
Diagnostic Performance of KLCA-NCC 2018 Criteria for Hepatocellular Carcinoma Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis
3. Results
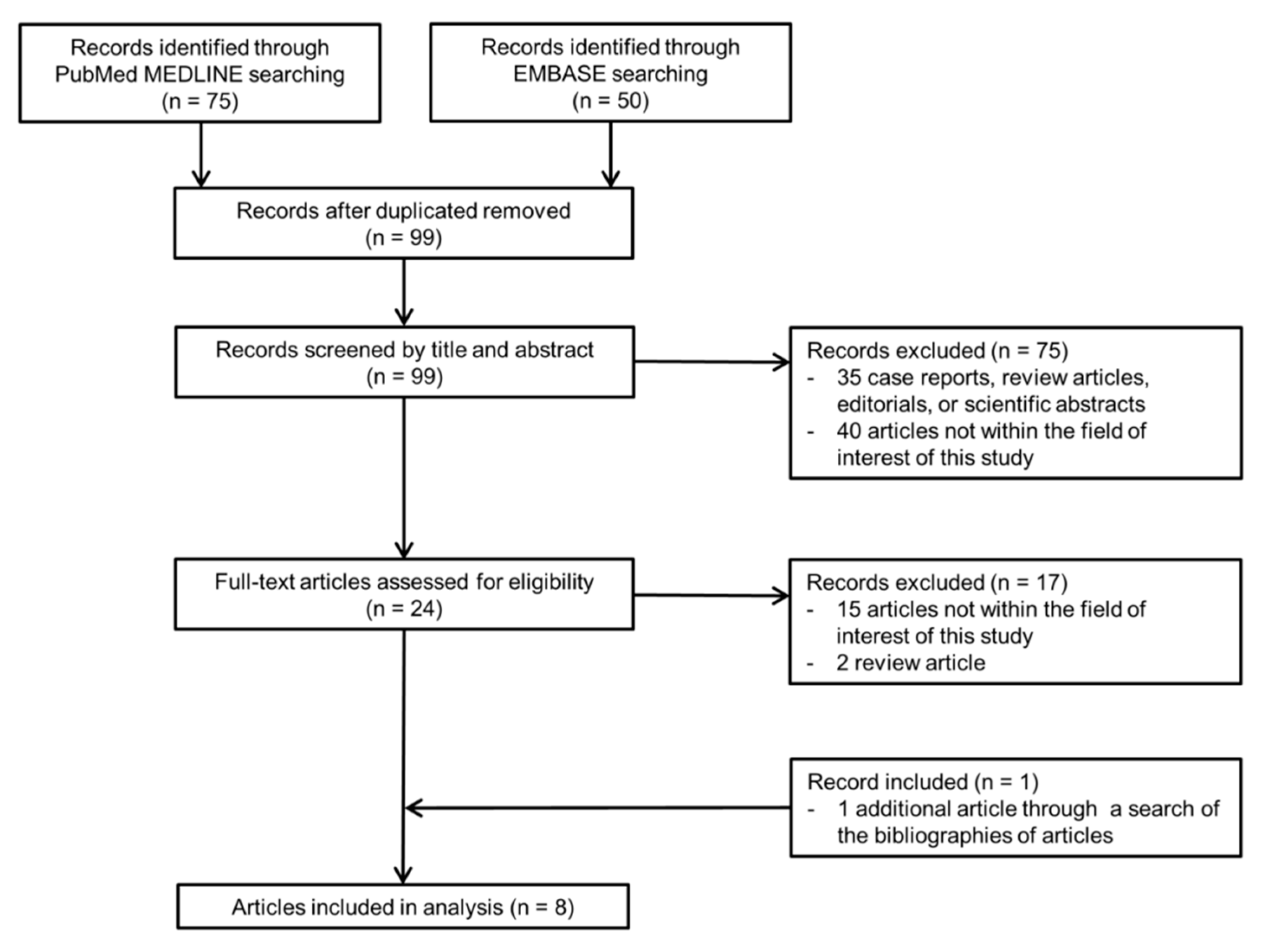
3.1. Literature Search
3.2. Quality Assessment
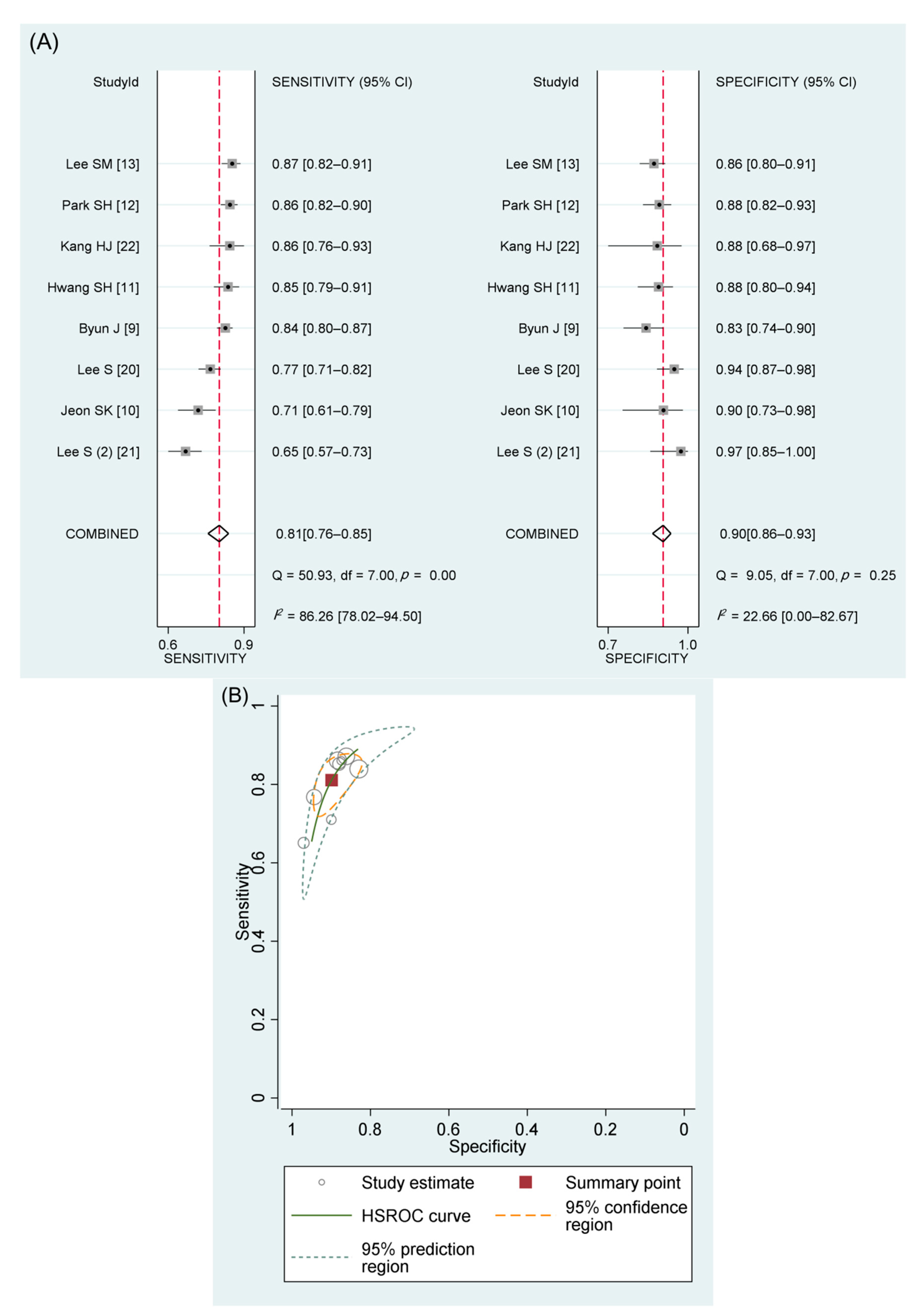
3.3. Performance of the KLCA-NCC 2018 Criteria in Diagnosing HCC
3.4. Subgroup Analysis Comparing the Performance of Different International Guidelines
3.5. Meta-Regression Analysis
3.6. Interobserver Agreement for Categorization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Korean Liver Cancer Association; National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Korean J. Radiol. 2019, 20, 1042–1113. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W. Korean Liver Cancer Study Group and National Cancer Center. Practice guideline for diagnosis and treatment of hepatocellular carcinoma. Korean J. Hepatol. 2004, 10, 88–98. [Google Scholar]
- Korean Liver Cancer Study Group and National Cancer Center, Korea. Practice guidelines for management of hepatocellular carcinoma 2009. Korean J. Hepatol. 2009, 15, 391–423. [Google Scholar] [CrossRef]
- Korean Liver Cancer Study Group (KLCSG); National Cancer Center, Korea (NCC). 2014 KLCSG-NCC Korea practice guideline for the management of hepatocellular carcinoma. Gut Liver 2015, 9, 267–317. [Google Scholar]
- Byun, J.; Choi, S.H.; Byun, J.H.; Lee, S.J.; Kim, S.Y.; Won, H.J.; Shin, Y.M.; Kim, P.N. Comparison of the diagnostic performance of imaging criteria for HCCs </= 3.0 cm on gadoxetate disodium-enhanced MRI. Hepatol. Int. 2020, 14, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.K.; Lee, J.M.; Joo, I.; Yoo, J.; Park, J.Y. Comparison of guidelines for diagnosis of hepatocellular carcinoma using gadoxetic acid-enhanced MRI in transplantation candidates. Eur. Radiol. 2020, 30, 4762–4771. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.H.; Park, M.S.; Park, S.; Lim, J.S.; Kim, S.U.; Park, Y.N. Comparison of the current guidelines for diagnosing hepatocellular carcinoma using gadoxetic acid-enhanced magnetic resonance imaging. Eur. Radiol. 2021, 31, 4492–4503. [Google Scholar] [CrossRef]
- Park, S.H.; Shim, Y.S.; Kim, B.; Kim, S.Y.; Kim, Y.S.; Huh, J.; Park, J.H.; Kim, K.W.; Lee, S.S. Retrospective analysis of current guidelines for hepatocellular carcinoma diagnosis on gadoxetic acid-enhanced MRI in at-risk patients. Eur. Radiol. 2021, 31, 4751–4763. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.M.; Ahn, S.J.; Kang, H.J.; Yang, H.K.; Yoon, J.H. Diagnostic Performance of 2018 KLCA-NCC Practice Guideline for Hepatocellular Carcinoma on Gadoxetic Acid-Enhanced MRI in Patients with Chronic Hepatitis B or Cirrhosis: Comparison with LI-RADS Version 2018. Korean J. Radiol. 2021, 22, 1066–1076. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Devillé, W.L.; Buntinx, F.; Bouter, L.M.; Montori, V.M.; De Vet, H.C.; Van der Windt, D.A.; Bezemer, P.D. Conducting systematic reviews of diagnostic studies: Didactic guidelines. BMC Med. Res. Methodol. 2002, 2, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Radiology. CT/MRI Liver Imaging Reporting and Data System Version 2018. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2018 (accessed on 8 May 2021).
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Kim, S.S.; Chang, D.R.; Kim, H.; Kim, M.J. Comparison of LI-RADS 2018 and KLCA-NCC 2018 for noninvasive diagnosis of hepatocellular carcinoma using magnetic resonance imaging. Clin. Mol. Hepatol. 2020, 26, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, M.J. Validation of the Korean Liver Cancer Association-National Cancer Center 2018 Criteria for the Noninvasive Diagnosis of Hepatocellular Carcinoma Using Magnetic Resonance Imaging. J. Liver Cancer 2020, 20, 120–127. [Google Scholar] [CrossRef]
- Kang, H.J.; Lee, J.M.; Yoon, J.H.; Han, J.K. Role of Contrast-Enhanced Ultrasound as a Second-Line Diagnostic Modality in Noninvasive Diagnostic Algorithms for Hepatocellular Carcinoma. Korean J. Radiol. 2021, 22, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Choi, S.H.; Kim, S.Y.; Kim, M.J.; Lee, S.S.; Byun, J.H. Gadoxetic Acid-enhanced MRI of Hepatocellular Carcinoma: Value of Washout in Transitional and Hepatobiliary Phases. Radiology 2019, 291, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Joo, I.; Lee, J.M.; Lee, D.H.; Jeon, J.H.; Han, J.K. Retrospective validation of a new diagnostic criterion for hepatocellular carcinoma on gadoxetic acid-enhanced MRI: Can hypointensity on the hepatobiliary phase be used as an alternative to washout with the aid of ancillary features? Eur. Radiol. 2019, 29, 1724–1732. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014, 272, 635–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Choi, S.H.; Park, S.H.; Kim, K.W.; Byun, J.H.; Kim, S.Y.; Lee, S.S.; Shin, Y.M.; Won, H.J.; Kim, P.N. Meta-analysis of the accuracy of Liver Imaging Reporting and Data System category 4 or 5 for diagnosing hepatocellular carcinoma. Gut 2019, 68, 1719–1721. [Google Scholar] [CrossRef]
- Fowler, K.J.; Sirlin, C.B. Is It Time to Expand the Definition of Washout Appearance in LI-RADS? Radiology 2019, 291, 658–659. [Google Scholar] [CrossRef]
- Kim, S.Y. Diagnosis of hepatocellular carcinoma: Which MRI contrast agent? Which diagnostic criteria? Clin. Mol. Hepatol. 2020, 26, 309–311. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Year of Publication) | Study Design | No. of Patients (% Male) | Patient Age, Years * | Most Common Etiology of Liver Disease (% of Cirrhosis) | No. of Hepatic Lesions | No. of HCC (%) | HCC Size, mm * | Indication for Liver MRI | MRI Magnet | MRI Contrast Agent (%) | Image Reviewer | Reference Standard for HCC | Reference Standard for Non-HCC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Byun J (2020) [9] | Retrospective | 400 (80.5) | 59.7 | Hepatitis B virus (NA) | 493 | 399 (80.9) | 21 (range, 10–30) | Evaluation of hepatic nodule detected during surveillance | 1.5- or 3.0-T | HBA | Multiple reviewers with consensus | Pathology or imaging follow-up | Pathology or imaging follow-up |
| Jeon SK (2020) [10] | Retrospective | 81 (82.7) | 54.1 ± 8.7 | Hepatitis B virus (NA) | 137 | 107 (78.1) | 20 ± 16 | Pretransplant work-up | 1.5- or 3.0-T | HBA | Multiple independent reviewers | Pathology only | Pathology only |
| Lee S (2020) [20] | Retrospective | 273 (68.9) | 57.3 ± 9.5 | Hepatitis B virus (54.9) | 352 | 263 (74.7) | 24 (range, 15–34) | Evaluation of hepatic nodule detected during surveillance | 3.0-T | ECA or HBA | Multiple reviewers with consensus | Pathology only | Pathology or imaging follow-up |
| Lee S (2020) (2) [21] | Retrospective | 142 (73.2) | 57.2 ± 9.9 | Hepatitis B virus (NA) | 183 | 149 (81.4) | 30.2 ± 23.9 | Evaluation of hepatic nodule detected during surveillance | 1.5- or 3.0-T | ECA or HBA | Multiple reviewers with consensus | Pathology only | Pathology or imaging follow-up |
| Hwang SH (2021) [11] | Retrospective | 177 (80.2) | 58 | Hepatitis B virus (NA) | 241 | 149 (61.8) | 20, median | Evaluation of hepatic nodule detected during surveillance | 3.0-T | HBA | Multiple independent reviewers | Pathology only | Pathology or imaging follow-up |
| Kang HJ (2021) [22] | Prospective | 103 (78.6) | 63.1 | Hepatitis B virus (43.7) | 103 | 79 (76.7) | 28.2 (range, 11–114) | Evaluation of hepatic nodule detected during surveillance | 1.5- or 3.0-T | HBA | Multiple independent reviewers | Pathology or imaging follow-up | Pathology or imaging follow-up |
| Lee SM (2021) [13] | Retrospective | 387 (78.8) | 59 ± 10 | Hepatitis B virus (74.2) | 422 | 234 (55.5) | 32 ± 21 (all lesions) | Evaluation of hepatic nodule detected during surveillance | 1.5- or 3.0-T | HBA | Multiple independent reviewers | Pathology only | Pathology or imaging follow-up |
| Park SH (2021) [12] | Retrospective | 386 (76.2) | 56.4 ± 10.3 | Hepatitis B virus (70.2) | 447 | 310 (69.4) | 18.6 ± 6.3 | Evaluation of hepatic nodule detected during surveillance | 1.5- or 3.0-T | HBA | Multiple independent reviewers | Pathology only | Pathology or imaging follow-up |
| For All HCCs | For HCCs Smaller than 20 mm | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Total Number of Nodules | Number of Lesions | Sensitivity (95% CI) | Specificity (95% CI) | Number of Lesions | Sensitivity (95% CI) | Specificity (95% CI) | ||||||
| TP | FP | FN | TN | TP | FP | FN | TN | ||||||
| Byun J (2020) [9] | 493 | 335 | 16 | 64 | 78 | 84% (80, 87) | 83% (74, 90) | 136 | 10 | 27 | 60 | 83% (77, 89) | 86% (75, 93) |
| Jeon SK (2020) [10] | 137 | 76 | 3 | 31 | 27 | 71% (61, 79) | 90% (73, 98) | 39 | 2 | 21 | 21 | 65% (52, 77) | 91% (72, 99) |
| Lee S (2020) [20] | 352 | 202 | 5 | 61 | 84 | 77% (71, 82) | 94% (87, 98) | 57 | 2 | 22 | 51 | 72% (61, 82) | 96% (87, 100) |
| Lee S (2020) (2) [21] | 183 | 97 | 1 | 52 | 33 | 65% (57, 73) | 97% (85, 100) | ||||||
| Hwang SH (2021) [11] | 241 | 127 | 11 | 22 | 81 | 85% (79, 91) | 88% (80, 94) | ||||||
| Kang HJ (2021) [22] | 103 | 68 | 3 | 11 | 21 | 86% (76, 93%) | 88% (68, 97) | ||||||
| Lee SM (2021) [13] | 422 | 204 | 26 | 30 | 162 | 87% (82, 91) | 86% (80, 91%) | 40 | 14 | 5 | 114 | 89% (76, 96) | 89% (82, 94) |
| Park SH (2021) [12] | 447 | 267 | 16 | 43 | 121 | 86% (82, 90) | 88% (82, 93%) | 111 | 12 | 20 | 106 | 85% (77, 90) | 90% (83, 95) |
| Higgins I2 for study heterogeneity | 86% | 23% | 76% | 0% | |||||||||
| Meta-analytic summary estimate using the bivariate model | 81% (76, 85) | 90% (86, 93) | 80% (72, 86) * | 91% (86, 94) * | |||||||||
| Meta-Analytic Summary Estimate | ||||
|---|---|---|---|---|
| Covariates | Subgroup | Sensitivity (95% CI) | Specificity (95% CI) | p-Value |
| Study design | Prospective (n = 1) | 86% (74, 98) | 88% (72, 100) | 0.74 |
| Retrospective (n = 7) | 80% (75, 86) | 90% (86, 94) | ||
| Number of patients | <200 (n = 4) | 77% (70, 85) | 91% (86, 96) | 0.42 |
| ≥200 (n = 4) | 84% (79, 89) | 88% (84, 93) | ||
| MRI scanner field | 3.0 T only (n = 2) | 81% (72, 91) | 91% (86, 97) | 0.70 |
| strength | 1.5 T or 3.0 T (n = 6) | 81% (75, 87) | 89% (85, 93) | |
| MRI contrast agent | Hepatobiliary contrast agent (n = 6) | 84% (80, 87) | 87% (84, 90) | 0.01 |
| Extracellular or hepatobiliary contrast agent (n = 2) | 72% (63, 80) | 95% (91, 99) | ||
| Image interpretation | Multiple independent reviewers (n = 5) | 84% (79, 89) | 89% (84, 93) | 0.27 |
| method | Multiple reviewers with consensus (n = 3) | 76% (69, 84) | 92% (86, 97) | |
| Reference standard | Pathology only (n = 6) | 80% (74, 86) | 91% (87, 95) | 0.25 |
| for HCC | Pathology or imaging follow-up (n = 2) | 85% (76, 93) | 84% (74, 93) | |
| Reference standard | Pathology only (n = 1) | 71% (54, 88) | 90% (77, 100) | 0.35 |
| for non-HCC | Pathology or imaging follow-up (n = 7) | 82% (78, 87) | 90% (86, 94) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Kim, B.; Youn, S.Y.; Kim, H.; Choi, J.-I. Diagnostic Performance of KLCA-NCC 2018 Criteria for Hepatocellular Carcinoma Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 1763. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101763
Kim DH, Kim B, Youn SY, Kim H, Choi J-I. Diagnostic Performance of KLCA-NCC 2018 Criteria for Hepatocellular Carcinoma Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Diagnostics. 2021; 11(10):1763. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101763
Chicago/Turabian StyleKim, Dong Hwan, Bohyun Kim, Seo Yeon Youn, Hokun Kim, and Joon-Il Choi. 2021. "Diagnostic Performance of KLCA-NCC 2018 Criteria for Hepatocellular Carcinoma Using Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis" Diagnostics 11, no. 10: 1763. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101763