White Matter Microstructural Differences between Hallucinating and Non-Hallucinating Schizophrenia Spectrum Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Image Acquisition
2.3. Image Processing
2.4. Statistical Analysis
3. Results
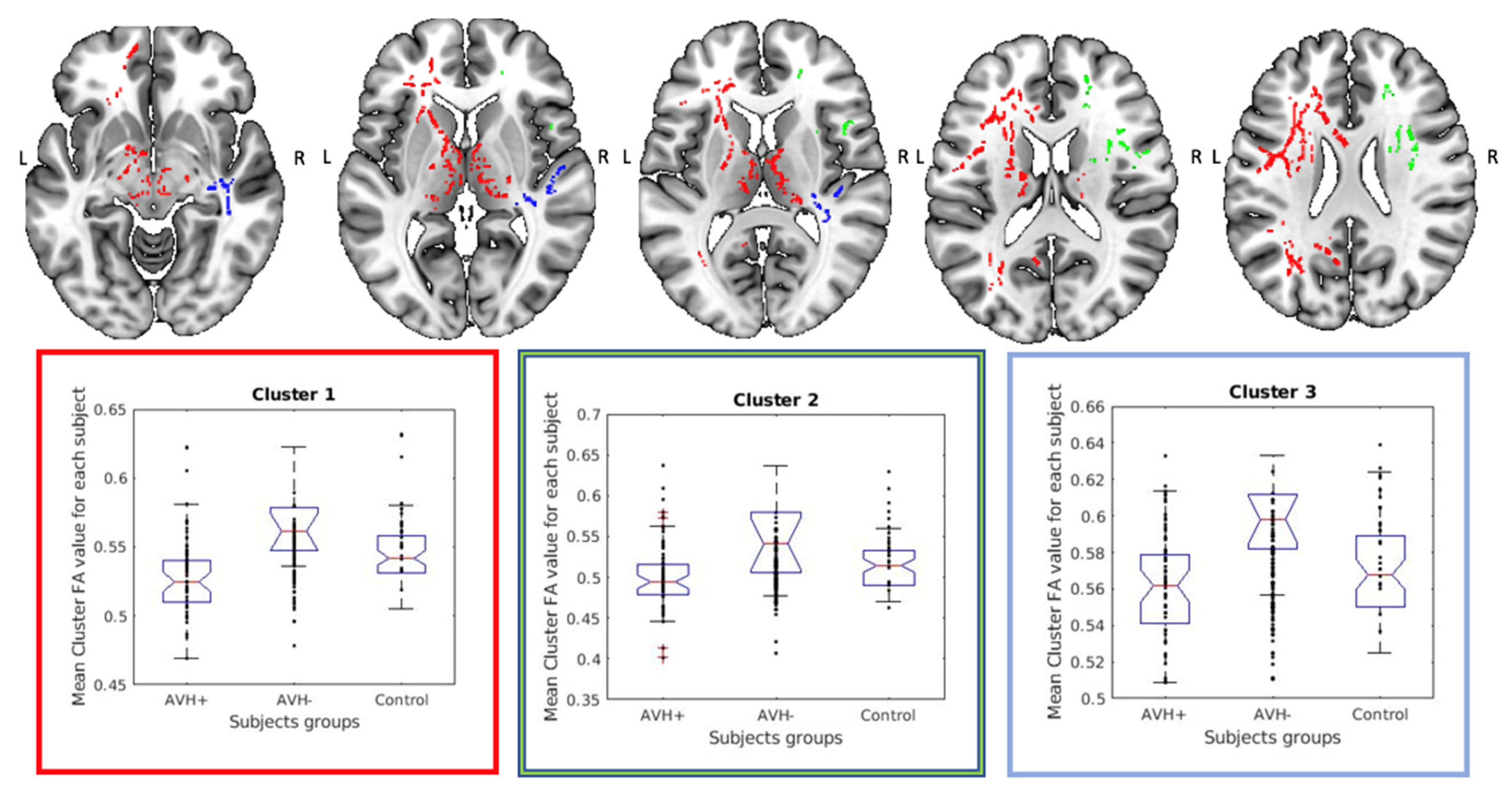
3.1. Group Comparison of the Original FA-Skeletons
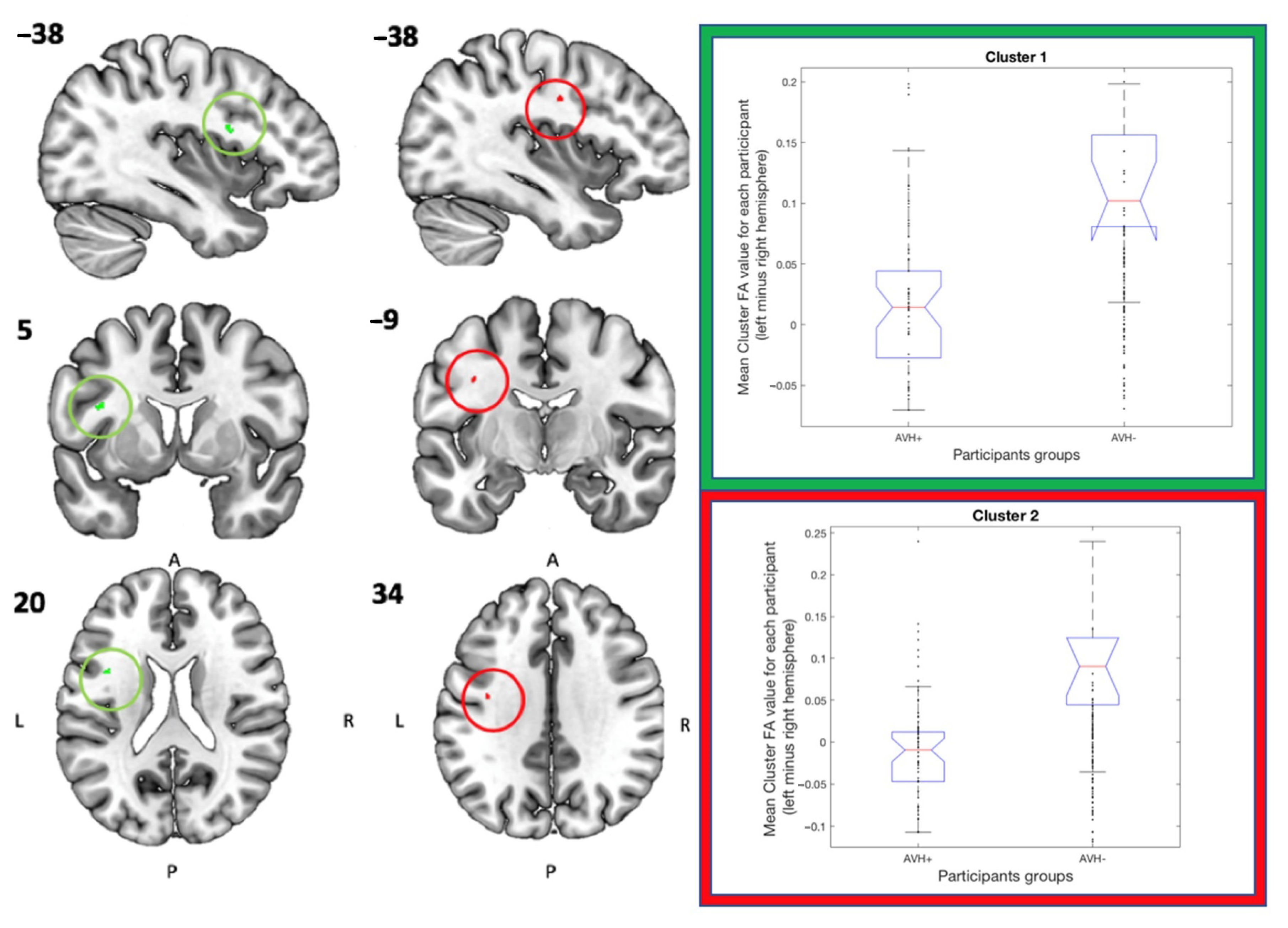
3.2. Hemispheric Asymmetry Comparisons
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 4D | Four Dimensional |
| ANOVA | Analysis of Variance |
| AVH | Auditory Verbal Hallucinations |
| BET | Brain Extraction Tool |
| DDD | Defined Daily Dose |
| DMN | Default Mode Network |
| DTI | Diffusion Tensor Imaging |
| ERC | European Research Council |
| FA | Fractional Anisotropy |
| FMRIB | Functional Magnetic Resonance Imaging of the Brain |
| FSL | FMRIB Software Library |
| FWE | Familywise Error |
| GE | General Electrics |
| HD | High-definition |
| ICD | International Classification of Diseases |
| P3 | Positive three |
| PANSS | Positive and Negative Syndrome Scale |
| SD | Standard Deviation |
| TBSS | Tract Based Special Statistics |
| TE | Echo Time |
| TFCE | Threshold Free Cluster Enhancement |
| TR | Repetition Time |
References
- Chaudhury, S. Hallucinations: Clinical aspects and management. Ind. Psychiatry J. 2010, 19, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M.; Mangalore, R.; Simon, J. The Global Costs of Schizophrenia. Schizophr. Bull. 2004, 30, 279–293. [Google Scholar] [CrossRef]
- Toh, W.L.; Thomas, N.; Hollander, Y.; Rossell, S.L. On the phenomenology of auditory verbal hallucinations in affective and non-affective psychosis. Psychiatry Res. 2020, 290, 113147. [Google Scholar] [CrossRef] [PubMed]
- Larøi, F.; Thomas, N.; Aleman, A.; Fernyhough, C.; Wilkinson, S.; Deamer, F.; McCarthy-Jones, S. The ice in voices: Understanding negative content in auditory-verbal hallucinations. Clin. Psychol. Rev. 2019, 67, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.M.; Schanda, H.; Karakula, H.; Olajossy-Hilkesberger, L.; Rudaleviciene, P.; Okribelashvili, N.; Chaudhry, H.R.; Idemudia, S.E.; Gscheider, S.; Ritter, K.; et al. Culture and the prevalence of hallucinations in schizophrenia. Compr. Psychiatry 2011, 52, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Ćurčić-Blake, B.; Ford, J.M.; Hubl, D.; Orlov, N.D.; Sommer, I.E.; Waters, F.; Allen, P.; Jardri, R.; Woodruff, P.W.; David, O.; et al. Interaction of language, auditory and memory brain networks in auditory verbal hallucinations. Prog. Neurobiol. 2017, 148, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Hugdahl, K.; Løberg, E.-M.; Nygård, M. Left temporal lobe structural and functional abnormality underlying auditory hallucinations. Front. Neurosci. 2009, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Weber, S.; Johnsen, E.; Kroken, R.A.; Løberg, E.-M.; Kandilarova, S.; Stoyanov, D.; Kompus, K.; Hugdahl, K. Dynamic Functional Connectivity Patterns in Schizophrenia and the Relationship with Hallucinations. Front. Psychiatry 2020, 11, 227. [Google Scholar] [CrossRef]
- Garrity, A.; Pearlson, G.D.; McKiernan, K.; Lloyd, D.; Kiehl, K.; Calhoun, V. Aberrant “Default Mode” Functional Connectivity in Schizophrenia. Am. J. Psychiatry 2007, 164, 450. [Google Scholar] [CrossRef]
- Sambataro, F.; Blasi, G.; Fazio, L.; Caforio, G.; Taurisano, P.; Romano, R.; Di Giorgio, A.; Gelao, B.; Bianco, L.L.; Papazacharias, A.; et al. Treatment with Olanzapine is Associated with Modulation of the Default Mode Network in Patients with Schizophrenia. Neuropsychopharmacology 2009, 35, 904–912. [Google Scholar] [CrossRef] [Green Version]
- De Weijer, A.D.; Mandl, R.; Diederen, K.; Neggers, S.; Kahn, R.S.; Pol, H.H.; Sommer, I. Microstructural alterations of the arcuate fasciculus in schizophrenia patients with frequent auditory verbal hallucinations. Schizophr. Res. 2011, 130, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellison-Wright, I.; Bullmore, E. Meta-analysis of diffusion tensor imaging studies in schizophrenia. Schizophr. Res. 2009, 108, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Jahanshad, N.; Zalesky, A.; Kochunov, P.; Agartz, I.; Alloza, C.; Andreassen, O.A.; Arango, C.; Banaj, N.; Bouix, S.; et al. Widespread white matter microstructural differences in schizophrenia across 4322 individuals: Results from the ENIGMA Schizophrenia DTI Working Group. Mol. Psychiatry 2018, 23, 1261–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubicki, M.; McCarley, R.; Westin, C.-F.; Park, H.-J.; Maier, S.; Kikinis, R.; Jolesz, F.A.; Shenton, M.E. A review of diffusion tensor imaging studies in schizophrenia. J. Psychiatr. Res. 2007, 41, 15–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leroux, E.; Delcroix, N.; Dollfus, S. Abnormalities of language pathways in schizophrenia patients with and without a lifetime history of auditory verbal hallucinations: A DTI-based tractography study. World J. Biol. Psychiatry 2017, 18, 528–538. [Google Scholar] [CrossRef]
- Oestreich, L.K.; Australian Schizophrenia Research Bank; McCarthy-Jones, S.; Whitford, T.J. Decreased integrity of the fronto-temporal fibers of the left inferior occipito-frontal fasciculus associated with auditory verbal hallucinations in schizophrenia. Brain Imaging Behav. 2016, 10, 445–454. [Google Scholar] [CrossRef]
- Seok, J.-H.; Park, H.-J.; Chun, J.-W.; Lee, S.-K.; Cho, H.S.; Kwon, J.S.; Kim, J.-J. White matter abnormalities associated with auditory hallucinations in schizophrenia: A combined study of voxel-based analyses of diffusion tensor imaging and structural magnetic resonance imaging. Psychiatry Res. Neuroimaging 2007, 156, 93–104. [Google Scholar] [CrossRef]
- Ćurčić-Blake, B.; Nanetti, L.; Van Der Meer, L.; Cerliani, L.; Renken, R.; Pijnenborg, G.H.M.; Aleman, A. Not on speaking terms: Hallucinations and structural network disconnectivity in schizophrenia. Brain Struct. Funct. 2013, 220, 407–418. [Google Scholar] [CrossRef]
- Shergill, S.S. A diffusion tensor imaging study of fasciculi in schizophrenia. Am. J. Psychiatry 2007, 164, 467–473. [Google Scholar] [CrossRef]
- Kühn, S.; Gallinat, J. Quantitative Meta-Analysis on State and Trait Aspects of Auditory Verbal Hallucinations in Schizophrenia. Schizophr. Bull. 2010, 38, 779–786. [Google Scholar] [CrossRef] [Green Version]
- Hugdahl, K.; Sommer, I.E. Auditory Verbal Hallucinations in Schizophrenia from a Levels of Explanation Perspective. Schizophr. Bull. 2018, 44, 234–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psomiades, M.; Fonteneau, C.; Mondino, M.; Luck, D.; Haesebaert, F.; Suaud-Chagny, M.-F.; Brunelin, J. Integrity of the arcuate fasciculus in patients with schizophrenia with auditory verbal hallucinations: A DTI-tractography study. NeuroImage Clin. 2016, 12, 970–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Case, M.; Stauffer, V.L.; Ascher-Svanum, H.; Conley, R.; Kapur, S.; Kane, J.M.; Kollack-Walker, S.; Jacob, J.; Kinon, B.J. The heterogeneity of antipsychotic response in the treatment of schizophrenia. Psychol. Med. 2010, 41, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.Z.; Rabinowitz, J.; Faries, D.; Lawson, A.H.; Ascher-Svanum, H. Treatment response trajectories and antipsychotic medications: Examination of up to 18months of treatment in the CATIE chronic schizophrenia trial. Schizophr. Res. 2012, 137, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Hirnstein, M.; Hugdahl, K. Excess of non-right-handedness in schizophrenia: Meta-analysis of gender effects and potential biases in handedness assessment. Br. J. Psychiatry 2014, 205, 260–267. [Google Scholar] [CrossRef]
- Bilder, R.M.; Wu, H.; Bogerts, B.; Degreef, G.; Ashtari, M.; Alvir, J.M.; Snyder, P.J.; Lieberman, J.A. Absence of regional hemispheric volume asymmetries in first-episode schizophrenia. Am. J. Psychiatry 1994, 151, 1437–1447. [Google Scholar] [CrossRef] [Green Version]
- Falkai, P. Loss of sylvian fissure asymmetry in schizophrenia: A quantitative post mortem study. Schizophr. Res. 1992, 7, 23–32. [Google Scholar] [CrossRef]
- Takao, H.; Abe, O.; Yamasue, H.; Aoki, S.; Kasai, K.; Ohtomo, K. Cerebral asymmetry in patients with schizophrenia: A voxel-based morphometry (VBM) and diffusion tensor imaging (DTI) study. J. Magn. Reson. Imaging 2009, 31, 221–226. [Google Scholar] [CrossRef]
- Dollfus, S.; Razafimandimby, A.; Delamillieure, P.; Brazo, P.; Joliot, M.; Mazoyer, B.; Tzourio-Mazoyer, N. Atypical hemispheric specialization for language in right-handed schizophrenia patients. Biol. Psychiatry 2005, 57, 1020–1028. [Google Scholar] [CrossRef]
- Oertel-Knöchel, V.; Linden, D.E.J. Cerebral Asymmetry in Schizophrenia. Neuroscience 2011, 17, 456–467. [Google Scholar] [CrossRef] [PubMed]
- McCarthy-Jones, S.; Oestreich, L.K.; Whitford, T. Reduced integrity of the left arcuate fasciculus is specifically associated with auditory verbal hallucinations in schizophrenia. Schizophr. Res. 2015, 162, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falkenberga, L.E.; Westerhausen, R.; Johnsen, E.; Kroken, R.; Løberg, E.-M.; Beresniewicz, J.; Kazimierczak, K.; Kompus, K.; Ersland, L.; Sandøy, L.B.; et al. Hallucinating schizophrenia patients have longer left arcuate fasciculus fiber tracks: A DTI tractography study. Psychiatry Res. Neuroimaging 2020, 302, 111088. [Google Scholar] [CrossRef] [PubMed]
- McCarthy-Jones, S.; Smailes, D.; Corvin, A.; Gill, M.; Morris, D.W.; Dinan, T.G.; Murphy, K.C.; O’neill, F.A.; Waddington, J.L.; null Australian Schizophrenia Research Bank; et al. Occurrence and co-occurrence of hallucinations by modality in schizophrenia-spectrum disorders. Psychiatry Res. 2017, 252, 154–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayani, T.H.; David, A.S. The auditory hallucination: A phenomenological survey. Psychol. Med. 1996, 26, 177–189. [Google Scholar] [CrossRef]
- Shinn, A.K.; Pfaff, D.; Young, S.; Lewandowski, K.E.; Cohen, B.M.; Öngür, D. Auditory hallucinations in a cross-diagnostic sample of psychotic disorder patients: A descriptive, cross-sectional study. Compr. Psychiatry 2012, 53, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage 2004, 23, S208–S219. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage 2006, 31, 1487–1505. [Google Scholar] [CrossRef]
- Jenkinson, M. TBSS User Guide. 2013. Available online: https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TBSS/UserGuide#Testing_left_vs._right_in_TBSS (accessed on 1 January 2019).
- Winkler, A.M.; Ridgway, G.R.; Webster, M.A.; Smith, S.M.; Nichols, T.E. Permutation inference for the general linear model. NeuroImage 2014, 92, 381–397. [Google Scholar] [CrossRef] [Green Version]
- Nichols, T.E.; Holmes, A.P. Nonparametric permutation tests for functional neuroimaging: A primer with examples. Hum. Brain Mapp. 2002, 15, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.M.; Nichols, T.E. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. NeuroImage 2009, 44, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Bopp, M.; Zöllner, R.; Jansen, A.; Dietsche, B.; Krug, A.; Kircher, T. White matter integrity and symptom dimensions of schizophrenia: A diffusion tensor imaging study. Schizophr. Res. 2017, 184, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Gao, J.; Zhu, F.; Wang, W.; Fan, Y.; Ma, Q.; Ma, X.; Yang, J. Reduced white matter connectivity associated with auditory verbal hallucinations in first-episode and chronic schizophrenia: A diffusion tensor imaging study. Psychiatry Res. Neuroimaging 2018, 273, 63–70. [Google Scholar] [CrossRef]
- Duffau, H.; Gatignol, P.; Mandonnet, E.; Peruzzi, P.; Tzourio-Mazoyer, N.; Capelle, L. New insights into the anatomo-functional connectivity of the semantic system: A study using cortico-subcortical electrostimulations. Brain 2005, 128, 797–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friederici, A.D. Allocating functions to fiber tracts: Facing its indirectness. Trends Cogn. Sci. 2009, 13, 370–371. [Google Scholar] [CrossRef]
- Glasser, M.F.; Rilling, J.K. DTI Tractography of the Human Brain’s Language Pathways. Cereb. Cortex 2008, 18, 2471–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rilling, J.K.; Glasser, M.F.; Preuss, T.M.; Ma, X.; Zhao, T.; Hu, X.; Behrens, T.E.J. The evolution of the arcuate fasciculus revealed with comparative DTI. Nat. Neurosci. 2008, 11, 426–428. [Google Scholar] [CrossRef]
- Geschwind, N. The Organization of Language and the Brain: Language disorders after brain damage help in elucidating the neural basis of verbal behavior. Science 1970, 170, 940–944. [Google Scholar] [CrossRef]
- Hagmann, P.; Cammoun, L.; Martuzzi, R.; Maeder, P.; Clarke, S.; Thiran, J.-P.; Meuli, R.A. Hand preference and sex shape the architecture of language networks. Hum. Brain Mapp. 2006, 27, 828–835. [Google Scholar] [CrossRef] [Green Version]
- Bubb, E.J.; Metzler-Baddeley, C.; Aggleton, J.P. The cingulum bundle: Anatomy, function, and dysfunction. Neurosci. Biobehav. Rev. 2018, 92, 104–127. [Google Scholar] [CrossRef] [PubMed]
- Panksepp, J. Affective Neuroscience: The Foundations of Human and Animal Emotions; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Panksepp, J. Affective consciousness: Core emotional feelings in animals and humans. Conscious. Cogn. 2005, 14, 30–80. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Peräkylä, J.; Polvivaara, M.; Öhman, J.; Peltola, J.; Lehtimäki, K.; Huhtala, H.; Hartikainen, K.M. Human anterior thalamic nuclei are involved in emotion–attention interaction. Neuropsychology 2015, 78, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyata, J.; Sasamoto, A.; Koelkebeck, K.; Hirao, K.; Ueda, K.; Kawada, R.; Fujimoto, S.; Tanaka, Y.; Kubota, M.; Fukuyama, H.; et al. Abnormal asymmetry of white matter integrity in schizophrenia revealed by voxelwise diffusion tensor imaging. Hum. Brain Mapp. 2011, 33, 1741–1749. [Google Scholar] [CrossRef] [PubMed]
- Jäncke, L.; Wustenberg, T.; Schulze, K.; Heinze, H.J. Asymmetric hemodynamic responses of the human auditory cortex to monaural and binaural stimulation. Heart Res. 2002, 170, 166–178. [Google Scholar] [CrossRef]
- Hugdahl, K.; Heiervang, E.; Ersland, L.; Lundervold, A.; Steinmetz, H.; Smievoll, A.I. Significant relation between MR measures of planum temporale area and dichotic processing of syllables in dyslexic children. Neuropsychology 2003, 41, 666–675. [Google Scholar] [CrossRef]
- Ribolsi, M.; Daskalakis, Z.J.; Siracusano, A.; Koch, G. Abnormal Asymmetry of Brain Connectivity in Schizophrenia. Front. Hum. Neurosci. 2014, 8, 1010. [Google Scholar] [CrossRef] [Green Version]
- Kamali, A.; Flanders, A.E.; Brody, J.; Hunter, J.V.; Hasan, K.M. Tracing superior longitudinal fasciculus connectivity in the human brain using high resolution diffusion tensor tractography. Brain Struct. Funct. 2014, 219, 269–281. [Google Scholar] [CrossRef]
- Abdul-Rahman, M.F.; Qiu, A.; Woon, P.S.; Kuswanto, C.; Collinson, S.L.; Sim, K. Arcuate Fasciculus Abnormalities and Their Relationship with Psychotic Symptoms in Schizophrenia. PLoS ONE 2012, 7, e29315. [Google Scholar] [CrossRef]
- Catani, M.; Craig, M.C.; Forkel, S.J.; Kanaan, R.; Picchioni, M.; Toulopoulou, T.; Shergill, S.; Williams, S.; Murphy, D.G.; McGuire, P. Altered Integrity of Perisylvian Language Pathways in Schizophrenia: Relationship to Auditory Hallucinations. Biol. Psychiatry 2011, 70, 1143–1150. [Google Scholar] [CrossRef]
- Hugdahl, K.; Løberg, E.-M.; Falkenberg, L.E.; Johnsen, E.; Kompus, K.; Kroken, R.A.; Nygård, M.; Westerhausen, R.; Alptekin, K.; Özgören, M. Auditory verbal hallucinations in schizophrenia as aberrant lateralized speech perception: Evidence from dichotic listening. Schizophr. Res. 2012, 140, 59–64. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.J.; Pasternak, O. Does diffusion MRI tell us anything about the white matter? An overview of methods and pitfalls. Schizophr. Res. 2015, 161, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, S.; Zhang, J. Principles of Diffusion Tensor Imaging and Its Applications to Basic Neuroscience Research. Neuron 2006, 51, 527–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tønnesen, S.; Kaufmann, T.; De Lange, A.-M.G.; Richard, G.; Doan, N.T.; Alnæs, D.; Van Der Meer, D.; Rokicki, J.; Moberget, T.; Maximov, I.I.; et al. Brain Age Prediction Reveals Aberrant Brain White Matter in Schizophrenia and Bipolar Disorder: A Multisample Diffusion Tensor Imaging Study. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2020, 5, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Stoyanov, D. A linkage of mind and brain: Towards translational validity between neurobiology and psychiatry. Biomed. Rev. 2014, 22, 65. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| AVH+ | AVH- | Cntrl | p (Value) | |
|---|---|---|---|---|
| Sample size (female/male) | 44 (12/32) | 13 (2/11) | 57 (15/42) | 0.72 Fisher’s Exact test |
| Age (mean ± SD) a | 30.1 ± 11.4 | 29.5 ± 9.3 | 30.7 ± 9.9 | 0.92 ANOVA |
| Handedness (A/L/R) b | 2/4/38 | 1/1/11 | 0/6/51 | 0.35 Fisher’s Exact test |
| Scanning after/before the upgrade | 21/23 | 5/8 | 25/32 | 0.86 Fisher’s Exact test |
| Duration of illness | 3.6 ± 4.7 | 2.2 ± 4.4 | - | 0.40 Welch Two Sample t-test |
| Defined Daily Dose (DDD) | 1.02 ± 0.63 | 0.91 ± 0.41 | - | 0.51 Welch Two Sample t-test |
| Smoking/non-smoking | 28/16 | 10/3 | - | 0.51 Fisher’s Exact test |
| Baseline PANSS c positive | 3.0 ± 0.7 | 2.6 ± 0.7 | - | 0.04 Welch Two Sample t-test |
| Baseline PANSS negative | 2.4 ± 0.8 | 2.0 ± 0.7 | - | 0.99 Welch Two Sample t-test |
| Baseline PANSS total | 2.7± 0.6 | 2.3 ± 0.6 | - | 0.03 Welch Two Sample t-test |
| Number of Voxels | X (mm) a | Y (mm) | Z (mm) | Major Tracts Included in a Cluster b |
|---|---|---|---|---|
| 13231 | −36 | −1 | 28 | Anterior thalamic radiation L c: 5.9 Anterior thalamic radiation R: 2.7 Corticospinal tract L: 1.8 Corticospinal tract R: 1.0 Forceps minor: 2.0 Inferior fronto-occipital fasciculus L: 1.4 Superior longitudinal fasciculus L: 2.2 |
| 1752 | 32 | 7 | 28 | Anterior thalamic radiation R: 1.2 Forceps minor: 3.8 Superior longitudinal fasciculus R: 6.4 Superior longitudinal fasciculus (temporal part) R: 2.4 |
| 948 | 45 | −22 | 5 | Inferior fronto-occipital fasciculus R: 14.4 Inferior longitudinal fasciculus R: 9.8 |
| 530 | 34 | −59 | 29 | Superior longitudinal fasciculus R: 7.5 Superior longitudinal fasciculus (temporal part) R: 1.3 |
| 295 | 17 | −52 | 25 | Cingulum (cingulate gyrus) R: 1.3 |
| 275 | 12 | 4 | −7 | Anterior thalamic radiation R: 14.8 |
| 89 | 49 | −4 | −12 | Inferior longitudinal fasciculus R: 6.8 |
| 53 | 31 | −32 | 37 | Superior longitudinal fasciculus R: 16.3 |
| 46 | 24 | −54 | 24 | Inferior fronto-occipital fasciculus R: 5.0 Inferior longitudinal fasciculus R: 1.7 Superior longitudinal fasciculus R: 1.3 |
| 38 | 34 | −11 | −5 | Inferior fronto-occipital fasciculus R:3 9.4 Inferior longitudinal fasciculus R: 1.2 |
| 30 | 36 | −4 | −5 | Inferior fronto-occipital fasciculus R: 8.7 Superior longitudinal fasciculus R: 3.8 Superior longitudinal fasciculus (temporal part) R: 2.3 |
| 25 | 23 | −50 | 32 | Anterior thalamic radiation R: 1.9 Inferior fronto-occipital fasciculus R: 2.9 Superior longitudinal fasciculus R: 1.6 |
| 15 | 19 | −47 | 35 | Cingulum (cingulate gyrus) R: 4.2 |
| Cluster Index | Number of Voxels | X a (mm) | Y (mm) | Z (mm) | Major Tracts Included in a Cluster b |
|---|---|---|---|---|---|
| 1 | 22 | −38 | 5 | 20 | Superior longitudinal fasciculus: 13.2 Superior longitudinal fasciculus (temporal part): 6.9 (marked in green on Figure 2) |
| 2 | 20 | −38 | −9 | 34 | Superior longitudinal fasciculus: 15.4 Superior longitudinal fasciculus (temporal part): 7.0 (marked in red on Figure 2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beresniewicz, J.; Craven, A.R.; Hugdahl, K.; Løberg, E.-M.; Kroken, R.A.; Johnsen, E.; Grüner, R. White Matter Microstructural Differences between Hallucinating and Non-Hallucinating Schizophrenia Spectrum Patients. Diagnostics 2021, 11, 139. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010139
Beresniewicz J, Craven AR, Hugdahl K, Løberg E-M, Kroken RA, Johnsen E, Grüner R. White Matter Microstructural Differences between Hallucinating and Non-Hallucinating Schizophrenia Spectrum Patients. Diagnostics. 2021; 11(1):139. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010139
Chicago/Turabian StyleBeresniewicz, Justyna, Alexander R. Craven, Kenneth Hugdahl, Else-Marie Løberg, Rune Andreas Kroken, Erik Johnsen, and Renate Grüner. 2021. "White Matter Microstructural Differences between Hallucinating and Non-Hallucinating Schizophrenia Spectrum Patients" Diagnostics 11, no. 1: 139. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010139