Prediction of Nonalcoholic Fatty Liver Disease Using Noninvasive and Non-Imaging Procedures in Japanese Health Checkup Examinees

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Physical Examination and Laboratory Tests
2.3. Abdominal Ultrasound Protocol and Definition of Fatty Liver
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Subjects
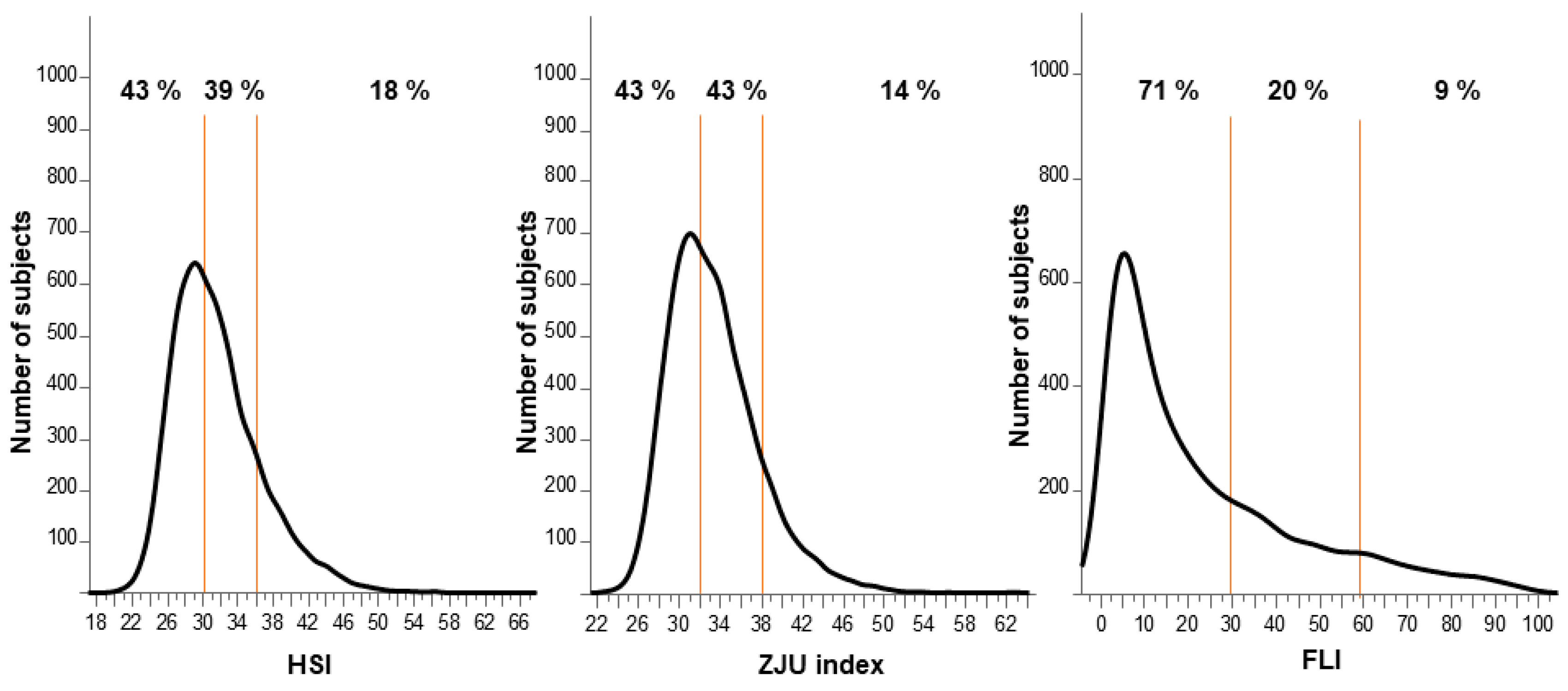
3.2. Frequency Distribution of Individual Indexes
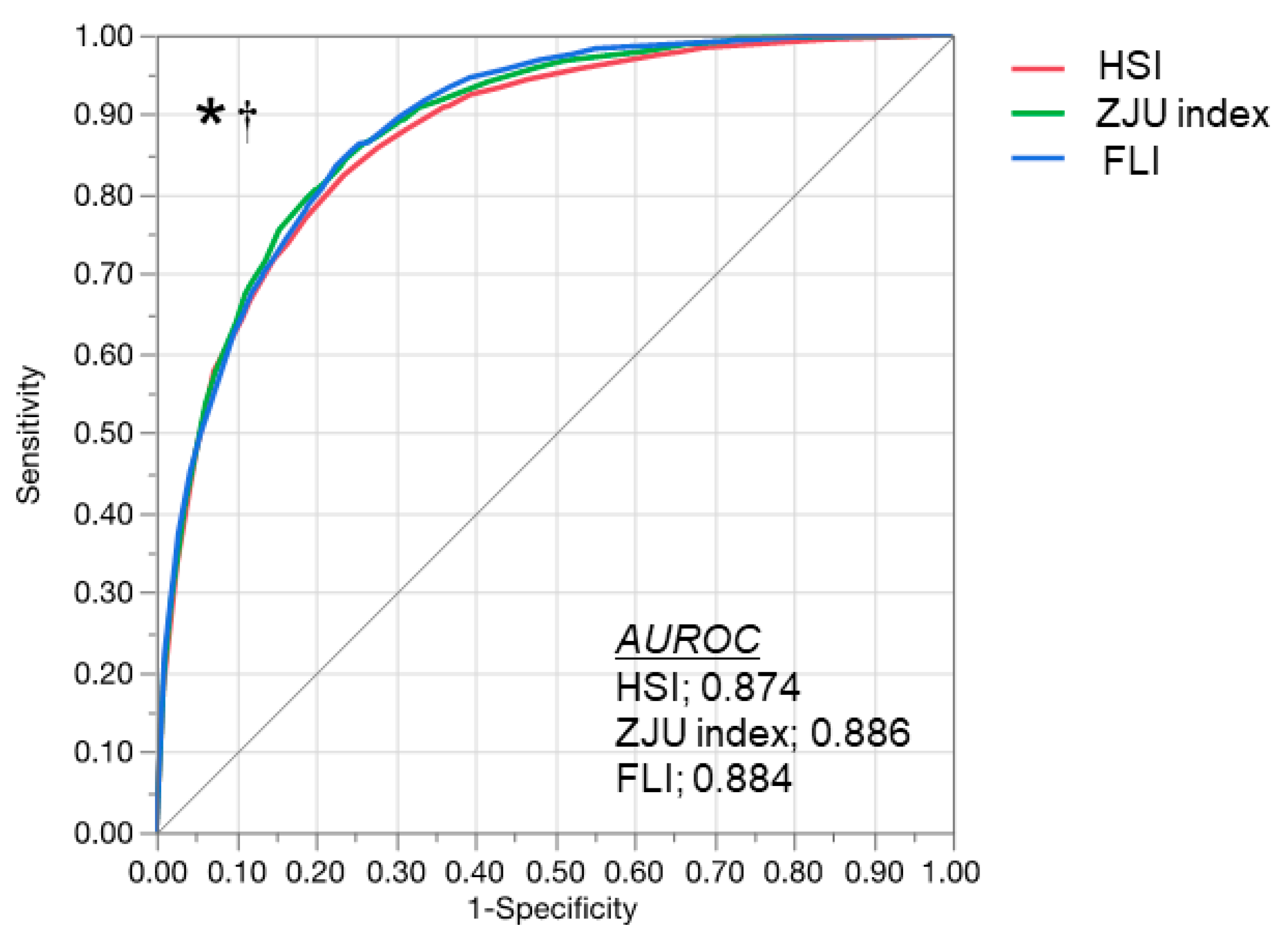
3.3. Comparison of HSI, ZJU Index, and FLI
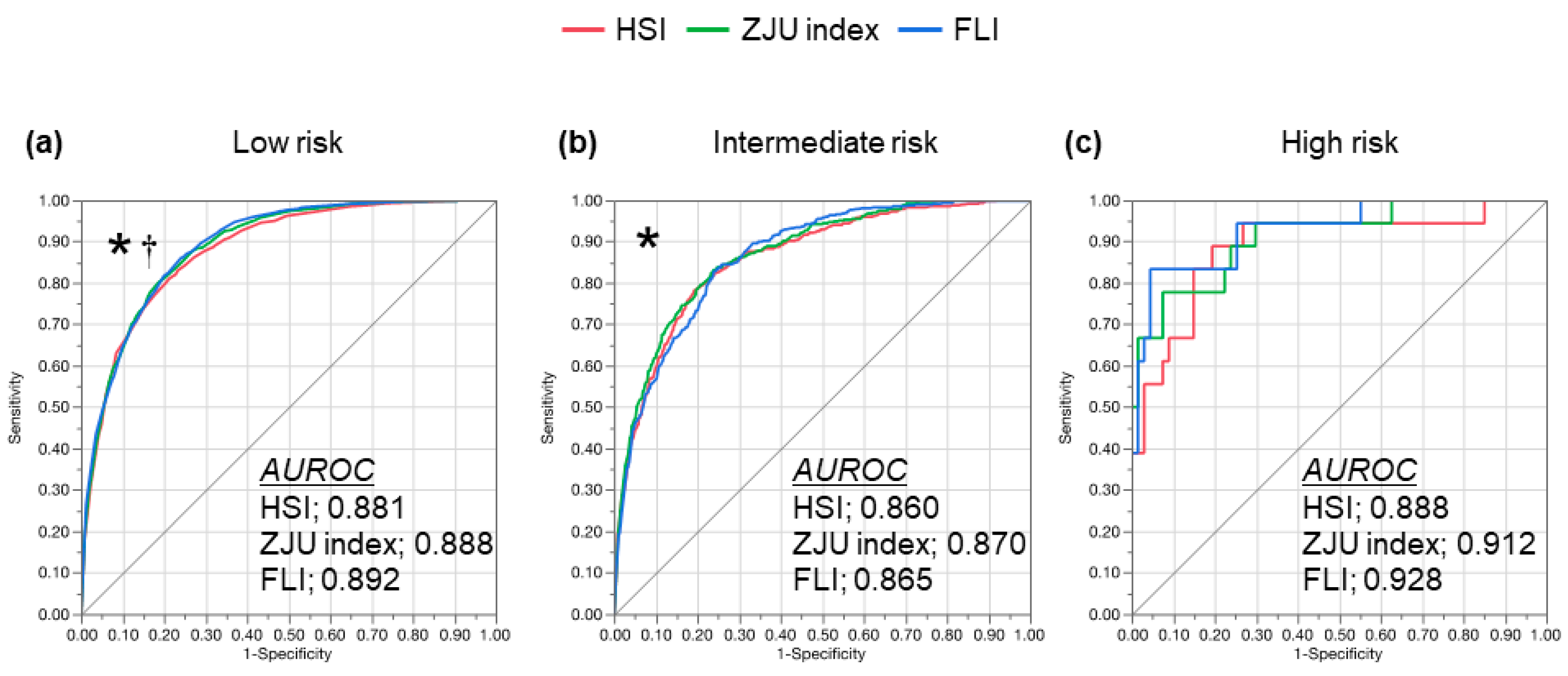
3.4. Diagnostic Performance in Patients with Potential Advanced Liver Fibrosis
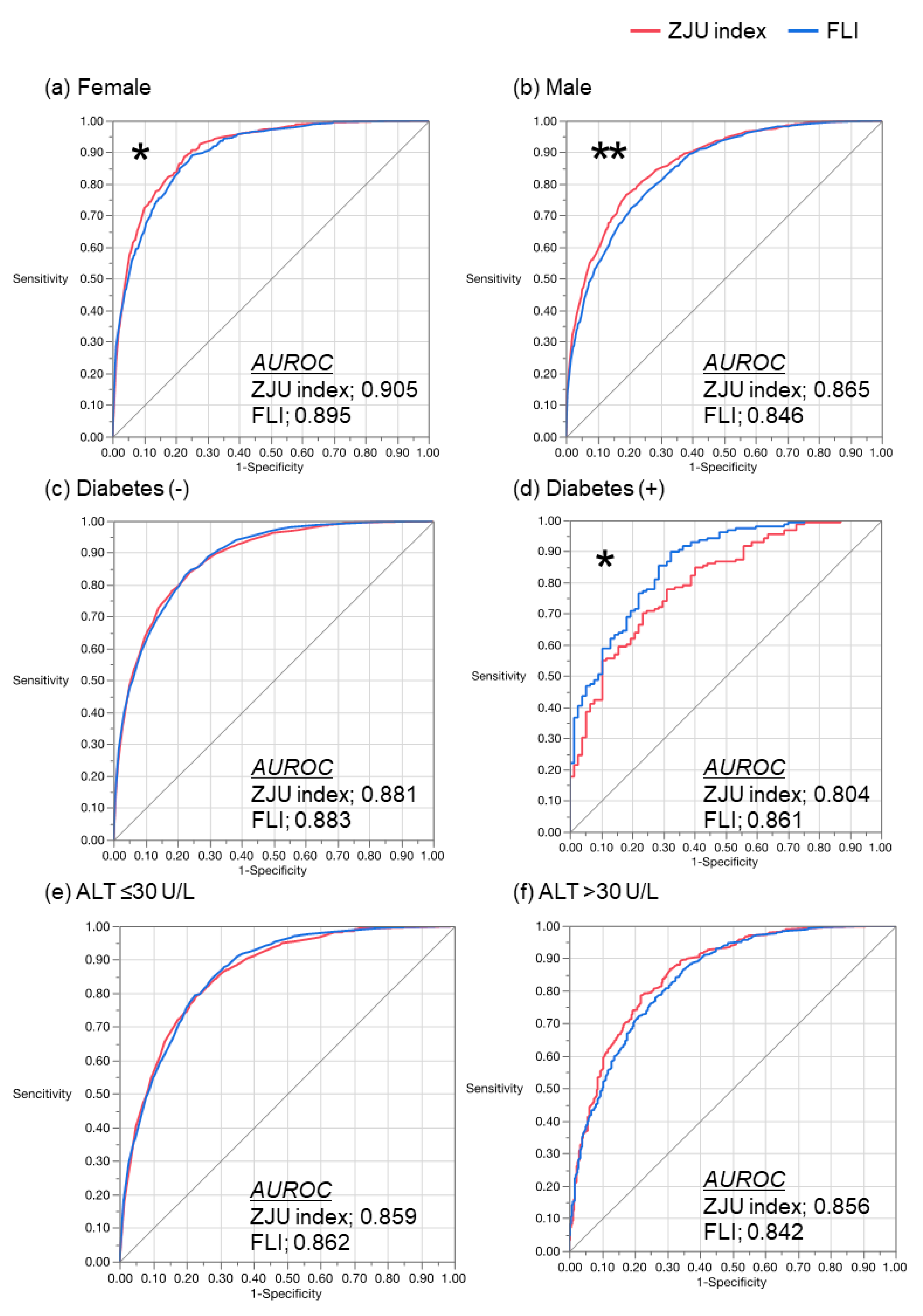
3.5. Comparison of the ZJU Index and the FLI
3.6. Characteristics of the Subjects with NAFLD Subjects Having a Negative ZJU Index and FLI
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults: Systematic review: Epidemiology of NAFLD and NASH. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Takeda, N.; Nakagawa, T.; Taniguchi, H.; Fujii, K.; Omatsu, T.; Nakajima, T.; Sarui, H.; Shimazaki, M.; et al. The Metabolic Syndrome as a Predictor of Nonalcoholic Fatty Liver Disease. Ann. Intern. Med. 2005, 143, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.-G.; Farrell, G.C. Epidemiology of non-alcoholic fatty liver disease in China. J. Hepatol. 2009, 50, 204–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, A. Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar]
- Neuschwander-Tetri, B. Nonalcoholic steatohepatitis: Summary of an AASLD Single Topic Conference. Hepatology 2003, 37, 1202–1219. [Google Scholar] [CrossRef]
- Gholam, P.M.; Flancbaum, L.; Machan, J.T.; Charney, D.A.; Kotler, D.P. Nonalcoholic Fatty Liver Disease in Severely Obese Subjects. Am. J. Gastroenterol. 2007, 102, 399–408. [Google Scholar] [CrossRef]
- Adams, L.A.; Lymp, J.F.; St Sauver, J.; Sanderson, S.O.; Lindor, K.D.; Feldstein, A.; Angulo, P. The Natural History of Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study. Gastroenterology 2005, 129, 113–121. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Ong, J.P.; Pitts, A.; Younossi, Z.M. Increased overall mortality and liver-related mortality in non-alcoholic fatty liver disease. J. Hepatol. 2008, 49, 608–612. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Poli, F.; Rodella, S.; Scala, L.; Tessari, R.; Zenari, L.; Falezza, G. Nonalcoholic Fatty Liver Disease and Risk of Future Cardiovascular Events Among Type 2 Diabetic Patients. Diabetes 2005, 54, 3541–3546. [Google Scholar] [CrossRef] [Green Version]
- Hamaguchi, M. Nonalcoholic fatty liver disease is a novel predictor of cardiovascular disease. WJG 2007, 13, 1579. [Google Scholar] [CrossRef] [Green Version]
- Musso, G.; Gambino, R.; Cassader, M.; Pagano, G. Meta-analysis: Natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann. Med. 2011, 43, 617–649. [Google Scholar] [CrossRef] [PubMed]
- Ekstedt, M.; Franzén, L.E.; Mathiesen, U.L.; Thorelius, L.; Holmqvist, M.; Bodemar, G.; Kechagias, S. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006, 44, 865–873. [Google Scholar] [CrossRef]
- Chang, Y.; Ryu, S.; Sung, E.; Woo, H.-Y.; Oh, E.; Cha, K.; Jung, E.; Kim, W.S. Nonalcoholic fatty liver disease predicts chronic kidney disease in nonhypertensive and nondiabetic Korean men. Metabolism 2008, 57, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Chonchol, M.; Bertolini, L.; Rodella, S.; Zenari, L.; Lippi, G.; Franchini, M.; Zoppini, G.; Muggeo, M. Increased Risk of CKD among Type 2 Diabetics with Nonalcoholic Fatty Liver Disease. JASN 2008, 19, 1564–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, S.T.; Cho, Y.K.; Yun, J.W.; Park, J.H.; Kim, H.J.; Park, D.I.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Rhee, E.J.; et al. Impact of non-alcoholic fatty liver disease on microalbuminuria in patients with prediabetes and diabetes: Impact of NAFLD on microalbuminuria. Intern. Med. J. 2010, 40, 437–442. [Google Scholar] [CrossRef]
- JSG-NAFLD; Eguchi, Y.; Hyogo, H.; Ono, M.; Mizuta, T.; Ono, N.; Fujimoto, K.; Chayama, K.; Saibara, T. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: A multicenter large retrospective study. J. Gastroenterol. 2012, 47, 586–595. [Google Scholar]
- Fix, O.K.; Hameed, B.; Fontana, R.J.; Kwok, R.M.; McGuire, B.M.; Mulligan, D.C.; Pratt, D.S.; Russo, M.W.; Schilsky, M.L.; Verna, E.C.; et al. Clinical Best Practice Advice for Hepatology and Liver Transplant Providers During the COVID-19 Pandemic: AASLD Expert Panel Consensus Statement. Hepatology 2020, 72, 287–304. [Google Scholar] [CrossRef]
- Mehta, N.; Parikh, N.; Kelley, R.K.; Hameed, B.; Singal, A.G. Surveillance and Monitoring of Hepatocellular Carcinoma During the COVID-19 Pandemic. Clin. Gastroenterol. Hepatol. 2020, S1542356520309381. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Implication of non-alcoholic fatty liver diseases (NAFLD) in patients with COVID-19: A preliminary analysis. J. Hepatol. 2020, S0168827820302063. [Google Scholar] [CrossRef]
- Wang, J.; Xu, C.; Xun, Y.; Lu, Z.; Shi, J.; Yu, C.; Li, Y. ZJU index: A novel model for predicting nonalcoholic fatty liver disease in a Chinese population. Sci. Rep. 2015, 5, 16494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef]
- Tanaka, K.; Hyogo, H.; Ono, M.; Takahashi, H.; Kitajima, Y.; Ono, N.; Eguchi, T.; Fujimoto, K.; Chayama, K.; Saibara, T.; et al. Upper limit of normal serum alanine aminotransferase levels in Japanese subjects: Normal serum ALT levels in Japan. Hepatol. Res. 2014, 44, 1196–1207. [Google Scholar] [CrossRef]
- Takahashi, H.; Ono, M.; Hyogo, H.; Tsuji, C.; Kitajima, Y.; Ono, N.; Eguchi, T.; Fujimoto, K.; Chayama, K.; Saibara, T.; et al. Biphasic effect of alcohol intake on the development of fatty liver disease. J. Gastroenterol. 2015, 50, 1114–1123. [Google Scholar] [CrossRef]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan. New Criteria for ‘Obesity Disease’ in Japan. Circ. J. 2002, 66, 987. [Google Scholar] [CrossRef] [Green Version]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Japan Study Group of Nonalcoholic Fatty Liver Disease (JSG-NAFLD); Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012, 12, 2. [Google Scholar]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Comparison of Noninvasive Markers of Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Itoh, Y.; Harano, Y.; Fujii, K.; Nakajima, T.; Kato, T.; Takeda, N.; Okuda, J.; Ida, K.; et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am. J. Gastroenterol. 2007, 102, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- EASL; EASD; EASO. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease: Is universal screening appropriate? Diabetologia 2016, 59, 1141–1144. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.-L.; Wu, W.-C.; Fang, K.-C.; Wang, Y.-C.; Huo, T.-I.; Huang, Y.-H.; Huo, T.-L.; Huang, Y.-H.; Yang, H.-I.; Su, C.-W.; et al. External Validation of Fatty Liver Index for Identifying Ultrasonographic Fatty Liver in a Large-Scale Cross-Sectional Study in Taiwan. PLoS ONE 2015, 10, e0120443. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.-W.; Huang, P.-R.; Chien, C.-H.; Lin, C.-L.; Chien, R.-N. A community-based study on the application of fatty liver index in screening subjects with nonalcoholic fatty liver disease. J. Formos. Med. Assoc. 2019, 119, 173–181. [Google Scholar] [CrossRef]
- Rinella, M.E.; Tacke, F.; Sanyal, A.J.; Anstee, Q.M. Report on the AASLD/EASL joint workshop on clinical trial endpoints in NAFLD. J. Hepatol. 2019, 71, 823–833. [Google Scholar] [CrossRef] [Green Version]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of Implementing a “FIB-4 First” Strategy on a Pathway for Patients With NAFLD Referred From Primary Care. Hepatol. Commun. 2019, 3, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imajo, K.; Kessoku, T.; Honda, Y.; Tomeno, W.; Ogawa, Y.; Mawatari, H.; Fujita, K.; Yoneda, M.; Taguri, M.; Hyogo, H.; et al. Magnetic Resonance Imaging More Accurately Classifies Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease Than Transient Elastography. Gastroenterology 2016, 150, 626–637.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oeda, S.; Takahashi, H.; Imajo, K.; Seko, Y.; Ogawa, Y.; Moriguchi, M.; Yoneda, M.; Anzai, K.; Aishima, S.; Kage, M.; et al. Accuracy of liver stiffness measurement and controlled attenuation parameter using FibroScan®M/XL probes to diagnose liver fibrosis and steatosis in patients with nonalcoholic fatty liver disease: A multicenter prospective study. J. Gastroenterol. 2019, 55, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, N.; Koizumi, Y.; Hirooka, M.; Yada, N.; Takada, H.; Nakashima, O.; Kudo, M.; Hiasa, Y.; Izumi, A.N. Novel quantitative assessment system of liver steatosis using a newly developed attenuation measurement method. Hepatol. Res. 2018, 48, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Tada, T.; Iijima, H.; Kobayashi, N.; Yoshida, M.; Nishimura, T.; Kumada, T.; Kondo, R.; Yano, H.; Kage, M.; Nakano, C.; et al. Usefulness of Attenuation Imaging with an Ultrasound Scanner for the Evaluation of Hepatic Steatosis. Ultrasound Med. Biol. 2019, 45, 2679–2687. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 6927) | |
|---|---|
| Age, years | 50.0 (42.0–56.5) |
| Male, n (%) | 3316 (47.8) |
| BMI, kg/m2 | 22.3 (20.2–24.4) |
| Waist circumference, cm | 81.4 (75.0–87.0) |
| Platelet counts, ×104/μL) | 21.3 (18.4–24.5) |
| AST, U/L | 19.0 (16.0–23.0) |
| ALT, U/L | 18.0 (13.0–25.0) |
| ALP, U/L | 202 (167–247) |
| GGT, U/L | 23.0 (16.0–36.0) |
| FPG, mg/dL | 96.0 (91.0–104) |
| TC, mg/dL | 204 (182–228) |
| TG, mg/dL | 88.0 (63.0–129) |
| HDL-C, mg/dL | 60.0 (50.0–73.0) |
| LDL-C, mg/dL | 120 (100–140) |
| HbA1c, % | 5.55 (5.35–5.86) |
| Fatty liver, n (%) | 1935 (28.0) |
| Index | Cut-Off Point | Sensitivity (%) | Specificity (%) | Sensitivity + Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| HSI | >36 | 49.4 | 94.4 | 143.8 | 77.6 | 82.8 |
| <30 | 93.4 | 56.8 | 150.2 | 45.6 | 95.7 | |
| ZJU index | >38 | 40.6 | 96.4 | 137.0 | 81.7 | 80.6 |
| <32 | 94.2 | 57.5 | 151.7 | 46.5 | 96.2 | |
| FLI | >60 | 28.2 | 98.4 | 126.6 | 87.5 | 77.8 |
| <30 | 68.8 | 87.0 | 155.8 | 67.6 | 87.7 |
| Advanced Fibrosis | Index | Cut-Off Point | Sensitivity (%) | Specificity (%) | Sensitivity + Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|
| Low risk | HSI | >36 | 54.4 | 93.4 | 147.8 | 77.8 | 83.0 |
| <30 | 95.3 | 52.8 | 148.1 | 45.9 | 96.4 | ||
| ZJU index | >38 | 42.6 | 95.9 | 138.5 | 81.8 | 79.7 | |
| <32 | 95.8 | 56.1 | 151.9 | 48.3 | 96.9 | ||
| FLI | >60 | 29.5 | 98.4 | 127.9 | 89.1 | 76.6 | |
| <30 | 70.4 | 86.8 | 157.2 | 69.6 | 87.3 | ||
| Intermediate risk | HSI | >36 | 34.9 | 96.7 | 131.6 | 78.1 | 81.7 |
| <30 | 93.4 | 56.8 | 150.2 | 45.6 | 95.7 | ||
| ZJU index | >38 | 34.7 | 97.4 | 132.1 | 81.8 | 81.7 | |
| <32 | 89.1 | 60.7 | 149.8 | 43.0 | 94.4 | ||
| FLI | >60 | 24.3 | 98.2 | 122.5 | 82.0 | 79.6 | |
| <30 | 63.9 | 86.8 | 150.7 | 61.7 | 87.9 | ||
| High risk | HSI | >36 | 38.8 | 98.5 | 137.3 | 87.5 | 85.7 |
| <30 | 88.8 | 77.6 | 166.4 | 51.6 | 96.3 | ||
| ZJU index | >38 | 44.4 | 100 | 144.4 | 100 | 87.0 | |
| <32 | 94.4 | 61.1 | 155.5 | 39.5 | 97.6 | ||
| FLI | >60 | 38.8 | 100 | 138.8 | 100 | 85.9 | |
| <30 | 83.3 | 94.0 | 177.3 | 78.9 | 95.5 |
| NAFLD+ n = 107 | NAFLD– n = 2815 | p-Value | |
|---|---|---|---|
| Age, years | 51 (43–59) | 47 (40–55) | <0.001 |
| Male, n (%) | 80 (74.7) | 959 (34.0) | <0.001 |
| BMI, kg/m2 | 21.3 (20.5–22.1) | 19.9 (18.8–20.9) | <0.001 |
| Waist circumference, cm | 80.8 (78–84) | 74.2 (70.2–78.4) | <0.001 |
| Systolic blood pressure, mmHg | 111 (102–121) | 105 (96–115) | <0.001 |
| Diastolic blood pressure, mmHg | 65 (61–73) | 63 (57–71) | 0.021 |
| AST, U/L | 20 (17–23) | 18 (16–22) | 0.013 |
| ALT, U/L | 17 (13–21) | 14 (11–18) | <0.001 |
| ALP, U/L | 194 (157–248.5) | 189.5 (155–232) | 0.224 |
| GGT, U/L | 22 (17–30) | 17 (13–25) | <0.001 |
| FPG, mg/dL | 95 (90–100) | 93 (88–98) | <0.001 |
| TC, mg/dL | 197 (181–217) | 200 (179–224) | 0.361 |
| TG, mg/dL | 92 (66–115) | 67 (52–89) | <0.001 |
| HDL-C, mg/dL | 57 (50–64) | 69 (59–79) | <0.001 |
| LDL-C, mg/dL | 123 (105–136) | 112 (93–131) | 0.003 |
| HbA1c, % | 5.55 (5.35–5.75) | 5.45 (5.35–5.65) | 0.390 |
| Odds Ratio | 95% CI | p-Value | |
|---|---|---|---|
| Gender (male) | 3.97 | 2.46–6.40 | <0.001 |
| BMI (>22 kg/m2) | 2.16 | 1.31–3.57 | 0.002 |
| Waist circumference (>85 cm in males and >90 cm in females) | 4.10 | 2.13–7.86 | <0.001 |
| Systolic blood pressure (≥130 mmHg) | 1.22 | 0.56–2.64 | 0.612 |
| Diastolic blood pressure (≥80 mmHg) | 0.74 | 0.33–1.62 | 0.454 |
| ALT (>30 U/L) | 1.29 | 0.50–3.34 | 0.594 |
| FPG (≥110 mg/dL) | 1.36 | 0.56–3.25 | 0.488 |
| TG (≥150 mg/dL) | 1.62 | 0.66–3.93 | 0.285 |
| HDL-C (<40 mg/dL) | 1.54 | 0.43–5.50 | 0.501 |
| LDL-C (≥140 mg/dL) | 1.12 | 0.67–1.84 | 0.655 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murayama, K.; Okada, M.; Tanaka, K.; Inadomi, C.; Yoshioka, W.; Kubotsu, Y.; Yada, T.; Isoda, H.; Kuwashiro, T.; Oeda, S.; et al. Prediction of Nonalcoholic Fatty Liver Disease Using Noninvasive and Non-Imaging Procedures in Japanese Health Checkup Examinees. Diagnostics 2021, 11, 132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010132
Murayama K, Okada M, Tanaka K, Inadomi C, Yoshioka W, Kubotsu Y, Yada T, Isoda H, Kuwashiro T, Oeda S, et al. Prediction of Nonalcoholic Fatty Liver Disease Using Noninvasive and Non-Imaging Procedures in Japanese Health Checkup Examinees. Diagnostics. 2021; 11(1):132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010132
Chicago/Turabian StyleMurayama, Kenichiro, Michiaki Okada, Kenichi Tanaka, Chika Inadomi, Wataru Yoshioka, Yoshihito Kubotsu, Tomomi Yada, Hiroshi Isoda, Takuya Kuwashiro, Satoshi Oeda, and et al. 2021. "Prediction of Nonalcoholic Fatty Liver Disease Using Noninvasive and Non-Imaging Procedures in Japanese Health Checkup Examinees" Diagnostics 11, no. 1: 132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010132