Comparison of Two Different Semiquantitative Urinary Dipstick Tests with Albumin-to-Creatinine Ratio for Screening and Classification of Albuminuria According to KDIGO. A Diagnostic Test Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
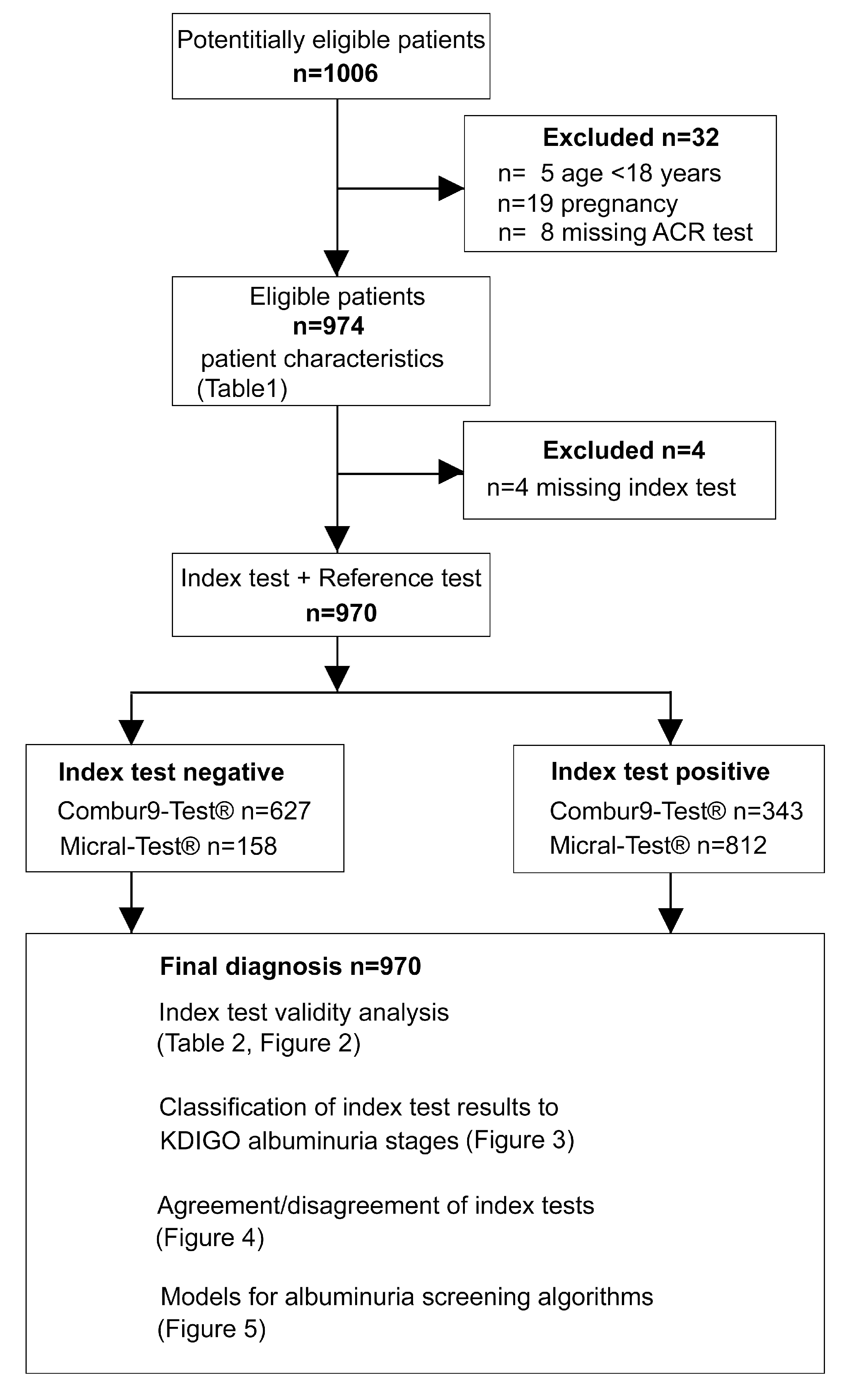
2.1. Study Population
2.2. Reporting
2.3. Measurements and Procedures
2.4. Outcomes/Aims
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
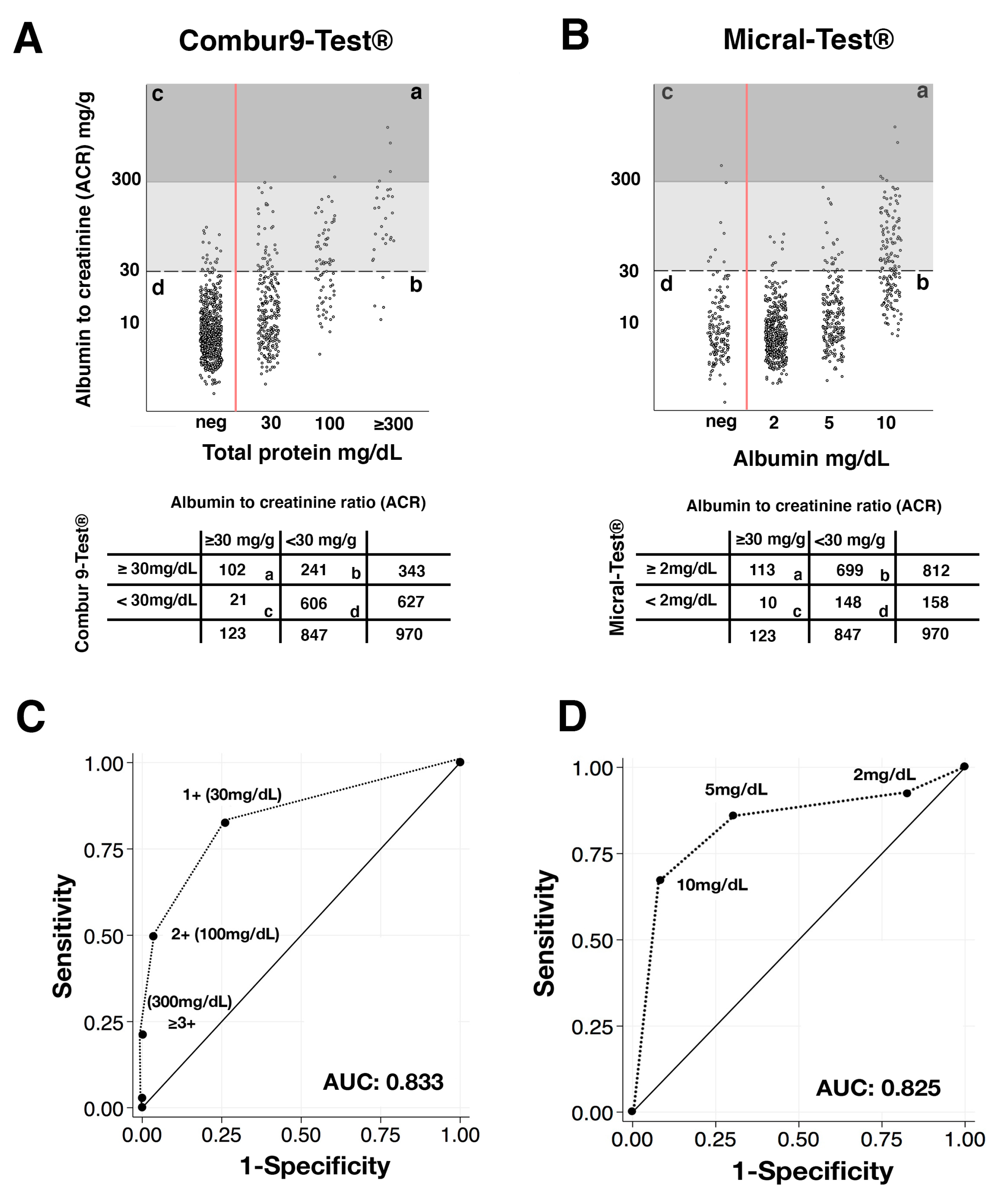
3.2. Sensitivity and Specificity Analysis of Semiquantitative Urine Dipstick Tests Compared with Albumin-to-Creatinine Ratio Test
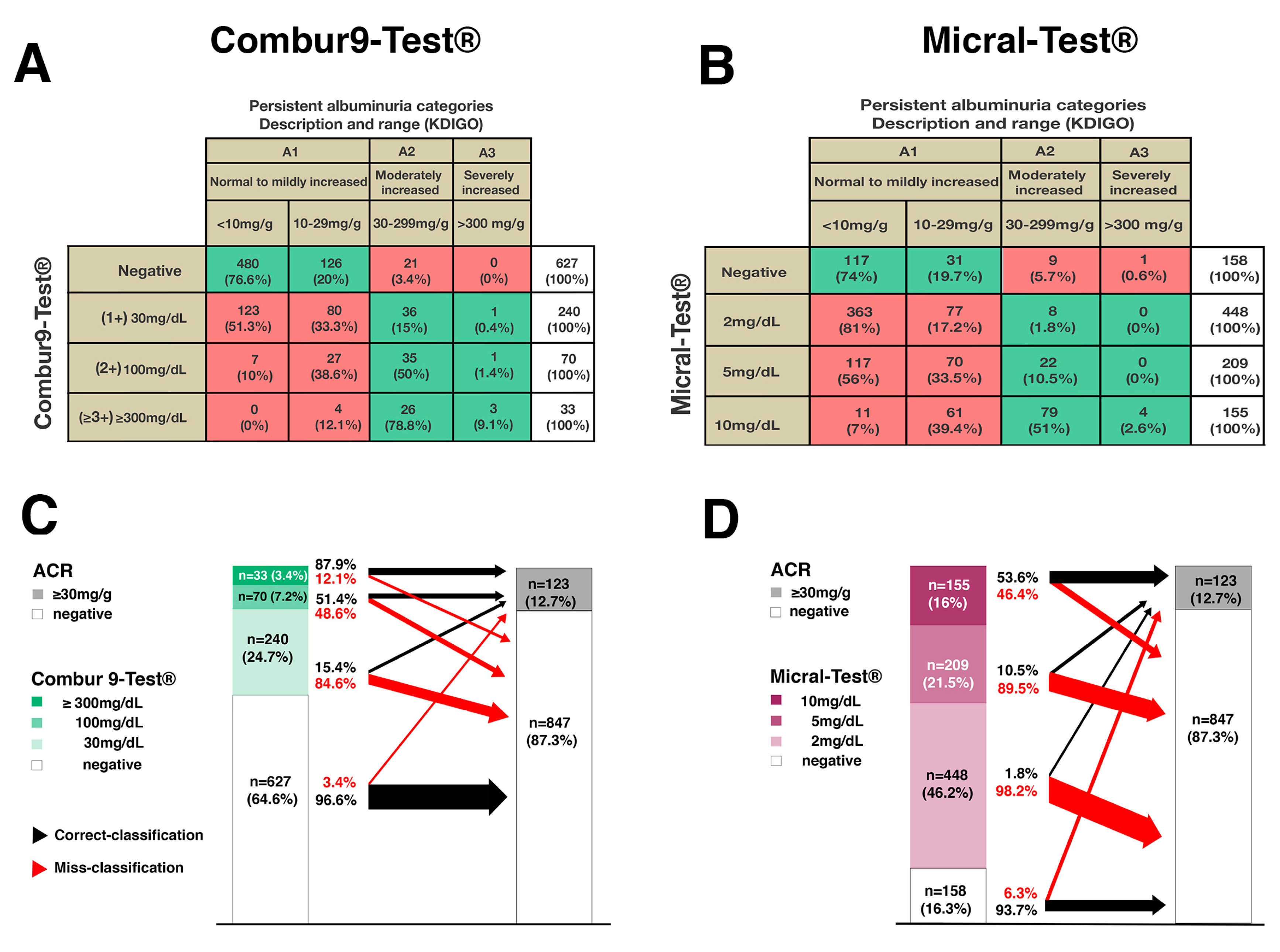
3.3. Distribution of The Semiquantitative Urine Dipstick Test Results within the KDIGO Albuminuria Classification
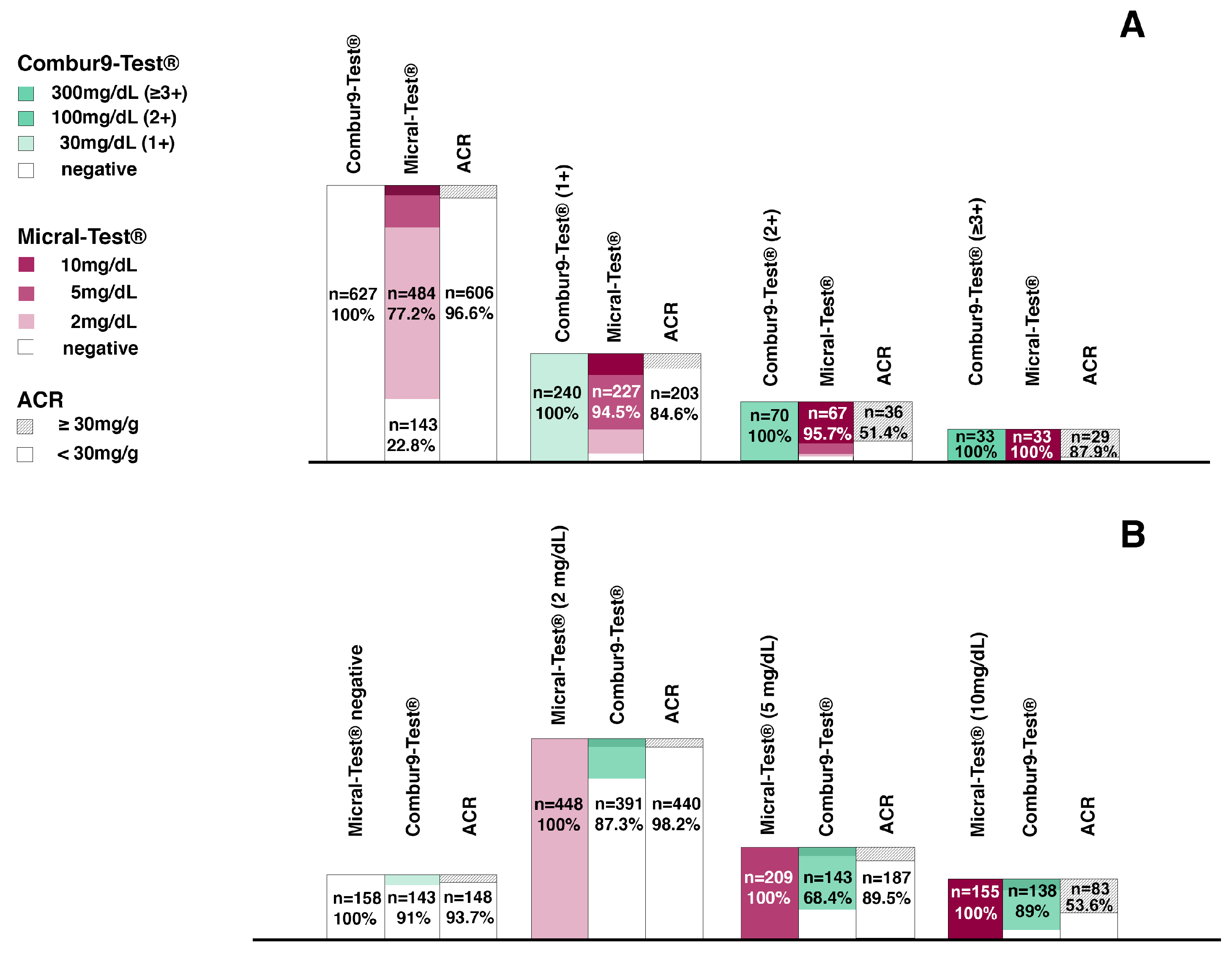
3.4. Agreement of the Micral-Test® with the Combur9-Test®
3.5. Significance of Possible Models for Albuminuria Screening Algorithms Based on Combur9-Test® or Micral-Test® in Clinical Practice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic kidney disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes. Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431. [Google Scholar] [CrossRef] [Green Version]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Hodel, N.C.; Hamad, A.; Praehauser, C.; Mwangoka, G.; Kasella, I.M.; Reither, K.; Abdulla, S.; Hatz, C.F.R.; Mayr, M. The epidemiology of chronic kidney disease and the association with non-communicable and communicable disorders in a population of Sub-Saharan Africa. PLoS ONE 2018, 13, e0205326. [Google Scholar] [CrossRef] [Green Version]
- Hallan, S.; Astor, B.; Romundstad, S.; Aasarod, K.; Kvenild, K.; Coresh, J. Association of kidney function and albuminuria with cardiovascular mortality in older vs younger individuals: The hunt II study. Arch. Intern. Med. 2007, 167, 2490–2496. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Graziani, M.S.; Gambaro, G.; Mantovani, L.; Sorio, A.; Yabarek, T.; Abaterusso, C.; Lupo, A.; Rizzotti, P. Diagnostic accuracy of a reagent strip for assessing urinary albumin excretion in the general population. Nephrol. Dial. Transplant. 2009, 24, 1490–1494. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.T.; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J. Lower estimated gfr and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011, 80, 93–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmelgarn, B.R.; Manns, B.J.; Lloyd, A.; James, M.T.; Klarenbach, S.; Quinn, R.R.; Wiebe, N.; Tonelli, M. Relation between kidney function, proteinuria, and adverse outcomes. JAMA 2010, 303, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Stanifer, J.W.; Maro, V.; Egger, J.; Karia, F.; Thielman, N.; Turner, E.L.; Shimbi, D.; Kilaweh, H.; Matemu, O.; Patel, U.D. The epidemiology of chronic kidney disease in northern Tanzania: A population-based survey. PLoS ONE 2015, 10, e0124506. [Google Scholar] [CrossRef] [Green Version]
- Kaze, F.F.; Kengne, A.-P.; Magatsing, C.T.; Halle, M.-P.; Yiagnigni, E.; Ngu, K.B. Prevalence and determinants of chronic kidney disease among hypertensive Cameroonians according to three common estimators of the glomerular filtration rate. J. Clin. Hypertens. 2016, 18, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Padilla, J.A.; Mendoza-Garcia, M.; Plascencia-Perez, S.; Renoirte-Lopez, K.; Garcia-Garcia, G.; Lloyd, A.; Tonelli, M. Screening for CKD and cardiovascular disease risk factors using mobile clinics in Jalisco, Mexico. Am. J. Kidney Dis. 2010, 55, 474–484. [Google Scholar] [CrossRef]
- Park, J.I.; Baek, H.; Kim, B.R.; Jung, H.H. Comparison of urine dipstick and albumin: Creatinine ratio for chronic kidney disease screening: A population-based study. PLoS ONE 2017, 12, e0171106. [Google Scholar] [CrossRef]
- Konta, T.; Hao, Z.; Takasaki, S.; Abiko, H.; Ishikawa, M.; Takahashi, T.; Ikeda, A.; Ichikawa, K.; Kato, T.; Kawata, S.; et al. Clinical utility of trace proteinuria for microalbuminuria screening in the general population. Clin. Exp. Nephrol. 2007, 11, 51–55. [Google Scholar] [CrossRef]
- Efundem, N.T.; Assob, J.C.N.; Feteh, V.F.; Choukem, S.-P. Prevalence and associations of microalbuminuria in proteinuria-negative patients with type 2 diabetes in two regional hospitals in Cameroon: A cross-sectional study. BMC Res. Notes 2017, 10, 477. [Google Scholar] [CrossRef] [Green Version]
- Davidson, M.B.; Smiley, J.F. Relationship between dipstick positive proteinuria and albumin: Creatinine ratios. J. Diabetes Complicat. 1999, 13, 52–55. [Google Scholar] [CrossRef]
- White, S.L.; Yu, R.; Craig, J.C.; Polkinghorne, K.R.; Atkins, R.C.; Chadban, S.J. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general community. Am. J. Kidney Dis. 2011, 58, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Tanzania Population Census 2012. National Bureau of Statistics Ministry of Finance dDar es Salaam. Available online: https://www.Nbs.Go.Tz/nbstz/index.Php/english/statistics-by-subject/population-and-housing-census (accessed on 12 December 2017).
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.; et al. Stard 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef] [PubMed]
- La-Roche. Kompendium der Urinanalyse. 2014. Available online: https://www.scribd.com/document/346737863/urinanalyse-kompendium (accessed on 5 March 2020).
- Boege, F.; Luther, A. Gesamtproteinbestimmung im urin: Adaptierung einer nephelometrischen methode zur erfassung typischer leitproteine und bence-jones-proteine. LaboratoriumsMedizin/J. Lab. Med. 1989, 13, 14. [Google Scholar] [CrossRef]
- Bökenkamp, A. Proteinuria—Take a closer look! Pediatr. Nephrol. 2020, 35, 533–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar]
- Van der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B.C.; Woodward, M.; Levey, A.; de Jong, P.; Gansevoort, R.T.; van der Velde, M.; Matsushita, K.; et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011, 79, 1341–1352. [Google Scholar] [CrossRef] [Green Version]
- Danaei, G.; Lu, Y.; Singh, G.M.; Carnahan, E.; Stevens, G.A.; Cowan, M.J.; Farzadfar, F.; Lin, J.K.; Finucane, M.M.; Rao, M. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: A comparative risk assessment. Lancet Diabetes Endocrinol. 2014, 2, 634–647. [Google Scholar]
- Gilbert, R.E.; Akdeniz, A.; Jerums, G. Detection of microalbuminuria in diabetic patients by urinary dipstick. Diabetes Res. Clin. Pract. 1997, 35, 57–60. [Google Scholar] [CrossRef]
- Spooren, P.F.M.J.; Lekkerkerker, J.F.F.; Vermes, I. Micral-test®: A qualitative dipstick test for micro-albuminuria. Diabetes Res. Clin. Pract. 1992, 18, 83–87. [Google Scholar] [CrossRef]
- FDA (U.S. Food and Drug Administration). 510(k) Safety and Effectiveness Summary (k963142). 1996. Available online: https://www.Accessdata.Fda.Gov/cdrh_docs/pdf/k963142.Pdf (accessed on 10 April 2020).
- Levey, A.S.; de Jong, P.E.; Coresh, J.; Nahas, M.E.I.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.-U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO controversies conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G. Hypertension: Strengths and limitations of the JNC 8 hypertension guidelines. Nat. Rev. Cardiol. 2014, 11, 189–190. [Google Scholar] [CrossRef] [PubMed]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011; Available online: http://www.Who.Int/vmnis/indicators/haemoglobin.Pdf (accessed on 21 February 2019).
- Nagrebetsky, A.; Jin, J.; Stevens, R.; James, T.; Adler, A.; Park, P.; Craven, A.; Shine, B.; Farmer, A. Diagnostic accuracy of urine dipstick testing in screening for microalbuminuria in type 2 diabetes: A cohort study in primary care. Fam. Pract. 2012, 30, 142–152. [Google Scholar] [CrossRef] [Green Version]
- Zeller, A.; Sigle, J.P.; Battegay, E.; Martina, B. Value of a standard urinary dipstick test for detecting microalbuminuria in patients with newly diagnosed hypertension. Swiss Med. Wkly. 2005, 135, 57–61. [Google Scholar]
- Vuljanić, D.; Dojder, A.; Špoljarić, V.; Saračević, A.; Dukić, L.; Leniček-Krleža, J.; Vlašić-Tanasković, J.; Maradin, I.; Grzunov, A.; Vogrinc, Ž; et al. Analytical verification of 12 most commonly used urine dipsticks in Croatia: Comparability, repeatability and accuracy. Biochem. Med. (Zagreb) 2019, 29, 010708. [Google Scholar]
- Wen, C.P.; Yang, Y.C.; Tsai, M.K.; Wen, S.F. Urine dipstick to detect trace proteinuria: An underused tool for an underappreciated risk marker. Am. J. Kidney Dis. 2011, 58, 1–3. [Google Scholar] [CrossRef]
- Masimango, M.I.; Sumaili, E.K.; Jadoul, M.; Wallemacq, P.; Mubagwa, D.K.; Makulo, R.J.; Lepira, F.B.; Nseka, N.M. Prevalence of microalbuminuria and diagnostic value of dipstick proteinuria in outpatients from HIV clinics in Bukavu, the Democratic Republic of Congo. BMC Nephrol. 2014, 15, 146. [Google Scholar] [CrossRef] [Green Version]
- Solarin, A.; Njokanma, F. The micral-test as a screening tool to detect microalbuminuria in children 5–15 years old with sickle cell anaemia, Lagos State University Teaching Hospital. SAJCH 2015, 9, 41–44. [Google Scholar]
- Brenner, H.; Gefeller, O. Variation of sensitivity, specificity, likelihood ratios and predictive values with disease prevalence. Stat. Med. 1997, 16, 981–991. [Google Scholar] [CrossRef]
- Peck, R.; Baisley, K.; Kavishe, B.; Were, J.; Mghamba, J.; Smeeth, L.; Grosskurth, H.; Kapiga, S. Decreased renal function and associated factors in cities, towns and rural areas of Tanzania: A community-based population survey. Trop. Med. Int. Health 2016, 21, 393–404. [Google Scholar] [CrossRef] [Green Version]
- Kalyesubula, R.; Nankabirwa, J.I.; Ssinabulya, I.; Siddharthan, T.; Kayima, J.; Nakibuuka, J.; Salata, R.A.; Mondo, C.; Kamya, M.R.; Hricik, D. Kidney disease in Uganda: A community based study. BMC Nephrol. 2017, 18, 116. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, G.; Upadhyay, A. Assessment of proteinuria. Adv. Chronic Kidney Dis. 2011, 18, 243–248. [Google Scholar] [CrossRef]
- Kamimura, T.; Fukumitsu, K.; Aihara, S.; Kondo, M.; Oka, H.; Harada, A. The importance of urine specific gravity measurment in urine dipstick testing. Nephrol. Dial. Transplant. 2017, 32, 484–485. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (Missing) | Overall | ACR < 30 mg/g | ACR ≥ 30 mg/g | p-Value | |
|---|---|---|---|---|---|
| Overall | 974 | 974 | 850 (87.3%) | 124 (12.7%) (# CI 95%: 10.6–14.8%) | |
| Male vs. | 974 | 301 (30%) | 261 (87%) | 40 (13%) | |
| Female | 673 (70%) | 589 (88%) | 84 (12%) | 0.755 * | |
| Age (years) | 968 (6) | 37 (18–91) | 36 (18–91) | 45 (18–84) | <0.001 ° |
| BMI (kg/m2) † | 971(3) | 24 (14–53) | 24.1 (14–53) | 23.8 (15–43) | 0.651 ° |
| BP systolic (mmHg) ‡ | 971 (3) | 124 (70–286) | 129 (70–222) | 144 (72–286) | <0.001 ° |
| BP diastolic (mmHg) § Hypertension stage I • Hypertension stage II •• HbA1c (%) ¶ HbA1c ≥ 6.5% Diabetes Φ Hemoglobin (g/dL)Anemia (WHO) ** Acute infection ## HIV positive ƒ History of tuberculosis | 971 (3) 971 (3) 971 (3) 965 (9) 965 (9) 974 910 (64) 903 (71) 974 974 972 (2) | 80 (36–150) 261 (27%) 115 (12%) 5.4 (3.9–14) 63 (6.5%) 67 (6.8%) 12.8 (4.1–22) 321 (36%) 81 (8.3%) 64 (6.6%) 46 (4.7%) | 80 (36–140) 204 (24%) 80 (9%) 5.4 (3.9–14) 44 (42%) 47 (5.5%) 12.8 (4.1–22) 275 (35%) 63 (7.4%) 50 (5.9%) 32 (3.8%) | 90 (42–150) 57 (46%) 35 (28%) 5.6 (4.2–14) 19 (15%) 20 (16%) 12.5 (6.3–16) 46 (43%) 18 (14%) 14 (11%) 14 (11%) | <0.001 ° <0.001 * <0.001 * 0.004 ° <0.001 * <0.001 * 0.017 ° 0.084 * 0.013 * 0.032 * 0.001 * |
| History of Smoking | 974 | 74 (7.6%) | 65 (7.7%) | 9 (7.3%) | 1.000 * |
| Test | n (%) | n (%) + ACR ≥30 mg/g | Sensitivity % (CI 95%) | Specificity % (CI 95%) | PPV (CI 95%) | NPV (CI 95%) |
|---|---|---|---|---|---|---|
| ACR ≥30 mg/g | 123 (12.7%) | |||||
| Combur9-Test® | 970 (100%) | |||||
| ≥30 mg/dL | 343 (35.4%) | 102 (10.5%) | 82.9% (75.1–89.1%) n = 102/123 * n = 21 | 71.5% (68.4–74.6%) n = 606/847 ° n = 241 | 29.7% (24.9–34.9%) n = 102/343 ° n = 241 | 96.7% (94.9–97.9%) n = 606/627 * n = 21 |
| ≥100 mg/dL | 102 (10.5%) | 65 (6.7%) | 52.8% (44.1–62.2%) n = 65/123 * n = 58 | 95.5% (93.5–96.5%) n = 809/847 ° n = 38 | 63.1% (51.8–70.9%) n = 65/103 ° n = 38 | 93.3% (91.4–94.9%) n = 809/867 * n = 58 |
| ≥300 mg/dL | 33 (3.7%) | 29 (3.3%) | 26.0% (17.0–32.7%) n = 29/123 * n = 94 | 99.5% (98.3–99.7%) n = 843/847 ° n = 4 | 87.9% (64.8–92.0%) n = 29/33 ° n = 4 | 90.0% (87.9–91.8%) n = 843/937 * n = 94 |
| Micral–Test® | 970 (100%) | |||||
| ≥2 mg/dL | 812 (83.7%) | 113 (11.6%) | 91.9% (85.6–96.3%) n = 113/123 * n = 10 | 17.5% (15.0–20.2%) n = 148/847 ° n = 699 | 13.9% (11.6–16.5%) n = 113/812 ° n = 699 | 93.7% (88.7–96.9%) n = 148/158 * n = 10 |
| ≥5 mg/dL | 364 (37.4%) | 105 (10.8%) | 85.4% (77.9–91.1%) n = 105/123 * n = 18 | 69.4% (66.2–72.5%) n = 588/847 ° n = 259 | 28.9% (24.3–33.8%) n = 105/364 ° n = 259 | 97.0% (95.4–98.2%) n = 588/606 * n = 18 |
| ≥10 mg/dL | 155 (15.9%) | 83 (8.6%) | 67.5% (58.5–75.7%) n = 83/123 * n = 40 | 91.5% (89.4–93.3%) n = 775/847 ° n = 72 | 53.5% (45.4–61.6%) n = 83/155 ° n = 72 | 95.1% (93.4–96.5%) n = 775/815 * n = 94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodel, N.C.; Hamad, A.; Reither, K.; Kasella, I.M.; Abdulla, S.; Schoetzau, A.; Hatz, C.F.R.; Mayr, M. Comparison of Two Different Semiquantitative Urinary Dipstick Tests with Albumin-to-Creatinine Ratio for Screening and Classification of Albuminuria According to KDIGO. A Diagnostic Test Study. Diagnostics 2021, 11, 81. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010081
Hodel NC, Hamad A, Reither K, Kasella IM, Abdulla S, Schoetzau A, Hatz CFR, Mayr M. Comparison of Two Different Semiquantitative Urinary Dipstick Tests with Albumin-to-Creatinine Ratio for Screening and Classification of Albuminuria According to KDIGO. A Diagnostic Test Study. Diagnostics. 2021; 11(1):81. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010081
Chicago/Turabian StyleHodel, Nikolai C., Ali Hamad, Klaus Reither, Irene Mndala Kasella, Salim Abdulla, Andreas Schoetzau, Christoph F. R. Hatz, and Michael Mayr. 2021. "Comparison of Two Different Semiquantitative Urinary Dipstick Tests with Albumin-to-Creatinine Ratio for Screening and Classification of Albuminuria According to KDIGO. A Diagnostic Test Study" Diagnostics 11, no. 1: 81. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010081