
Evaluation of Plasma/Serum Adiponectin (an Anti-Inflammatory Factor) Levels in Adult Patients with Obstructive Sleep Apnea Syndrome: A Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Identification of Articles
2.3. Eligibility Criteria
2.4. Data Collection
2.5. Quality Evaluation
2.6. Statistical Analysis
3. Results
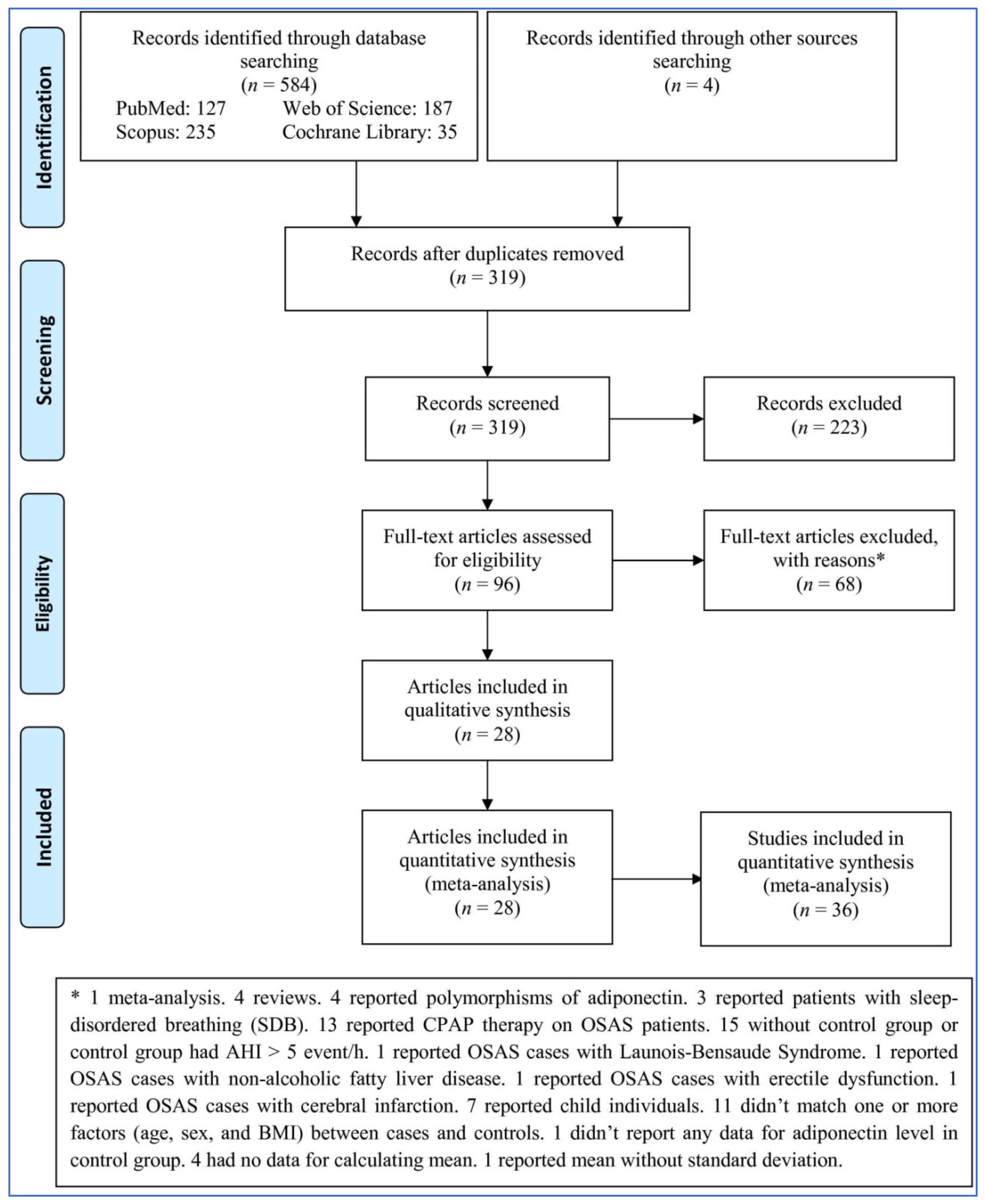
3.1. Study Selection
3.2. Characteristics
3.3. Pooled Analysis
3.4. Subgroup Analysis
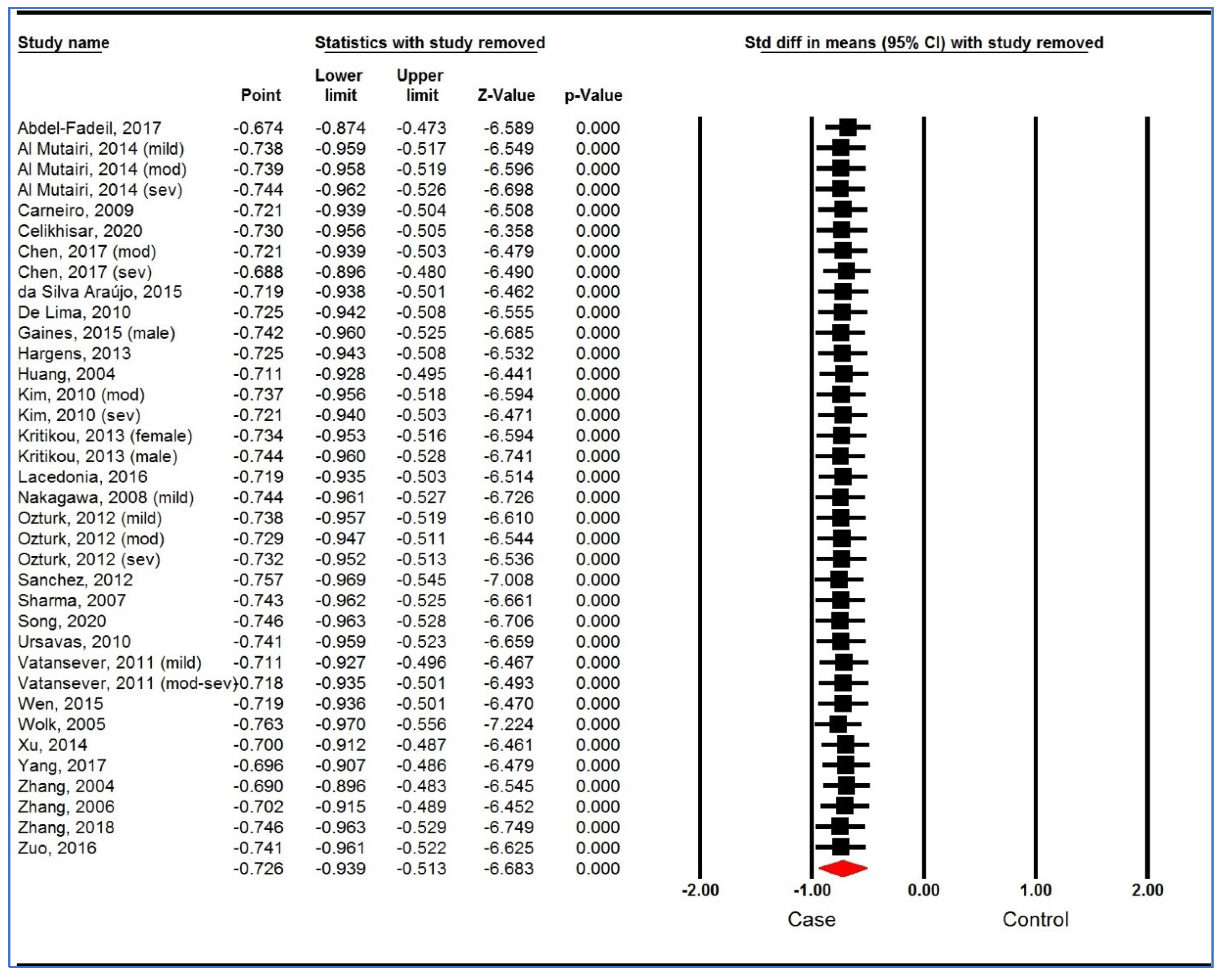
3.5. Sensitivity Analysis
3.6. Trial Sequential Analysis
3.7. Meta-Regression
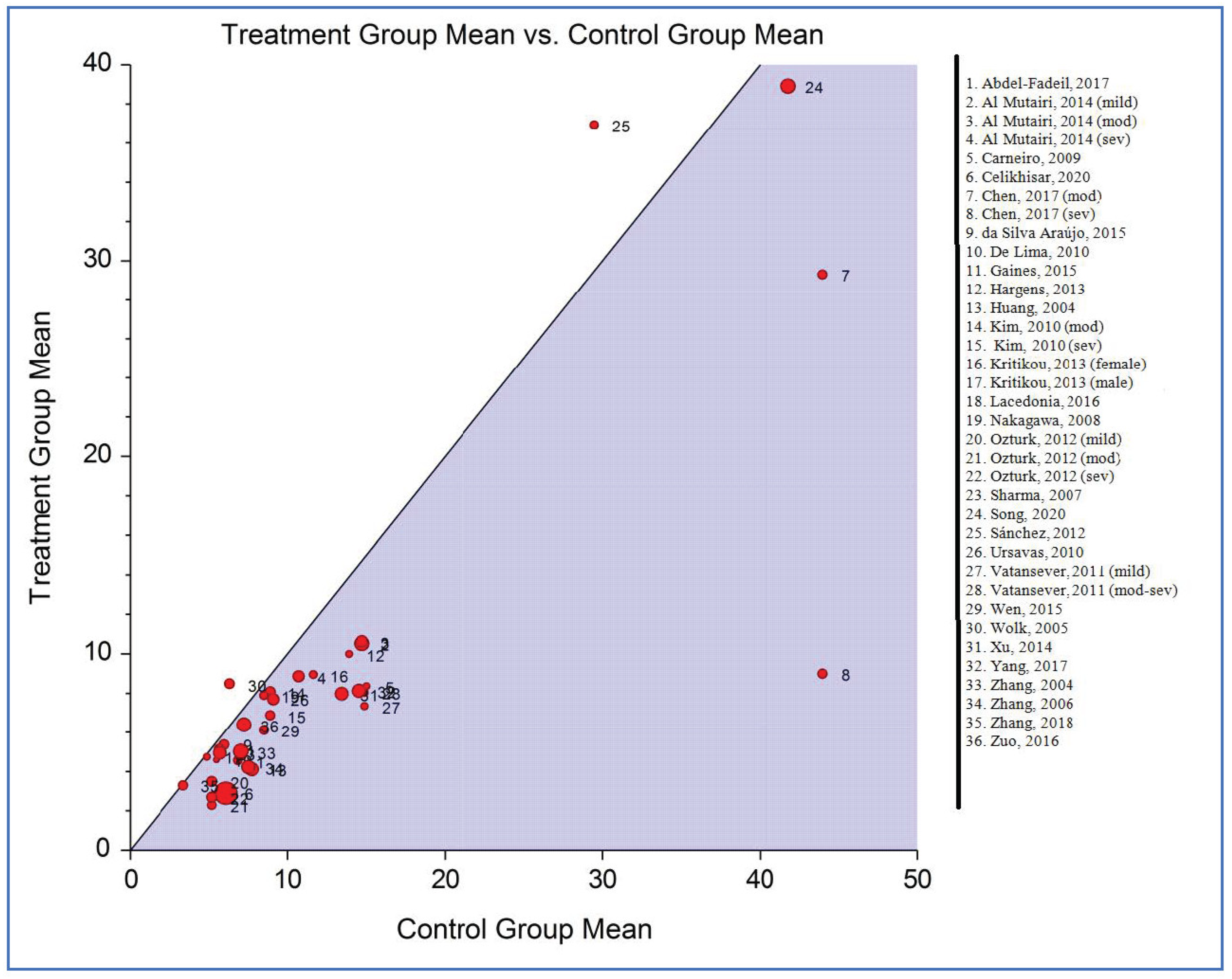
3.8. Heterogeneity
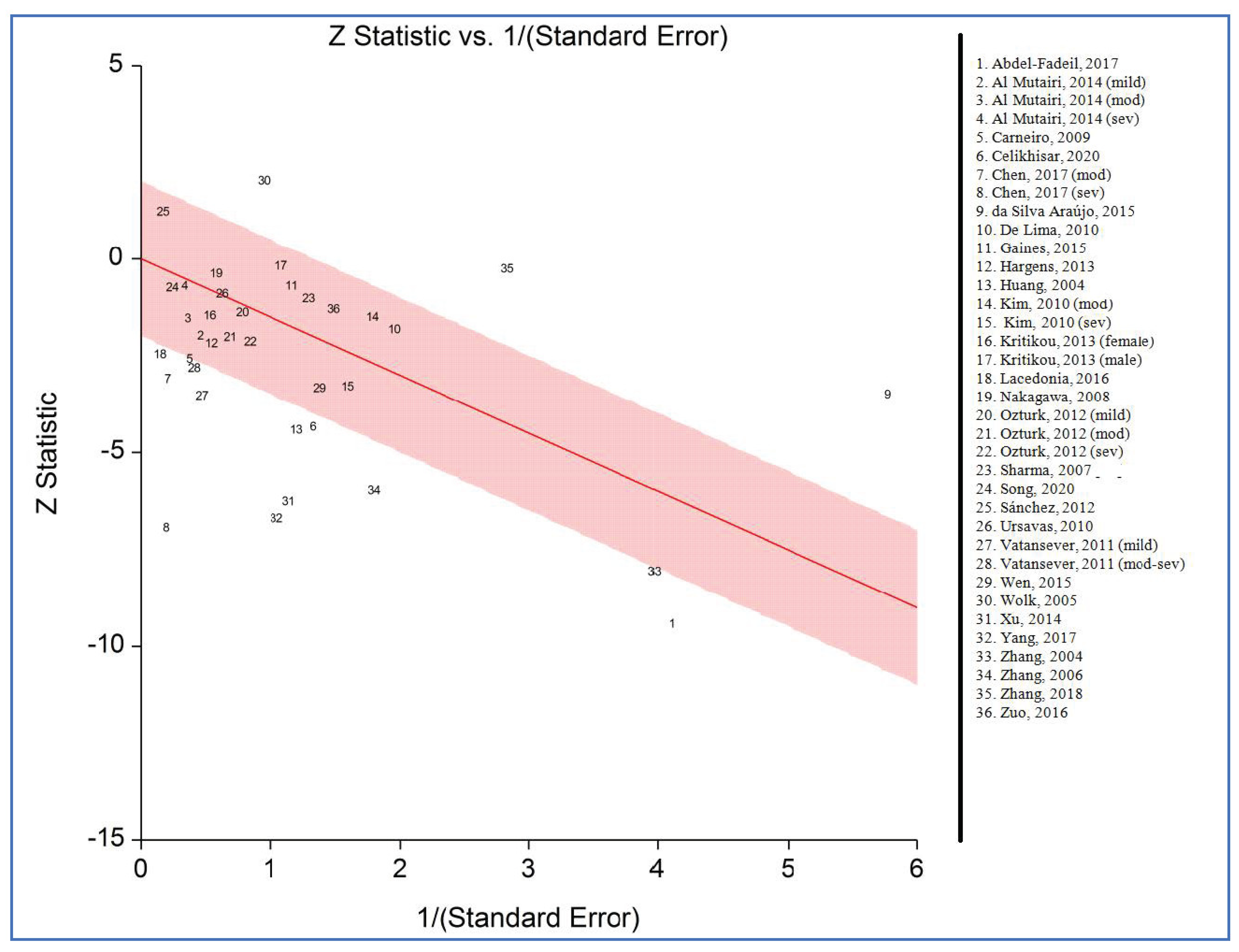
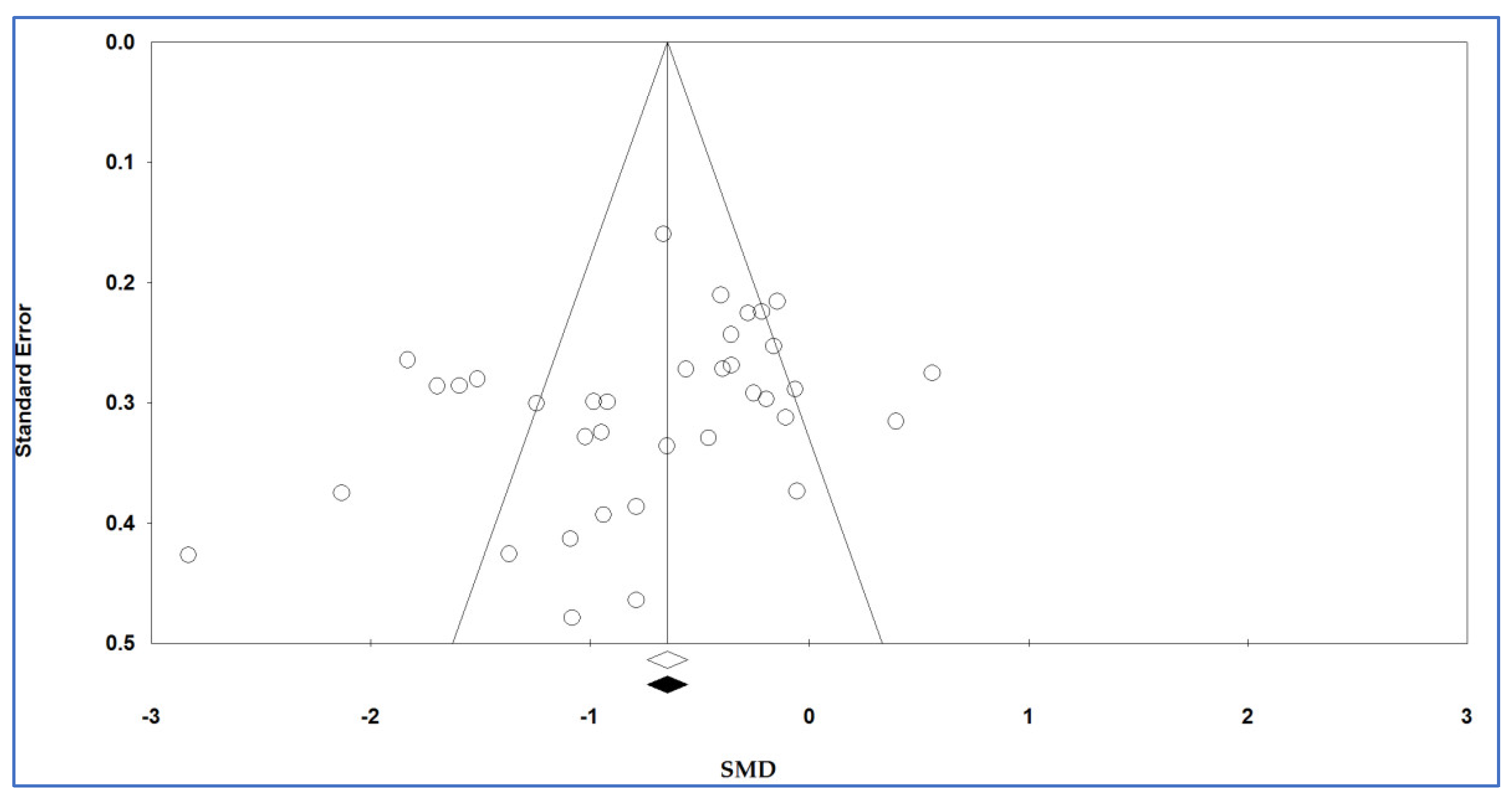
3.9. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult obstructive sleep apnea: Pathophysiology and diagnosis. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacedonia, D.; Carpagnano, G.E.; Patricelli, G.; Carone, M.; Gallo, C.; Caccavo, I.; Sabato, R.; Depalo, A.; Aliani, M.; Capozzolo, A. Prevalence of comorbidities in patients with obstructive sleep apnea syndrome, overlap syndrome and obesity hypoventilation syndrome. Clin. Respir. J. 2018, 12, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Lynch, M.K.; Elliott, L.C.; Avis, K.T.; Schwebel, D.C.; Goodin, B.R. Quality of life in youth with obstructive sleep apnea syndrome (OSAS) treated with continuous positive airway pressure (CPAP) therapy. Behav. Sleep Med. 2019, 17, 238–245. [Google Scholar] [CrossRef]
- Lacasse, Y.; Godbout, C.; Series, F. Health-related quality of life in obstructive sleep apnoea. Eur. Respir. J. 2002, 19, 499–503. [Google Scholar] [CrossRef] [Green Version]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef] [Green Version]
- Epstein, L.J.; Kristo, D.; Strollo Jr, P.; Friedman, N.; Malhotra, A.; Patil, S.; Ramar, K.; Rogers, R.; Schwab, R.; Weaver, E. Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Goyal, M.; Johnson, J. Obstructive sleep apnea diagnosis and management. Mo. Med. 2017, 114, 120. [Google Scholar]
- American Academy of Sleep Medicine Task Force. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. Sleep 1999, 22, 667–689. [Google Scholar] [CrossRef]
- Palmer, L.J.; Redline, S. Genomic approaches to understanding obstructive sleep apnea. Respir. Physiol. Neurobiol. 2003, 135, 187–205. [Google Scholar] [CrossRef]
- Tarasiuk, A.; Reuveni, H. The economic impact of obstructive sleep apnea. Curr. Opin. Pulm. Med. 2013, 19, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Pollicina, I.; Maniaci, A.; Lechien, J.R.; Iannella, G.; Vicini, C.; Cammaroto, G.; Cannavicci, A.; Magliulo, G.; Pace, A.; Cocuzza, S.; et al. Neurocognitive Performance Improvement after Obstructive Sleep Apnea Treatment: State of the Art. Behav. Sci. 2021, 11, 180. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.N.; Li, Q.Y.; Zhang, X.J. Interaction between smoking and obstructive sleep apnea: Not just participants. Chin. Med. J. 2012, 125, 3150–3156. [Google Scholar]
- Simou, E.; Britton, J.; Leonardi-Bee, J. Alcohol and the risk of sleep apnoea: A systematic review and meta-analysis. Sleep Med. 2018, 42, 38–46. [Google Scholar] [CrossRef]
- Elmasry, A.; Lindberg, E.; Berne, C.; Janson, C.; Gislason, T.; Tageldin, M.A.; Boman, G. Sleep-disordered breathing and glucose metabolism in hypertensive men: A population-based study. J. Intern. Med. 2001, 249, 153–161. [Google Scholar] [CrossRef]
- Hannon, T.S.; Rofey, D.L.; Ryan, C.M.; Clapper, D.A.; Chakravorty, S.; Arslanian, S.A. Relationships among obstructive sleep apnea, anthropometric measures, and neurocognitive functioning in adolescents with severe obesity. J. Pediatr. 2012, 160, 732–735. [Google Scholar] [CrossRef] [Green Version]
- Simpson, L.; Hillman, D.R.; Cooper, M.N.; Ward, K.L.; Hunter, M.; Cullen, S.; James, A.; Palmer, L.J.; Mukherjee, S.; Eastwood, P. High prevalence of undiagnosed obstructive sleep apnoea in the general population and methods for screening for representative controls. Sleep Breath. 2013, 17, 967–973. [Google Scholar] [CrossRef]
- Broström, A.; Sunnergren, O.; Årestedt, K.; Johansson, P.; Ulander, M.; Riegel, B.; Svanborg, E. Factors associated with undiagnosed obstructive sleep apnoea in hypertensive primary care patients. Scand. J. Prim. Health Care 2012, 30, 107–113. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Tadakamadla, S.K.; Brühl, A.; Sadeghi Bahmani, D.; Taheri, M.; Brand, S. Polymorphisms of ATP-Binding Cassette, Sub-Family A, Member 4 (rs560426 and rs481931) and Non-Syndromic Cleft Lip/Palate: A Meta-Analysis. Life 2021, 11, 58. [Google Scholar] [CrossRef]
- Zhu, M.; Bai, X. Association of LEPR Gln223Arg Polymorphism with Obstructive Sleep Apnea Syndrome: A Meta-Analysis. Crit. Rev. Eukaryot. Gene Expr. 2019, 29, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Evaluation of serum and plasma interleukin-6 levels in obstructive sleep apnea syndrome: A meta-analysis and meta-regression. Front. Immunol. 2020, 11, 1343. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Serum and Plasma Tumor Necrosis Factor Alpha Levels in Individuals with Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Life 2020, 10, 87. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.M.; Sadeghi, M.; Farokhzadeh, F.; Khazaie, H.; Brand, S.; Dürsteler, K.M.; Brühl, A.; Sadeghi-Bahmani, D. Evaluation of Blood Levels of C-Reactive Protein Marker in Obstructive Sleep Apnea: A Systematic Review, Meta-Analysis and Meta-Regression. Life 2021, 11, 362. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Sanjabi, A.; Brand, S.; Brühl, A.; Sadeghi Bahmani, D. Associations Between Morning Salivary and Blood Cortisol Concentrations in Individuals With Obstructive Sleep Apnea Syndrome: A Meta-Analysis. Front. Endocrinol. 2021, 11, 568823. [Google Scholar] [CrossRef]
- Li, X.; He, J. The Association Between Serum/Plasma Leptin Levels and Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Front. Endocrinol. 2021, 12, 696418. [Google Scholar] [CrossRef]
- Tian, Z.; Sun, H.; Kang, J.; Mu, Z.; Liang, J.; Li, M. Association between the circulating superoxide dismutase and obstructive sleep apnea: A meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. 2022, 279, 1663–1673. [Google Scholar] [CrossRef]
- Rezaei, F.; Abbasi, H.; Sadeghi, M.; Imani, M.M. The effect of obstructive sleep apnea syndrome on serum S100B and NSE levels: A systematic review and meta-analysis of observational studies. BMC Pulm. Med. 2020, 20, 31. [Google Scholar] [CrossRef]
- Maeda, K.; Okubo, K.; Shimomura, I.; Funahashi, T.; Matsuzawa, Y.; Matsubara, K. cDNA cloning and expression of a novel adipose specific collagen-like factor, apM1 (AdiPoseMost abundant Gene transcript 1). Biochem. Biophys. Res. Commun. 1996, 221, 286–289. [Google Scholar] [CrossRef]
- Yamauchi, T.; Kamon, J.; Waki, H.; Terauchi, Y.; Kubota, N.; Hara, K.; Mori, Y.; Ide, T.; Murakami, K.; Tsuboyama-Kasaoka, N. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat. Med. 2001, 7, 941–946. [Google Scholar] [CrossRef]
- Okamoto, Y.; Kihara, S.; Ouchi, N.; Nishida, M.; Arita, Y.; Kumada, M.; Ohashi, K.; Sakai, N.; Shimomura, I.; Kobayashi, H. Adiponectin reduces atherosclerosis in apolipoprotein E-deficient mice. Circulation 2002, 106, 2767–2770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, M.; Shimomura, I.; Sata, M.; Arita, Y.; Nishida, M.; Maeda, N.; Kumada, M.; Okamoto, Y.; Nagaretani, H.; Nishizawa, H. Role of adiponectin in preventing vascular stenosis: The missing link of adipo-vascular axis. J. Biol. Chem. 2002, 277, 37487–37491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigro, E.; Scudiero, O.; Monaco, M.L.; Palmieri, A.; Mazzarella, G.; Costagliola, C.; Bianco, A.; Daniele, A. New insight into adiponectin role in obesity and obesity-related diseases. BioMed Res. Int. 2014, 2014, 658913. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Fadeil, M.R.; Abedelhaffez, A.S.; Makhlouf, H.A.; Al Qirshi, G.A. Obstructive sleep apnea: Influence of hypertension on adiponectin, inflammatory markers and dyslipidemia. Pathophysiology 2017, 24, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Al Mutairi, S.; Mojiminiyi, O.A.; Al Alawi, A.; Al Rammah, T.; Abdella, N. Study of leptin and adiponectin as disease markers in subjects with obstructive sleep apnea. Dis. Markers 2014, 2014, 706314. [Google Scholar] [CrossRef] [PubMed]
- Wolk, R.; Svatikova, A.; Nelson, C.A.; Gami, A.S.; Govender, K.; Winnicki, M.; Somers, V.K. Plasma levels of adiponectin, a novel adipocyte-derived hormone, in sleep apnea. Obes. Res. 2005, 13, 186–190. [Google Scholar] [CrossRef]
- Song, F.; Zou, J.; Song, Z.; Xu, H.; Qian, Y.; Zhu, H.; Liu, S.; Guan, J.; Chen, J.; Yi, H. Association of Adipocytokines With Carotid Intima Media Thickness and Arterial Stiffness in Obstructive Sleep Apnea Patients. Front. Endocrinol. 2020, 11, 177. [Google Scholar] [CrossRef]
- Lu, M.; Fang, F.; Wang, Z.; Wei, P.; Hu, C.; Wei, Y. Association between serum/plasma levels of adiponectin and obstructive sleep apnea hypopnea syndrome: A meta-analysis. Lipids Health Dis. 2019, 18, 30. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Morgan, R.L.; Thayer, K.A.; Bero, L.; Bruce, N.; Falck-Ytter, Y.; Ghersi, D.; Guyatt, G.; Hooijmans, C.; Langendam, M.; Mandrioli, D.; et al. GRADE: Assessing the quality of evidence in environmental and occupational health. Environ. Int. 2016, 92–93, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Morgan, R.L.; Thayer, K.A.; Santesso, N.; Holloway, A.C.; Blain, R.; Eftim, S.E.; Goldstone, A.E.; Ross, P.; Guyatt, G.; Schünemann, H.J. Evaluation of the risk of bias in non-randomized studies of interventions (ROBINS-I) and the ‘target experiment’ concept in studies of exposures: Rationale and preliminary instrument development. Environ. Int. 2018, 120, 382–387. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 January 2016).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Galbraith, R. Graphical display of estimates having differing standard errors. Technometrics 1988, 30, 271–281. [Google Scholar] [CrossRef]
- Song, F. Exploring heterogeneity in meta-analysis: Is the L’Abbe plot useful? J. Clin. Epidemiol. 1999, 52, 725–730. [Google Scholar] [CrossRef]
- L’abbé, K.A.; Detsky, A.S.; O’rourke, K. Meta-analysis in clinical research. Ann. Intern. Med. 1987, 107, 224–233. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Imberger, G.; Thorlund, K.; Gluud, C.; Wetterslev, J. False-positive findings in Cochrane meta-analyses with and without application of trial sequential analysis: An empirical review. BMJ Open 2016, 6, e011890. [Google Scholar] [CrossRef]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial sequential analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.-S.; Huang, M.; Su, M.; Zhang, X.-L.; JIA, E.-Z.; Yin, K.-S. Research on the changes of serum adiponectin levels in adult male patients with obstructive sleep apnea syndrome. Acta Acad. Med. Nanjing 2004, 24, 650–653. [Google Scholar]
- Zhang, X.-L.; Yin, K.-s.; Mao, H.; Wang, H.; Yang, Y. Serum adiponectin level in patients with obstructive sleep apnea hypopnea syndrome. Chin. Med. J. 2004, 117, 1603–1606. [Google Scholar]
- Zhang, X.-L.; Yin, K.-S.; Wang, H.; Su, S. Serum adiponectin levels in adult male patients with obstructive sleep apnea hypopnea syndrome. Respiration 2006, 73, 73–77. [Google Scholar] [CrossRef]
- Xu, M.; Yuan, Y.; Cai, K. The clinical significance of serum visfatin and adiponectin in patients with obstructive sleep apnea-hypopnea syndrome combined with type 2 diabetes mellitus. Chin. J. Prev. Contr. Chron. Dis. 2014, 22, 16–18. [Google Scholar]
- Wen, J.; Zhang, D.; Ming, H.; Mao, Y.; Ma, J.; Jiang, S.; Chen, R. Detect and clinical analysis of the serum leptin and adiponectin levels in patients with obstructive sleep apnea hypopnea syndrome. Chin. Otorhinolaryngol. J. Integr. Med. 2015, 23, 104–108. [Google Scholar]
- Zuo, L.; Qi, C.; Liu, H. Serum adiponectin levels in patients with obstructive sleep apnoea and Dysglycemia. Chin. Gene Pract. 2016, 19, 912–915. [Google Scholar]
- Chen, D.-D.; Huang, J.-F.; Lin, Q.-C.; Chen, G.-P.; Zhao, J.-M. Relationship between serum adiponectin and bone mineral density in male patients with obstructive sleep apnea syndrome. Sleep Breath. 2017, 21, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Shi, M.; Dong, H.; Peng, Y. Changes of adiponectin and retinol-binding protein 4 in patients with obstructive sleep apnea-hypopnea syndrome and type 2 diabetes mellitus and their clinical significance. J. Clin. Med. Pract. 2017, 21, 31–34. [Google Scholar]
- Zhang, D.M.; Pang, X.L.; Huang, R.; Gong, F.Y.; Zhong, X.; Xiao, Y. Adiponectin, Omentin, Ghrelin, and Visfatin Levels in Obese Patients with Severe Obstructive Sleep Apnea. BioMed Res. Int. 2018, 2018, 3410135. [Google Scholar] [CrossRef] [Green Version]
- Hargens, T.A.; Guill, S.G.; Kaleth, A.S.; Nickols-Richardson, S.M.; Miller, L.E.; Zedalis, D.; Gregg, J.M.; Gwazdauskas, F.; Herbert, W.G. Insulin resistance and adipose-derived hormones in young men with untreated obstructive sleep apnea. Sleep Breath. 2013, 17, 403–409. [Google Scholar] [CrossRef]
- Kritikou, I.; Basta, M.; Vgontzas, A.N.; Pejovic, S.; Liao, D.; Tsaoussoglou, M.; Bixler, E.O.; Stefanakis, Z.; Chrousos, G.P. Sleep apnoea, sleepiness, inflammation and insulin resistance in middle-aged males and females. Eur. Respir. J. 2014, 43, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Gaines, J.; Vgontzas, A.N.; Fernandez-Mendoza, J.; Kritikou, I.; Basta, M.; Bixler, E.O. Gender differences in the association of sleep apnea and inflammation. Brain Behav. Immun. 2015, 47, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursavas, A.; Ilcol, Y.O.; Nalci, N.; Karadag, M.; Ege, E. Ghrelin, leptin, adiponectin, and resistin levels in sleep apnea syndrome: Role of obesity. Ann. Thorac. Med. 2010, 5, 161. [Google Scholar] [CrossRef] [PubMed]
- Vatansever, E.; Surmen-Gur, E.; Ursavas, A.; Karadag, M. Obstructive sleep apnea causes oxidative damage to plasma lipids and proteins and decreases adiponectin levels. Sleep Breath. 2011, 15, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, E.; Dursunoğlu, N.; Dursunoğlu, D.; Özkurt, S.; Rota, S. Evaluation of serum adiponectin levels in patients with obstructive sleep apnea syndrome. Turk Kardiyol. Dern. Ars. Turk Kardiyol. Dern. Yayin Organidir. 2012, 40, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Celikhisar, H.; Ilkhan, G.D. Alterations in Serum Adropin, Adiponectin, and Proinflammatory Cytokine Levels in OSAS. Can. Respir. J. 2020, 2020, 2571283. [Google Scholar] [CrossRef]
- Carneiro, G.; Togeiro, S.M.; Ribeiro-Filho, F.F.; Truksinas, E.; Ribeiro, A.B.; Zanella, M.T.; Tufik, S. Continuous positive airway pressure therapy improves hypoadiponectinemia in severe obese men with obstructive sleep apnea without changes in insulin resistance. Metab. Syndr. Relat. Disord. 2009, 7, 537–542. [Google Scholar] [CrossRef]
- De Lima, A.M.J.; Franco, C.M.R.; De Castro, C.M.M.B.; de Andrade Bezerra, A.; Ataíde, L., Jr.; Halpern, A. Effects of nasal continuous positive airway pressure treatment on oxidative stress and adiponectin levels in obese patients with obstructive sleep apnea. Respiration 2010, 79, 370–376. [Google Scholar] [CrossRef]
- Da Silva Araújo, L.; Fernandes, J.F.R.; Klein, M.R.S.T.; Sanjuliani, A.F. Obstructive sleep apnea is independently associated with inflammation and insulin resistance, but not with blood pressure, plasma catecholamines, and endothelial function in obese subjects. Nutrition 2015, 31, 1351–1357. [Google Scholar] [CrossRef]
- Sharma, S.; Kumpawat, S.; Goel, A.; Banga, A.; Ramakrishnan, L.; Chaturvedi, P. Obesity, and not obstructive sleep apnea, is responsible for metabolic abnormalities in a cohort with sleep-disordered breathing. Sleep Med. 2007, 8, 12–17. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Kishida, K.; Kihara, S.; Sonoda, M.; Hirata, A.; Yasui, A.; Nishizawa, H.; Nakamura, T.; Yoshida, R.; Shimomura, I. Nocturnal reduction in circulating adiponectin concentrations related to hypoxic stress in severe obstructive sleep apnea-hypopnea syndrome. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E778–E784. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, C.H.; Park, C.S.; Kim, B.G.; Kim, S.W.; Cho, J.H. Plasma levels of MCP-1 and adiponectin in obstructive sleep apnea syndrome. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 896–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-de-la-Torre, M.; Mediano, O.; Barceló, A.; Piérola, J.; de la Peña, M.; Esquinas, C.; Miro, A.; Durán-Cantolla, J.; Agustí, A.G.; Capote, F. The influence of obesity and obstructive sleep apnea on metabolic hormones. Sleep Breath. 2012, 16, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Lacedonia, D.; Nigro, E.; Matera, M.G.; Scudiero, O.; Monaco, M.L.; Polito, R.; Carpagnano, G.E.; Barbaro, M.P.F.; Mazzarella, G.; Bianco, A. Evaluation of adiponectin profile in Italian patients affected by obstructive sleep apnea syndrome. Pulm. Pharmacol. Ther. 2016, 40, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Punjabi, N.M.; Shahar, E.; Redline, S.; Gottlieb, D.J.; Givelber, R.; Resnick, H.E. Sleep-disordered breathing, glucose intolerance, and insulin resistance: The Sleep Heart Health Study. Am. J. Epidemiol. 2004, 160, 521–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zidan, M.H.; Gharraf, H.S.; Ayad, M.W.; Gaid, H.S. Study of serum adiponectin and resistin in patients with obstructive sleep apnea. Egypt. J. Chest Dis. Tuberc. 2019, 68, 303. [Google Scholar]
- Masserini, B.; Morpurgo, P.; Donadio, F.; Baldessari, C.; Bossi, R.; Beck-Peccoz, P.; Orsi, E. Reduced levels of adiponectin in sleep apnea syndrome. J. Endocrinol. Investig. 2006, 29, 700–705. [Google Scholar] [CrossRef]
- Qi, L.; Doria, A.; Manson, J.E.; Meigs, J.B.; Hunter, D.; Mantzoros, C.S.; Hu, F.B. Adiponectin genetic variability, plasma adiponectin, and cardiovascular risk in patients with type 2 diabetes. Diabetes 2006, 55, 1512–1516. [Google Scholar] [CrossRef] [Green Version]
- Hui, X.; Lam, K.S.; Vanhoutte, P.M.; Xu, A. Adiponectin and cardiovascular health: An update. Br. J. Pharmacol. 2012, 165, 574–590. [Google Scholar] [CrossRef] [Green Version]
- Zoccali, C.; Mallamaci, F.; Tripepi, G.; Benedetto, F.A.; Cutrupi, S.; Parlongo, S.; Malatino, L.S.; Bonanno, G.; Seminara, G.; Rapisarda, F. Adiponectin, metabolic risk factors, and cardiovascular events among patients with end-stage renal disease. J. Am. Soc. Nephrol. 2002, 13, 134–141. [Google Scholar] [CrossRef]
- Ouchi, N.; Kihara, S.; Arita, Y.; Okamoto, Y.; Maeda, K.; Kuriyama, H.; Hotta, K.; Nishida, M.; Takahashi, M.; Muraguchi, M. Adiponectin, an adipocyte-derived plasma protein, inhibits endothelial NF-κB signaling through a cAMP-dependent pathway. Circulation 2000, 102, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, R.S.; Funahashi, T.; Hanson, R.L.; Matsuzawa, Y.; Tanaka, S.; Tataranni, P.A.; Knowler, W.C.; Krakoff, J. Adiponectin and development of type 2 diabetes in the Pima Indian population. Lancet 2002, 360, 57–58. [Google Scholar] [CrossRef]
- Leung, R.S.; Douglas Bradley, T. Sleep apnea and cardiovascular disease. Am. J. Respir. Crit. Care Med. 2001, 164, 2147–2165. [Google Scholar] [CrossRef]
- Wolk, R.; Kara, T.; Somers, V.K. Sleep-disordered breathing and cardiovascular disease. Circulation 2003, 108, 9–12. [Google Scholar] [CrossRef] [PubMed]
- López-Jaramillo, P.; Gómez-Arbeláez, D.; López-López, J.; López-López, C.; Martínez-Ortega, J.; Gómez-Rodríguez, A.; Triana-Cubillos, S. The role of leptin/adiponectin ratio in metabolic syndrome and diabetes. Horm. Mol. Biol. Clin. Investig. 2014, 18, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.; Lin, N.; Xing, Z.; Weng, H.; Zhang, H. Association between the level of circulating adiponectin and prediabetes: A meta-analysis. J. Diabetes Investig. 2015, 6, 416–429. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Publication Year | Country | Ethnicity | Adiponectin Source | Assay Approach | NOS |
|---|---|---|---|---|---|
| Huang, 2004 [52] | China | Asian | Serum | RIA | 6 |
| Zhang, 2004 [53] | China | Asian | Serum | RIA | 6 |
| Wolk, 2005 [36] | USA | Mixed | Serum | RIA | 7 |
| Zhang, 2006 [54] | China | Asian | Plasma | RIA | 6 |
| Sharma, 2007 [71] | India | Asian | Plasma | ELISA | 7 |
| Nakagawa, 2008 [72] | Japan | Asian | Serum | ELISA | 7 |
| Carneiro, 2009 [68] | Brazil | Mixed | Plasma | RIA | 7 |
| Ursavas, 2010 [64] | Turkey | Caucasian | Serum | RIA | 8 |
| De Lima, 2010 [69] | Brazil | Mixed | Plasma | ELISA | 7 |
| Kim, 2010 [73] | Korea | Asian | Plasma | RIA | 7 |
| Vatansever, 2011 [65] | Turkey | Caucasian | Serum | RIA | 7 |
| Öztürk, 2012 [66] | Turkey | Caucasian | Serum | ELISA | 6 |
| Sánchez, 2012 [74] | Spain | Caucasian | Plasma | RIA | 7 |
| Kritikou, 2013 [62] | USA | Mixed | Serum | ELISA | 7 |
| Hargens, 2013 [61] | USA | Mixed | Serum | ELISA | 8 |
| Al Mutairi, 2014 [35] | Kuwait | Caucasian | Plasma | ELISA | 7 |
| Xu, 2014 [55] | China | Asian | Serum | ELISA | 7 |
| Gaines, 2015 [63] | USA | Mixed | Plasma | ELISA | 7 |
| da Silva Araújo, 2015 [70] | Brazil | Mixed | Plasma | ELISA | 7 |
| Wen, 2015 [56] | China | Asian | Serum | ELISA | 7 |
| Lacedonia, 2016 [75] | Italy | Caucasian | Serum | ELISA | 7 |
| Zuo, 2016 [57] | China | Asian | Serum | ELISA | 6 |
| Chen, 2017 [58] | China | Asian | Serum | ELISA | 8 |
| Abdel-Fadeil, 2017 [34] | Egypt | Caucasian | Serum | ELISA | 7 |
| Yang, 2017 [59] | China | Asian | Serum | ELISA | 7 |
| Zhang, 2018 [60] | China | Asian | Plasma | ELISA | 8 |
| Song, 2020 [37] | China | Asian | Serum | ELISA | 8 |
| Celikhisar, 2020 [67] | Turkey | Caucasian | Serum | ELISA | 8 |
| First Author, Publication Year | Number: (Case/Control) | Adiponectin (Mean ± SD) | Age (Mean ± SD), Year | BMI (Mean ± SD), kg/m2 | AHI (Mean ± SD), Events/h | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | Case | Control | Case | Control | Case | Control | |
| Huang, 2004 [52] | 69 | 15 | 4.12 ± 2.49 | 7.74 ± 4.42 | 51.71 ± 12.37 | 56.37 ± 11.49 | 26.35 ± 2.60 | 26.02 ± 1.78 | 39.28 ± 22.80 | 3.67 ± 1.38 |
| Zhang, 2004 [53] | 71 | 26 | 5.03 ± 1.01 | 7.04 ± 1.31 | 51.4 ± 11.8 | 49.2 ± 10.1 | 26.7 ± 2.1 | 27.8 ± 1.9 | - | - |
| Wolk, 2005 [36] | 26 | 29 | 8.49 ± 4.69 | 6.32 ± 2.96 | 46 ± 5.10 | 46 ± 10.77 | 31 ± 5.10 | 31 ± 5.39 | 44 ± 20.40 | 3.0 ± 2.15 |
| Zhang, 2006 [54] | 20 | 66 | 4.23 ± 2.04 | 7.52 ± 2.21 | 50.7 ± 12.9 | 49.6 ± 9.2 | 26.8 ± 2.5 | 25.6 ± 1.8 | 36.8 ± 21.4 | 2.4 ± 1.8 |
| Sharma, 2007 [71] | 40 | 40 | 4.96 ± 3.21 | 5.71 ± 3.67 | 42.3 ± 8.3 | 43.3 ± 7.8 | 29.8 ± 3.3 | 29.1 ± 2.3 | 32.19 ± 9.94 | 1.35 ± 0.61 |
| Nakagawa, 2008 [72] | 24 | 18 | 7.9 ± 5.6 | 8.5 ± 5.5 | 45.9 ± 12.6 | 43.8 ± 12.2 | 26.7 ± 5.8 | 23.8 ± 4.0 | 8.9 ± 2.7 | 2.4 ± 1.5 |
| Carneiro, 2009 [68] | 16 | 13 | 8.7 ± 4.72 | 15.0 ± 9.19 | 40.1 ± 2.8 | 38.8 ± 3.3 | 46.9 ± 2.0 | 42.8 ± 1.3 | 65.7 ± 9.9 | 3.2 ± 0.5 |
| Ursavas, 2010 [64] | 55 | 15 | 7.7 ± 5.2 | 9.1 ± 6.6 | 51.1 ± 8.9 | 48.4 ± 36.65 | 32.5 ± 64.11 | 31.6 ± 7.0 | 43.5 ± 26.7 | 2.8 ± 1.5 |
| De Lima, 2010 [69] | 10 | 10 | 4.6 ± 1.58 | 5. 5± 0.32 | 57 ± 33.18 | 56.8 ± 4.7 | 34.1 ± 1.3 | 33.1 ± 7.9 | 29.5 ± 11.69 | 3.6 ± 0.32 |
| Kim, 2010 (sev) [73] | 28 | 22 | 6.88 ± 1.78 | 8.90 ± 2.63 | 42 ± 10.77 | 26 ± 6.91 | 28.69 ± 4.05 | 23.88 ± 2.30 | 52.71 ± 22.23 | 1.25 ± 1.25 |
| Kim, 2010 (mod) [73] | 37 | 22 | 8.08 ± 1.66 | 8.90 ± 2.63 | 38 ± 15.04 | 26 ± 6.91 | 24.43 ± 2.45 | 23.88 ± 2.30 | 14.40 ± 4.07 | 1.25 ± 1.25 |
| Vatansever, 2011 (mod-sev) [65] | 9 | 24 | 8.04 ± 6.55 | 14.87 ± 6.17 | 50 ± 27.11 | 47 ± 39.19 | 29.3 ± 4.12 | 28.4 ± 2.45 | 54.4 ± 66.79 | 2.05 ± 1.32 |
| Vatansever, 2011 (mild) [65] | 9 | 24 | 7.35 ± 2.7 | 14.87 ± 6.17 | 48 ± 27 | 47 ± 39.19 | 27.6 ± 1.8 | 28.4 ± 2.45 | 8.0 ± 2.52 | 2.05 ± 1.32 |
| Sánchez, 2012 [74] | 21 | 20 | 36.94 ± 21.42 | 29.47 ± 15.88 | 49.33 ± 10.71 | 42.9 ± 9.16 | 25.02 ± 1.22 | 24.71 ± 2.39 | 41.45 ± 18.3 | 2.87 ± 1.51 |
| Öztürk, 2012 (sev) [66] | 25 | 32 | 2.7 ± 3.2 | 5.2 ± 5.2 | 50.0 ± 11.7 | 48.3 ± 10.8 | 34.0 ± 5.5 | 31.3 ± 5.6 | 61.6 ± 20.4 | 1.8 ± 1.4 |
| Öztürk, 2012 (mod) [66] | 12 | 32 | 2.3 ± 1.2 | 5.2 ± 5.2 | 58.7 ± 8.6 | 48.3 ± 10.8 | 32.7 ± 5.8 | 31.3 ± 5.6 | 23.4 ± 4.6 | 1.8 ± 1.4 |
| Öztürk, 2012 (mild) [66] | 25 | 32 | 3.5 ± 4.2 | 5.2 ± 5.2 | 48.8 ± 10.6 | 48.3 ± 10.8 | 32.1 ± 6.6 | 31.3 ± 5.6 | 9.0 ± 2.6 | 1.8 ± 1.4 |
| Kritikou, 2013 (female) [62] | 20 | 18 | 8.96 ± 5.48 | 11.63 ± 6.17 | 57.28 ± 6.00 | 54.21 ± 6.61 | 31.52 ± 1.54 | 30.36 ± 2.75 | 33.94 ± 18.78 | 1.69 ± 1.61 |
| Kritikou, 2013 (male) [62] | 16 | 13 | 4.75 ± 2.41 | 4.89 ± 2.55 | 53.87 ± 6.76 | 52.39 ± 6.23 | 27.09 ± 2.60 | 26.60 ± 2.65 | 42.42 ± 22.51 | 3.03 ± 1.98 |
| Hargens, 2013 [61] | 12 | 18 | 10.0 ± 2.77 | 13.9 ± 5.94 | 22.8 ± 2.77 | 22.5 ± 2.97 | 32.4 ± 3.46 | 31.6 ± 4.67 | 25.4 ± 18.71 | 2.2 ± 1.27 |
| Al Mutairi, 2014 (sev) [35] | 25 | 42 | 8.87 ± 7.41 | 14.70 ± 13.01 | 50.0 ± 14.8 | 55.8 ± 16.3 | 44.4 ± 16.8 | 40.5 ± 11.9 | 48.9 ± 13.1 | 2.6 ± 1.6 |
| Al Mutairi, 2014 (mod) [35] | 29 | 42 | 10.64 ± 8.36 | 14.70 ± 13.01 | 53.0 ± 16.3 | 55.8 ± 16.3 | 49.8 ± 13.9 | 40.5 ± 11.9 | 18.0 ± 6.9 | 2.6 ± 1.6 |
| Al Mutairi, 2014 (mild) [35] | 51 | 42 | 10.53 ± 7.41 | 14.70 ± 13.01 | 49.1 ± 17.0 | 55.8 ± 16.3 | 43.3 ± 10.5 | 40.5 ± 11.9 | 10.3 ± 3.8 | 2.6 ± 1.6 |
| Xu, 2014 [55] | 62 | 20 | 7.98 ± 3.74 | 13.43 ± 2.04 | 50.8 ± 11.7 | 51.3 ± 10.5 | - | - | 18.03 ± 5.10 | 2.14 ± 0.89 |
| Gaines, 2015 [63] | 47 | 15 | 5.13 ± 2.88 | 5.70 ± 2.94 | 53.46 ± 0.86 | 52.70 ± 1.52 | 27.79 ± 0.35 | 26.50 ± 0.63 | 22.94 ±2.47 | 2.26 ± 4.37 |
| da Silva Araújo, 2015 [70] | 33 | 20 | 5.38 ± 0.44 | 5.98 ± 0.82 | 39.60 ± 1.48 | 32.50 ± 2.09 | 34.39 ± 0.51 | 34.51 ± 0.66 | 20.16 ± 3.57 | 2.55 ± 0.35 |
| Wen, 2015 [56] | 33 | 15 | 6.13 ± 1.16 | 8.51 ± 3.84 | 48.5 ± 10.06 | 46 ± 10.4 | 27.4 ± 5.0 | 27 ± 4.6 | 41.3 ± 3.6 | 2.8 ± 0.4 |
| Lacedonia, 2016 [75] | 10 | 10 | 63.43 ± 11.53 | 80.10 ± 18.50 | 62.80 ± 8.19 | 58.80 ± 17.55 | 27.29 ± 2.41 | 27.58 ± 1.40 | - | - |
| Zuo, 2016 [57] | 59 | 30 | 6.4 ± 3.25 | 7.24 ± 2.42 | 47.3 ± 14.6 | 43.3 ± 7.8 | 27.3 ± 5.0 | 26.1 ± 1.7 | 20.6 ± 26.3 | - |
| Chen, 2017 (sev) [58] | 35 | 15 | 9 ± 13.35 | 43.98 ± 22.13 | 42.06 ± 11.75 | 41.33 ± 12.45 | 26.12 ± 3.49 | 25.51 ± 2.17 | 72.47 ± 15.73 | 4.86 ± 2.31 |
| Chen, 2017 (mod) [58] | 34 | 15 | 29.31 ± 11.57 | 43.98 ± 22.13 | 43.32 ± 11.95 | 41.33 ± 12.45 | 25.35 ± 2.07 | 25.51 ± 2.17 | 32.12 ± 10.21 | 4.86 ± 2.31 |
| Abdel-Fadeil, 2017 [34] | 22 | 22 | 4.57 ± 0.98 | 6.85 ± 0.58 | 49.92 ± 2.10 | 47.55 ± 2.35 | 36.00 ± 1.10 | 36.62 ± 1.14 | 32.17 ± 20.59 | 3.72 ± 1.69 |
| Yang, 2017 [59] | 20 | 66 | 8.13 ± 2.28 | 14.52 ± 4.10 | 50.12 ± 11.25 | 49.30 ± 10.70 | 24.61 ± 3.80 | 23.37 ± 3.55 | 37.87 ± 14.90 | - |
| Zhang, 2018 [60] | 30 | 20 | 3.30 ± 1.10 | 3.38 ± 1.39 | 40.73 ± 8.90 | 36.10 ± 13.67 | 28.85 ± 2.62 | 27.55 ± 2.97 | 61.48 ± 15.00 | 1.93 ± 1.38 |
| Song, 2020 [37] | 62 | 33 | 38.92 ± 18.51 | 41.80 ± 21.63 | 40.38 ± 9.50 | 37.51 ± 10.87 | 24.18 ± 1.55 | 23.30 ± 3.07 | 29.11 ± 20.45 | 1.78 ± 1.41 |
| Celikhisar, 2020 [67] | 84 | 82 | 2.9 ± 3.6 | 6.1 ± 5.8 | 50.9 ± 5.7 | 49.3 ± 5.8 | 32.4 ± 6.0 | 30.6 ± 5.6 | 27.4 ± 18.6 | 1.8 ± 1.4 |
| Subgroup | Variable (N) | SDM | 95% CI | Z | p-Value | I2, % | Ph | |
|---|---|---|---|---|---|---|---|---|
| Min | Max | |||||||
| Ethnicity | Asian (15) | −0.91 | −1.27 | −0.56 | 5.07 | <0.00001 | 84 | <0.00001 |
| Caucasian (13) | −0.63 | −0.94 | −0.32 | 4.00 | <0.0001 | 74 | <0.00001 | |
| Mixed (8) | −0.41 | −0.82 | −0.01 | 2.01 | 0.04 | 65 | 0.006 | |
| Country (region) | China (11) | −1.10 | −1.54 | −0.67 | 4.98 | <0.00001 | 85 | <0.00001 |
| Turkey (7) | −0.61 | −0.81 | −0.42 | 6.09 | <0.00001 | 10 | 0.35 | |
| USA (5) | −0.15 | −0.60 | 0.30 | 0.65 | 0.52 | 59 | 0.04 | |
| Brazil (3) | −0.91 | −1.33 | −0.49 | 4.27 | <0.0001 | 0 | 0.93 | |
| Adiponectin Source | Serum (23) | −0.85 | −1.15 | −0.55 | 5.58 | <0.00001 | 82 | <0.00001 |
| Plasma (13) | −0.47 | −0.73 | −0.22 | 3.61 | 0.0003 | 64 | 0.0009 | |
| Assay approach | ELISA (25) | −0.69 | −0.92 | −0.45 | 5.81 | <0.00001 | 75 | <0.00001 |
| RIA (11) | −0.76 | −1.25 | −0.28 | 3.08 | 0.002 | 58 | <0.00001 | |
| Sample size | ≥50 (23) | −0.69 | −0.94 | −0.43 | 5.24 | <0.00001 | 82 | <0.00001 |
| <50 (13) | −0.77 | −1.17 | −0.37 | 3.75 | 0.0002 | 74 | <0.00001 | |
| Publication year | ≥2015 (14) | −0.89 | −1.25 | −0.53 | 4.83 | <0.00001 | 82 | <0.00001 |
| <2015 (22) | −0.60 | −0.87 | −0.34 | 4.43 | <0.00001 | 78 | <0.00001 | |
| Mean AHI in cases, event/h | ≥30 (19) | −0.76 | −1.11 | −0.41 | 4.24 | <0.0001 | 84 | <0.00001 |
| 15–30 (10) | −0.61 | −0.87 | −0.34 | 4.43 | <0.00001 | 61 | 0.006 | |
| 5–15 (5) | −0.42 | −0.66 | −0.18 | 3.40 | 0.0007 | 30 | 0.22 | |
| Mean BMI, kg/m2 | BMI ≥ 30 (15) | −0.52 | −0.80 | −0.24 | 3.64 | 0.0003 | 75 | <0.00001 |
| BMI < 30 (21) | −0.87 | −1.16 | −0.57 | 5.69 | <0.00001 | 81 | <0.00001 | |
| Mean age, y | Age ≥ 50 (18) | −0.79 | −1.06 | −0.53 | 5.86 | <0.00001 | 75 | <0.00001 |
| Age < 50 (18) | −0.64 | −0.96 | −0.31 | 3.87 | 0.0001 | 81 | <0.00001 | |
| Variable (N) | Point Estimate | Standard Error | Lower Limit | Upper Limit | Z-Value | p-Value |
|---|---|---|---|---|---|---|
| Publication year | −0.00627 | 0.02642 | −0.05805 | 0.04552 | −0.23716 | 0.81254 |
| Sample size | −0.00006 | 0.00388 | −0.00825 | 0.00694 | −0.169166 | 0.86567 |
| Mean AHI for cases, event/h | −0.00431 | 0.00651 | −0.01708 | 0.00845 | −0.66203 | 0.50795 |
| Mean BMI for cases, kg/m2 | 0.01046 | 0.017066 | −0.02297 | 0.04389 | 0.61354 | 0.53952 |
| Mean BMI for control, kg/m2 | 0.00337 | 0.02080 | −0.03740 | 0.04414 | 0.16182 | 0.87145 |
| Mean age for cases, y | −0.00344 | 0.01438 | −0.03163 | 0.02474 | −0.23942 | 0.81078 |
| Mean age for controls, y | −0.00469 | 0.01294 | −0.3005 | 0.02067 | −0.36255 | 0.71694 |
| Value | Studies Trimmed | Fixed-Effects | Random-Effects | Q Value | ||||
|---|---|---|---|---|---|---|---|---|
| Point Estimate | Lower Limit | Upper Limit | Point Estimate | Lower Limit | Upper Limit | |||
| Observed | - | −0.64667 | −0.74011 | −0.55323 | −0.72636 | −0.93939 | −0.51334 | 174.28741 |
| Adjusted | 0 | −0.64667 | −0.74011 | −0.55323 | −0.72636 | −0.93939 | −0.51334 | 174.28741 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najafi, A.; Mohammadi, I.; Sadeghi, M.; Brühl, A.B.; Sadeghi-Bahmani, D.; Brand, S. Evaluation of Plasma/Serum Adiponectin (an Anti-Inflammatory Factor) Levels in Adult Patients with Obstructive Sleep Apnea Syndrome: A Systematic Review and Meta-Analysis. Life 2022, 12, 738. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050738
Najafi A, Mohammadi I, Sadeghi M, Brühl AB, Sadeghi-Bahmani D, Brand S. Evaluation of Plasma/Serum Adiponectin (an Anti-Inflammatory Factor) Levels in Adult Patients with Obstructive Sleep Apnea Syndrome: A Systematic Review and Meta-Analysis. Life. 2022; 12(5):738. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050738
Chicago/Turabian StyleNajafi, Amir, Iman Mohammadi, Masoud Sadeghi, Annette Beatrix Brühl, Dena Sadeghi-Bahmani, and Serge Brand. 2022. "Evaluation of Plasma/Serum Adiponectin (an Anti-Inflammatory Factor) Levels in Adult Patients with Obstructive Sleep Apnea Syndrome: A Systematic Review and Meta-Analysis" Life 12, no. 5: 738. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050738