
Antithrombotic Therapy for Secondary Prevention in Patients with Non-Cardioembolic Stroke or Transient Ischemic Attack: A Systematic Review

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Mechanisms Leading to Stroke
1.2. Medical Treatment in Stroke Prevention
2. Materials and Methods
3. Results
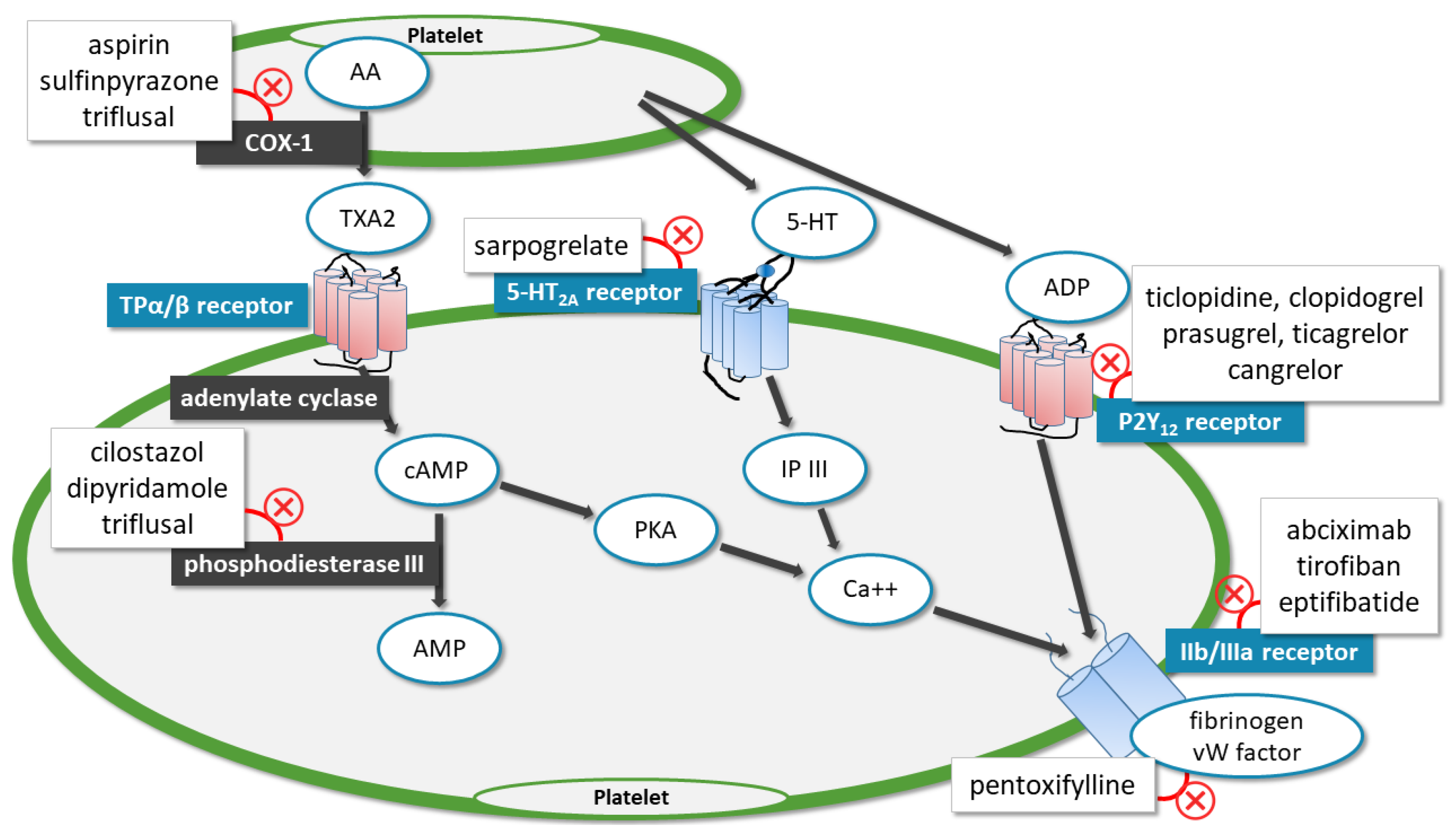
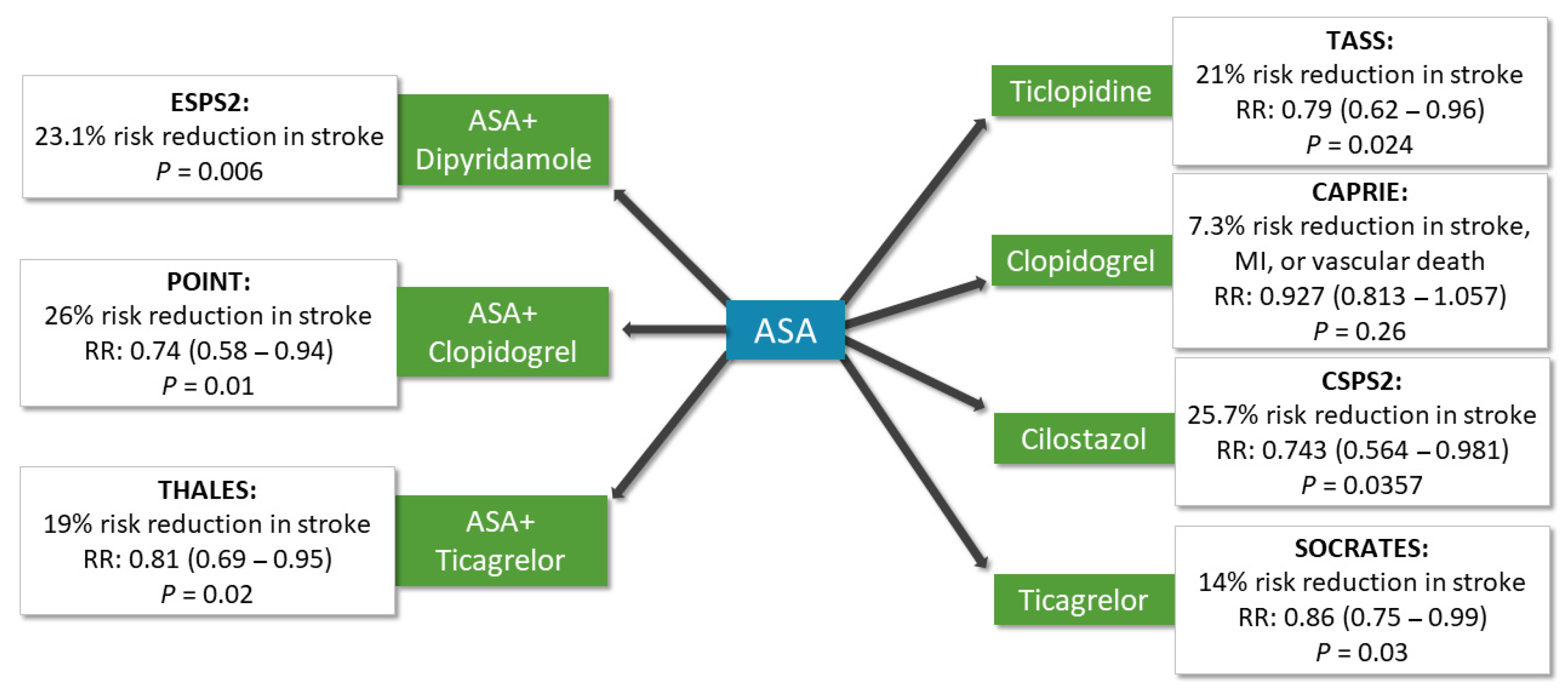
3.1. Antiplatelet Agents
3.1.1. Aspirin/Acetylsalicylic Acid
3.1.2. Ticlopidine
3.1.3. Clopidogrel
3.1.4. Cilostazol
3.1.5. Ticagrelor
3.1.6. Combinations
Dipyridamole and ASA
Clopidogrel and ASA
Ticagrelor and ASA
3.2. Alternative Agents with Antiplatelet Properties
3.2.1. Sulfinpyrazone
3.2.2. Pentoxifylline
3.2.3. Triflusal
3.2.4. Sarpogrelate
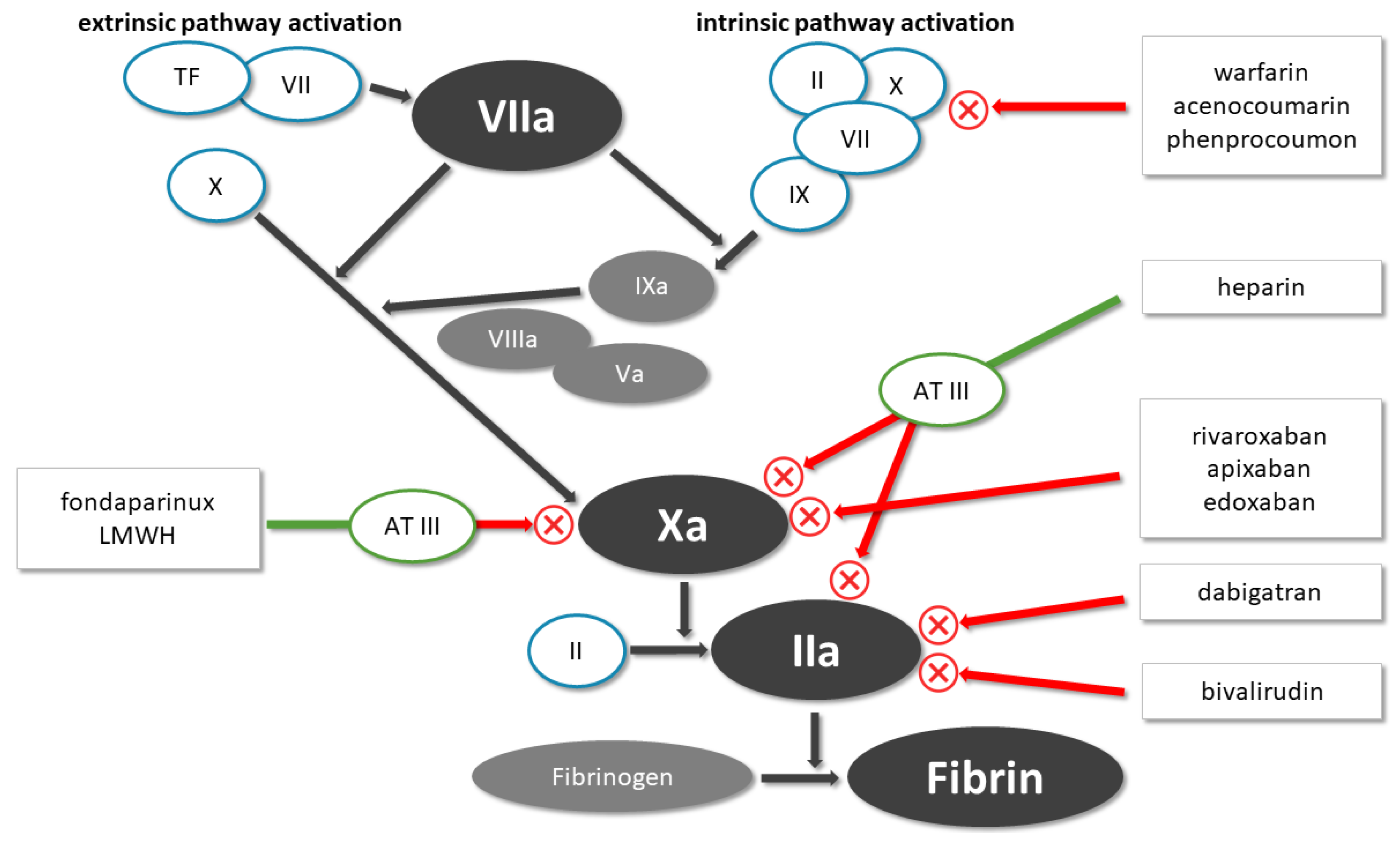
3.3. Anticoagulant Therapy
3.3.1. Warfarin
3.3.2. Rivaroxaban/Dabigatran
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke A. Stroke 2019, 50, E344–E418. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2020 update: A report from the American heart association. Circulation 2020, 141, E139–E596. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Johnston, S.C.; Amarenco, P.; Denison, H.; Evans, S.R.; Himmelmann, A.; James, S.; Knutsson, M.; Ladenvall, P.; Molina, C.A.; Wang, Y.; et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. N. Engl. J. Med. 2020, 383, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Van der Worp, H.B.; van Gijn, J. Clinical practice. Acute ischemic stroke. N. Engl. J. Med. 2007, 357, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020. [Google Scholar] [CrossRef]
- The Canadian Cooperative Study Group. A randomized trial of aspirin and sulfinpyrazone in threatened stroke. N. Engl. J. Med. 1978, 299, 53–59. [Google Scholar] [CrossRef]
- The Salt Collaborative Group Swedish Aspirin Low-dose Trial (SALT) of 75 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet 1991, 338, 1345–1349. [CrossRef]
- Gent, M. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef]
- Sacco, R.L.; Diener, H.C.; Yusuf, S.; Cotton, D.; Ôunpuu, S.; Lawton, W.A.; Palesch, Y.; Martin, R.H.; Albers, G.W.; Bath, P.; et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N. Engl. J. Med. 2008, 359, 1238–1251. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Oh, G.T.; Park, S.Y.; Choi, J.H.; Park, J.G.; Kim, C.D.; Lee, W.S.; Rhim, B.Y.; Shin, Y.W.; Hong, K.W. Cilostazol reduces atherosclerosis by inhibition of superoxide and tumor necrosis factor-α formation in low-density lipoprotein receptor-null mice fed high cholesterol. J. Pharmacol. Exp. Ther. 2005, 313, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Boulanger, J.M.; Lindsay, M.P.; Gubitz, G.; Smith, E.E.; Stotts, G.; Foley, N.; Bhogal, S.; Boyle, K.; Braun, L.; Goddard, T.; et al. Canadian stroke best practice recommendations for acute stroke management: Prehospital, emergency department, and acute inpatient stroke care, 6th edition, update 2018. Int. J. Stroke 2018, 13, 949–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, S.C.; Amarenco, P.; Albers, G.W.; Denison, H.; Easton, J.D.; Evans, S.R.; Held, P.; Jonasson, J.; Minematsu, K.; Molina, C.A.; et al. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. N. Engl. J. Med. 2016, 375, 35–43. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, W.; Lin, Y.; Meng, X.; Chen, G.; Wang, Z.; Wu, J.; Wang, D.; Li, J.; Cao, Y.; et al. Ticagrelor plus aspirin versus clopidogrel plus aspirin for platelet reactivity in patients with minor stroke or transient ischaemic attack: Open label, blinded endpoint, randomised controlled phase II trial. BMJ 2019, 365. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Pan, Y.; Zhao, X.; Li, H.; Wang, D.; Johnston, S.C.; Liu, L.; Meng, X.; Wang, A.; Wang, C.; et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack (CHANCE) trial one-year outcomes. Circulation 2015, 132, 40–46. [Google Scholar] [CrossRef]
- Dengler, R.; Diener, H.C.; Schwartz, A.; Grond, M.; Schumacher, H.; Machnig, T.; Eschenfelder, C.C.; Leonard, J.; Weissenborn, K.; Kastrup, A.; et al. Early treatment with aspirin plus extended-release dipyridamole for transient ischaemic attack or ischaemic stroke within 24 h of symptom onset (EARLY trial): A randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010, 9, 159–166. [Google Scholar] [CrossRef]
- Nakamura, T.; Tsuruta, S.; Uchiyama, S. Cilostazol combined with aspirin prevents early neurological deterioration in patients with acute ischemic stroke: A pilot study. J. Neurol. Sci. 2012, 313, 22–26. [Google Scholar] [CrossRef]
- Claiborne Johnston, S.; Donald Easton, J.; Farrant, M.; Barsan, W.; Conwit, R.A.; Elm, J.J.; Kim, A.S.; Lindblad, A.S.; Palesch, Y.Y. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. N. Engl. J. Med. 2018, 379, 215–225. [Google Scholar] [CrossRef]
- Fields, W.S.; Lemak, N.A.; Frankowski, R.F.; Hardy, R.J. Controlled trial of aspirin in cerebral ischemia. Stroke 1977, 8, 301–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, P.S.; Pedersen, H.; Marquardsen, J.; Petersson, H.; Heltberg, A.; Simonsen, N.; Munck, O.; Andersen, L.A. Acetylsalicylic acid in the prevention of stroke in patients with reversible cerebral ischemic attacks. A Danish cooperative study. Stroke 1983, 14, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britton, M.; Helmers, C.; Samuelsson, K.; Arbin, M.V.; Britton, M.; Carlsson, A.; Faire, D.D.; Gustafsson, C.; Kolmodin, G.; Landin, S.; et al. Original contributions high-dose acetylsalicylic acid after cerebral infarction. Stroke 1987, 18, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Farrell, B.; Godwin, J.; Richards, S.; Warlow, C. The United Kingdom transient ischaemic attack (UK-TIA) aspirin trial: Final results. J. Neurol. Neurosurg. Psychiatry 1951, 54, 1044–1054. [Google Scholar] [CrossRef]
- Sandercock, P.A.G. The International Stroke Trial (IST): A randomised trial of aspirin, subcutaneous heparin, both, or neither among 19 435 patients with acute ischaemic stroke. Lancet 1997, 349, 1569–1581. [Google Scholar] [CrossRef]
- Chen, Z.M. CAST: Randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997, 349, 1641–1649. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Richardson, D.J.; Kelly, M.; Ruland, S.; Hung, E.; Harris, Y.; Kittner, S.; Leurgans, S. Aspirin and ticlopidine for prevention of recurrent stroke in black patients: A randomized trial. J. Am. Med. Assoc. 2003, 289, 2947–2957. [Google Scholar] [CrossRef] [Green Version]
- Ito, E.; Takahashi, A.; Yamamoto, H.; Kuzuhara, S.; Uchiyama, S.; Nakajima, M. Ticlopidine alone versus ticlopidine plus aspirin for preventing recurrent stroke. Intern. Med. 2003, 42, 793–799. [Google Scholar] [CrossRef] [Green Version]
- Gent, M.; Donald Easton, J.; Hachinski, V.C.; Panak, E.; Sicurella, J.; Blakely, J.A.; Ellis, D.J.; Harbison, J.W.; Roberts, R.S.; Turpie, A.G.G. The canadian american ticlopidine study (Cats) in thromboembolic stroke. Lancet 1989, 333, 1215–1220. [Google Scholar] [CrossRef]
- Hass, W.K.; Easton, J.D.; Adams, H.P.; Pryse-Phillips, W.; Molony, B.A.; Anderson, S.; Kamm, B. A Randomized trial comparing ticlopidine hydrochloride with aspirin for the prevention of stroke in high-risk patients. N. Engl. J. Med. 1989, 321, 501–507. [Google Scholar] [CrossRef]
- Fukuuchi, Y.; Tohgi, H.; Okudera, T.; Ikeda, Y.; Miyanaga, Y.; Uchiyama, S.; Hirano, M.; Shinohara, Y.; Matsumoto, M.; Yamaguchi, T. A randomized, double-blind study comparing the safety and efficacy of clopidogrel versus ticlopidine in japanese patients with noncardioembolic cerebral infarction. Cerebrovasc. Dis. 2008, 25, 40–49. [Google Scholar] [CrossRef]
- Uchiyama, S.; Fukuuchi, Y.; Yamaguchi, T. The safety and efficacy of clopidogrel versus ticlopidine in Japanese stroke patients: Combined results of two Phase III, multicenter, randomized clinical trials. J. Neurol. 2009, 256, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Hayato, U.; Toshio, T.; Yukio, K.; Hiroyoshi, H. Purification of cyclic adenosine monophosphate phosphodiesterase from human platelets using new-inhibitor sepharose chromatography. Biochem. Pharmacol. 1984, 33, 3339–3344. [Google Scholar] [CrossRef]
- Weintraub, W.S. The vascular effects of cilostazol. Can. J. Cardiol. 2006, 22, 56B–60B. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.K.; Kim, Y.K.; Kim, K.Y.; Lee, J.H.; Hong, K.W. Remnant lipoprotein particles induce apoptosis in endothelial cells by NAD(P)H oxidase-mediated production of superoxide and cytokines via lectin-like oxidized low-density lipoprotein receptor-1 activation: Prevention by cilostazol. Circulation 2004, 109, 1022–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.M.; Shin, H.K.; Kim, K.I.Y.; Lee, J.H.; Hong, K.I.W. Neuroprotective effect of cilostazol against focal cerebral ischemia via antiapoptotic action in rats. J. Pharmacol. Exp. Ther. 2002, 300, 787–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otsuki, M.; Saito, H.; Xu, X.; Sumitani, S.; Kouhara, H.; Kurabayashi, M.; Kasayama, S. Cilostazol represses vascular cell adhesion molecule-1 gene transcription via inhibiting NF-κB binding to its recognition sequence. Atherosclerosis 2001, 158, 121–128. [Google Scholar] [CrossRef]
- Rybalkin, S.D.; Rybalkina, I.; Beavo, J.A.; Bornfeldt, K.E. Cyclic nucleotide phosphodiesterase 1C promotes human arterial smooth muscle cell proliferation. Circ. Res. 2002, 90, 151–157. [Google Scholar] [CrossRef]
- Goto, S. Cilostazol: Potential mechanism of action for antithrombotic effects accompanied by a low rate of bleeding. Atheroscler. Suppl. 2005, 6, 3–11. [Google Scholar] [CrossRef]
- Gotoh, F.; Tohgi, H.; Hirai, S.; Terashi, A.; Fukuuchi, Y.; Otomo, E.; Shinohara, Y.; Itoh, E.; Matsuda, T.; Sawada, T.; et al. Cilostazol stroke prevention study: A placebo-controlled double-blind trial for secondary prevention of cerebral infarction. J. Stroke Cerebrovasc. Dis. 2000, 9, 147–157. [Google Scholar] [CrossRef]
- Huang, Y.; Cheng, Y.; Wu, J.; Li, Y.; Xu, E.; Hong, Z.; Li, Z.; Zhang, W.; Ding, M.; Gao, X.; et al. Cilostazol as an alternative to aspirin after ischaemic stroke: A randomised, double-blind, pilot study. Lancet Neurol. 2008, 7, 494–499. [Google Scholar] [CrossRef]
- Kim, B.J.; Lee, E.J.; Kwon, S.U.; Park, J.H.; Kim, Y.J.; Hong, K.S.; Wong, L.K.S.; Yu, S.; Hwang, Y.H.; Lee, J.S.; et al. Prevention of cardiovascular events in Asian patients with ischaemic stroke at high risk of cerebral haemorrhage (PICASSO): A multicentre, randomised controlled trial. Lancet Neurol. 2018, 17, 509–518. [Google Scholar] [CrossRef]
- Shinohara, Y.; Katayama, Y.; Uchiyama, S.; Yamaguchi, T.; Handa, S.; Matsuoka, K.; Ohashi, Y.; Tanahashi, N.; Yamamoto, H.; Genka, C.; et al. Cilostazol for prevention of secondary stroke (CSPS 2): An aspirin-controlled, double-blind, randomised non-inferiority trial. Lancet Neurol. 2010, 9, 959–968. [Google Scholar] [CrossRef]
- Acheson, J.; Danta, G.; Hutchinson, E.C. Controlled trial of dipyridamole in cerebral vascular disease. Br. Med. J. 1969, 1, 614–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jan, A.L. European stroke prevention study. ESPS group. Stroke 1990, 21, 1122–1130. [Google Scholar] [CrossRef] [Green Version]
- Diener, H.C.; Cunha, L.; Forbes, C.; Sivenius, J.; Smets, P.; Lowenthal, A. European stroke prevention study 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J. Neurol. Sci. 1996, 143, 1–13. [Google Scholar] [CrossRef]
- Bousser, M.G.; Eschwege, E.; Haguenau, M.; Lefaucconnier, J.M.; Thibult, N.; Touboul, D.; Touboul, P.J. “AICLA” controlled trial of aspirin and dipyridamole in the secondary prevention of athero-thrombotic cerebral ischemia. Stroke 1983, 14, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Fields, W.S. Persantine Aspirin Trial in cerebral ischemia. Part II: Endpoint results. The American-canadian co-operative study group. Stroke 1985, 16, 406–415. [Google Scholar] [CrossRef] [Green Version]
- Halkes, P.H.A. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): Randomised controlled trial. Lancet 2006, 367, 1665–1673. [Google Scholar] [CrossRef]
- Uchiyama, S.; Ikeda, Y.; Urano, Y.; Horie, Y.; Yamaguchi, T. The Japanese aggrenox (extended-release dipyridamole plus aspirin) stroke prevention versus aspirin programme (JASAP) study: A randomized, Double-blind, controlled trial. Cerebrovasc. Dis. 2011, 31, 601–613. [Google Scholar] [CrossRef]
- Diener, P.H.C.; Bogousslavsky, P.J.; Brass, P.L.M.; Cimminiello, P.C.; Csiba, P.L.; Kaste, P.M.; Leys, P.D.; Matias-Guiu, P.J.; Rupprecht, P.H.J. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): Randomised, double-blind, placebo-controlled trial. Lancet 2004, 364, 331–337. [Google Scholar] [CrossRef]
- Hankey, G.J.; Johnston, S.C.; Easton, J.D.; Hacke, W.; Mas, J.L.; Brennan, D.; Mak, K.H.; Bhatt, D.L.; Fox, K.A.A.; Topol, E.J. Effect of clopidogrel plus ASA vs. ASA early after TIA and ischaemic stroke: A substudy of the CHARISMA trial. Int. J. Stroke 2011, 6, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Benavente, O.R.; Hart, R.G.; McClure, L.A.; Szychowski, J.M.; Coffey, C.S.; Pearce, L.A. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N. Engl. J. Med. 2012, 367, 817–825. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.; Hill, M.D.; Ryckborst, K.J.; Eliasziw, M.; Demchuk, A.M.; Buchan, A.M. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): A randomised controlled pilot trial. Lancet Neurol. 2007, 6, 961–969. [Google Scholar] [CrossRef]
- He, F.; Xia, C.; Zhang, J.H.; Li, X.Q.; Zhou, Z.H.; Li, F.P.; Li, W.; Lv, Y.; Chen, H.S. Clopidogrel plus aspirin versus aspirin alone for preventing early neurological deterioration in patients with acute ischemic stroke. J. Clin. Neurosci. 2015, 22, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Lin, J.; Wang, C.; Zhang, B.; Chi, W. A comparative study of dual versus monoantiplatelet therapy in patients with acute large-artery atherosclerosis stroke. J. Stroke Cerebrovasc. Dis. 2014, 23, 1975–1981. [Google Scholar] [CrossRef]
- Candelise, L.; Landi, G.; Perrone, P.; Bracchi, M.; Brambilla, G. A randomized trial of aspirin and sulfinpyrazone in patients with TIA. Stroke 1982, 13, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Herskovits, E.; Famulari, A.; Tamaroff, L.; Gonzalez, A.M.; Vazquez, A.; Smud, R.; Fraiman, H.; Vila, J.; Matera, V. Randomised trial of pentoxifylline versus acetylsalicylic acid plus dipyridamole in preventing transient ischaemic attacks. Lancet 1981, 317, 966–968. [Google Scholar] [CrossRef]
- Culebras, A.; Rotta-Escalante, R.; Vila, J.; Domínguez, R.; Abiusi, G.; Famulari, A.; Rey, R.; Bauso-Tosselli, L.; Gori, H.; Ferrari, J.; et al. Triflusal vs aspirin for prevention of cerebral infarction: A randomized stroke study. Neurology 2004, 62, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, Y.; Nishimaru, K.; Sawada, T.; Terashi, A.; Handa, S.; Hirai, S.; Hayashi, K.; Tohgi, H.; Fukuuchi, Y.; Uchiyama, S.; et al. Sarpogrelate-aspirin comparative clinical study for efficacy and safety in secondary prevention of cerebral infarction (S-ACCESS): A randomized, double-blind, aspirin-controlled trial. Stroke 2008, 39, 1827–1833. [Google Scholar] [CrossRef] [Green Version]
- Mohr, J.P.; Thompson, J.L.P.; Lazar, R.M.; Levin, B.; Sacco, R.L.; Furie, K.L.; Kistler, J.P.; Albers, G.W.; Pettigrew, L.C.; Adams, H.P.; et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N. Engl. J. Med. 2001, 345, 1444–1451. [Google Scholar] [CrossRef] [PubMed]
- Chimowitz, M.I.; Lynn, M.J.; Howlett-Smith, H.; Stern, B.J.; Hertzberg, V.S.; Frankel, M.R.; Levine, S.R.; Chaturvedi, S.; Kasner, S.E.; Benesch, C.G.; et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N. Engl. J. Med. 2005, 352, 1305–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, R.G.; Sharma, M.; Mundl, H.; Kasner, S.E.; Bangdiwala, S.I.; Berkowitz, S.D.; Swaminathan, B.; Lavados, P.; Wang, Y.; Wang, Y.; et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N. Engl. J. Med. 2018, 378, 2191–2201. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.-C.; Sacco, R.L.; Easton, J.D.; Granger, C.B.; Bernstein, R.A.; Uchiyama, S.; Kreuzer, J.; Cronin, L.; Cotton, D.; Grauer, C.; et al. Dabigatran for prevention of stroke after embolic stroke of undetermined source. N. Engl. J. Med. 2019, 380, 1906–1917. [Google Scholar] [CrossRef] [PubMed]
- Xiang, R.-W.; Han, R.-B.; Yang, J.-Y.; Zhao, M.-Y.; Zhao, Q.-C.; Chen, H.-S.; Zhao, F.-Q.; Sun, Z.-Y.; Zhao, T.; Song, T.-Y. Comparative efficacy and safety of multiple antiplatelet therapies for secondary prevention of ischemic stroke or transient ischemic attack: A network meta-analysis. J. Neurol. Sci. 2019, 399, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Antman, E.M.; Gibson, C.M.; Montalescot, G.; Riesmeyer, J.; Weerakkody, G.; Winters, K.J.; Warmke, J.W.; McCabe, C.H.; Braunwald, E. Evaluation of prasugrel compared with clopidogrel in patients with acute coronary syndromes: Design and rationale for the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet InhibitioN with prasugrel Thrombolysis In Myocardial Infarction 38 (TRITON-TIMI 38). Am. Heart J. 2006, 152, 627–635. [Google Scholar] [CrossRef]
- Elhorany, M.; Lenck, S.; Degos, V.; Sourour, N.A.; Frasca Polara, G.; Shotar, E.; Godier, A.; Drir, M.; Mahtout, J.; Premat, K.; et al. Cangrelor and stenting in acute ischemic stroke: Monocentric case series. Clin. Neuroradiol. 2020, 1–10. [Google Scholar] [CrossRef]
- Pan, F.; Hernandez, L.; Ward, A. Cost-effectiveness of stroke treatments and secondary preventions. Expert Opin. Pharmacother. 2012, 13, 1751–1760. [Google Scholar] [CrossRef]
- Pan, Y.; Wang, A.; Liu, G.; Zhao, X.; Meng, X.; Zhao, K.; Liu, L.; Wang, C.; Claiborne Johnston, S.; Wang, Y.; et al. Cost-effectiveness of clopidogrel-aspirin versus aspirin alone for acute transient ischemic attack and minor stroke. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Rahman, H.; Khan, S.U.; Nasir, F.; Hammad, T.; Meyer, M.A.; Kaluski, E. Optimal duration of aspirin plus clopidogrel after ischemic stroke or transient ischemic attack: A systematic review and meta-analysis. Stroke 2019, 50, 947–953. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tornyos, D.; Bálint, A.; Kupó, P.; El Abdallaoui, O.E.A.; Komócsi, A. Antithrombotic Therapy for Secondary Prevention in Patients with Non-Cardioembolic Stroke or Transient Ischemic Attack: A Systematic Review. Life 2021, 11, 447. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050447
Tornyos D, Bálint A, Kupó P, El Abdallaoui OEA, Komócsi A. Antithrombotic Therapy for Secondary Prevention in Patients with Non-Cardioembolic Stroke or Transient Ischemic Attack: A Systematic Review. Life. 2021; 11(5):447. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050447
Chicago/Turabian StyleTornyos, Dániel, Alexandra Bálint, Péter Kupó, Oumaima El Alaoui El Abdallaoui, and András Komócsi. 2021. "Antithrombotic Therapy for Secondary Prevention in Patients with Non-Cardioembolic Stroke or Transient Ischemic Attack: A Systematic Review" Life 11, no. 5: 447. https://0-doi-org.brum.beds.ac.uk/10.3390/life11050447