
Histomorphometry of Ossification in Functionalised Ceramics with Tripeptide Arg-Gly-Asp (RGD): An In Vivo Study

 ,
,  ,
,
Abstract
:1. Introduction
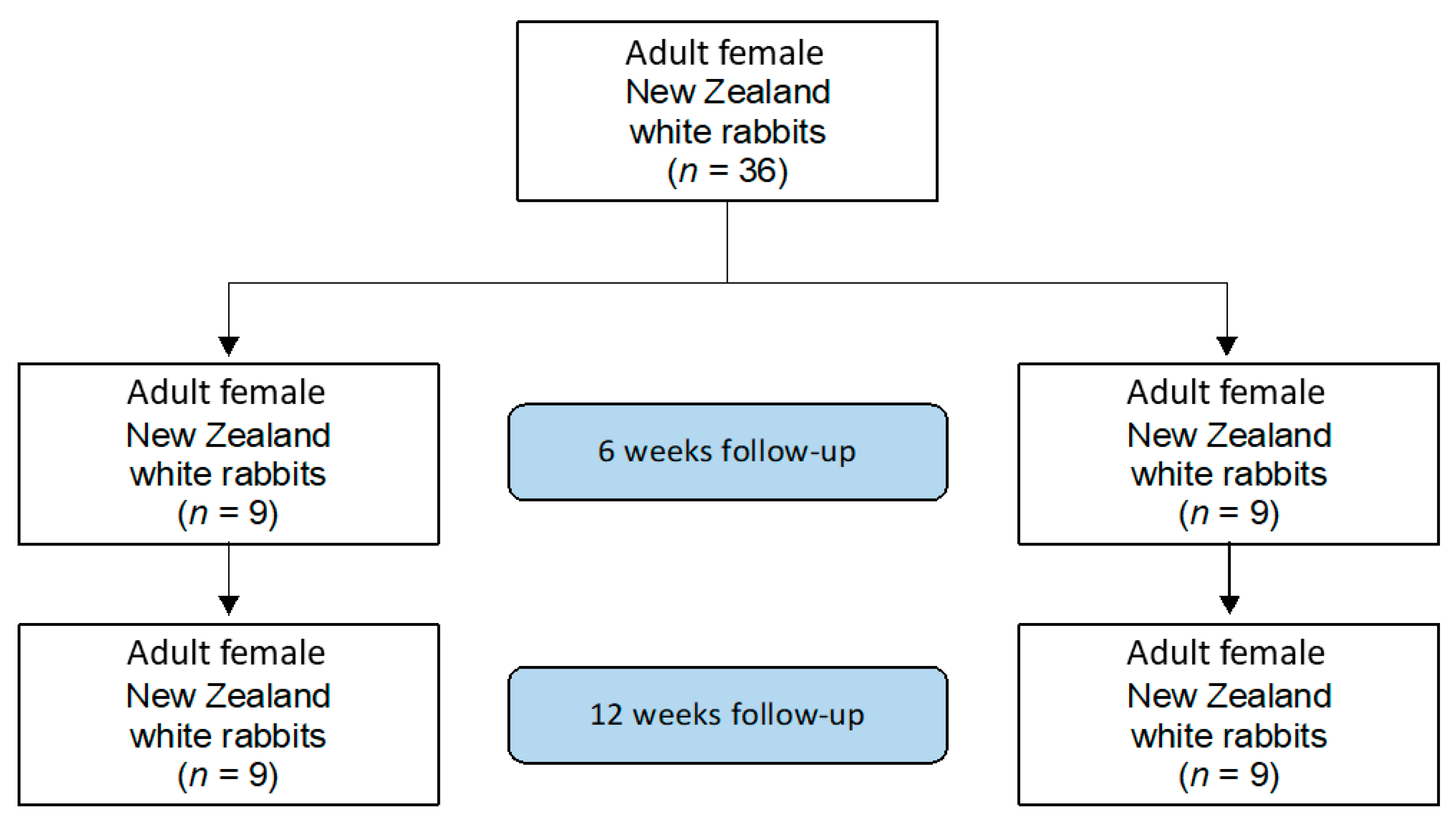
2. Material and Methods
2.1. Sample Preparation
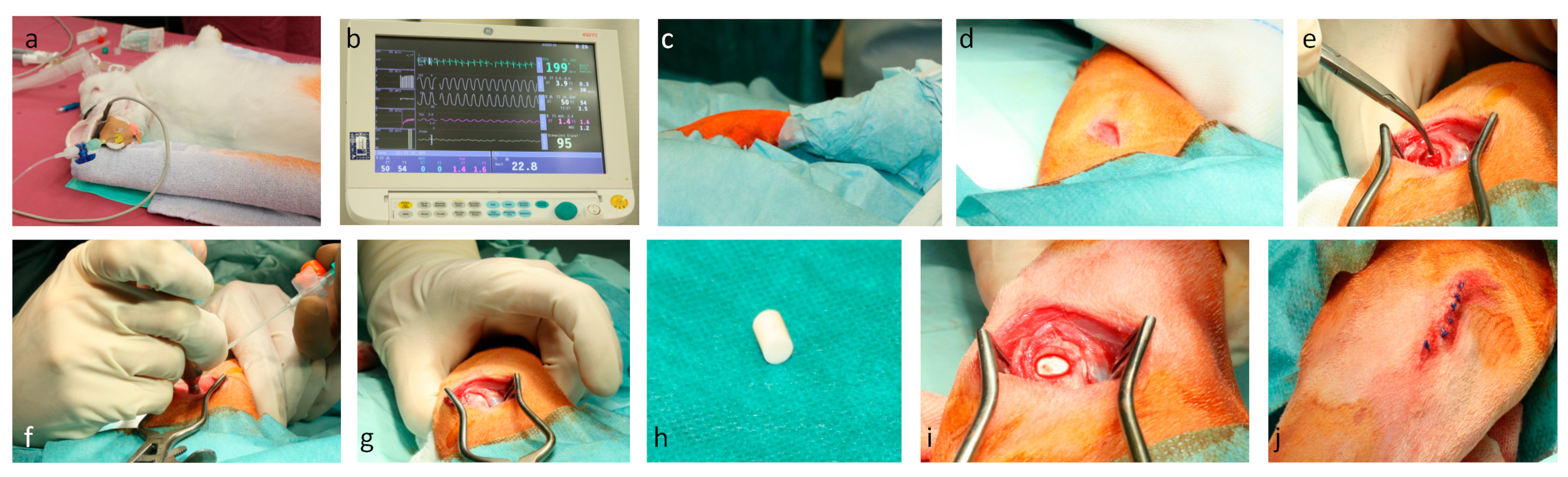
2.2. Surgical Procedure
2.3. Sample Preparation
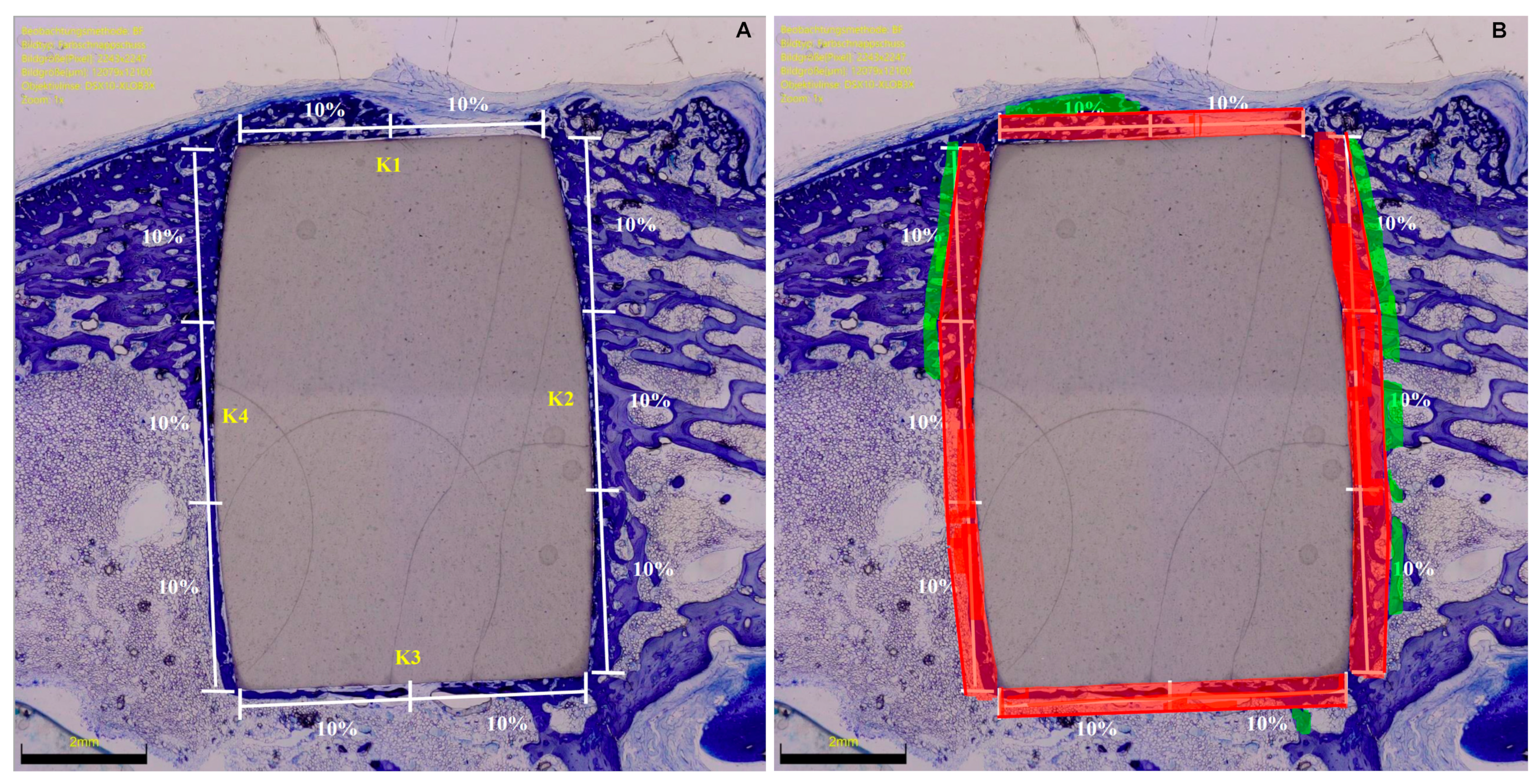
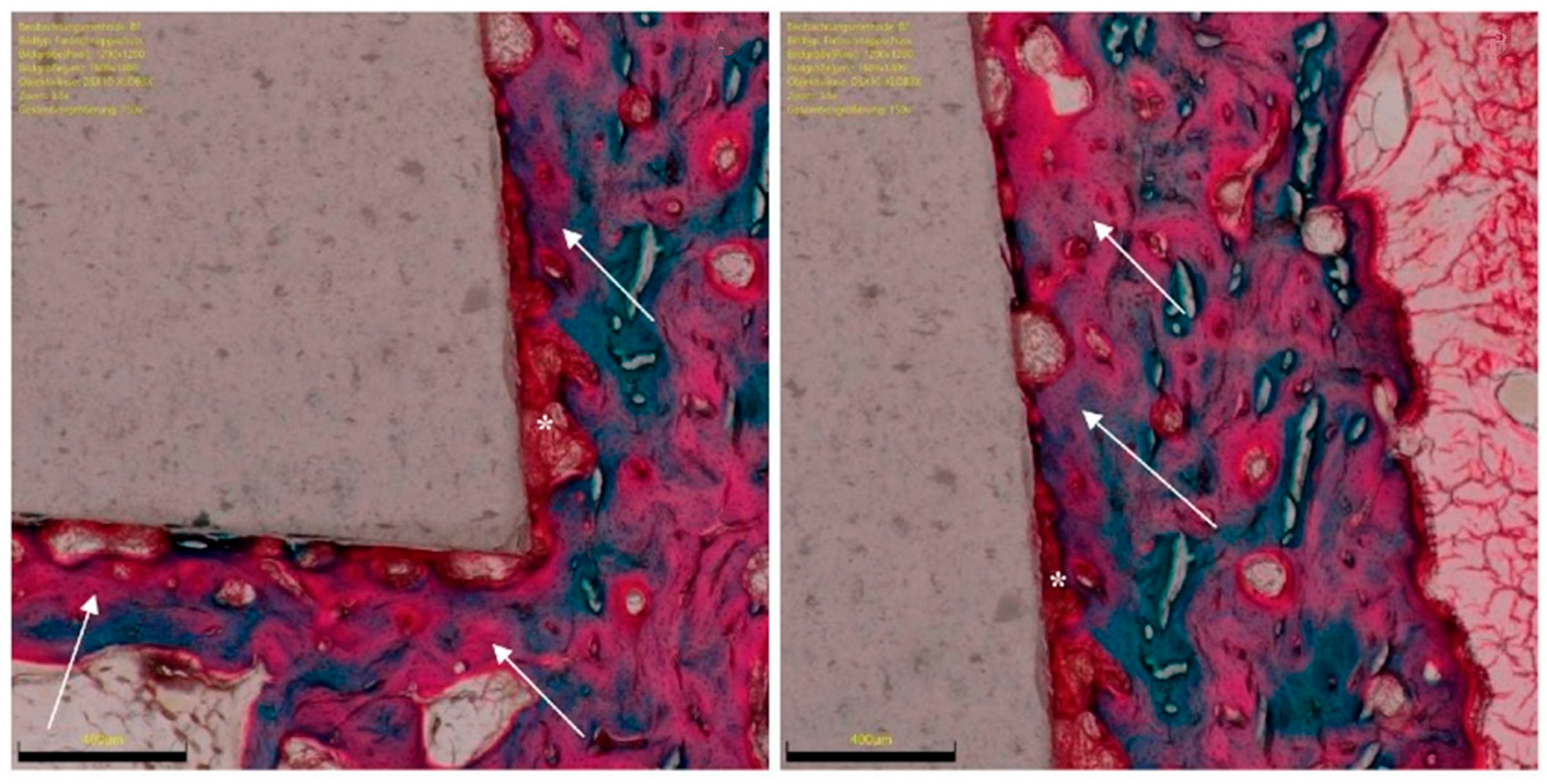
2.4. Histomorphometry
2.5. Outcomes of Interests
2.6. Statistical Analysis
3. Results
3.1. Ossification from 6- to 12-Weeks Follow-up of the RGD Enhanced Implants
3.2. Comparison of RGD Enhanced Versus Titanium Implants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Endpoint | 6 Weeks | 12 Weeks | |
|---|---|---|---|
| Lateral | BIC (%) | 3.1 ± 4.1 | 4.9 ± 4.6 |
| OIC (%) | 0 | −1.4 ± 0.8 | |
| Distal | BIC (%) | 11.5 ± 2.3 | 14.1 ± 8.1 |
| OIC (%) | 1.5 ± 3.0 | 5.4 ± 4.1 | |
| Medial | BIC (%) | 5.3 ± 3.4 | 7.5 ± 2.1 |
| OIC (%) | −0.3 ± 0.7 | 3.3 ± 2.0 | |
| Proximal | BIC (%) | 10.9 ± 9.1 | 12.1 ± 3.7 |
| OIC (%) | 5.0 ± 0.3 | 4.9 ± 1.9 | |
| Overall | BIC (%) | 34.6 ± 15.1 | 39.9 ± 19.3 |
| OIC (%) | 6.3 ± 2.4 | 11.1 ± 6.5 | |
References
- Pilliar, R.M. Metallic Biomaterials. In Biomedical Materials; Narayan, R.C., Ed.; Springer Science+Business Media, LLC: Berlin/Heidelberg, Germany, 2009; Volume 2, pp. 41–81. [Google Scholar]
- Kaur, M.; Singh, K. Review on titanium and titanium based alloys as biomaterials for orthopaedic applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 102, 844–862. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontology 2000 2017, 73, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, K.A. Allergy to Surgical Implants. Clin. Rev. Allergy Immunol. 2019, 56, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Swiatkowska, I.; Martin, N.G.; Henckel, J.; Apthorp, H.; Hamshere, J.; Hart, A.J. Blood and plasma titanium levels associated with well-functioning hip implants. J. Trace Elements Med. Biol. 2020, 57, 9–17. [Google Scholar] [CrossRef]
- Teo, W.Z.W.; Schalock, P.C. Metal Hypersensitivity Reactions to Orthopedic Implants. Dermatol. Ther. 2017, 7, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Kretzer, J.P.; Reinders, J.; Sonntag, R.; Hagmann, S.; Streit, M.; Jeager, S.; Moradi, B. Wear in total knee arthroplasty—Just a question of polyethylene? Metal ion release in total knee arthroplasty. Int. Orthop. 2014, 38, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Solarino, G.; Piconi, C.; De Santis, V.; Piazzolla, A.; Moretti, B. Ceramic Total Knee Arthroplasty: Ready to Go? Joints 2017, 5, 224–228. [Google Scholar] [CrossRef] [Green Version]
- Middleton, S.; Toms, A. Allergy in total knee arthroplasty: A review of the facts. Bone Jt. J. 2016, 98-B, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Haddouti, E.-M.; Welle, K.; Burger, C.; Kabir, K.; Schildberg, F.A. Local Cellular Responses to Metallic and Ceramic Nanoparticles from Orthopedic Joint Arthroplasty Implants. Int. J. Nanomed. 2020, 15, 6705–6720. [Google Scholar] [CrossRef]
- Trieb, K.; Glinz, J.; Reiter, M.; Kastner, J.; Senck, S. Non-Destructive Testing of Ceramic Knee Implants Using Micro-Computed Tomography. J. Arthroplast. 2019, 34, 2111–2117. [Google Scholar] [CrossRef]
- Li, C.; Ai, F.; Miao, X.; Liao, H.; Li, F.; Liu, M.; Yu, F.; Dong, L.; Li, T.; Wang, X. “The return of ceramic implants”: Rose stem inspired dual layered modification of ceramic scaffolds with improved mechanical and anti-infective properties. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 93, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Vladescu, A.; Cotrut, C.M.; Azem, F.A.; Bramowicz, M.; Pana, I.; Braic, V.; Birlik, I.; Kiss, A.; Braic, M.; Abdulgader, R.; et al. Sputtered Si and Mg doped hydroxyapatite for biomedical applications. Biomed. Mater. 2018, 13, 025011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Wang, X.; Lin, Z.; Lin, H.; Zhang, Z.; Li, W.; Yang, X.; Cui, J. Ti-Based Biomedical Material Modified with TiOx/TiNx Duplex Bioactivity Film via Micro-Arc Oxidation and Nitrogen Ion Implantation. Nanomaterials 2017, 7, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, W.J.; Lee, M.-H.; Bae, T.-S.; Lee, S.-J.; Gay, J.; Loch, C. Anodisation Increases Integration of Unloaded Titanium Implants in Sheep Mandible. BioMed Res. Int. 2015, 2015, 857969. [Google Scholar] [CrossRef]
- Song, C.; Wang, S.; Liu, J.; Zhai, S. Microstructure and Mechanical Properties of Al2O3/Er3Al5O12 Binary Eutectic Ceramic Prepared by Bridgman Method. Materials 2018, 11, 534. [Google Scholar] [CrossRef] [Green Version]
- Denes, E.; Barrière, G.; Poli, E.; Lévêque, G. Alumina Biocompatibility. J. Long-Term Eff. Med. Implant. 2018, 28, 9–13. [Google Scholar] [CrossRef]
- Kim, S.-E.; Cho, W.-J.; Yoon, J.-K.; Shon, I.-J. The Effect of BN Reinforcement on the Mechanical Properties of Nanostructured Al₂O₃ Ceramics. J. Nanosci. Nanotechnol. 2020, 20, 4353–4357. [Google Scholar] [CrossRef]
- Chugunov, S.; Adams, N.A.; Akhatov, I.S. Evolution of SLA-Based Al2O3 Microstructure During Additive Manufacturing Process. Materials 2020, 13, 3928. [Google Scholar] [CrossRef]
- Agarwal, R.; García, A.J. Biomaterial strategies for engineering implants for enhanced osseointegration and bone repair. Adv. Drug Deliv. Rev. 2015, 94, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Shao, Z.; Zhang, X.; Pi, Y.; Wang, X.; Jia, Z.; Zhu, J.; Dai, L.; Chen, W.; Yin, L.; Chen, H.; et al. Polycaprolactone electrospun mesh conjugated with an MSC affinity peptide for MSC homing in vivo. Biomaterials 2012, 33, 3375–3387. [Google Scholar] [CrossRef]
- Cho, H.; Balaji, S.; Sheikh, A.Q.; Hurley, J.R.; Tian, Y.F.; Collier, J.H.; Crombleholme, T.M.; Narmoneva, D.A. Regulation of endothelial cell activation and angiogenesis by injectable peptide nanofibers. Acta Biomater. 2012, 8, 154–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böke, F.; Giner, I.; Keller, A.; Grundmeier, G.; Fischer, H. Plasma-Enhanced Chemical Vapor Deposition (PE-CVD) yields better Hydrolytical Stability of Biocompatible SiOx Thin Films on Implant Alumina Ceramics compared to Rapid Thermal Evaporation Physical Vapor Deposition (PVD). ACS Appl. Mater. Interfaces 2016, 8, 17805–17816. [Google Scholar] [CrossRef] [PubMed]
- Vasudev, M.C.; Anderson, K.D.; Bunning, T.J.; Tsukruk, V.V.; Naik, R.R. Exploration of Plasma-Enhanced Chemical Vapor Deposition as a Method for Thin-Film Fabrication with Biological Applications. ACS Appl. Mater. Interfaces 2013, 5, 3983–3994. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, J.; Wang, B.; Lu, W.; Wang, H.; Hou, W. Development of biobased multilayer films with improved compatibility between polylactic acid-chitosan as a function of transition coating of SiOx. Int. J. Biol. Macromol. 2020, 165, 1258–1263. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Sung, G.Y.; Park, M. Efficient Portable Urea Biosensor Based on Urease Immobilized Membrane for Monitoring of Physiological Fluids. Biomedicines 2020, 8, 596. [Google Scholar] [CrossRef]
- Si, Y.J.; Ren, Q.H.; Bi, L. miR-135b-5p regulates human mesenchymal stem cell osteogenic differentiation by facilitating the Hippo signaling pathway. Int. J. Clin. Exp. Pathol. 2017, 10, 7767–7775. [Google Scholar]
- Walker, J.M. The bicinchoninic acid (BCA) assay for protein quantitation. Methods Mol. Biol. 1994, 32, 5–8. [Google Scholar] [CrossRef]
- Böke, F.; Labude, N.; Lauria, I.; Ernst, S.; Müller-Newen, G.; Neuss, S.; Fischer, H. Biological Activation of Bioinert Medical High-Performance Oxide Ceramics by Hydrolytically Stable Immobilization of c(RGDyK) and BMP-2. ACS Appl. Mater. Interfaces 2018, 10, 38669–38680. [Google Scholar] [CrossRef]
- Doschak, M.R.; Cooper, D.M.L.; Huculak, C.N.; Matyas, J.R.; Hart, D.A.; Hallgrimsson, B.; Zernicke, R.F.; Bray, R.C. Angiogenesis in the distal femoral chondroepiphysis of the rabbit during development of the secondary centre of ossification. J. Anat. 2003, 203, 223–233. [Google Scholar] [CrossRef]
- Alberty, A. Effects of Physeal Distraction on the Vascular Supply of the Growth Area: A microangiographical study in rabbits. J. Pediatr. Orthop. 1993, 13, 373–377. [Google Scholar] [CrossRef]
- Wegst, U.G.; Bai, H.; Saiz, E.; Tomsia, A.P.; Ritchie, R.O. Bioinspired structural materials. Nat. Mater. 2015, 14, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franz, S.; Rammelt, S.; Scharnweber, D.; Simon, J.C. Immune responses to implants—A review of the implications for the design of immunomodulatory biomaterials. Biomaterials 2011, 32, 6692–6709. [Google Scholar] [CrossRef] [PubMed]
- Puleo, D.A.; Nanci, A. Understanding and controlling the bone-implant interface. Biomaterials 1999, 20, 2311–2321. [Google Scholar] [CrossRef]
- Lhotta, K.; Würzner, R.; Kronenberg, F.; Oppermann, M.; König, P. Rapid activation of the complement system by cuprophane depends on complement component C4. Kidney Int. 1998, 53, 1044–1051. [Google Scholar] [CrossRef]
- Hed, J.; Johansson, M.; Lindroth, M. Complement activation according to the alternate pathway by glass and plastic surfaces and its role in neutrophil adhesion. Immunol. Lett. 1984, 8, 295–299. [Google Scholar] [CrossRef]
- Wilson, C.J.; Clegg, R.E.; Leavesley, D.I.; Pearcy, M.J. Mediation of Biomaterial-Cell Interactions by Adsorbed Proteins: A Review. Tissue Eng. 2005, 11, 1–18. [Google Scholar] [CrossRef]
- Zhuo, R.; Siedlecki, C.A.; Vogler, E.A. Autoactivation of blood factor XII at hydrophilic and hydrophobic surfaces. Biomaterials 2006, 27, 4325–4332. [Google Scholar] [CrossRef]
- Kalltorp, M.; Askendal, A.; Thomsen, P.; Tengvall, P. Ellipsometric studies in vitro on kinetics of rat complement activation. J. Biomed. Mater. Res. 1999, 44, 222–225. [Google Scholar] [CrossRef]
- Sarma, J.V.; Ward, P.A. The complement system. Cell Tissue Res. 2011, 343, 227–235. [Google Scholar] [CrossRef]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J. Complement activation during extracorporeal therapy: Biochemistry, cell biology and clinical relevance. Nephrol. Dial. Transpl. 1994, 9 (Suppl. 2), 36–45. [Google Scholar]
- Giorgetti, A.; Marchetto, M.C.N.; Li, M.; Yu, D.; Fazzina, R.; Mu, Y.; Adamo, A.; Paramonov, I.; Cardoso, J.C.; Monasterio, M.B.; et al. Cord blood-derived neuronal cells by ectopic expression of Sox2 and c-Myc. Proc. Natl. Acad. Sci. USA 2012, 109, 12556–12561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, M.; Sperling, C.; Werner, C. Synergistic effect of hydrophobic and anionic surface groups triggers blood coagulation in vitro. J. Mater. Sci. Mater. Med. 2010, 21, 931–937. [Google Scholar] [CrossRef]
- Salasznyk, R.M.; Williams, W.A.; Boskey, A.; Batorsky, A.; Plopper, G.E. Adhesion to Vitronectin and Collagen I Promotes Osteogenic Differentiation of Human Mesenchymal Stem Cells. J. Biomed. Biotechnol. 2004, 2004, 24–34. [Google Scholar] [CrossRef]
- Xiong, J.-P.; Stehle, T.; Diefenbach, B.; Zhang, R.; Dunker, R.; Scott, D.L.; Joachimiak, A.; Goodman, S.L.; Arnaout, M.A. Crystal Structure of the Extracellular Segment of Integrin αVβ3. Science 2001, 294, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Xiao, T.; Takagi, J.; Coller, B.S.; Wang, J.-H.; Springer, T.A. Structural basis for allostery in integrins and binding to fibrinogen-mimetic therapeutics. Nature 2004, 432, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Hynes, R.O. Integrins: Bidirectional, Allosteric Signaling Machines. Cell 2002, 110, 673–687. [Google Scholar] [CrossRef] [Green Version]
- Danen, E.; Sonnenberg, A. Erratum: Integrins in regulation of tissue development and function. J. Pathol. 2003, 201, 632–641. [Google Scholar] [CrossRef]
- Humphries, J.D.; Byron, A.; Humphries, M.J. Integrin ligands at a glance. J. Cell Sci. 2006, 119 Pt 19, 3901–3903. [Google Scholar] [CrossRef] [Green Version]
- Zachary, I.; Rozengurt, E. Focal adhesion kinase (p125FAK): A point of convergence in the action of neuropeptides, integrins, and oncogenes. Cell 1992, 71, 891–894. [Google Scholar] [CrossRef]
- Abedi, H.; Zachary, I. Vascular Endothelial Growth Factor Stimulates Tyrosine Phosphorylation and Recruitment to New Focal Adhesions of Focal Adhesion Kinase and Paxillin in Endothelial Cells. J. Biol. Chem. 1997, 272, 15442–15451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aro, H.T.; Alm, J.J.; Moritz, N.; Mäkinen, T.J.; Lankinen, P. Low BMD affects initial stability and delays stem osseointegration in cementless total hip arthroplasty in women: A 2-year RSA study of 39 patients. Acta Orthop. 2012, 83, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-K.; Ha, Y.-C.; Chang, B.-K.; Kim, K.-C.; Kim, T.-Y.; Koo, K.-H. Cementless Bipolar Hemiarthroplasty Using a Hydroxyapatite-Coated Long Stem for Osteoporotic Unstable Intertrochanteric Fractures. J. Arthroplast. 2011, 26, 626–632. [Google Scholar] [CrossRef]
- Tao, Z.; Zhou, W.; Jiang, Y.; Wu, X.; Xu, Z.; Yang, M.; Xie, J. Effects of strontium-modified calcium phosphate cement combined with bone morphogenetic protein-2 on osteoporotic bone defects healing in rats. J. Biomater. Appl. 2018, 33, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Tao, Z.-S.; Zhou, W.-S.; He, X.-W.; Liu, W.; Bai, B.-L.; Zhou, Q.; Huang, Z.-L.; Tu, K.-K.; Li, H.; Sun, T.; et al. A comparative study of zinc, magnesium, strontium-incorporated hydroxyapatite-coated titanium implants for osseointegration of osteopenic rats. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 226–232. [Google Scholar] [CrossRef]
- Gong, T.; Chen, Y.; Zhang, Y.; Zhang, Y.; Liu, X.; Troczynski, T.; Häfeli, U.O. Osteogenic and anti-osteoporotic effects of risedronate-added calcium phosphate silicate cement. Biomed. Mater. 2016, 11, 045002. [Google Scholar] [CrossRef]
- Lozano, D.; Trejo, C.G.; Gómez-Barrena, E.; Manzano, M.; Doadrio, J.C.; Salinas, A.J.; Vallet-Regí, M.; García-Honduvilla, N.; Esbrit, P.; Buján, J. Osteostatin-loaded onto mesoporous ceramics improves the early phase of bone regeneration in a rabbit osteopenia model. Acta Biomater. 2012, 8, 2317–2323. [Google Scholar] [CrossRef]
- Luo, E.; Hu, J.; Bao, C.; Li, Y.; Tu, Q.; Murray, D.; Chen, J. Sustained release of adiponectin improves osteogenesis around hydroxyapatite implants by suppressing osteoclast activity in ovariectomized rabbits. Acta Biomater. 2012, 8, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Plaza, J.Q.; Garzón, L.B.; Gimenez, B.B.; Moraleda, B.F.; Collía, F.; Rodríguez-Lorenzo, L.M. Application of calcium phosphates and fibronectin as complementary treatment for osteoporotic bone fractures. Injury 2016, 47, 15–21. [Google Scholar] [CrossRef]
- Shen, X.; Ma, P.; Hu, Y.; Xu, G.; Xu, K.; Chen, W.; Ran, Q.; Dai, L.; Yu, Y.; Mu, C.; et al. Alendronate-loaded hydroxyapatite-TiO2 nanotubes for improved bone formation in osteoporotic rabbits. J. Mater. Chem. 2016, 4, 1423–1436. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Kuo, C.L.; Fan, F.Y.; Yang, K.-C. Strontium-impregnated bioabsorbable composite for osteoporotic fracture fixation. J. Biomed. Mater. Res. 2015, 103, 3355–3363. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Xu, L.; Li, K.; Xie, N.; Xi, Y.; Wang, Y.; Zheng, X.; Chen, X.; Wang, M.; Ye, X. Zinc-modified calcium silicate coatings promote osteogenic differentiation through TGF-β/Smad pathway and osseointegration in osteopenic rabbits. Sci. Rep. 2017, 7, 3440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnella, F.; Kunisch, E.; Bungartz, M.; Maenz, S.; Horbert, V.; Xin, L.; Mika, J.; Borowski, J.; Bischoff, S.; Schubert, H.; et al. Low-dose BMP-2 is sufficient to enhance the bone formation induced by an injectable, PLGA fiber-reinforced, brushite-forming cement in a sheep defect model of lumbar osteopenia. Spine J. 2017, 17, 1699–1711. [Google Scholar] [CrossRef] [PubMed]






| Endpoint | 6 Weeks | 12 Weeks | MD | 95% CI | SE | t Value | p | |
|---|---|---|---|---|---|---|---|---|
| Lateral | BIC (%) | 3.1 ± 3.4 | 3.9 ± 1.3 | 0.8 | −0.41 to 2.01 | 0.61 | 1.32 | 0.2 |
| OIC (%) | 0.9 ± 1.2 | 0.5 ± 0.9 | −0.4 | −0.90 to 0.10 | 0.25 | −1.60 | 0.1 | |
| Distal | BIC (%) | 12.1 ± 4.6 | 14.3 ± 5.8 | 2.2 | −0.26 to 4.66 | 1.23 | 1.78 | 0.08 |
| OIC (%) | 3.4 ± 3.0 | 6.0 ± 4.7 | 2.6 | 0.75 to 4.45 | 0.93 | 2.80 | 0.007 | |
| Medial | BIC (%) | 6.8 ± 4.2 | 8.6 ± 3.2 | 1.8 | 0.05 to 3.56 | 0.88 | 2.05 | 0.04 |
| OIC (%) | 3.2 ± 3.2 | 4.6 ± 4.3 | 1.4 | −0.38 to 3.18 | 0.89 | 1.57 | 0.1 | |
| Proximal | BIC (%) | 12.6 ± 3.5 | 13.1 ± 3.5 | 0.5 | −1.14 to 2.14 | 0.83 | 0.61 | 0.5 |
| OIC (%) | 5.0 ± 0.0 | 5.6 ± 1.8 | 0.6 | 0.00 to 1.20 | 0.30 | 2.00 | 0.05 | |
| Overall | BIC (%) | 34.6 ± 7.9 | 39.9 ± 6.9 | 5.3 | 1.81 to 8.78 | 1.75 | 3.03 | 0.003 |
| OIC (%) | 12.6 ± 6.0 | 16.8 ± 9.3 | 4.2 | 0.52 to 7.87 | 1.85 | 2.28 | 0.03 | |
| Endpoint | 6 Weeks | 12 Weeks | |||
|---|---|---|---|---|---|
| MD | p | MD | p | ||
| Lateral | BIC (%) | 0.0 | 0.5 | −1.0 | 0.05 |
| OIC (%) | 0.9 | 0.02 | 1.1 | 0.4 | |
| Distal | BIC (%) | 0.6 | 0.4 | 0.2 | 0.4 |
| OIC (%) | 1.9 | 0.1 | 0.6 | 0.3 | |
| Medial | BIC (%) | 1.5 | 0.2 | 1.1 | 0.05 |
| OIC (%) | 3.5 | 0.004 | 1.3 | 0.05 | |
| Proximal | BIC (%) | 1.7 | 0.3 | 1.0 | 0.4 |
| OIC (%) | 0.0 | 1.0 | 0.7 | 0.09 | |
| Overall | BIC (%) | 0.0 | 0.3 | 0.0 | 0.4 |
| OIC (%) | 6.3 | 0.01 | 5.7 | 0.1 | |
| Author, Year | Rabbit Model | Rabbits (n) and Implant Site | Materials | Follow-Up | Type of Analyses |
|---|---|---|---|---|---|
| Gong et al., 2016 [58] | 30 New Zealand rabbits | Right medial tibia epiphysis of the (d = 6 mm, ø = 3 mm) | Calcium silicate powder, RA-CPSC, MCP, Ca(H2PO4)2, and risedronate added into calcium silicate powder and homogeneously mixed, respectively. | 8, 10 weeks | X-ray semi-quantitative analysis; PCR |
| Lozano et al., 2012 [59] | Osteoporosis induced rabbits | Medial and lateral distal femoral epiphysis | SBA15 and SiO2. The surface was chemically modified with an organic modification of silica walls with alkoxysilane, n-octyltriethoxysilane and functionalized by soaking the mesoporous in a solution of PTHrP in PBS. | 2 weeks | Histology; Immunohistochemistry |
| Luo et al., 2012 [60] | 60 New Zealand rabbits | Sub-periosteal mandibular (4 mm × 5 mm × 10 mm) | Porous commercial HA was physically functionalized in surface with or without APN or Matrigel or combination of both. | 4 weeks | Micro-CT; Biomechanical analyses |
| Plaza et al., 2016 [61] | 42 New Zealand white rabbits | Medial femoral condyles A | Physical incorporation of fibronectin in HA bulk material by adding HA to a fibronectin solution of in PBS. | 1, 2, 5 days | Micro-CT; Histology |
| Shen et al. 2016 [62] | 43 New Zealand white rabbits | Femoral epiphysis | TNT were immersed in supersaturated Ca(OH)2 solution, Ca(NO3)2·4H2O (0.2 M) and (NH4)2HPO4 (0.2 M) solutions to create a coating of HA. TNT-HA was subsequently functionalized with Aln by immersion in Aln solution (physical absorption). | 12 weeks | X-rays; Micro-CT; Biomechanical analyses; Histology |
| Wu et al., 2015 [63] | 16 New Zealand White rabbits | Distal femur | Strontium enriched CPC in the solid phase and PCL. | 24 weeks | Micro-CT |
| Yu et al., 2017 [64] | 40 New Zealand white rabbits | Two implants (2 mm diameter, 10 mm depth) into each femur | Ti–6Al–4V implants (ø10 × 2 mm) coated by means of plasma-spray technique with HA or CaSiO3 or zinc-modified calcium silicate (Ca2ZnSi2O7) at two different Zn contents. | 4, 8, 12 weeks | Micro-CT; Histology |
| Gunnella et al., 2017 [65] | 30 California rabbits | Not specified (5 mm wide and 4 mm) | A composite material of HA/TCP granules with or without Sr substitution. | 12 weeks | Histomorphometry; Immunohistochemistry |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Schenker, H.; Maffulli, N.; Hildebrand, F.; Eschweiler, J. Histomorphometry of Ossification in Functionalised Ceramics with Tripeptide Arg-Gly-Asp (RGD): An In Vivo Study. Life 2022, 12, 761. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050761
Migliorini F, Schenker H, Maffulli N, Hildebrand F, Eschweiler J. Histomorphometry of Ossification in Functionalised Ceramics with Tripeptide Arg-Gly-Asp (RGD): An In Vivo Study. Life. 2022; 12(5):761. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050761
Chicago/Turabian StyleMigliorini, Filippo, Hanno Schenker, Nicola Maffulli, Frank Hildebrand, and Jörg Eschweiler. 2022. "Histomorphometry of Ossification in Functionalised Ceramics with Tripeptide Arg-Gly-Asp (RGD): An In Vivo Study" Life 12, no. 5: 761. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050761