SARS-CoV-2 in Mexico: Beyond Detection Methods, Scope and Limitations

 ,
,
Abstract
:1. Introduction
2. Symptoms and Transmission Routes of COVID-19
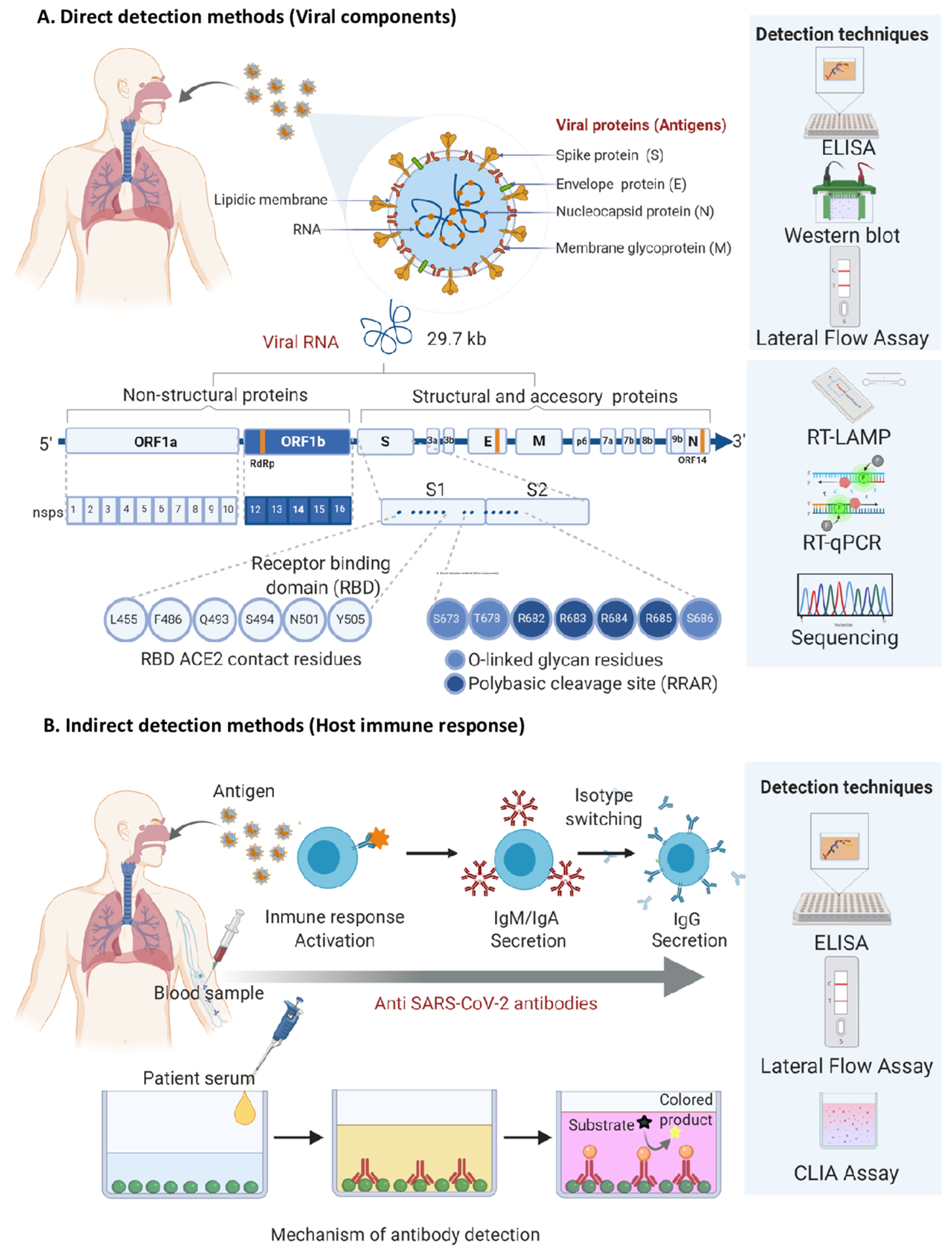
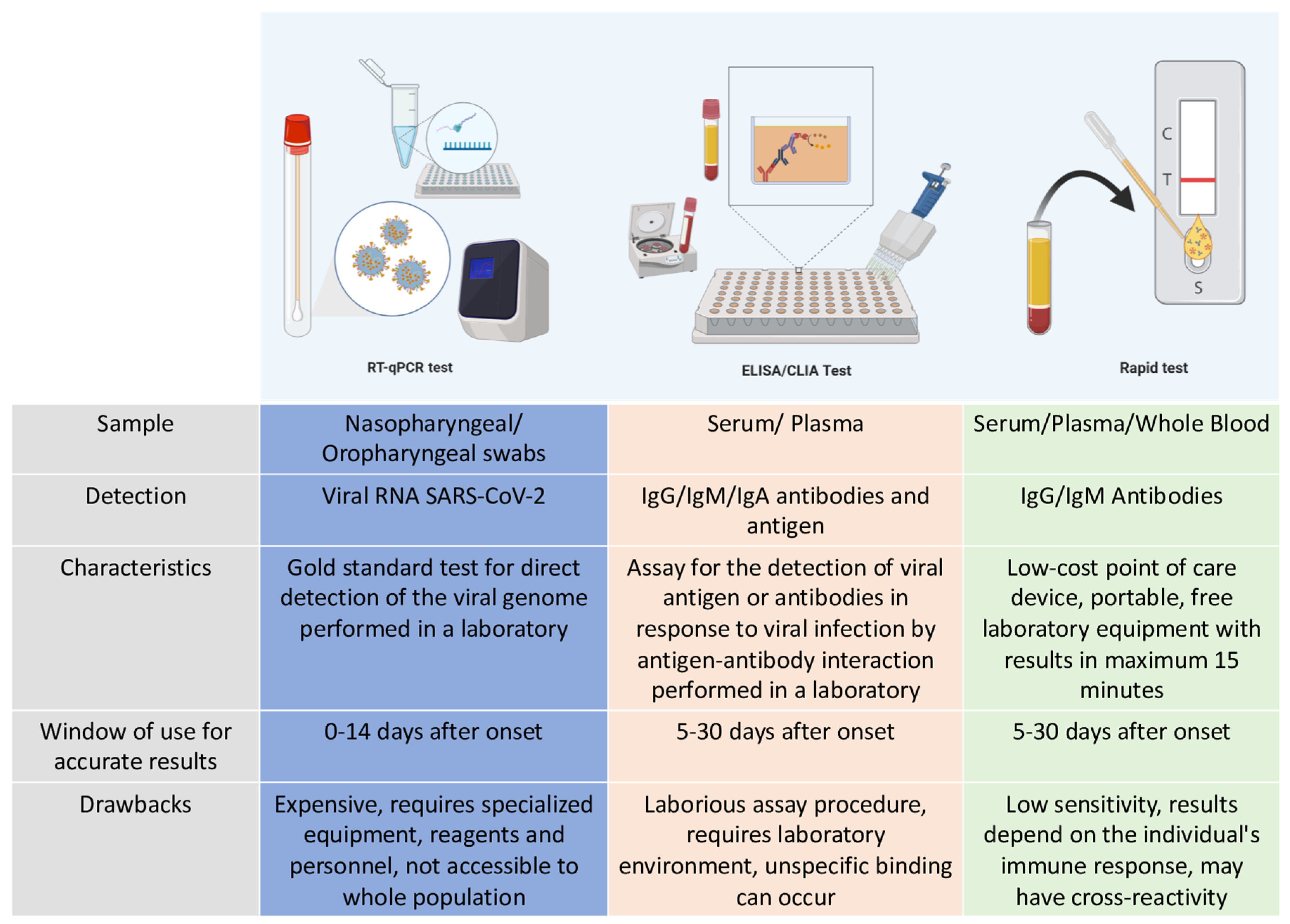
3. Diagnostic Tests for SARS-CoV-2
4. What Are Molecular Tests and How Do They Work to Identify COVID-19?
5. What Are Immunological Assays and How Do They Work to Detect COVID-19?
6. Interpretation of Results Obtained by SARS-CoV-2 Detection Methods in Mexico and Their Pitfalls
7. Future Prospect: Use of Point-Of-Care Tests as Tools to Detect COVID-19
Funding
Conflicts of Interest
References
- Ren, L.L.; Wang, Y.M.; Wu, Z.Q.; Xiang, Z.C.; Guo, L.; Xu, T.; Jiang, Y.Z.; Xiong, Y.; Li, Y.J.; Li, X.W.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015–1024. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochi, A.; Tagliari, A.; Forleo, G.; Fassini, G.; Tondo, C. Cardiac and arrhythmic complications in patients with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 1003–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef]
- Alharthy, A.; Faqihi, F.; Memish, Z.; Karakitsos, D. Fragile endothelium and brain dysregulated neurochemical activity in COVID-19. Acs Chem. Neurosci. 2020, 11, 2159–2162. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–Infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Sanche, S.; Lin, Y.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High contagiousness and rapid spread of severe acute respiratory syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef]
- Borysiak, M.; Thompson, M.; Posner, J. Translating diagnostic assays from the laboratory to the clinic: Analytical and clinical metrics for device development and evaluation. Lab Chip 2016, 16, 1293–1313. [Google Scholar] [CrossRef]
- Lalkhen, A.; McCluskey, A. Clinical tests: Sensitivity and specificity. Contin. Educ. Anaesth. Crit. Care Pain 2008, 8, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Trevethan, R. Sensitivity, specificity, and predictive values: Foundations, pliabilities, and pitfalls in research and practice. Front. Public Health 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Esmaeilzadeh, E.; Li, Y.; Bosch, R.; Li, J. SARS-CoV-2 detection in different respiratory sites: A systematic review and meta-analysis. Ebiomedicine 2020, 102903. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, S.; Fujisawa, S.; Nakakubo, S.; Kamada, K.; Yamashita, Y.; Fukumoto, T.; Sato, K.; Oguri, S.; Taki, K.; Senjo, H.; et al. Comparison of SARS-CoV-2 detection in nasopharyngeal swab and saliva. J. Infect. 2020, 81, e145–e147. [Google Scholar] [CrossRef]
- Azzi, L.; Carcano, G.; Gianfagna, F.; Grossi, P.; Gasperina, D.D.; Genoni, A.; Fasano, M.; Sessa, F.; Tettamanti, L.; Carinci, F.; et al. Saliva is a reliable tool to detect SARS-CoV-2. J. Infect. 2020, 81, e45–e50. [Google Scholar] [CrossRef]
- Vaz, S.N.; Santana, D.S.; Netto, E.M.; Pedroso, C.; Wang, W.K.; Santos, F.; Brites, C. Saliva is a reliable, non-invasive specimen for SARS-CoV-2 detection. Braz. J. Infect. Dis. Off. Publ. Braz. Soc. Infect. Dis. 2020, 24, 422–427. [Google Scholar] [CrossRef]
- China CDC. China CDC Primers and Probes for Detection 2019-nCoV. Available online: http://ivdc.chinacdc.cn/kyjz/202001/t20200121_211337.html (accessed on 27 August 2020).
- Institut Pasteur, Paris. Protocol: Real-Time RT-PCR Assays for the Detection of SARS-CoV-2. Available online: https://www.who.int/docs/default-source/coronaviruse/real-time-rt-pcr-assays-for-the-detectionof-sars-cov-2-institut-pasteur-paris.pdf?sfvrsn=3662fcb6_2 (accessed on 27 August 2020).
- Corman, V.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. A CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 27 August 2020).
- School of Public Health, The University of Hong Kong, Hong Kong (Leo Poon, Daniel Chu and Malik Peiris). Detection of 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases by RT-PCR. Available online: https://www.who.int/docs/default-source/coronaviruse/peiris-protocol-16-1-20.pdf?sfvrsn=af1aac73_4 (accessed on 27 August 2020).
- Department of Medical Sciences, Ministry of Public Health, Thailand. Diagnostic Detection of Novel Coronavirus 2019 by Real Time RT-PCR. Available online: https://www.who.int/docs/default-source/coronaviruse/conventional-rt-pcr-followed-by-sequencing-for-detection-of-ncov-rirl-nat-inst-health-t.pdf?sfvrsn=42271c6d_4 (accessed on 27 August 2020).
- Nao, N.; Shirato, K.; Katano, H.; Matsuyama, S.; Takeda, M. Detection of Second Case of 2019-nCoV Infection in Japan. Available online: https://www.who.int/docs/default-source/coronaviruse/method-niid-20200123-2.pdf?sfvrsn=fbf75320_7 (accessed on 27 August 2020).
- Xia, J.; Tong, J.; Liu, M.; Shen, Y.; Guo, D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J. Med. Virol. 2020, 92, 589–594. [Google Scholar] [CrossRef] [Green Version]
- Arora, R.; Goel, R.; Kumar, S.; Chhabra, M.; Saxena, S.; Manchanda, V.; Pumma, P. Evaluation of SARS-CoV-2 in tears of patients with moderate to severe COVID-19. Ophthalmology 2020. [Google Scholar] [CrossRef]
- Peng, L.; Liu, J.; Xu, W.; Luo, Q.; Chen, D.; Lei, Z.; Huang, Z.; Li, X.; Deng, K.; Lin, B.; et al. SARS-CoV-2 can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens. J. Med. Virol. 2020, 92, 1676–1680. [Google Scholar] [CrossRef]
- Zhen, W.; Manji, R.; Smith, E.; Berry, G. Comparison of four molecular in vitro diagnostic assays for the detection of SARS-CoV-2 in Nasopharyngeal specimens. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Iglói, Z.; Abou-Nouar, Z.A.K.; Weller, B.; Matheeussen, V.; Coppens, J.; Koopmans, M.; Molenkamp, R. Comparison of commercial real time reverse transcription PCR assays for the detection of SARS-CoV-2. J. Clin. Virol. 2020, 129, 104510. [Google Scholar] [CrossRef]
- Yu, H.Q.; Sun, B.Q.; Fang, Z.F.; Zhao, J.C.; Liu, X.Y.; Li, Y.M.; Sun, X.Z.; Liang, H.F.; Zhong, B.; Huang, Z.F.; et al. Distinct features of SARS-CoV-2-specific IgA response in COVID-19 patients. Eur. Respir. J. 2020, 56, 2001526. [Google Scholar] [CrossRef] [PubMed]
- Lou, B.; Li, T.; Zheng, S.; Su, Y.; Li, Z.; Liu, W.; Yu, F.; Ge, S.-X.; Da Zou, Q.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur. Respir. J. 2020, 56, 2000763. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.; Bailey, M.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370. [Google Scholar] [CrossRef]
- Rashid, Z.Z.; Othman, S.N.; Samat, M.N.A.; Ali, U.K.; Wong, K.K. Diagnostic performance of COVID-19 serology assays. Malays. J. Pathol 2020, 42, 13–21. [Google Scholar]
- Bastos, M.L.; Tavaziva, G.; Abidi, S.K.; Campbell, J.R.; Haraoui, L.P.; Johnston, J.C.; Lan, Z.; Law, S.; MacLean, E.; Trajman, A.; et al. Diagnostic accuracy of serological tests for covid-19: Systematic review and meta-analysis. BMJ 2020, m2516. [Google Scholar] [CrossRef]
- Ong, D.; de Man, S.; Lindeboom, F.; Koeleman, J. Comparison of diagnostic accuracies of rapid serological tests and ELISA to molecular diagnostics in patients with suspected coronavirus disease 2019 presenting to the hospital. Clin. Microbiol. Infect. 2020, 26, 1094.e7–1094.e10. [Google Scholar] [CrossRef]
- Kontou, P.; Braliou, G.; Dimou, N.; Nikolopoulos, G.; Bagos, P. Antibody tests in detecting SARS-CoV-2 infection: A meta-analysis. Diagnostics 2020, 10, 319. [Google Scholar] [CrossRef]
- La Marca, A.; Capuzzo, M.; Paglia, T.; Roli, L.; Trenti, T.; Nelson, S. Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reprod. Biomed. Online 2020. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Prado, E.; Simbaña-Rivera, K.; Gómez- Barreno, L.; Rubio-Neira, M.; Guaman, L.; Kyriakidis, N.; Muslina, C.; Jaramilloe, A.M.G.; Barba-Ostriaa, C.; Cevallos-Robalino, D.; et al. Clinical, molecular, and epidemiological characterization of the SARS-CoV-2 virus and the Coronavirus Disease 2019 (COVID-19), a comprehensive literature review. Diagn. Microbiol. Infect. Dis. 2020, 98, 115094. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.; Cheung, P. Presence of mismatches between diagnostic PCR assays and coronavirus SARS-CoV-2 genome. R. Soc. Open Sci. 2020, 7, 200636. [Google Scholar] [CrossRef] [PubMed]
- Artesi, M.; Bontems, S.; Göbbels, P.; Franckh, M.; Maes, P.; Boreux, R.; Meex, C.; Melin, P.; Hayette, M.; Bours, V.; et al. A recurrent mutation at position 26,340 of SARS-CoV-2 is associated with failure of the E-gene qRT-PCR utilized in a commercial dual-target diagnostic assay. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef]
- Kellam, P.; Barclay, W. The dynamics of humoral immune responses following SARS-CoV-2 infection and the potential for reinfection. J. Gen. Virol. 2020, 101, 791–797. [Google Scholar] [CrossRef]
- Liu, A.; Li, Y.; Peng, J.; Huang, Y.; Xu, D. Antibody responses against SARS-CoV-2 in COVID-19 patients. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Ni, L.; Ye, F.; Cheng, M.; Feng, Y.; Deng, Y.; Zhao, H.; Wei, P.; Ge, J.; Gou, M.; Li, X.; et al. Detection of SARS-CoV-2-specific humoral and cellular immunity in COVID-19 convalescent individuals. Immunity 2020, 52, 971–977.e3. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T cell immunity in convalescent individuals with asymptomatic or mild COVID-19. Cell 2020. [Google Scholar] [CrossRef]
- Le Bert, N.; Tan, A.; Kunasegaran, K.; Tham, C.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef]
- Long, Q.; Tang, X.; Shi, Q.; Li, Q.; Deng, H.; Yuan, J.; Hu, J.; Xu, W.; Zhang, Y.; Lv, F.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Zhang, Z.; Xiao, T.; Wang, Y.; Yuan, J.; Ye, H.; Wei, L.; Wang, H.; Liao, X.; Qian, S.; Wang, Z.; et al. Early viral clearance and antibody kinetics of COVID-19 among asymptomatic carriers. MedRxiv 2020. [Google Scholar] [CrossRef]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.L.; Liao, C.H.; Liu, P.Y.; Cheng, C.Y.; Chung, M.Y.; Liu, C.E.; Chang, S.Y.; Hsueh, P.R. Dynamics of anti-SARS-Cov-2 IgM and IgG antibodies among COVID-19 patients. J. Infect. 2020, 81, e55–e58. [Google Scholar] [CrossRef] [PubMed]
- Tuaillon, E.; Bolloré, K.; Pisoni, A.; Debiesse, S.; Renault, C.; Marie, S.; Grocc, S.; Nielsc, C.; Pansuc, N.; Dupuy, A.M.; et al. Detection of SARS-CoV-2 antibodies using commercial assays and seroconversion patterns in hospitalized patients. J. Infect. 2020, 81, e39–e45. [Google Scholar] [CrossRef] [PubMed]
- Margiotti, K.; Cupellaro, M.; Emili, S.; Mesoraca, A.; Giorlandino, C. Evaluation of A Rapid IgM-IgG Combined Antibody Test for SARS-CoV-2 Infection: Single Italian Center Study. Am. J. Infect. Dis. 2020, 16, 85–88. [Google Scholar] [CrossRef]
- Wu, J.; Tseng, W.; Lin, C.; Lee, T.; Chung, M.; Huang, C.; Chenac, S.; Hsuehbd, P.; Chen, S. Four point-of-care lateral flow immunoassays for diagnosis of COVID-19 and for assessing dynamics of antibody responses to SARS-CoV-2. J. Infect. 2020, 81, 435–442. [Google Scholar] [CrossRef]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, E63. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Mauk, M.G.; Hackett, B.A.; Cherry, S.; Bau, H.H.; Liu, C. Instrument-free point-of-care molecular detection of Zika virus. Anal. Chem. 2016, 88, 7289–7294. [Google Scholar] [CrossRef] [Green Version]
- Benzine, J.W.; Brown, K.M.; Agans, K.N.; Godiska, R.; Mire, C.E.; Gowda, K.; Converse, B.; Geisbert, T.W.; Mead, D.A.; Chander, Y. Molecular diagnostic field test for point-of-care detection of Ebola virus directly from blood. J. Infect. Dis. 2016, 214 (Suppl. 3), S234–S242. [Google Scholar] [CrossRef]
- Curtis, K.A.; Rudolph, D.L.; Morrison, D.; Guelig, D.; Diesburg, S.; McAdams, D.; Burton, R.A.; LaBarre, P.; Owen, M. Single-use, electricity-free amplification device for detection of HIV-1. J. Virol. Methods 2016, 237, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Ali, Z.; Aman, R.; Mahas, A.; Rao, G.S.; Tehseen, M.; Marsic, T.; Salunke, R.; Subudhi, A.K.; Hala, S.M.; Hamdan, S.M.; et al. iSCAN: An RT-LAMP-coupled CRISPR-Cas12 module for rapid, sensitive detection of SARS-CoV-2. Virus Res. 2020, 288, 198129. [Google Scholar] [CrossRef] [PubMed]
- Dao Thi, V.L.; Herbst, K.; Boerner, K.; Meurer, M.; Kremer, L.P.; Kirrmaier, D.; Freistaedter, A.; Papagiannidis, D.; Galmozzi, C.; Stanifer, M.L.; et al. A colorimetric RT-LAMP assay and LAMP-sequencing for detecting SARS-CoV-2 RNA in clinical samples. Sci. Transl. Med. 2020, 12, eabc7075. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.M.; Hackl, W.; Griesmacher, A. Point-of-Care-Testing--das Intensivlaboratorium [Point-of-care-testing--the intensive care laboratory. Anaesthesist 1999, 48, 3–8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Institution | Gene Targets | LoD | Reference |
|---|---|---|---|
| China CDC, China | ORF1ab and N | 100 RNA copies/µL | [17] |
| Institut Pasteur, Paris, France | RdRp IP2 and RdRp IP4 | 10 copies RNA genome | [18] |
| Charité (Germany) | RdRP, E and N | E: 3.9 copies RNA genome | [19] |
| RdRp: 3.6 copies RNA genome | |||
| US CDC, USA | N1 and N2 | 100 RNA copies/µL | [20] |
| HKU, Hong Kong SAR | ORF1b-nsp14 and N | Not specified | [21] |
| National Institute of Health, Thailand | N | Not specified | [22] |
| National Institute of Infectious Diseases, Japan | ORF1a and S | Not specified | [23] |
| Name | Manufacturer | Technology | Target | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|
| Architect SARS CoV-2 IgG | Abbott Laboratories Inc | CLIA | IgG | 100 2 | 99.6 2 |
| 2019-nCoV Specific Test (IgG and IgM antibody determination kit) | Beijing Diagret Biotechnologies Co., Ltd | LFA | IgG/IgM | 83 1 | 93 1 |
| COVID 19 IgG-IgM Cassette | Hangzhou Biotest Biotech Co. Ltd. | LFA | IgG | 90 2 | 100 2 |
| IgM | 100 2 | 98.8 2 | |||
| Certum 2019-nCov IgG/IgM Rapid Test | Hangzhou AllTest Biotech Co. Ltd. | LFA | IgG | 99.9 [49] | 98 [49] |
| IgM | 90.9 [49] | 97 [49] | |||
| Standard Q COVID-19 IgM/IgG Combo Test | SD Biosensor, Inc. | LFA | IgM | 53.3 2 | 100 2 |
| IgG | 73.3 2 | 98.8 2 | |||
| Panbio COVID-19 IgG/IgM Rapid Test Device | Abon Biopharm (Hangzhou) Co.,Ltd | LFA | IgG/IgM | 96.2 1 | 100 1 |
| Novel Coronavirus 2019 nCoV IgG/IgM Test Kit (colloidal gold) | Genrui Biotech Inc. | LFA | IgG/IgM | 90.74 1 | 94.64 1 |
| COVID-19 Antibody Test Kit (SARSCoV-2) ACC100-CRDT-COVID19-KIT | Accutest Research Laboratories México, S.A. de C.V. | LFA | IgG/IgM | 89.67 1 | 99.33 1 |
| EdinburghGenetics COVID-19 Colloidal Gold Immunoassay Testing Kit, IgG/IgM Combined | EdinburghGenetics Limited | LFA | IgG/IgM | 98.43 1 | 99.31 1 |
| Elecsys Anti-SARS-COV-2. Cobas® | Roche Diagnostics GmbH | CLIA | IgG | 99.5 1 | 99.44 1 |
| Anti-SARS-CoV-2 ELISA (IgA) | Euroimmun Medizinische Labordiagnostika AG | ELISA | IgA | 93.3 [50] | 80.0 [50] |
| COVID-19 IgG/IgM Test Cassette (Testsealabs®) | Hangzhou Testsea Biotechnology, Co., Ltd. | LFA | IgG | 40 2 | 93.8 2 |
| IgM | 73.3 2 | 98.8 2 | |||
| WHPM COVID-19 /IgM /IgG Rapid Test | W.H.P.M., Inc. | LFA | IgG /IgM | 76.7 2 | 97.1 2 |
| 2019-nCoV Ab IgM/IgG (Innovita) | Innovita (Tangshan) Biological Technology Co., Ltd | LFA | IgG/IgM | 87.3 1 | 100 1 |
| Innoscreen COVID 19 IgG/IgM Rapid test | Innovation Scientific Pty LTD | LFA | IgG/IgM | Not specified | Not specified |
| Liaison SARS-CoV-2 S1/S2 IgG | Diasorin, S.p.A | CLIA | IgG | 64 1 | 97.7 1 |
| MAGLUMI 2019-nCoV IgG (CLIA) | Shenzhen New Industries Biomedical Engineering Co., Ltd | CLIA | IgG | 95.6 1 | 96 1 |
| MAGLUMI 2019-nCoV IgM (CLIA) | Shenzhen New Industries Biomedical Engineering Co., Ltd | CLIA | IgM | 89.89 1 | 96.5 1 |
| COVID-19 lgG/lgM Rapid Test Cassette (Wb/S/P) | Hangzhou Clongene Biotech Co., Ltd. | LFA | IgG/IgM | Not specified | Not specified |
| Anti-SARS-CoV-2 ELISA (IgG) | Euroimmun Medizinische Labordiagnostika AG | ELISA | IgG | 90 1 | 100 1 |
| Anti-SARS-CoV-2 NCP ELISA (IgG) | Euroimmun Medizinische Labordiagnostika AG | ELISA | IgG | 94.6 1 | 99.8 1 |
| 2019-nCoV IgG/IgM Rapid Test Device | Hangzhou Realy Tech Co., Ltd. | LFA | IgG/IgM | 95.5 [51] | 96.8 [51] |
| Vitros Anti-SARS-CoV-2 IgG | Ortho-Clinical Diagnostics, Inc. | CLIA | IgG | 90 2 | 100 2 |
| Vitros Anti-SARS-CoV-2Total Antibodies (IgA, IgM e IgG) | Ortho-Clinical Diagnostics, Inc. | CLIA | IgA/IgG/IgM | 100 2 | 100 2 |
| NADAL COVID 19 lgG/lgM TEST KIT (Test cassette) | NAL VON MINDEN GmbH | LFA | IgG/IgM | 93.7 1 | 99.1 1 |
| careUS COVID-19 lgM/lgG | Wells Bio, Inc. | LFA | lgM/lgG | 93.6 1 | 98 1 |
| WANTAI SARS-CoV-2 Ab Rapid Test | Beijing Wantai Biological Pharmacy Enterprise Co. | LFA | lgM/lgG | 100 2 | 98.8 2 |
| VIDAS SARS-CoV-2 IgG (9COG) | Biomerieux, S.A. | ELFA | IgG | 96.6 1 | 99.9 1 |
| VIDAS SARS-CoV-2 IgM (9COM) | Biomerieux, S.A. | ELFA | IgM | 100 1 | 99.4 1 |
| Cellex qSARS-CoV-2 IgG/IgM Cassette Rapid Test | Cellex Biotech (Suzhou) Co, Ltd. | LFA | IgG/IgM | 20 [35] | 100 [35] |
| SureScreen COVID-19 IgG/IgM Rapid test | Surescreen Diagnostics, Ltd | LFA | IgG/IgM | 96.5 1 | 99.67 1 |
| Diagnostics Kit (Colloidal Gold) for IgG/IgM Antibody SARS-CoV-2 | Xiamen Wiz Biotech Co., Ltd. | LFA | IgG/IgM | Not specified | Not specified |
| Biocredit COVID-19IgG+IgM Duo Rapid Test | RapiGEN, Inc. | LFA | IgG | 94.2 1 | 98.7 1 |
| IgM | 100 1 | 98.7 1 | |||
| QikTech COVID-19 IgG/IgM Antibody Test | Lusys Laboratories, Inc. | LFA | IgG/IgM | Not specified | Not specified |
| Acon® SARS-CoV-2 IgG/IgM Rapid Test | Acon Biotech (Hangzhou) Co., Ltd. | LFA | IgG/IgM | 99.1 1 | 98.2 1 |
| NOVA test | AtlasLink (Beijing) Technology Co., Ltd. | LFA | IgG | 90 2 | 90 2 |
| IgM | 90 2 | 90 2 | |||
| COVID 19 IgG/IgM Antibody Rapid Test Kit | Changchun Wancheng Bio-Electron Co., Ltd. | LFA | IgG/IgM | Not specified | Not specified |
| 2019-nCoV IgG/IgM Detection Kit (Colloidal Gold-Based) | Nanjing Vazyme Medical Technology Co., Ltd. | LFA | IgG | 96.7 2 | 90 2 |
| IgM | 66.7 2 | 77.5 2 | |||
| SARS-CoV-2 Antibody Test (lateral Flow Method) Wondfo | Guangzhou Wondfo Biotech Co., Ltd. | LFA | Total Antibodies | 86.4 [52] | 99.6 [52] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Liu, C.; Martínez-Acuña, N.; Arellanos-Soto, D.; Galan-Huerta, K.; Lozano-Sepulveda, S.; Martínez-Guzmán, M.d.C.; Rivas-Estilla, A.M. SARS-CoV-2 in Mexico: Beyond Detection Methods, Scope and Limitations. Diagnostics 2021, 11, 124. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010124
Martinez-Liu C, Martínez-Acuña N, Arellanos-Soto D, Galan-Huerta K, Lozano-Sepulveda S, Martínez-Guzmán MdC, Rivas-Estilla AM. SARS-CoV-2 in Mexico: Beyond Detection Methods, Scope and Limitations. Diagnostics. 2021; 11(1):124. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010124
Chicago/Turabian StyleMartinez-Liu, Cynthia, Natalia Martínez-Acuña, Daniel Arellanos-Soto, Kame Galan-Huerta, Sonia Lozano-Sepulveda, María del Carmen Martínez-Guzmán, and Ana Maria Rivas-Estilla. 2021. "SARS-CoV-2 in Mexico: Beyond Detection Methods, Scope and Limitations" Diagnostics 11, no. 1: 124. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010124