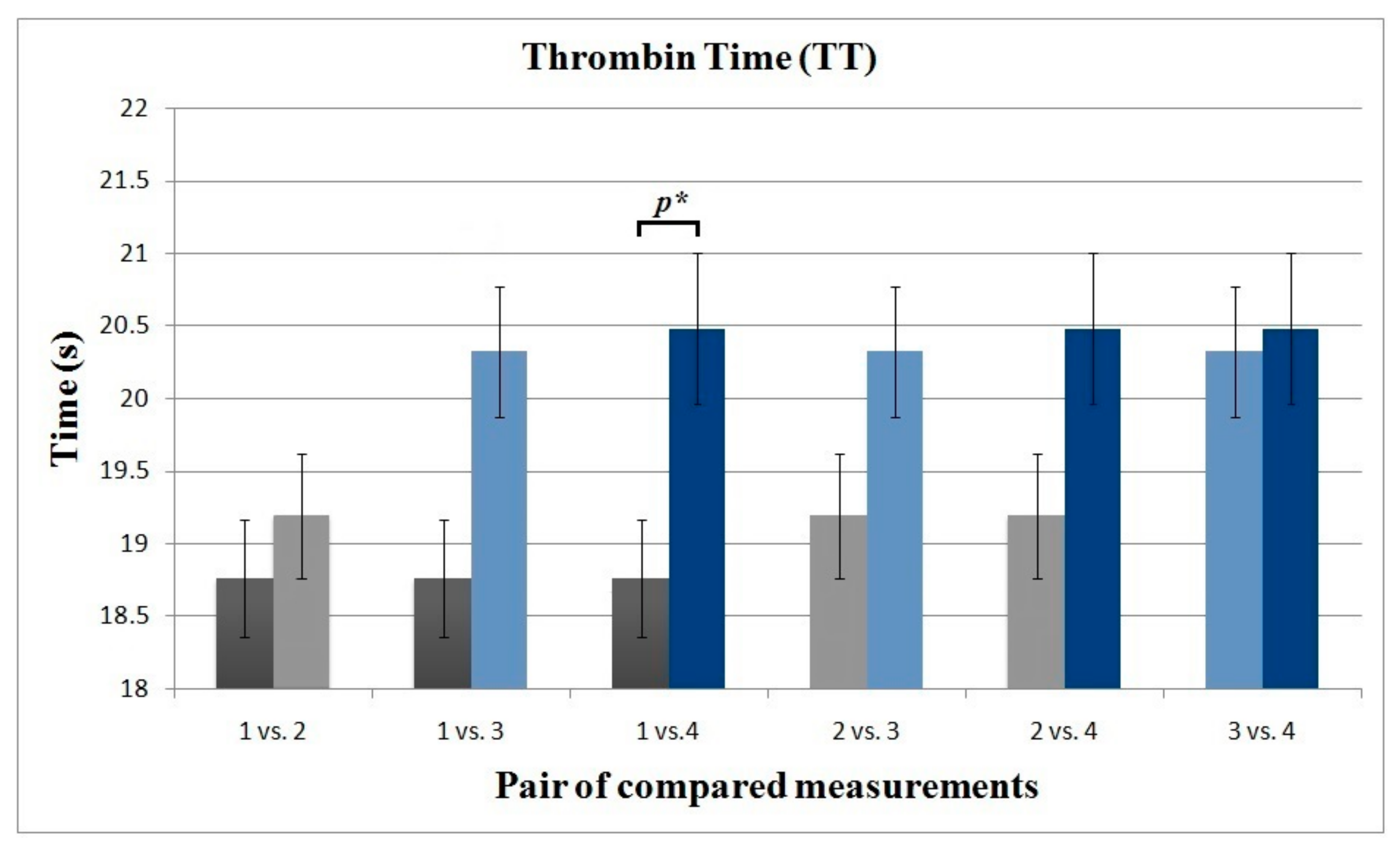
3.1. Blood Coagulation Parameters
3.2. AMDA and NO
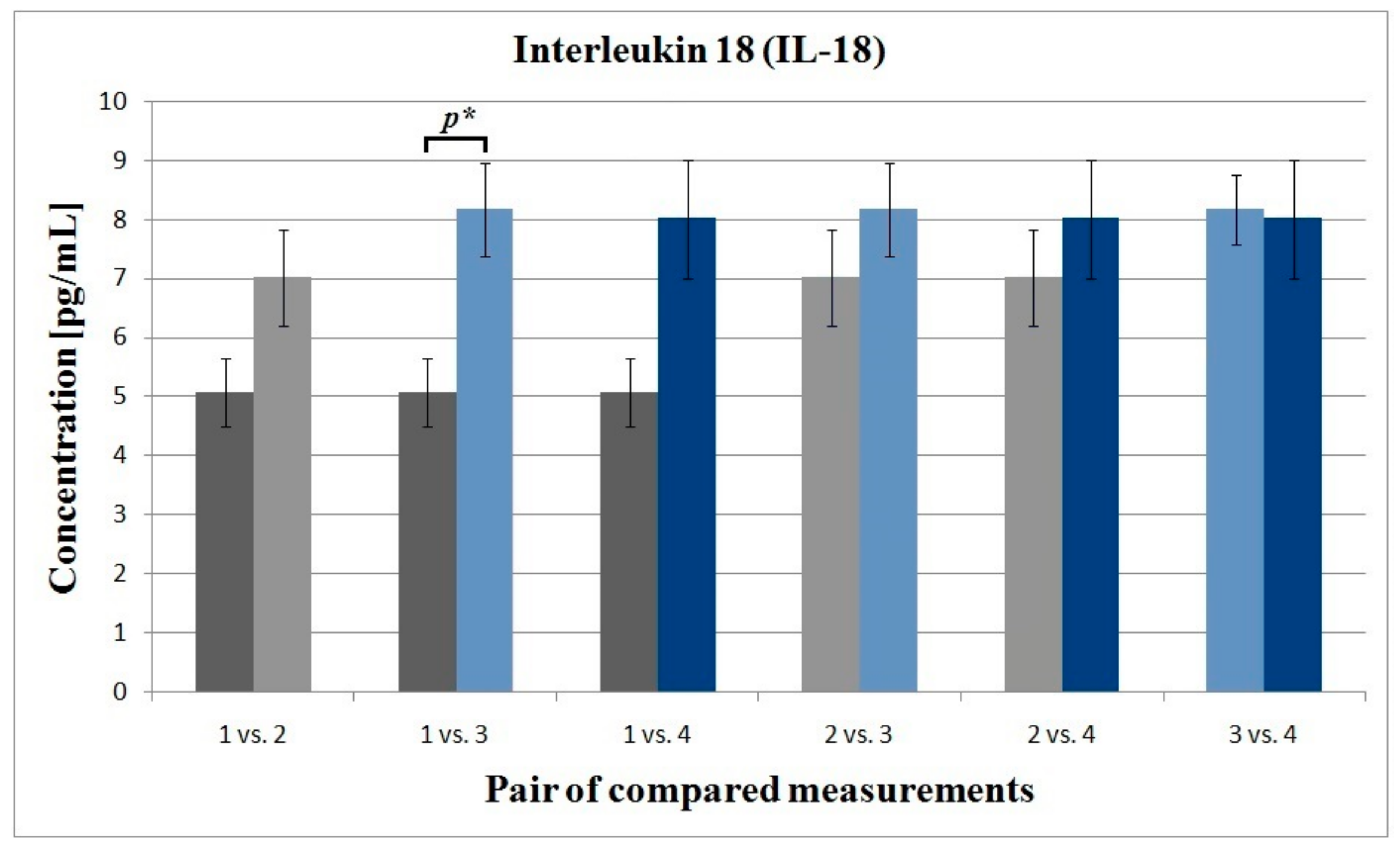
3.3. Interleukin 6 and Interleukin 18
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.; Chioreso, C.; Schweizer, M.L.; Abramoff, M.D. Effects of aflibercept for neovascular age-related macular degeneration: A systematic review and meta-analysis of observational comparative studies. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5616–5627. [Google Scholar]
- Semeraro, F.; Morescalchi, F.; Duse, S.; Parmeggiani, F.; Gambicorti, E.; Costagliola, C. Aflibercept in wet AMD: Specific role and optimal use. Drug Des. Devel. Ther. 2013, 7, 711–722. [Google Scholar] [CrossRef] [Green Version]
- Cheung, G.C.M.; Lai, T.Y.Y.; Gomi, F.; Ruamviboonsuk, P.; Koh, A.; Lee, W.K. Anti-VEGF therapy for neovascular AMD and polypoidal choroidal vasculopathy. Asia Pac. J. Ophthalmol. 2017, 6, 527–534. [Google Scholar]
- Sato, T.; Takeuchi, M.; Karasawa, Y.; Enoki, T.; Ito, M. Intraocular inflammatory cytokines in patients with neovascular age-related macular degeneration before and after initiation of intravitreal injection of anti-VEGF inhibitor. Sci. Rep. 2018, 8, 1098. [Google Scholar] [CrossRef] [PubMed]
- Förstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef] [Green Version]
- Sobolewska, B.; Golenko, J.; Poeschel, S.; Grimmel, C.; Gatsiou, A.; Sopova, K.; Biedermann, T.; Schenke-Layland, K.; Stellos, K.; Ziemssen, F. Influence of aflibercept on platelet activation profile. Exp. Eye Res. 2018, 175, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.; Ross, J.S.; Sangaralingham, L.R.; Adelman, R.A.; Shah, N.D.; Barkmeier, A.J. Trends of anti-vascular endothelial growth Factor use in ophthalmology among privately insured and medicare advantage patients. Ophthalmology 2017, 124, 352–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Nasir, M.A.; Rabena, M.D.; Maia, M.; et al. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab, and ranibizumab. Retina 2017, 37, 1847–1858. [Google Scholar] [CrossRef] [Green Version]
- Yi, Z.; Chen, C.; Su, Y.; Li, L.; Zhou, Y. Changes in clotting time, plasma fibrinogen levels, and blood viscosity after administration of ranibizumab for treatment of choroidal neovascularization. Curr. Eye Res. 2015, 40, 1166–1171. [Google Scholar] [CrossRef]
- Edington, M.; Connolly, J.; Chong, N.V. Pharmacokinetics of intravitreal anti-VEGF drugs in vitrectomized versus non-vitrectomized eyes. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1217–1224. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Das, A.; Do, D.V.; Dugel, P.U.; Gomes, A.; Holz, F.G.; Koh, A.; Pan, C.K.; Sepah, Y.J.; Patel, N.; et al. Brolucizumab: Evolution through preclinical and clinical studies and theimplications for the management of neovascular age-related macular degeneration. Ophthalmology 2020, 127, 963–976. [Google Scholar] [CrossRef] [PubMed]
- Christoforidis, J.; Byron, B.K.; Binzel, K.; Bhatia, P.; Wei, L.; Kumar, K.; Knopp, M.V. Systemic biodistribution and intravitreal pharmacokinetic properties of bevacizumab, ranibizumab, and aflibercept in a nonhuman primate model. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5636–5645. [Google Scholar] [CrossRef] [Green Version]
- Qian, J.; Jiang, Y.R. Decreased prothrombin time after intravitreal bevacizumab in the early period in patients with proliferative diabetic retinopathy. Acta Ophthal. 2011, 89, 332–335. [Google Scholar] [CrossRef]
- Luaces-Rodríguez, A.; Amo, E.M.D.; Mondelo-García, C.; Gómez-Lado, N.; Gonzalez, F.; Ruibal, Á.; González-Barcia, M.; Zarra-Ferro, I.; Otero-Espinar, F.J.; Fernández-Ferreiro, A.; et al. PET study of ocular and blood pharmacokinetics of intravitreal bevacizumab and aflibercept in rats. Eur. J. Pharm. Biopharm. 2020, 154, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.E.; Flax, S.D.; Harris, N.S. Coagulation testing in the core laboratory. Lab. Med. 2017, 48, 295–313. [Google Scholar] [CrossRef]
- Kamal, A.H.; Tefferi, A.; Pruthi, R.K. How to interpret and pursue an abnormal prothrombin time, activated partial thromboplastin time, and bleeding time in adults. Mayo Clin. Proc. 2007, 82, 864–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, W.Z.; Moufak, S.K.; Yusof, Z.; Mohamad, M.S.; Kamarul, I.M. Shortened activated partial thromboplastin time, a hemostatic marker for hypercoagulable state during acute coronary event. Transl. Res. 2010, 155, 315–319. [Google Scholar] [CrossRef]
- Sauls, D.L.; Banini, A.E.; Boyd, L.C.; Hoffman, M. Elevated prothrombin level and shortened clotting times in subjects with type 2 diabetes. J. Thromb. Haemost. 2007, 5, 638–639. [Google Scholar] [CrossRef]
- Korte, W.; Clarke, S.; Lefkowitz, J.B. Short activated partial thromboplastin times are related to increased thrombin generation and an increased risk for thromboembolism. Am. J. Clin. Pathol. 2000, 113, 123–127. [Google Scholar] [CrossRef]
- Altinkaynak, H.; Kars, M.E.; Kurkcuoglu, P.Z.; Ugurlu, N. Blood coagulation parameters after intravitreal injection of aflibercept in patients with neovascular age-related macular degeneration. Int. Ophthalmol. 2018, 38, 2397–2402. [Google Scholar] [CrossRef]
- Georgakopoulos, C.G.; Makri, O.E.; Pallikari, A.; Kagkelaris, K.; Plotas, P.; Grammenou, V.; Emmanuil, A. Effect of intravitreal injection of aflibercept on blood coagulation parameters in patients with age-related macular degeneration. Ther. Adv. Ophthalmol. 2020, 12, 2515841420903929. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, M.; Matsumoto, M.; Hayakawa, M.; Sakai, K.; Fujimura, Y.; Ogata, N. Intravitreal injection of aflibercept, an anti-VEGF antagonist, down-regulates plasma von Willebrand factor in patients with age-related macular degeneration. Sci. Rep. 2018, 8, 1491. [Google Scholar] [CrossRef]
- Peyvandi, F.; Garagiola, I.; Baronciani, L. Role of von Willebrand factor in the haemostasis. Blood Transfus. 2011, 9, 3–8. [Google Scholar]
- Machlus, K.R.; Cardenas, J.C.; Church, F.C.; Wolberg, A.S. Causal relationship between hyperfibrinogenemia, thrombosis, and resistance to thrombolysis in mice. Blood 2011, 117, 4953–4963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannel, W.B.; Wolf, P.A.; Castelli, W.P.; D’Agostino, R.B. Fibrinogen and risk of cardiovascular disease: The Framingham Study. JAMA 1987, 258, 1183–1186. [Google Scholar] [CrossRef]
- Floyd, C.N.; Ferro, A. The platelet fibrinogen receptor: From megakaryocyte to the mortuary. JRSM Cardiovasc. Dis. 2012, 1, 1–13. [Google Scholar]
- Nomura, Y.; Kaneko, M.; Miyata, K.; Yatomi, Y.; Yanagi, Y. Bevacizumab and aflibercept activate platelets via FcγRIIa. Investig. Ophthalmol. Vis. Sci. 2015, 56, 8075–8082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutto, I.A.; Baba, T.; Merges, C.; McLeod, D.S.; Lutty, G.A. Low nitric oxide synthases (NOSs) in eyes with age-related macular degeneration (AMD). Exp. Eye Res. 2010, 90, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Farah, C.; Mithchel, L.Y.; Balligand, J.L. Nitric oxide signalling in cardiovascular health and disease. Nat. Rev. Cardiol. 2018, 15, 292. [Google Scholar] [CrossRef]
- Freedman, J.E.; Loscalzo, J. Nitric oxide and its relationship to thrombotic disorders. J. Thromb. Haemost. 2003, 1, 1183–1188. [Google Scholar] [CrossRef]
- Fiedler, L.R.; Bachetti, T.; Leiper, J.; Zachary, I.; Chen, L.; Renné, T.; Wojciak-Stothard, B. The ADMA/DDAH pathway regulates VEGF-mediated angiogenesis. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 2117–2124. [Google Scholar] [CrossRef] [Green Version]
- Keles, S.; Ates, O.; Kartal, B.; Alp, H.H.; Ekinci, M.; Ceylan, E.; Ondas, O.; Arpali, E.; Dogan, S.; Yildirim, K.; et al. Evaluation of cardiovascular biomarkers in patients with age-related wet macular degeneration. Clin. Ophthalmol. 2014, 8, 1573–1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogg, R.E.; Gilchrist, S.E.C.M.; Woodside, J.V.; Jiang, J.; Ni, Z.; Wang, J.; Sun, X. Homocysteine, B–vitamin status, ADMA and risk of age-related macular disease–A case-control study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 2197. [Google Scholar]
- Pinna, A.; Zinellu, A.; Tendas, D.; Blasetti, F.; Carru, C.; Castiglia, P. Plasma homocysteine and asymmetrical dimethyl-L-arginine (ADMA) and whole blood DNA methylation in early and neovascular age-related macular degeneration: A pilot study. Med. Sci. Monit. 2014, 41, 88–96. [Google Scholar] [CrossRef]
- Kersten, E.; Paun, C.C.; Schellevis, R.L.; Hoyng, C.B.; Delcourt, C.; Lengyel, I.; Peto, T.; Ueffing, M.; Klaver, C.C.W.; Dammeier, S.; et al. Systemic and ocular fluid compounds as potential biomarkers in age-related macular degeneration. Surv. Ophthalmol. 2018, 63, 9–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winnik, S.; Lohmann, C.; Siciliani, G.; Von Lukowicz, T.; Kuschnerus, K.; Kraenkel, N.; Brokopp, C.E.; Enseleit, F.; Michels, S.; Ruschitzka, F.; et al. Systemic VEGF inhibition accelerates experimental atherosclerosis and disrupts endothelial homeostasis—Implications for cardiovascular safety. Int. J. Cardiol. 2013, 168, 2453–2461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sümbül, A.T.; Dişel, U.; Sezgin, N.; Sezer, A.; Köse, F.; Beşen, A.A.; Sümbül, Z.; Abalı, H.; Özyılkan, Ö. Can serial monitoring of serum vascular endothelial growth factor (VEGF), nitric oxide (NO), and angiotensin II (ANGII) levels have predictive role during bevacizumab treatment? Med. Sci. Monit. 2014, 20, 428–433. [Google Scholar]
- Ghasemi, A.; Zahediasl, S.; Azizi, F. Reference values for serum nitric oxide metabolites in anadult population. Clin. Biochem. 2010, 43, 89–94. [Google Scholar] [CrossRef]
- Hov, G.G.; Sagen, E.; Bigonah, A.; Asberg, A. Health-associated reference values for arginine, asymmetric dimethylarginine (ADMA) and symmetric dimethylarginine (SDMA) measured with high-performance liquid chromatography. Scand. J. Clin. Lab. Investig. 2007, 67, 868–876. [Google Scholar] [CrossRef]
- Knickelbein, J.E.; Chan, C.C.; Sen, H.N.; Ferris, F.L.; Nussenblatt, R.B. Inflammatory mechanisms of age-related macular degeneration. Int. Ophthalmol. Clin. 2015, 55, 63–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.; Doyle, S.; Humphries, P. IL-18: A new player in immunotherapy for age-related macular degeneration? Expert Rev. Clin. Immunol. 2014, 10, 1273–1275. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Choy, D.F.; Yoshida, T.; Iwase, T.; Hafiz, G.; Xie, B.; Hackett, S.F.; Arron, J.R.; Campochiaro, P.A. Interleukin-18 has antipermeablity and antiangiogenic activities in the eye: Reciprocal suppression with VEGF. J. Cell Physiol. 2014, 229, 974–983. [Google Scholar] [CrossRef] [Green Version]
- Echevarria, F.D.; Formichella, C.R.; Sappington, R.M. Interleukin-6 deficiency attenuates retinal ganglion cell axonopathy and glaucoma-related vision loss. Front. Neurosci. 2017, 11, 318. [Google Scholar] [CrossRef] [Green Version]
- Pham, B.H.; Hien, D.L.; Matsumiya, W.; Ngoc, T.T.T.; Doan, H.L.; Akhavanrezayat, A.; Yaşar, C.; Nguyen, H.V.; Halim, M.S.; Nguyen, Q.D. Anti-interleukin-6 receptor therapy with tocilizumab for refractory pseudophakic cystoid macular edema. Am. J. Ophthalmol. Case Rep. 2020, 20, 100881. [Google Scholar] [CrossRef] [PubMed]
- Chong, D.Y.; Boehlke, C.S.; Zheng, Q.D.; Zhang, L.; Han, Y.; Zacks, D.N. Interleukin-6 as a photoreceptor neuroprotectant in an experimental model of retinal detachment. IOVS 2008, 49, 3193–3200. [Google Scholar]
- Wainstein, M.V.; Mossmann, M.; Araujo, G.N.; Gonçalves, S.C.; Gravina, G.L.; Sangalli, M.; Veadrigo, F.; Matte, R.; Reich, R.; Costa, F.G.; et al. Elevated serum interleukin-6 is predictive of coronary artery disease in intermediate risk overweight patients referred for coronary angiography. Diabetol. Metab. Syndr. 2017, 9, 67. [Google Scholar] [CrossRef]
- Bacchiega, B.C.; Bacchiega, A.B.; Usnayo, M.J.G.; Bedirian, R.; Singh, G.; Pinheiro, G.D. Interleukin 6 inhibition and coronary artery disease in a high-risk population: A prospective community-based clinical study. J. Am. Heart Assoc. 2017, 6, e005038. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Li, Z.; Li, X.; Chen, Y.; Zhang, Y.; Ding, D.; Deng, X.; Xia, M.; Qiu, J.; Ling, W. Association between serum interleukin-6 concentration and mortality in patients with coronary artery disease. Mediat. Inflamm. 2013, 2013, 726178. [Google Scholar] [CrossRef]
- Jefferis, B.J.; Papacosta, O.; Owen, C.G.; Wannamethee, S.G.; Humphries, S.E.; Woodward, M.; Lennon, L.T.; Thomson, A.; Welsh, P.; Rumley, A.; et al. Interleukin 18 and coronary heart disease: Prospective study and systematic review. Atherosclerosis 2011, 217, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Blankenberg, S.; Luc, G.; Ducimetière, P.; Arveiler, D.; Ferrières, J.; Amouyel, P.; Evans, A.; Cambien, F.; Tiret, L. Interleukin-18 and the risk of coronary heart disease in European men: The prospective epidemiological study of myocardial infarction (PRIME). Circulation 2003, 108, 2453–2459. [Google Scholar] [CrossRef]
- Formanowicz, D.; Wanic-Kossowska, M.; Pawliczak, E.; Radom, M.; Formanowicz, P. Usefulness of serum interleukin-18 in predicting cardiovascular mortality in patients with chronic kidney disease—Systems and clinical approach. Sci. Rep. 2015, 5, 18332. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, Z.; Wei, R.; Miao, X.; Sun, S.; Liang, G.; Chu, C.; Zhao, L.; Zhu, X.; Guo, Q.; et al. IL (interleukin)-6 contributes to deep vein thrombosis and is negatively regulated by miR-338–5p. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 323–334. [Google Scholar] [CrossRef]
- Wassmann, S.; Stumpf, M.; Strehlow, K.; Schmid, A.; Schieffer, B.; Böhm, M.; Nickenig, G. Interleukin-6 induces oxidative stress and endothelial dysfunction by overexpression of the angiotensin II type 1 receptor. Circ. Res. 2004, 94, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Kerr, R.; Stirling, D.; Ludlam, C.A. Interleukin 6 and haemostasis. Br. J. Haematol. 2001, 115, 3–12. [Google Scholar]
- Senchenkova, E.Y.; Komoto, S.; Russell, J.; Almeida-Paula, L.D.; Yan, L.S.; Zhang, S.; Grangder, D.N. Interleukin-6 mediates the platelet abnormalities and thrombogenesis associated with experimental colitis. Am. J. Pathol. 2013, 183, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Zhou, R.; Zhao, X.; Liu, R.; Ye, C. Correlation between the expression of IL-18 and deep venous thrombosis. Int. J. Mol. Med. 2018, 42, 883–896. [Google Scholar]
- Trøseid, M.; Seljeflot, I.; Hjerkinn, E.M.; Arnesen, H. Interleukin-18 is a strong predictor of cardiovascular events in elderly men with the metabolic syndrome: Synergistic effect of inflammation and hyperglycemia. Diabetes Care 2009, 32, 486–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiner, G.; Marcuzzi, A.; Zanin, V.; Monasta, L.; Zauli, G. Cytokine levels in the serum of healthy subjects. Mediators Inflamm. 2013, 434010. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Takahashi, H.; Tan, X.; Inoue, Y.; Nomura, Y.; Arai, Y.; Fujino, Y.; Kawashima, H.; Yanagi, Y. Changes in multiple cytokine concentrations in the aqueous humour of neovascular age-related macular degeneration after 2 months of ranibizumab therapy. Br. J. Ophthalmol. 2018, 102, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Kotake, O.; Noma, H.; Yasuda, K.; Motohashi, R.; Goto, H.; Shimura, M. Comparing cytokine kinetics between ranibizumab and aflibercept in central retinal vein occlusion with macular edema. Ophthalmic Res. 2019, 61, 210–217. [Google Scholar] [CrossRef]
- Smidowicz, A.; Regula, J. Effect of nutritional status and dietary patterns on human serum C-reactive protein and interleukin-6 Concentrations. Adv. Nutr. 2015, 6, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Trøseid, M.; Arnesen, H.; Hijerkinn, E.M.; Seljeflot, I. Serum levels of interleukin-18 are reduced by diet and n-3 fatty acid intervention in elderly high-risk men. Metabolism 2009, 58, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Engeli, S.; Tsikas, D.; Lehmann, A.C.; Bönke, J.; Haas, V.; Strauß, A.; Jordan, J. Influence of dietary fat ingestion on asymmetrical dimethylarginine in lean and obese human subjects. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 720–726. [Google Scholar]
- Tayeh, O.; Fahmi, A.; Islam, M.; Saied, M. Asymmetric dimethylarginine as a prognostic marker for cardiovascular complications in hypertensive patients. Egypt Heart J. 2011, 63, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Pascale, V.; Pascale, W.; Lavanga, V.; Sansone, V.; Ferrario, P.; Colonna, V.D.G. L-arginine, asymmetric dimethylarginine, and symmetric dimethylarginine in plasma and synovial fluid of patients with knee osteoarthritis. Med. Sci. Monit. 2013, 19, 1057–1062. [Google Scholar] [CrossRef] [Green Version]
- Livshits, G.; Zhai, G.; Hart, D.J.; Kato, B.S.; Wang, H.; Williams, F.M.; Spector, T.D. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: The Chingford study. Arthritis Rheum. 2009, 60, 2037–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, U.H. Effects of androgens on haemostasis. Maturitas 1996, 24, 147–155. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Number of Patients (Eyes), N (%) | |
|---|---|
| All | 22 |
| Female | 13 (59.01) |
| Male | 9 (40.9) |
| Age in years (mean value) | |
| Female | 78.69 |
| Male | 76.89 |
| Range | 66–99 |
| Visual Acuity (mean LogMAR) | |
| BVA a | 0.2944 |
| FVA b | 0.2399 |
| p-value c | 0.001 |
| Compared Measurements | Parameter | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PT | APTT | TT | IL-6 | IL-18 | ADMA | NO | |||||||||||||||
| MV (s) | SE | p-Val. | MV (s) | SE | p-Val. | MV (s) | SE | p-Val. | MV (pg/mL) | SE | p-Val. | MV (pg/mL) | SE | p-Val. | MV (µmol/L) | SE | p-Val. | MV (µmol/L) | SE | p-Val. | |
| 1 2 | 14.87 14.79 | 0.22 0.23 | 0.981 | 26.31 27.83 | 0.35 0.60 | 0.311 | 18.76 19.19 | 0.40 0.43 | 0.891 | 11.74 11.13 | 1.54 1.17 | 0.278 | 5.06 7.02 | 0.58 0.81 | 0.317 | 0.87 0.79 | 0.10 0.12 | 0.946 | 9.38 6.86 | 1.23 0.83 | 0.387 |
| 1 3 | 14.87 15.20 | 0.22 0.20 | 0.864 | 26.31 27.75 | 0.35 0.65 | 0.360 | 18.76 20.32 | 0.40 0.45 | 0.076 | 11.74 11.54 | 1.54 1.82 | 0.702 | 5.06 8.16 | 0.58 1.00 | 0.037 | 0.87 0.76 | 0.10 0.06 | 0.874 | 9.38 10.01 | 1.23 1.12 | 0.979 |
| 1 4 | 14.87 15.40 | 0.22 0.45 | 0.584 | 26.31 28.58 | 0.35 0.78 | 0.053 | 18.76 20.48 | 0.40 0.52 | 0.041 | 11.74 12.21 | 1.54 2.58 | 0.385 | 5.06 8.01 | 0.58 0.78 | 0.052 | 0.87 0.91 | 0.10 0.13 | 0.992 | 9.38 9.73 | 1.23 1.24 | 0.996 |
| 2 3 | 14.79 15.20 | 0.23 0.20 | 0.758 | 27.83 27.75 | 0.60 0.65 | 0.891 | 19.19 20.32 | 0.43 0.45 | 0.291 | 11.13 11.54 | 1.17 1.82 | 0.330 | 7.02 8.16 | 0.81 1.00 | 0.719 | 0.79 0.76 | 0.12 0.06 | 0.997 | 6.86 10.01 | 0.83 1.12 | 0.199 |
| 2 4 | 14.79 15.40 | 0.23 0.45 | 0.455 | 27.83 28.58 | 0.60 0.78 | 0.802 | 19.19 20.48 | 0.43 0.52 | 0.186 | 11.13 12.21 | 1.17 2.58 | 0.074 | 7.02 8.01 | 0.81 0.78 | 0.792 | 0.79 0.91 | 0.12 0.13 | 0.877 | 6.86 9.73 | 0.83 1.24 | 0.272 |
| 3 4 | 15.20 15.40 | 0.20 0.45 | 0.961 | 27.75 28.58 | 0.65 0.78 | 0.750 | 20.32 20.48 | 0.45 0.52 | 0.902 | 11.54 12.21 | 1.82 2.58 | 0.459 | 8.16 8.01 | 0.81 0.78 | 0.899 | 0.76 0.91 | 0.06 0.13 | 0.774 | 10.01 9.73 | 1.12 1.24 | 0.998 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiciński, M.; Seredyka-Burduk, M.; Liberski, S.; Marczak, D.; Pol, M.; Malinowski, B.; Pawlak-Osińska, K.; Kaluzny, B.J. Evaluation of Blood Coagulation Parameters and ADMA, NO, IL-6, and IL-18 Serum Levels in Patients with Neovascular AMD before, during, and after the Initial Loading Phase of Intravitreal Aflibercept. Life 2021, 11, 441. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050441
Wiciński M, Seredyka-Burduk M, Liberski S, Marczak D, Pol M, Malinowski B, Pawlak-Osińska K, Kaluzny BJ. Evaluation of Blood Coagulation Parameters and ADMA, NO, IL-6, and IL-18 Serum Levels in Patients with Neovascular AMD before, during, and after the Initial Loading Phase of Intravitreal Aflibercept. Life. 2021; 11(5):441. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050441
Chicago/Turabian StyleWiciński, Michał, Małgorzata Seredyka-Burduk, Sławomir Liberski, Daria Marczak, Magdalena Pol, Bartosz Malinowski, Katarzyna Pawlak-Osińska, and Bartlomiej J. Kaluzny. 2021. "Evaluation of Blood Coagulation Parameters and ADMA, NO, IL-6, and IL-18 Serum Levels in Patients with Neovascular AMD before, during, and after the Initial Loading Phase of Intravitreal Aflibercept" Life 11, no. 5: 441. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050441