Childhood Epilepsy with Centrotemporal Spikes: Clinical and Neuropsychological Outcomes 5 Years after Remission

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection
2.3. Follow-Up
2.4. Neuropsychological Evaluation
2.5. Statistical Analyses
3. Results
3.1. Clinical Data
3.2. Health, Academic Performances, and Familial SES after Remission
3.3. Neuropsychological and Behavioral Assessment after Remission
3.3.1. Neuropsychological Profile
- In visuomotor and visuospatial skills (VMI developmental test), mean normal scores were obtained in all subtests (visuomotor integration, visual perception, motor coordination).
- In attention and executive functioning (Nepsy II) domains, mean results within the normal range were obtained in visual and auditory attention and inhibition. Borderline mean results were recorded in response tests, graphic fluency, rapid naming, and cognitive flexibility.
- In language skills (Nepsy II and BVN 12–18) mean normal scores were obtained in lexical denomination, instruction understanding, and semantic fluency, whereas mean borderline results were reached in the phonological fluency test.
- In memory and learning skills (Nepsy II), mean normal scores were obtained in all subtests (immediate list memory, deferred list memory, immediate design memory, deferred design memory).
- In academic skills (DDE-2, MT, BDE-2, BVSCO-2 tests), mean normal scores were recorded in all tests (reading, writing, comprehension, calculation, graphomotor fluence), except for dictation, where a mean pathological result was obtained.
3.3.2. Behavioral Assessment (Table 1 and Table 2)
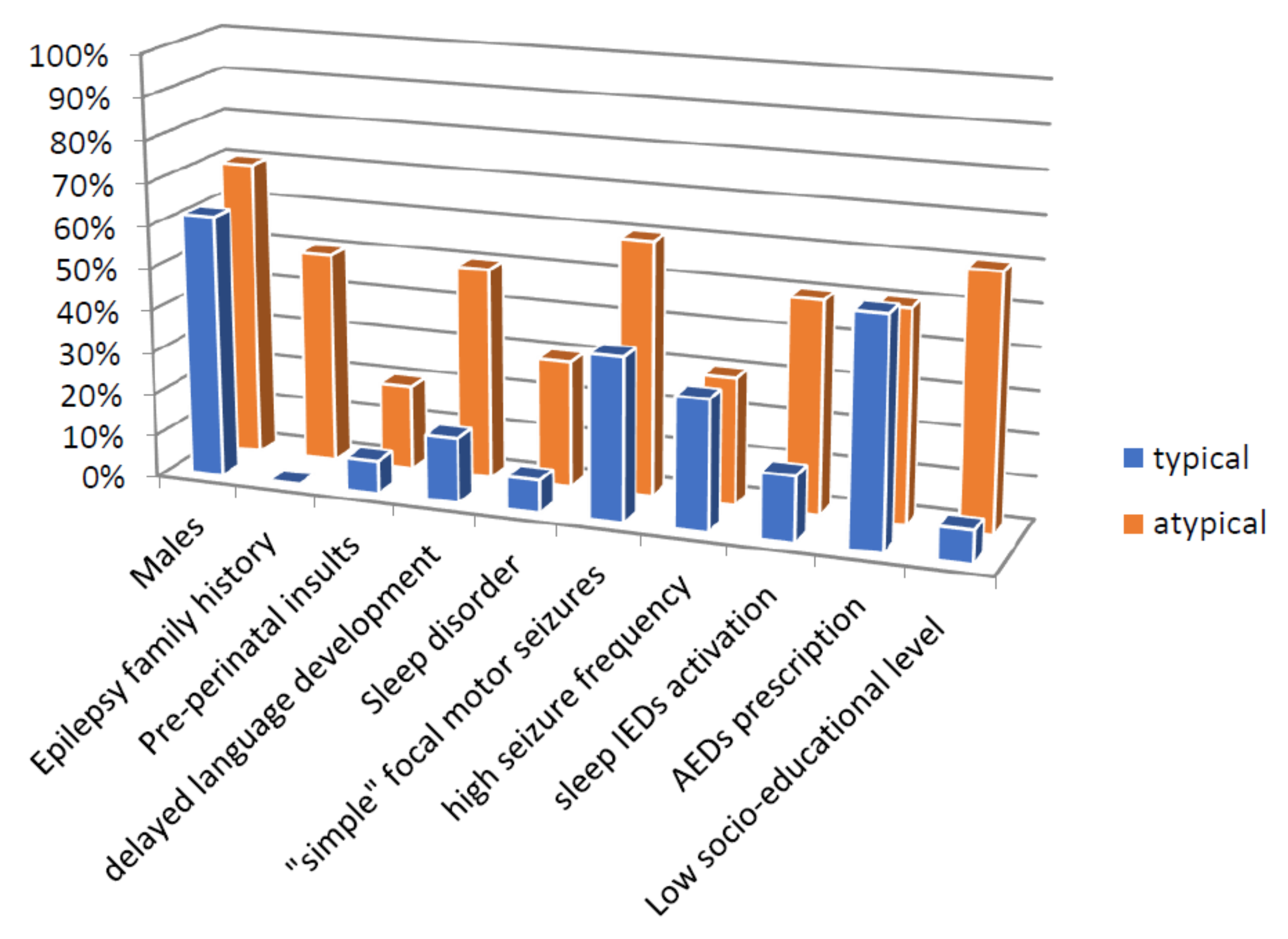
3.3.3. Predictors of Neuropsychological Outcome
- Positive family history for epilepsy: 5 out of 10 patients in the “atypical” group versus 0 out of 13 patients in the “typical” group (p = 0.01769).
- Familial SES: A better SES level was reported in the “typical” (1 high, 11 middle, 1 low level) compared to the “atypical” group (0 high, 3 middle, 7 low level). In particular, higher mother’s schooling (p = 0.04169), higher father’s schooling (p = 0.01939), higher mother’s income (p = 0.0262), and higher father’s income (p = 0.01331) were obtained in the “typical” compared to the “atypical” group.
- IED activation in sleep: higher IED activation in sleep EEG recordings was found in the “atypical” as compared to the “typical” group. In particular, 5 out of 10 patients in the “atypical” group had a generalized IED activation in sleep; conversely, 2 out of 13 patients in the typical group had the same EEG pattern (p = 0.09748).
- Mean AED treatment duration: in the “typical” group, a lower AED treatment duration was observed (mean 3.5 years) as compared to the “atypical” group (mean of 5.6 years) (p = 0.1027).
- Presence of language disorder before epilepsy onset: in the “typical” group, 2 out of 13 patients presented delayed language development as compared to 5 out of 10 in the “atypical” group (p = 0.183).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A: Neuropsychological Assessment
Appendix A.1. Intellectual Functioning
Appendix A.2. Domain Language
Appendix A.3. Domain Attention and Executive Functioning
Appendix A.4. Domain Visuomotor and Visuospatial Skills
Appendix A.5. Domain Memory and Learning
Appendix A.6. Domain Academic Skills
Appendix A.7. Domain Behavioral and Emotional Functioning
References
- Holmes, G.L. Benign Focal Epilepsies of Childhood. Epilepsia 2010, 34, S49–S61. [Google Scholar] [CrossRef] [PubMed]
- Vannest, J.; Tenney, J.R.; Gelineau-Morel, R.; Maloney, T.; Glauser, T.A. Cognitive and behavioral outcomes in benign childhood epilepsy with centrotemporal spikes. Epilepsy Behav. 2015, 45, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Panayiotopoulos, C.P.; Michael, M.; Sanders, S.; Valeta, T.; Koutroumanidis, M. Benign childhood focal epilepsies: Assessment of established and newly recognized syndromes. Brain 2008, 131, 2264–2286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, H.; Wang, Y.; Hua, Y.; Wang, J.; Jing, M.; Hu, X. Analysis of serial electroencephalographic predictors of seizure recurrence in Rolandic epilepsy. Child’s Nerv. Syst. 2019, 35, 1579–1583. [Google Scholar] [CrossRef]
- Hughes, J.R. Benign epilepsy of childhood with centrotemporal spikes (BECTS): To treat or not to treat, that is the question. Epilepsy Behav. 2010, 19, 197–203. [Google Scholar] [CrossRef]
- Aicardi, J. Atypical semiology of rolandic epilepsy in some related syndromes. Epileptic Disord. 2000, 2, 5–9. [Google Scholar]
- Datta, A.; Sinclair, D.B. Benign Epilepsy of Childhood With Rolandic Spikes: Typical and Atypical Variants. Pediatr. Neurol. 2007, 36, 141–145. [Google Scholar] [CrossRef]
- Callenbach, P.M.C.; Bouma, P.A.D.; Geerts, A.T.; Arts, W.F.M.; Stroink, H.; Peeters, E.A.J.; Van Donselaar, C.A.; Peters, A.C.B.; Brouwer, O.F. Long term outcome of benign childhood epilepsy with centrotemporal spikes: Dutch Study of Epilepsy in Childhood. Seizure 2010, 19, 501–506. [Google Scholar] [CrossRef]
- Parisi, P.; Paolino, M.C.; Raucci, U.; Ferretti, A.; Villa, M.P.; Trenite, D.K.-N. “Atypical forms” of benign epilepsy with centrotemporal spikes (BECTS): How to diagnose and guide these children. A practical/scientific approach. Epilepsy Behav. 2017, 75, 165–169. [Google Scholar] [CrossRef]
- Gobbi, G.; Boni, A.; Filippini, M. The Spectrum of Idiopathic Rolandic Epilepsy Syndromes and Idiopathic Occipital Epilepsies: From the Benign to the Disabling. Epilepsia 2006, 47, 62–66. [Google Scholar] [CrossRef]
- Filippini, M.; Boni, A.; Giannotta, M.; Gobbi, G. Neuropsychological development in children belonging to BECTS spectrum: Long-term effect of epileptiform activity. Epilepsy Behav. 2013, 28, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Wickens, S.; Bowden, S.C.; D’Souza, W. Cognitive functioning in children with self-limited epilepsy with centrotemporal spikes: A systematic review and meta-analysis. Epilepsia 2017, 58, 1673–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Giorgis, V.; Filippini, M.; Macasaet, J.A.; Masnada, S.; Veggiotti, P. Neurobehavioral consequences of continuous spike and waves during slow sleep (CSWS) in a pediatric population: A pattern of developmental hindrance. Epilepsy Behav. 2017, 74, 1–9. [Google Scholar] [CrossRef]
- Camfield, C.S.; Camfield, P.R. Rolandic epilepsy has little effect on adult life 30 years later: A population-based study. Neurology 2014, 82, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.E.; Stoyell, S.M.; Kramer, M.A.; Berg, A.T.; Chu, C.J. The natural history of seizures and neuropsychiatric symptoms in childhood epilepsy with centrotemporal spikes (CECTS). Epilepsy Behav. 2020, 103, 106437. [Google Scholar] [CrossRef]
- Scheffer, I.E.; Berkovic, S.; Meletti, S.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshé, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Montanaro, M.; Battistella, P.A.; Boniver, C.; Galeone, D. Quality of life in young Italian patients with epilepsy. Neurol. Sci. 2004, 25, 264–273. [Google Scholar] [CrossRef]
- Jackson, D.C. Childhood epilepsy with centrotemporal spikes: Perhaps not so benign after all. Epilepsy Behav. 2015, 45, 92–93. [Google Scholar] [CrossRef]
- Wheless, J.W.; Clarke, D.F.; Arzimanoglou, A.; Carpenter, D. Treatment of pediatric epilepsy: European expert opinion, 2007. Epileptic Disord. 2007, 9, 412. [Google Scholar]
- Wong, P.K.H.; Bencivenga, R.; Gregory, D. Statistical classification of spikes in Benign Rolandic Epilepsy. Brain Topogr. 1988, 1, 123–129. [Google Scholar] [CrossRef]
- Holmes, G.L. Rolandic epilepsy: Clinical and electroencephalographic features. Epilepsy Res. Suppl. 1992, 6, 29–43. [Google Scholar] [PubMed]
- Loddenkemper, T.; Burgess, R.C.; Syed, T.; Pestana, E.M. Lateralization of Interictal EEG Findings. J. Clin. Neurophysiol. 2007, 24, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Northcott, E.; Connolly, A.M.; Berroya, A.; Sabaz, M.; McIntyre, J.; Christie, J.; Taylor, A.; Batchelor, J.; Bleasel, A.F.; Lawson, J.A.; et al. The Neuropsychological and Language Profile of Children with Benign Rolandic Epilepsy. Epilepsia 2005, 46, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Deltour, L.; Barathon, M.; Quaglino, V.; Vernier, M.-P.; Despretz, P.; Boucart, M.; Berquin, P. Children with benign epilepsy with centrotemporal spikes (BECTS) show impaired attentional control: Evidence from an attentional capture paradigm. Epileptic Disord. 2007, 9, 32–38. [Google Scholar] [PubMed]
- Northcott, E.; Connolly, A.M.; Berroya, A.; McIntyre, J.; Christie, J.; Taylor, A.; Bleasel, A.F.; Lawson, J.A.; Bye, A.M. Memory and phonological awareness in children with Benign Rolandic Epilepsy compared to a matched control group. Epilepsy Res. 2007, 75, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Piccinelli, P.; Borgatti, R.; Aldini, A.; Bindelli, D.; Ferri, M.; Perna, S.; Pitillo, G.; Termine, C.; Zambonin, F.; Balottin, U. Academic performance in children with rolandic epilepsy. Dev. Med. Child. Neurol. 2008, 50, 353–356. [Google Scholar] [PubMed]
- Danielsson, J.; Petermann, F. Cognitive deficits in children with benign rolandic epilepsy of childhood or rolandic discharges: A study of children between 4 and 7 years of age with and without seizures compared with healthy controls. Epilepsy Behav. 2009, 16, 646–651. [Google Scholar] [CrossRef]
- Kim, E.-H.; Yum, M.-S.; Kim, H.-W.; Ko, T.-S. Attention-deficit/hyperactivity disorder and attention impairment in children with benign childhood epilepsy with centrotemporal spikes. Epilepsy Behav. 2014, 37, 54–58. [Google Scholar] [CrossRef]
- Filippini, M.; Ardu, E.; Stefanelli, S.; Boni, A.; Gobbi, G.; Benso, F. Neuropsychological profile in new-onset benign epilepsy with centrotemporal spikes (BECTS): Focusing on executive functions. Epilepsy Behav. 2016, 54, 71–79. [Google Scholar] [CrossRef]
- Monjauze, C.; Ebroadbent, H.; Boyd, S.G.; Neville, B.G.R.; Baldeweg, T. Language deficits and altered hemispheric lateralization in young people in remission from BECTS. Epilepsia 2011, 52, e79–e83. [Google Scholar] [CrossRef]
- Neri, M.L.; Guimarães, C.A.; Oliveira, E.P.; Duran, M.H.; Medeiros, L.L.; Montenegro, M.A.; Boscariol, M.; Guerreiro, M.M. Neuropsychological assessment of children with rolandic epilepsy: Executive functions. Epilepsy Behav. 2012, 24, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.M.; Rzezak, P.; Guimarães, C.A.; Montenegro, M.A.; Guerreiro, M.M.; Valente, K.D. The executive profile of children with Benign Epilepsy of Childhood with Centrotemporal Spikes and Temporal Lobe Epilepsy. Epilepsy Behav. 2017, 72, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Monjauze, C.; Tuller, L.; Hommet, C.; Barthez, M.-A.; Khomsi, A. Language in benign childhood epilepsy with centro-temporal spikes abbreviated form: Rolandic epilepsy and language. Brain Lang. 2005, 92, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Jurkevičienė, G.; Endziniene, M.; Laukienė, I.; Saferis, V.; Rastenyte, D.; Plioplys, S.; Vaiciene-Magistris, N. Association of language dysfunction and age of onset of benign epilepsy with centrotemporal spikes in children. Eur. J. Paediatr. Neurol. 2012, 16, 653–661. [Google Scholar] [CrossRef]
- Garcia-Ramos, C.; Jackson, D.C.; Lin, J.J.A.; Dabbs, K.; Jones, J.E.; Hsu, D.A.; Stafstrom, C.E.; Zawadzki, L.; Seidenberg, M.; Prabhakaran, V.; et al. Cognition and brain development in children with benign epilepsy with centrotemporal spikes. Epilepsia 2015, 56, 1615–1622. [Google Scholar] [CrossRef]
- Teixeira, J.; Santos, M.E. Language skills in children with benign childhood epilepsy with centrotemporal spikes: A systematic review. Epilepsy Behav. 2018, 84, 15–21. [Google Scholar] [CrossRef]
- Ebus, S.; Overvliet, G.; Arends, J.; Aldenkamp, A.A. Reading performance in children with rolandic epilepsy correlates with nocturnal epileptiform activity, but not with epileptiform activity while awake. Epilepsy Behav. 2011, 22, 518–522. [Google Scholar] [CrossRef]
- Overvliet, G.M.; Aldenkamp, A.P.; Klinkenberg, S.; Nicolai, J.; Vles, J.; Besseling, R.M.H.; Backes, W.; Jansen, J.F.A.; Hofman, P.A.; Hendriksen, J.G.M. Correlation between language impairment and problems in motor development in children with rolandic epilepsy. Epilepsy Behav. 2011, 22, 527–531. [Google Scholar] [CrossRef]
- Massa, R.; De Saint-Martin, A.; Carcangiu, R.; Rudolf, G.; Seegmuller, C.; Kleitz, C.; Metz-Lutz, M.N.; Hirsch, E.; Marescaux, C. EEG criteria predictive of complicated evolution in idiopathic rolandic epilepsy. Neurology 2001, 57, 1071–1079. [Google Scholar] [CrossRef]
- Joachim, K.C.; Wilk, P.; Ryan, B.L.; Speechley, K.N. Family-centered care in children with epilepsy: Evaluating the Measure of Processes of Care (MPOC-20). Epilepsia 2016, 57, 1660–1668. [Google Scholar] [CrossRef]
- Galea, S.; Tracy, M. Participation Rates in Epidemiologic Studies. Ann. Epidemiol. 2007, 17, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Orsini, A.; Pezzuti, L.; Picone, L. Wechsler Intelligence Scale for Children IV- Edizione Italiana. Giunti, O.S.: Firenze, Italy, 2012. [Google Scholar]
- Orsini, A.; Pezzuti, L. Wechsler Adult Intelligence Scale—Forth Edition [WAIS-IV] Edizione Italiana. Giunti, O.S.: Firenze, Italy, 2013. [Google Scholar]
- Gugliotto, M.; Bislacchi, P.S.; Cendron, M. Test BVN 12-18. Batteria di valutazione neuropsicologica per l’adolescenza. Erickson: Trento, Italy, 2009. [Google Scholar]
- Urgesi, C.; Campanella, F.; Fabbro, F. NEPSY-II, Contributo alla Taratura Italiana. Giunti, O.S.: Firenze, Italy, 2011. [Google Scholar]
- Berry, K.E.; Buktenica, N.A. The VMI: Developmental test of visual motor integration. Giunti, O.S.: Firenze, Italy, 2000. [Google Scholar]
- Sartori, G.; Job, R.; Tressoldi, R.P. DDE 2 Batteria per la valutazione della dislessia e della disortografia evolutiva. 2nd ed. Giunti, O.S.: Firenze, Italy, 2007. [Google Scholar]
- Arina, S.; Iervolino, I.; Stella, G. Prima raccolta di dati normativi per la valutazione della dislessia evolutiva negli adolescenti su un campione di scuola secondaria di secondo grado. Rivista Dislessia, 10, 1. Erickson: Trento, Italy, 2010; 9–38. [Google Scholar]
- Cornoldi, C.; Colpo, G. Nuove Prove di lettura MT per la Scuola media Inferiore. Giunti, O.S: Firenze, Italy, 1998. [Google Scholar]
- Cornoldi, C.; Colpo, G. Prove di Lettura MT per la Scuola Elementare—2. Giunti, O.S.: Firenze, Italy, 1998. [Google Scholar]
- Cornoldi, C.; Tressoldi, P.; Perini, N. Valutare la rapidità e la correttezza della lettura di brani Nuove norme e alcune chiarificazioni per l’uso delle prove MT. Rivista Dislessia, Erickson: Trento, Italy, 2010; 7, 89–100. [Google Scholar]
- Cornoldi, C.; Candela, M. Prove di lettura e scrittura MT-16-19. Erickson: Trento, Italy, 2015. [Google Scholar]
- Tressoldi, P.E.; Cornoldi, C.; Anna Maria, R. BVSCO-2 Batteria per la Valutazione della Scrittura e della Competenza Ortografica—2. Giunti, O.S.: Firenze, Italy, 2012. [Google Scholar]
- Biancardi, A.; Bachmann, C.; Nicoletti, C. BDE 2—batteria discalculia evolutiva—elaborazione numerica e calcolotest per la diagnosi dei disturbi dell’elaborazione numerica e del calcolo in eta’ evolutiva 8-13 anni. Erickson: Trento, Italy, 2016. [Google Scholar]
- Achenbach, T.M. CBCL (Child Behavior Checklist 4–18). Adattamento italiano e standardizzazione a cura di M. Molteni e A. Frigerio. Available online: https://emedea.it/medea/it/ricerca-it/topics/aseba-laboratorio-per-l-adattamento-italiano (accessed on 5 October 2020).


{kind=link}
| Domain | Test/Subtest-Index | Mean (SD) | Level |
|---|---|---|---|
| Intellectual functioning | Wechsler Intelligence Scale for children (full-scale IQ) a | 97.74 (20.45) | Normal |
| Verbal Comprehension Index (VCI) a | 100.91 (16.34) | Normal | |
| Perceptual Reasoning Index (PRI) a | 102.78 (18.06) | Normal | |
| Working Memory Index (WMI) a | 92.22 (19.31) | Normal | |
| Processing Speed Index (PSI) a | 94.17 (19.12) | Normal | |
| Language | Picture naming b | −0,47 (1.34) | Normal |
| Comprehension of instructions a | 8,04 (3.71) | Normal | |
| Word generation | |||
| Semantic a | 9.13 (3.91) | Normal | |
| Phonemic a | 7.35 (2.77) | Mildly impaired | |
| Attention and executive functioning | Visual attention a | 9.61 (4.47) | Normal |
| Auditory attention b | −0.61 (2.32) | Normal | |
| Response set b | −2.2 (7.97) | Severely impaired | |
| Design fluency a | 7.83 (2.81) | Mildly impaired | |
| Inhibition naming a | 7.5 (2.92) | Mildly impaired | |
| Inhibition a | 8 (3.09) | Normal | |
| Switching a | 7.18 (2.52) | Mildly impaired | |
| Visuomotor and visuospatial skills | VMI b | 88.48 (12.63) | Normal |
| Visual perception b | 94.87 (14.38) | Normal | |
| Motor coordination b | 86.09 (14.73) | Normal | |
| Memory and learning | List memory | ||
| Immediate memory a | 8.83 (2.59) | Normal | |
| Delayed memory a | 8.35 (3.59) | Normal | |
| Total memory a | 8.52 (2.63) | Normal | |
| Memory for designs | |||
| Immediate memory a | 6.48 (4.57) | Mildly impaired | |
| Delayed memory a | 8 (4.36) | Normal | |
| Academic skills | Word reading | ||
| Rapidity sill/sec b | −0.53 (1.36) | Normal | |
| Accuracy b | 0.57 (1.82) | Normal | |
| Non-word reading | |||
| Rapidity b | −0.62 (1.11) | Normal | |
| Accuracy b | 0.2 (1.36) | Normal | |
| Reading test | |||
| Rapidity sill/sec b | −0.87 (1.66) | Normal | |
| Accuracy b | 0.56 (1.86) | Normal | |
| Reading comprehension test b | −0.46 (1.1) | Normal | |
| Dictations of words and pseudowords b | 0.74 (3.68) | Normal | |
| Dictations of pseudowords b | −0.28 (1.76) | Normal | |
| Text dictation b | 3.88 (9.55) | Severely impaired | |
| Handwriting speed | |||
| Task 1 b | −0.57 (1.42) | Normal | |
| Task 2 b | −0.99 (1.49) | Normal | |
| Task 3 b | −1.11 (1.47) | Mildly impaired | |
| Mathematics competence | |||
| Number Index b | 103.41 (22.89) | Normal | |
| Calculation Index b | 91.27 (27.81) | Normal | |
| Sense of Number Index b | 100.64 (23.4) | Normal | |
| Total Index b | 97.45 (24.48) | Normal | |
| Behavioral and emotional functioning | Internalizing problems c | 55.85 (9.03) | Normal |
| Externalizing problems c | 50.93 (12.22) | Normal | |
| Total problems c | 53.24 (11.55) | Normal |
| z-Scores | Scaled Score | T Score | Standard Score | |
|---|---|---|---|---|
| Normal or typical | >−0.99 | >8 | <65 | 85–114 normal |
| Mildly impaired | −2 and −1 | 7–6 | 65–70 | 70–84 borderline |
| severely impaired | <−2 as | <5 | >70 | <70 deficit |
| Typical n = 13 | Atypical n = 10 | p-Value | |
|---|---|---|---|
| Males | 8/13 | 7/10 | 1 |
| Pre-perinatal insults | 1/13 | 2/10 | 0.4919 |
| Epilepsy family history | 0/13 | 5/10 | 0.01769 ** |
| Delayed language development | 2/13 | 5/10 | 0.183 * |
| Sleep disorders | 1/13 | 3/10 | 0.5812 |
| Age at epilepsy onset (mean) | 6 | 5.9 | 0.8019 |
| Epilepsy duration (mean) | 2 | 1.9 | 0.8015 |
| Total seizures during follow-up (mean) | 4 | 6 | 0.7606 |
| “Simple” motor focal seizures | 5/13 | 6/10 | 0.5683 |
| High seizure frequency | 4/13 | 3/10 | 0.4773 |
| Sleep IEDs activation | 2/13 | 5/10 | 0.09748 * |
| AEDs prescription | 7/13 | 5/10 | 1 |
| AEDs duration (years) | 3.5 | 5.6 | 0.1027 * |
| Low educational level | |||
| Father | 1/13 | 6/10 | 0.01939 ** |
| Mother | 1/13 | 5/10 | 0.04169 ** |
| Low income bracket | |||
| Father | 0/13 | 5/10 | 0.01331 ** |
| Mother | 2/13 | 7/10 | 0.02626 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varesio, C.; Zanaboni, M.P.; Salmin, E.C.; Totaro, C.; Totaro, M.; Ballante, E.; Pasca, L.; Veggiotti, P.; De Giorgis, V. Childhood Epilepsy with Centrotemporal Spikes: Clinical and Neuropsychological Outcomes 5 Years after Remission. Diagnostics 2020, 10, 931. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10110931
Varesio C, Zanaboni MP, Salmin EC, Totaro C, Totaro M, Ballante E, Pasca L, Veggiotti P, De Giorgis V. Childhood Epilepsy with Centrotemporal Spikes: Clinical and Neuropsychological Outcomes 5 Years after Remission. Diagnostics. 2020; 10(11):931. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10110931
Chicago/Turabian StyleVaresio, Costanza, Martina Paola Zanaboni, Elisa Carlotta Salmin, Chiara Totaro, Martina Totaro, Elena Ballante, Ludovica Pasca, Pierangelo Veggiotti, and Valentina De Giorgis. 2020. "Childhood Epilepsy with Centrotemporal Spikes: Clinical and Neuropsychological Outcomes 5 Years after Remission" Diagnostics 10, no. 11: 931. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10110931