Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
- To the best of our knowledge, this study is the first that propose a balancing methodology for three classes healthy, partial, and ruptured tears based on hybrid class balancing and real-time data augmentation.
- This study propose a customized ResNet-14 CNN model without transfer learning to detect three classes of ACL.
- We perform an extensive experimental validation of the proposed approaches in term of sensitivity, specificity, precision, recall, F1- measure, receiver operating curve (ROC), area under curve (AUC).
2. Related Work
3. Materials and Methods
3.1. Dataset
3.2. Data Pre-Processing
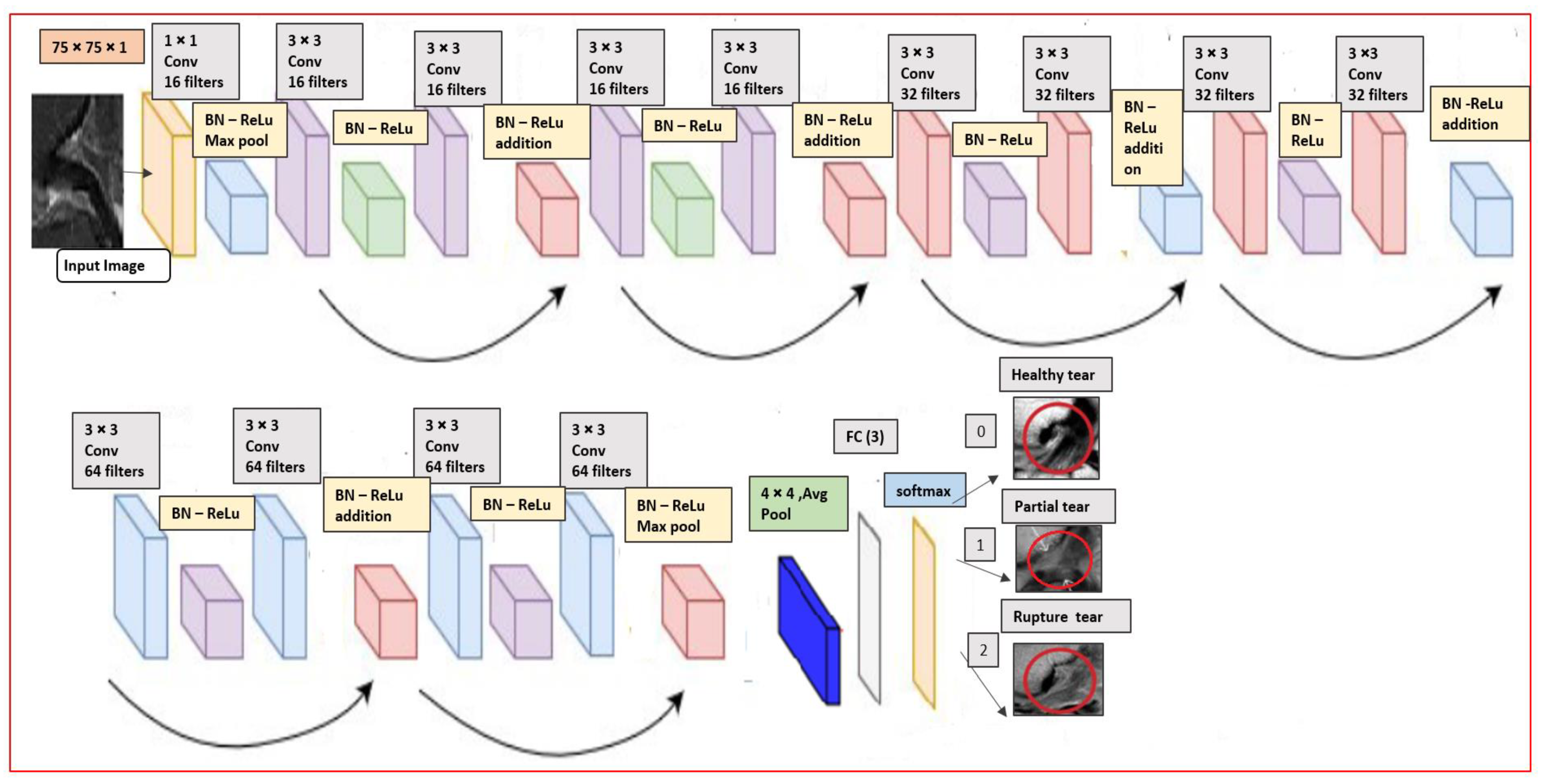
3.3. Our Proposed Custom ResNet-14 Architecture
4. Experimental Results
4.1. Experimental Setup
4.2. Train/Test Split
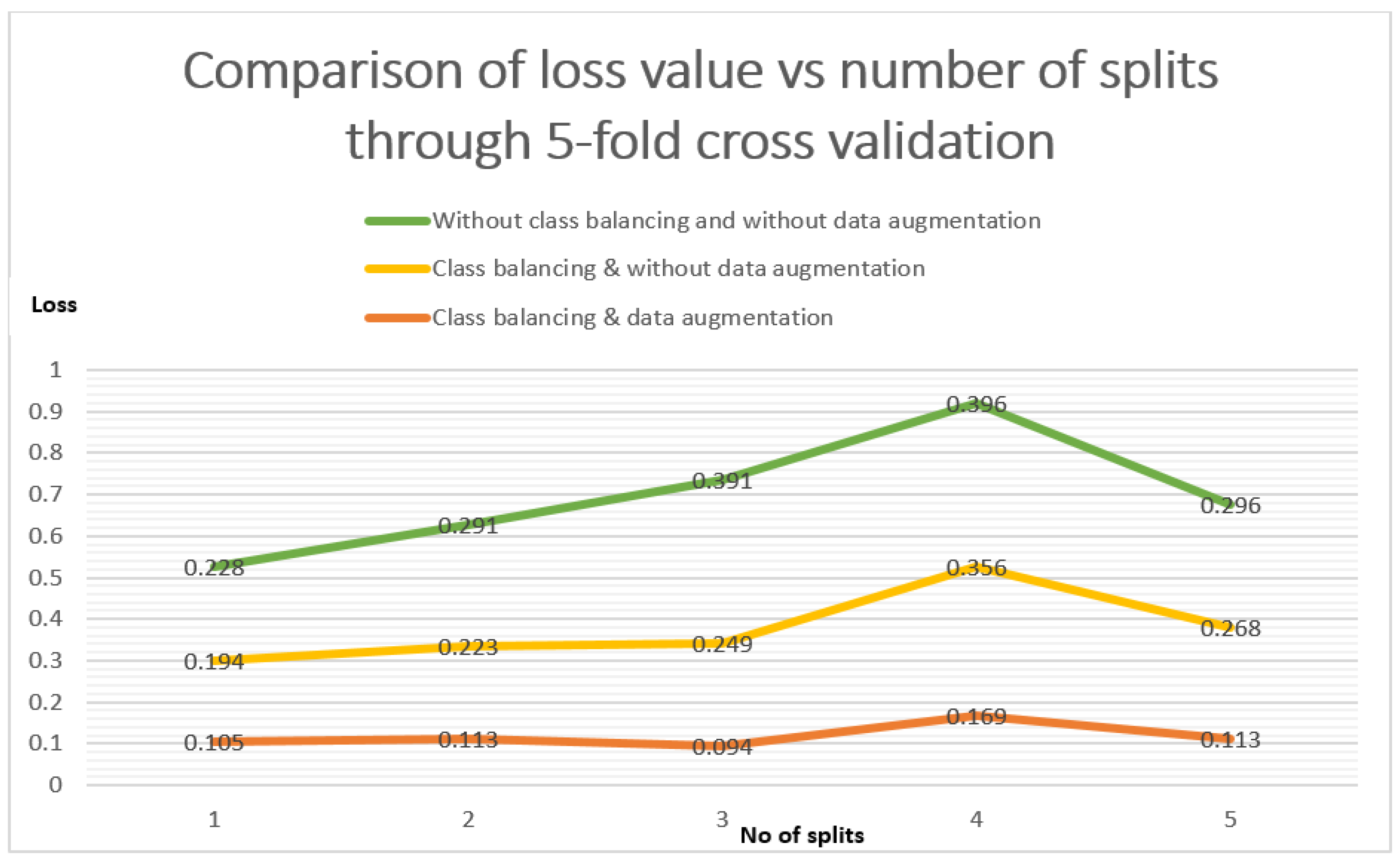
4.3. K- Fold Cross-Validation
4.4. Prediction Performance of Proposed ResNet
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zantop, T.; Petersen, W.; Fu, F.H. Anatomy of the anterior cruciate ligament. Oper. Tech. Orthop. 2005, 15, 20–28. [Google Scholar] [CrossRef]
- Musahl, V.; Karlsson, J. Anterior cruciate ligament tear. N. Engl. J. Med. 2019, 20, 2135–2142. [Google Scholar] [CrossRef] [PubMed]
- Naraghi, A.M.; White, L.M. Imaging of athletic injuries of knee ligaments and menisci: Sports imaging series. Radiology 2016, 281, 23–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalid, V.; Schønheyder, H.C.; Larsen, L.H.; Nielsen, P.T.; Kappel, A.; Thomsen, T.R.; Aleksyniene, R.; Lorenzen, J.; Ørsted, I.; Simonsen, O.; et al. Multidisciplinary Diagnostic Algorithm for Evaluation of Patients Presenting with a Prosthetic Problem in the Hip or Knee: A Prospective Study. Diagnostics 2020, 10, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prodromos, C.C.; Han, Y.; Rogowski, J.; Joyce, B.; Shi, K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy 2007, 23, 1320–1325. [Google Scholar] [CrossRef] [PubMed]
- Kopkow, C.; Lange, T.; Hoyer, A.; Lützner, J.; Schmitt, J. Physical tests for diagnosing anterior cruciate ligament rupture. Cochrane. Database Syst. Rev. 2018, 2018, 12. [Google Scholar]
- Nenezic, D.; Kocijancic, I. The value of the sagittal-oblique MRI technique for injuries of the anterior cruciate ligament in the knee. Radiol. Oncol. 2013, 47, 19–25. [Google Scholar] [CrossRef]
- Huda, W.; Abrahams, R.B. X-ray-based medical imaging and resolution. AJR Am. J. Roentgenol. 2015, 204, W393–W397. [Google Scholar] [CrossRef]
- Martin, T.; Janzen, C.; Li, X.; Del Rosario, I.; Chanlaw, T.; Choi, S.; Armstrong, T.; Masamed, R.; Wu, H.H.; Devaskar, S.U.; et al. Characterization of Uterine Motion in Early Gestation Using MRI-Based Motion Tracking. Diagnostics 2020, 10, 840. [Google Scholar] [CrossRef]
- Dachena, C.; Casu, S.; Fanti, A.; Lodi, M.B.; Mazzarella, G. Combined Use of MRI, fMRIand Cognitive Data for Alzheimer’s Disease: Preliminary Results. Appl. Sci. 2019, 9, 3156. [Google Scholar] [CrossRef] [Green Version]
- Kocabey, Y.; Tetik, O.; Isbell, W.M.; Atay, O.A.; Johnson, D.L. The value of clinical examination versus magnetic resonance imaging in the diagnosis of meniscal tears and anterior cruciate ligament rupture. Arthroscopy 2004, 20, 696–700. [Google Scholar] [CrossRef]
- Hong, S.H.; Choi, J.Y.; Lee, G.K.; Choi, J.A.; Chung, H.W.; Kang, H.S. Grading of anterior cruciate ligament injury. Diagnostic efficacy of oblique coronal magnetic resonance imaging of the knee. J. Comput. Assist. Tomogr. 2003, 27, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, M.A.; Ghani, M.K.A.; Arunkumar, N.A.; Mostafa, S.A.; Abdullah, M.K.; Burhanuddin, M.A. Trainable model for segmenting and identifying Nasopharyngeal carcinoma. Comput. Electr. Eng. 2018, 71, 372–387. [Google Scholar] [CrossRef]
- Ghani, M.K.A.; Mohammed, M.A.; Arunkumar, N.; Mostafa, S.A.; Ibrahim, D.A.; Abdullah, M.K.; Jaber, M.M.; Abdulhay, E.; Ramirez-Gonzalez, G.; Burhanuddin, M.A. Decision-level fusion scheme for nasopharyngeal carcinoma identification using machine learning techniques. Neural Comput. Appl. 2020, 32, 625–638. [Google Scholar] [CrossRef]
- Obaid, O.I.; Mohammed, M.A.; Ghani, M.K.A.; Mostafa, A.; Taha, F. Evaluating the performance of machine learning techniques in the classification of Wisconsin Breast Cancer. Int. J. Eng. Technol. 2018, 7, 160–166. [Google Scholar]
- Norouzi, A.; Rahim, M.S.M.; Altameem, A.; Saba, T.; Rad, A.E.; Rehman, A.; Uddin, M. Medical image segmentation methods, algorithms, and applications. IETE Tech. Rev. 2014, 31, 199–213. [Google Scholar] [CrossRef]
- Al-Waisy, A.S.; Al-Fahdawi, S.; Mohammed, M.A.; Abdulkareem, K.H.; Mostafa, S.A.; Maashi, M.S.; Arif, M.; Garcia-Zapirain, B. COVID-CheXNet: Hybrid deep learning framework for identifying COVID-19 virus in chest X-rays images. Soft Comput. 2020. [Google Scholar] [CrossRef]
- Mohammed, M.A.; Abdulkareem, K.H.; Mostafa, S.A.; Khanapi Abd Ghani, M.; Maashi, M.S.; Garcia-Zapirain, B.; Oleagordia, I.; Alhakami, H.; AL-Dhief, F.T. Voice Pathology Detection and Classification Using Convolutional Neural Network Model. Appl. Sci. 2020, 10, 3723. [Google Scholar] [CrossRef]
- Varma, M.; Lu, M.; Gardner, R. Automated abnormality detection in lower extremity radiographs using deep learning. Nat. Mach. Intell. 2019, 12, 578–583. [Google Scholar] [CrossRef]
- Tiulpin, A.; Saarakkala, S. Automatic Grading of Individual Knee Osteoarthritis Features in Plain Radiographs Using Deep Convolutional Neural Networks. Diagnostics 2020, 10, 932. [Google Scholar] [CrossRef]
- Mazlan, S.; Ayob, M.; Bakti, Z. Anterior cruciate ligament (ACL) injury classification system using support vector machine (SVM). In Proceedings of the 2017 International Conference on Engineering Technology and Technopreneurship (ICE2T), Kuala Lumpur, Malaysia, 18–20 September 2017; pp. 1–5. [Google Scholar]
- Ashinsky, B.G.; Coletta, C.E.; Bouhrara, M.; Lukas, V.A.; Boyle, J.M.; Reiter, D.A.; Neu, C.P.; Goldberg, I.G.; Spencer, R.G. Machine learning classification of OARSI-scored human articular cartilage using magnetic resonance imaging. Osteoarthr. Cartil. 2015, 23, 1704–1712. [Google Scholar]
- Štajduhar, I.; Mamula, M.; Miletić, D.; Ünal, G. Semi-automated detection of anterior cruciate ligament injury from MRI. Comput. Methods. Programs Biomed. 2017, 140, 151–164. [Google Scholar] [PubMed]
- Lao, Y.; Jia, B.; Yan, P.; Pan, M.; Hui, X.; Li, J.; Luo, W.; Li, X.; Han, J.; Yan, P.; et al. Diagnostic accuracy of machine-learning-assisted detection for anterior cruciate ligament injury based on magnetic resonance imaging: Protocol for a systematic review and meta-analysis. Medicine 2019, 9, 18324. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Ismail, S.A.; Pappas, E. Detecting the presence of anterior cruciate ligament injury based on gait dynamics disparity and neural networks. Artif. Intell. Rev. 2020, 53, 3153–3176. [Google Scholar]
- Manna, S.; Bhattacharya, S.; Pal, U. Self-Supervised Representation Learning for Detection of ACL Tear Injury in Knee MRI. arXiv 2020, arXiv:2007.07761. [Google Scholar]
- Bien, N.; Rajpurkar, P.; Ball, R.L.; Irvin, J.; Park, A.; Jones, E.; Bereket, M.; Patel, B.N.; Yeom, K.W.; Shpanskaya, K.; et al. Deep-learning-assisted diagnosis for knee magnetic resonance imaging: Development and retrospective validation of MRNet. PLoS Med. 2018, 15, e1002699. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Cham, Germany, 2015; pp. 234–241. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Zbontar, J.; Knoll, F.; Sriram, A.; Murrell, T.; Huang, Z.; Muckley, M.J.; Defazio, A.; Stern, R.; Johnson, P.; Bruno, M.; et al. fastMRI: An open dataset and benchmarks for accelerated MRI. arXiv 2018, arXiv:1811.08839. [Google Scholar]
- Chang, P.D.; Wong, T.T.; Rasiej, M.J. Deep Learning for Detection of Complete Anterior Cruciate Ligament Tear. J. Digit. Imaging 2019, 32, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Guan, B.; Zhou, Z.; Samsonov, A.; Rosas, H.; Lian, K.; Sharma, R.; Kanarek, A.; Kim, J.; Guermazi, A.; et al. Fully Automated Diagnosis of Anterior Cruciate Ligament Tears on Knee MR Images by Using Deep Learning. Radiol. Artif. Intell. 2019, 1, 180091. [Google Scholar] [CrossRef] [PubMed]
- El-Sawy, A.; EL-Bakry, H.M.; Loey, M. CNN for handwritten arabic digits recognition based on LeNet-5. In Proceedings of the International Conference on Advanced Intelligent Systems and Informatics, Cairo, Egypt, 24–26 October 2016; Springer: Cham, Germany, 2016; pp. 566–575. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Wang, L.; Guo, S.; Huang, W.; Qiao, Y. Places205-vggnet models for scene recognition. arXiv 2015, arXiv:1508.01667. [Google Scholar]
- Namiri, N.K.; Flament, I.; Astuto, B.; Shah, R.; Tibrewala, R.; Caliva, F.; Link, T.M.; Pedoia, V.; Majumdar, S. Deep Learning for Hierarchical Severity Staging of Anterior Cruciate Ligament Injuries from MRI. Radiol. Artif. Intell 2020, 2, 190207. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, M.; Zhou, Y.; Lu, G.; Zhou, Q. Deep Learning Approach for Anterior Cruciate Ligament Lesion Detection: Evaluation of Diagnostic Performance Using Arthroscopy as the Reference Standard. J. Magn. Reson. Imaging 2020, 52, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Irmakci, I.; Anwar, S.M.; Torigian, D.A.; Bagci, U. Deep Learning for Musculoskeletal Image Analysis. In Proceedings of the 2019 53rd Asilomar Conference on Signals, Systems, and Computers, Pacific Grove, CA, USA, 3–6 November 2019; pp. 1481–1485. [Google Scholar]
- Tsai, C.H.; Kiryati, N.; Konen, E.; Eshed, I.; Mayer, A. Knee Injury Detection using MRI with Efficiently-Layered Network (ELNet). arXiv 2005, arXiv:2005.02706. [Google Scholar]
- Tan, M.; Le, Q.V. Efficientnet: Rethinking model scaling for convolutional neural networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- Tiulpin, A.; Thevenot, J.; Rahtu, E.; Saarakkala, S. A novel method for automatic localization of joint area on knee plain radiographs. In Proceedings of the Scandinavian Conference on Image Analysis, Tromsø, Norway, 12–14 June 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 290–301. [Google Scholar]
- Zhang, C. Medical Image Classification under Class Imbalance. Ph.D. Thesis, Iowa State University, Ames, IA, USA, 2019. [Google Scholar]
- Small, H.; Ventura, J. Handling Unbalanced Data in Deep Image Segmentation; University of Colorado: Boulder, CO, USA, 2017. [Google Scholar]
- Johnson, J.M.; Khoshgoftaar, T.M. Survey on deep learning with class imbalance. J. Big Data 2019, 6, 27. [Google Scholar] [CrossRef]
- Mikołajczyk, A.; Grochowski, M. Data augmentation for improving deep learning in image classification problem. In Proceedings of the 2018 International Interdisciplinary PhD workshop (IIPhDW), Swinoujście, Poland, 9–12 May 2018; pp. 117–122. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In Proceedings of the 32nd International Conference on International Conference on Machine Learning, Lile, France, 6–11 July 2015. [Google Scholar]
- Kingma, D.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Tang, Z.; Gao, Y.; Karlinsky, L.; Sattigeri, P.; Feris, R.; Metaxas, D. OnlineAugment: Online Data Augmentation with Less Domain Knowledge. arXiv 2007, arXiv:2007.09271. [Google Scholar]
- Safdar, M.F.; Alkobaisi, S.S.; Zahra, F.T. A Comparative Analysis of Data Augmentation Approaches for Magnetic Resonance Imaging (MRI) Scan Images of Brain Tumor. Acta Inform. Med. 2020, 28, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Maqsood, M.; Nazir, F.; Khan, U.; Aadil, F.; Awan, K.M.; Mehmood, I.; Song, O.Y. A data augmentation-based framework to handle class imbalance problem for Alzheimer’s stage detection. IEEE Access 2019, 7, 115528–115539. [Google Scholar]
- Ali, Y.; Farooq, A.; Alam, T.M.; Farooq, M.S.; Awan, M.J.; Baig, T.I. Detection of Schistosomiasis Factors Using Association Rule Mining. IEEE Access 2019, 7, 186108–186114. [Google Scholar]
- Rai, R.; Sisodia, D.S. Real-time data augmentation based transfer learning model for breast cancer diagnosis using histopathological images. In Advances in Biomedical Engineering and Technology; Springer: Singapore, 2020; pp. 473–488. [Google Scholar]
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data 2019, 6, 60. [Google Scholar]
- Keras Documentation Image Preprocessing. Available online: https://foroit.com/keras-docs/1.2.0/preprocessing/image/ (accessed on 10 June 2020).
- Mohammed, M.A.; Abdulkareem, K.H.; Garcia-Zapirain, B.; Mostafa, S.A.; Maashi, M.S. A Comprehensive Investigation of Machine Learning Feature Extraction and Classification Methods for Automated Diagnosis of COVID-19 Based on X-ray Images. Comput. Mater. Contin. 2021, 66, 3289–3310. [Google Scholar] [CrossRef]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Ismail, A.W.; Shabbir, H. Acceleration of Knee MRI Cancellous Bone Classification on Google Colaboratory Using Convolutional Neural Network. Int. J. Adv. Trends Comput. Sci. 2019, 8, 83–88. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade Stages | Injuries/Symptoms |
|---|---|
| Grade-I | Intra-ligament injury No changes in the ligaments length |
| Grade-II | Intra-Ligament injury Change in ligament length Partial tears |
| Grade-III | Complete ligament disruption |
| Series No | Knee LR | ROIX | ROIY | ROIZ | ROI Height | ROI Width | ROI Depth | Volume Filename | ACL Diagnosis |
|---|---|---|---|---|---|---|---|---|---|
| 5 | 0 | 126 | 96 | 14 | 78 | 79 | 4 | 502889-5.pck | 0 |
| 5 | 0 | 116 | 177 | 13 | 83 | 79 | 4 | 507277-5.pck | 1 |
| 5 | 1 | 113 | 140 | 9 | 89 | 96 | 4 | 496580-5.pck | 2 |
| Layer Name | Output Size | Layer Information |
|---|---|---|
| Input layer | 75 × 75 × 1 | |
| conv1 | 75 × 75 | 1 × 1, strides 2, 16 |
| conv2_d (1 block) | 75 × 75 | 3 × 3, maxpool stride 2 3 × 3, 16 |
| conv2_d (2 block) | 75 × 75 | 3 × 3, 16 |
| conv3_d (1 block) | 38 × 38 | 3 × 3, 32 |
| conv3_d (2 block) | 38 × 38 | 3 × 3, 32 |
| conv4_d (1 block) | 19 × 19 | 3 × 3, 64 |
| conv4_d (2 block) | 19 × 19 | maxpool 3 × 3, 64 |
| Average Pool | 4 × 4 | 4 × 4 average pool |
| Fully Connected Layer | Three classes | 64 × 3 fully connections |
| Softmax | output three classes | Healthy, partial and rupture |
| Total parameters | 179,075 | |
| Sr.No | Augmentation Arguments | Description |
|---|---|---|
| 1. | featurewise_center | Set input mean to 0 over the dataset |
| 2. | featurewise_std_normalization | Divide inputs by standard deviation of dataset |
| 3. | zca_epsilon = 1 × 10−6 | Epsilon for Zero-phase whitening (ZCA) whitening |
| 4. | fill mode = ‘nearest’ | Set mode for filling points outside the input boundaries |
| 5. | horizontal flip = True | Randomly flip images horizontally |
| 6. | vertical flip = True | Randomly flip images vertically |
| ResNet-14 CNN Model Tested Approaches | Test Loss | Test Accuracy |
|---|---|---|
| Without class balancing and data augmentation (5-fold cross-validation) | 1.294 | 0.805 |
| Without class balancing but data augmentation (5-fold cross-validation) | 1.089 | 0.774 |
| Class balancing and without data augmentation (random splitting) | 0.537 | 0.884 |
| Class balancing and data augmentation (random splitting) | 0.526 | 0.895 |
| Class balancing and data augmentation (3-fold cross-validation) | 0.533 | 0.895 |
| Class balancing and data augmentation (5-fold cross-validation) | 0.466 | 0.919 |
| Evaluation Metrics of ResNet-14 CNN | |||||
|---|---|---|---|---|---|
| Multi Classes | |||||
| Approaches | Evaluation | Healthy Tear | Partial Tear | Full Torn | Average |
| Without class balancing and data augmentation (5-fold cross-validation) | Precision | 0.85 | 0.57 | 0.57 | 0.663 |
| Sensitivity | 0.96 | 0.39 | 0.22 | 0.523 | |
| F1-Score | 0.90 | 0.47 | 0.31 | 0.563 | |
| Specificity | 0.78 | 0.86 | 0.95 | 0.863 | |
| Accuracy | 0.81 | ||||
| AUC | 0.87 | 0.81 | 0.91 | 0.863 | |
| Without class balancing with data augmentation (5-fold cross validation) | Precision | 0.83 | 0.47 | 0.47 | 0.590 |
| Sensitivity | 0.94 | 0.29 | 0.22 | 0.483 | |
| F1-Score | 0.88 | 0.36 | 0.30 | 0.513 | |
| Specificity | 0.70 | 0.78 | 0.96 | 0.813 | |
| Accuracy | 0.77 | ||||
| AUC | 0.83 | 0.76 | 0.91 | 0.833 | |
| Hybrid class balancing without data augmentation (Random Splitting) | Precision | 0.87 | 0.81 | 0.96 | 0.880 |
| Sensitivity | 0.85 | 0.79 | 0.99 | 0.877 | |
| F1-score | 0.86 | 0.80 | 0.98 | 0.880 | |
| Specificity | 0.90 | 0.92 | 0,99 | 0.910 | |
| Accuracy | 0.88 | ||||
| AUC | 0.96 | 0.95 | 0.99 | 0.967 | |
| Hybrid class balancing with data augmentation (random splitting) | Precision | 0.89 | 0.84 | 0.94 | 0.890 |
| Sensitivity | 0.86 | 0.81 | 0.99 | 0.887 | |
| F1- score | 0.88 | 0.83 | 0.97 | 0.893 | |
| Specificity | 0.91 | 0.92 | 0.99 | 0.940 | |
| Accuracy | 0.90 | ||||
| AUC | 0.97 | 0.96 | 0.99 | 0.973 | |
| Hybrid class balancing with data augmentation (3-fold cross validation) | Precision | 0.90 | 0.83 | 0.94 | 0.890 |
| Sensitivity | 0.87 | 0.80 | 0.99 | 0.887 | |
| F1- score | 0.88 | 0.82 | 0.97 | 0.890 | |
| Specificity | 0.91 | 0.92 | 0.99 | 0.940 | |
| Accuracy | 0.90 | ||||
| AUC | 0.97 | 0.94 | 0.99 | 0.967 | |
| Hybrid class balancing with data augmentation (5-fold cross validation) | Precision | 0.92 | 0.87 | 0.96 | 0.917 |
| Sensitivity | 0.89 | 0.87 | 0.99 | 0.917 | |
| F1-score | 0.90 | 0.87 | 0.98 | 0.917 | |
| Specificity | 0.93 | 0.92 | 0.99 | 0.947 | |
| Accuracy | 0.92 | ||||
| AUC | 0.98 | 0.97 | 0.99 | 0.980 | |
| Author, Year | Model | Dataset | Target Output | Evaluation | ||||
|---|---|---|---|---|---|---|---|---|
| Accuracy | Sensitivity | Precision | Specificity | AUC | ||||
| Štajduhar et al. [23] | HOG+ Linear-kernel SVM (k = 10) | KneeMRI 917 (exams) | partial tear | - | - | - | - | 0.894 |
| ruptured tear | - | - | - | - | 0.943 | |||
| Bien et al., 2018 [27] | AlexNet | MRNet 1370 exams | ACL tear | 0.867 | 0.759 | - | 0.968 | 0.965 |
| abnormal | 0.850 | 0.879 | - | 0.714 | 0.937 | |||
| meniscus tear | 0.725 | 0.892 | 0.741 | 0.847 | ||||
| Logistic Regression | KneeMRI 917 exam | partial tear, ruptured tear | - | - | - | - | 0.911 | |
| Chang et al., 2019 [33] | Dynamic patch + ResNet | 260 MRI coronal volumes | partial AC, full torn | 0.967 | 1.00 | 0.938 | 0.933 | - |
| Liu et al., 2019 [34] | VGG16 | sagittal MR 175 (exams) | full thickness ACL tear, Intact ACL | - | 0.92 | - | 0.92 | 0.95 |
| DenseNet | - | 0.96 | - | 0.96 | 0.98 | |||
| Alex Net | - | 0.89 | - | 0.88 | 0.90 | |||
| Namiri et al., 2019 [39] | 2D CNN 3D CNN | NIH MRI 1243 (exams) | Intact ACL | - | 0.22 0.89 | - | 0.90 0.88 | - |
| 2D CNN 3D CNN | Partial tear | - | 0.75 0.25 | - | 1.00 0.92 | - | ||
| 2D CNN 3D CNN | Full tear | - | 0.82 0.76 | - | 0.94 1.00 | - | ||
| Zhang et al., 2020 [40] | 3D DenseNet | sagittal MR 408 (exams) | ACL tears Intact ACL | 0.957 0.943 0.899 | 0.976 0.952 0.912 | 0.940 0.952 0.869 | 0.944 0.909 0.886 | 0.960 0.946 0.859 |
| ResNet | ||||||||
| VGG16 | ||||||||
| Irmakci et al., 2020 [41] | AlexNet | MRNet 1370 exams | abnormal | 0.8583 | 0.978 | - | 0.400 | 0.891 |
| ACL tear | 0.833 | 0.685 | - | 0.954 | 0.938 | |||
| ResNet-18 | abnormal | 0.825 | 0.968 | - | 0.280 | 0.811 | ||
| ACL tear | 0.866 | 0.777 | - | 0.939 | 0.954 | |||
| GoogleLeNet | abnormal | 0.833 | 0.978 | - | 0.280 | 0.909 | ||
| ACL tear | 0.808 | 0.666 | - | 0.924 | 0.890 | |||
| Tsai et al., 2020 [42] | EfficientNet | MRNet 1370 | abnormal | 0.917 | 0.968 | - | 0.72 | 0.941 |
| ACL tear | 0.904 | 0.923 | - | 0.891 | 0.960 | |||
| ELNet 5 -fold | KneeMRI 917 exams | ruptured ACL | - | - | - | - | 0.913 | |
| Proposed Customized ResNet-14 5-fold cross-validation | KneeMRI 917 exams | ACL Intact | 0.92 | 0.89 | 0.92 | 0.93 | 0.98 | |
| partial tear | 0.91 | 0.87 | 0.87 | 0.92 | 0.97 | |||
| ruptured | 0.93 | 0.99 | 0.96 | 0.99 | 0.99 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javed Awan, M.; Mohd Rahim, M.S.; Salim, N.; Mohammed, M.A.; Garcia-Zapirain, B.; Abdulkareem, K.H. Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach. Diagnostics 2021, 11, 105. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010105
Javed Awan M, Mohd Rahim MS, Salim N, Mohammed MA, Garcia-Zapirain B, Abdulkareem KH. Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach. Diagnostics. 2021; 11(1):105. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010105
Chicago/Turabian StyleJaved Awan, Mazhar, Mohd Shafry Mohd Rahim, Naomie Salim, Mazin Abed Mohammed, Begonya Garcia-Zapirain, and Karrar Hameed Abdulkareem. 2021. "Efficient Detection of Knee Anterior Cruciate Ligament from Magnetic Resonance Imaging Using Deep Learning Approach" Diagnostics 11, no. 1: 105. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010105