EDTA-Anticoagulated Whole Blood for SARS-CoV-2 Antibody Testing by Electrochemiluminescence Immunoassay (ECLIA) and Enzyme-Linked Immunosorbent Assay (ELISA)

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Study Population
2.2. Data Collection and Measurements
2.3. Statistical Methods
3. Results
3.1. Baseline Characteristics
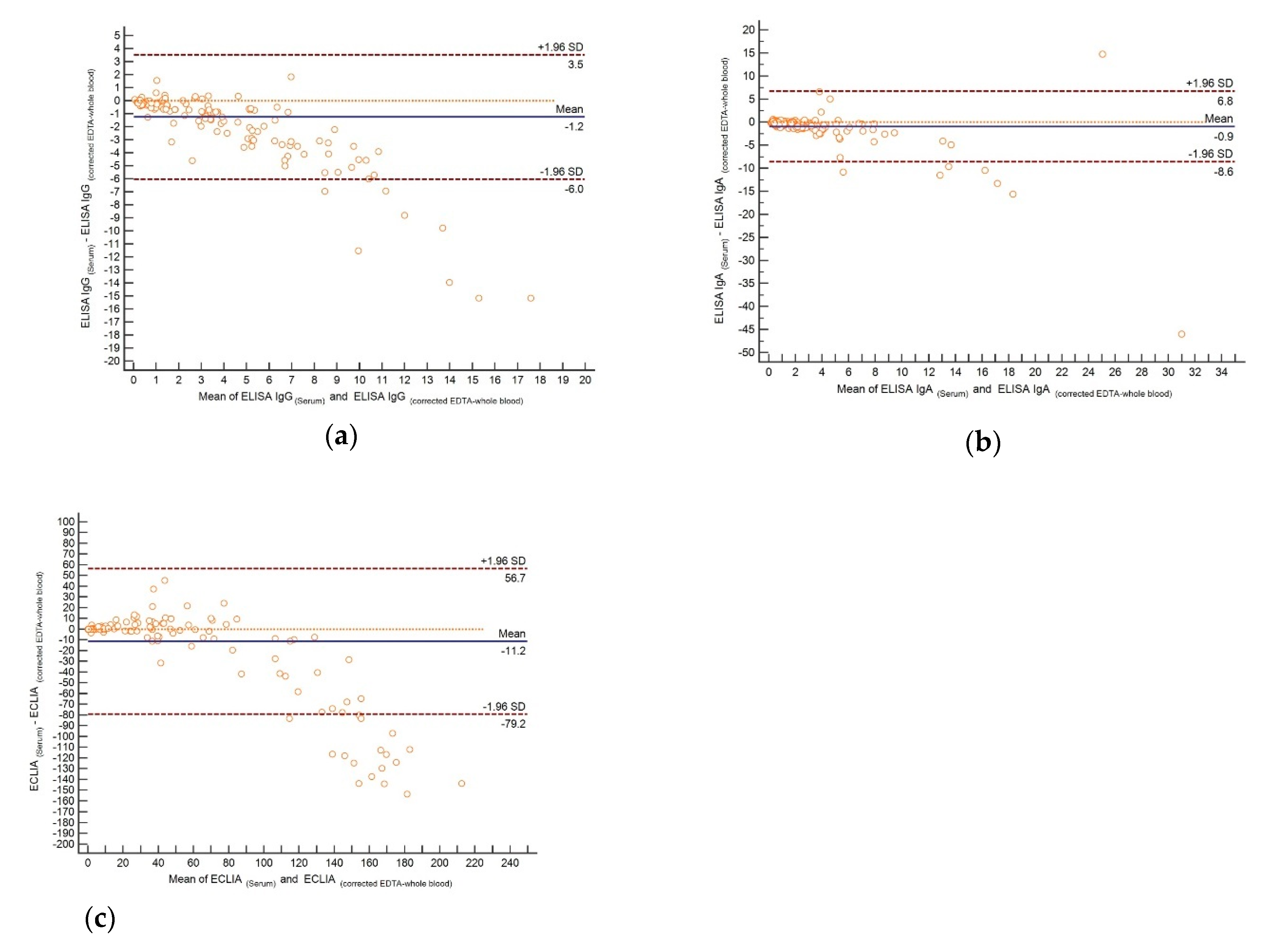
3.2. Association between Serum and Whole Blood Results
3.3. Detection Rates of Whole Blood Compared to Serum
3.4. Evaluation of Hematocrit Correction
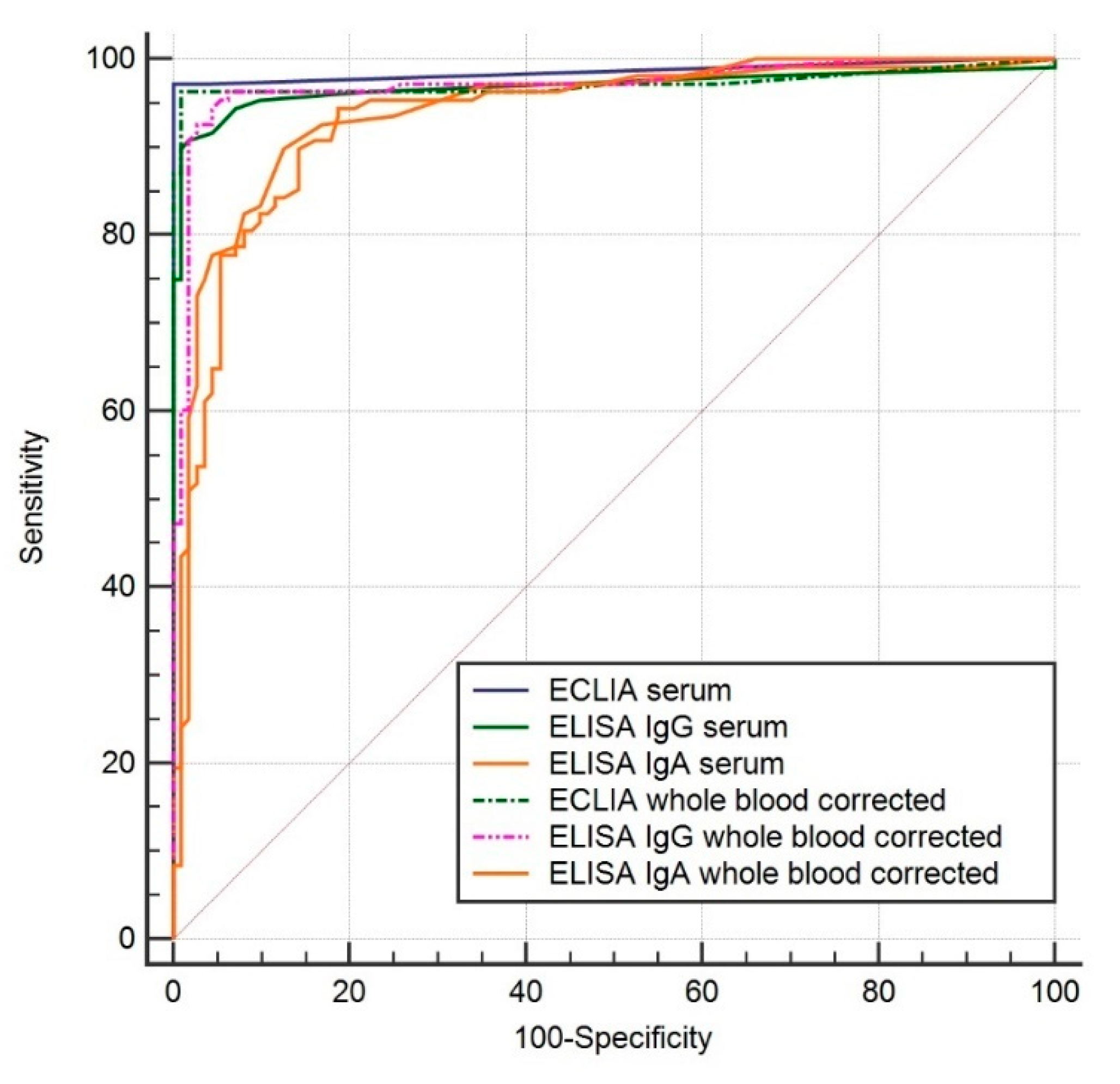
3.5. Diagnostic Sensitivity and Specificity of Serum and Whole Blood
3.6. Diagnostic Accuracy of Whole Blood Assays
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dramé, M.; Teguo, M.T.; Proye, E.; Hequet, F.; Hentzien, M.; Kanagaratnam, L.; Godaert, L. Should RT-PCR be considered a gold standard in the diagnosis of Covid-19? J. Med. Virol. 2020. [CrossRef]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody Responses to Sars-Cov-2 in Patients with Covid-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Patel, R.; Babady, E.; Theel, E.S.; Storch, G.A.; Pinsky, B.A.; George, K.S.; Smith, T.C.; Bertuzzi, S. Report from the American Society for Microbiology Covid-19 International Summit, 23 March 2020: Value of Diagnostic Testing for Sars-Cov-2/Covid-19. mBio 2020, 11. [Google Scholar] [CrossRef] [Green Version]
- Stowell, S.; Guarner, J. Role of Serology in the Covid-19 Pandemic. Clin. Infect. Dis. 2020. [CrossRef]
- Theel, E.S.; Slev, P.; Wheeler, S.; Couturier, M.R.; Wong, S.J.; Kadkhoda, K. The Role of Antibody Testing for Sars-Cov-2: Is There One? J. Clin. Microbiol. 2020. [CrossRef]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses During Infection by Sars-Cov-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Zhao, R.; Li, M.; Song, H.; Chen, J.; Ren, W.; Feng, Y.; Gao, G.F.; Song, J.; Peng, Y.; Su, B.; et al. Early Detection of Sars-Cov-2 Antibodies in Covid-19 Patients as a Serologic Marker of Infection. Clin. Infect. Dis. 2020. [CrossRef]
- Kubina, R.; Dziedzic, A. Molecular and Serological Tests for Covid-19 a Comparative Review of Sars-Cov-2 Coronavirus Laboratory and Point-of-Care Diagnostics. Diagnostics 2020, 10, 434. [Google Scholar] [CrossRef]
- Allam, M.; Cai, S.; Ganesh, S.; Venkatesan, M.; Doodhwala, S.; Song, Z.; Hu, T.; Kumar, A.; Heit, J.; COVID-19 Study Group; et al. Covid-19 Diagnostics, Tools, and Prevention. Diagnostics 2020, 10, 409. [Google Scholar] [CrossRef]
- Ghaffari, A.; Meurant, R.; Ardakani, A. Covid-19 Serological Tests: How Well Do They Actually Perform? Diagnostics 2020, 10, 453. [Google Scholar] [CrossRef]
- Guo, L.; Ren, L.; Yang, S.; Xiao, M.; Chang, D.; Yang, F.; Cruz, C.S.D.; Wang, Y.; Wu, C.; Xiao, Y.; et al. Profiling Early Humoral Response to Diagnose Novel Coronavirus Disease (Covid-19). Clin. Infect. Dis. 2020. [CrossRef] [PubMed] [Green Version]
- Mallapaty, S. Will Antibody Tests for the Coronavirus Really Change Everything? Nature 2020, 580, 571–572. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K. In Vitro Diagnostic Assays for Covid-19: Recent Advances and Emerging Trends. Diagnostics 2020, 10, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryan, A.; Pepper, G.; Wener, M.H.; Fink, S.L.; Morishima, C.; Chaudhary, A.; Jerome, K.R.; Mathias, P.C.; Greninger, A.L. Performance Characteristics of the Abbott Architect Sars-Cov-2 Igg Assay and Seroprevalence in Boise, Idaho. J. Clin. Microbiol. 2020. [CrossRef]
- Okba, N.M.; Müller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; De Bruin, E.; Chandler, F.D.; et al. Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibody Responses in Coronavirus Disease 2019 Patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Padoan, A.; Cosma, C.; Sciacovelli, L.; Faggian, D.; Plebani, M. Analytical Performances of a Chemiluminescence Immunoassay for Sars-Cov-2 Igm/Igg and Antibody Kinetics. Clin. Chem. Lab. Med. 2020, 58, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Lan, J.; Ge, J.; Yu, J.; Shan, S.; Zhou, H.; Fan, S.; Zhang, Q.; Shi, X.; Wang, Q.; Zhang, L.; et al. Structure of the Sars-Cov-2 Spike Receptor-Binding Domain Bound to the Ace2 Receptor. Nature 2020, 581, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Wijngaert, S.V.D.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of Two Automated and Three Rapid Lateral Flow Immunoassays for the Detection of Anti-Sars-Cov-2 Antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef]
- Jaaskelainen, A.J.; Kekalainen, E.; Kallio-Kokko, H.; Mannonen, L.; Kortela, E.; Vapalahti, O.; Kurkela, S.; Lappalainen, M. Evaluation of Commercial and Automated Sars-Cov-2 Igg and Iga Elisas Using Coronavirus Disease (Covid-19) Patient Samples. Eurosurveillance 2020, 25, 2000603. [Google Scholar] [CrossRef]
- Hoffman, T.; Nissen, K.; Krambrich, J.; Ronnberg, B.; Akaberi, D.; Esmaeilzadeh, M.; Salaneck, E.; Lindahl, J.; Lundkvist, A. Evaluation of a Covid-19 Igm and Igg Rapid Test; an Efficient Tool for Assessment of Past Exposure to Sars-Cov-2. Infect. Ecol. Epidemiol. 2020, 10, 1754538. [Google Scholar]
- Gaillard, H.M.; Hamilton, G.C. Hemoglobin/Hematocrit and Other Erythrocyte Parameters. Emerg. Med. Clin. N. Am. 1986, 4, 15–40. [Google Scholar]
- Tang, R.; Yang, H.; Choi, J.R.; Gong, Y.; You, M.; Wen, T.; Li, A.; Li, X.; Xu, B.; Zhang, S.; et al. Capillary Blood for Point-of-Care Testing. Crit. Rev. Clin. Lab. Sci. 2017, 54, 294–308. [Google Scholar] [CrossRef] [PubMed]
- Hoenderboom, B.M.; Van Ess, E.; Broek, I.V.D.; Van Loo, I.; Hoebe, C.; Ouburg, S.; Morré, S.A. Chlamydia Trachomatis Antibody Detection in Home-Collected Blood Samples for Use in Epidemiological Studies. J. Microbiol. Methods 2018, 144, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Kiya, G.T.; Zewudie, F.M. Comparison of Three-Fold Converted Hematocrit and Micro-Hematocrit in Pregnant Women. PLoS ONE 2019, 14, e0220740. [Google Scholar] [CrossRef] [Green Version]
- Toprak, B.; Yalcin, H.; Arı, E.; Çolak, A.; Ari, E. Interference in Electrochemiluminescence Acth Assay. Ann. Clin. Biochem. Int. J. Lab. Med. 2016, 53, 699–701. [Google Scholar] [CrossRef]
- Bowen, R.A.; Remaley, A.T. Interferences from Blood Collection Tube Components on Clinical Chemistry Assays. Biochem. Medica 2014, 24, 31–44. [Google Scholar]
- Tate, J.; Ward, G. Interferences in Immunoassay. Clin. Biochem. Rev. 2004, 25, 105–120. [Google Scholar]



{kind=link}
{kind=link}
| Serum | Whole Blood Corrected for Hematocrit | |||
|---|---|---|---|---|
| Sensitivity% [95% CI] | Specificity% [95% CI] | Sensitivity% [95% CI] | Specificity% [95% CI] | |
| IgG ELISA | 88% [80, 93] | 99% [95, 99.8] | 93% [86, 96] | 97% [93, 99] |
| (97/110) | (112/113) | (102/110) | (110/113) | |
| IgA ELISA | 78% [70, 85] | 93% [87, 96] | 84% [76, 89] | 89% [81, 93] |
| (86/110) | (105/113) | (92/110) | (100/113) | |
| ECLIA | 97% [92, 99] | 100% [97, 100] | 96% [91, 99] | 99% [95, 99.8] |
| (107/110) | (113/113) | (106/110) | (112/113) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovac, M.; Risch, L.; Thiel, S.; Weber, M.; Grossmann, K.; Wohlwend, N.; Lung, T.; Hillmann, D.; Ritzler, M.; Bigler, S.; et al. EDTA-Anticoagulated Whole Blood for SARS-CoV-2 Antibody Testing by Electrochemiluminescence Immunoassay (ECLIA) and Enzyme-Linked Immunosorbent Assay (ELISA). Diagnostics 2020, 10, 593. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080593
Kovac M, Risch L, Thiel S, Weber M, Grossmann K, Wohlwend N, Lung T, Hillmann D, Ritzler M, Bigler S, et al. EDTA-Anticoagulated Whole Blood for SARS-CoV-2 Antibody Testing by Electrochemiluminescence Immunoassay (ECLIA) and Enzyme-Linked Immunosorbent Assay (ELISA). Diagnostics. 2020; 10(8):593. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080593
Chicago/Turabian StyleKovac, Marc, Lorenz Risch, Sarah Thiel, Myriam Weber, Kirsten Grossmann, Nadja Wohlwend, Thomas Lung, Dorothea Hillmann, Michael Ritzler, Susanna Bigler, and et al. 2020. "EDTA-Anticoagulated Whole Blood for SARS-CoV-2 Antibody Testing by Electrochemiluminescence Immunoassay (ECLIA) and Enzyme-Linked Immunosorbent Assay (ELISA)" Diagnostics 10, no. 8: 593. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080593