
Depth of Stromal Invasion as the Most Prognostically Relevant Regression System in Locally Advanced Cervical Cancer after Neoadjuvant Treatment: A Systematic Review and Meta-Analysis Grading

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Risk of Bias Assessment
2.4. Data Analysis
3. Results
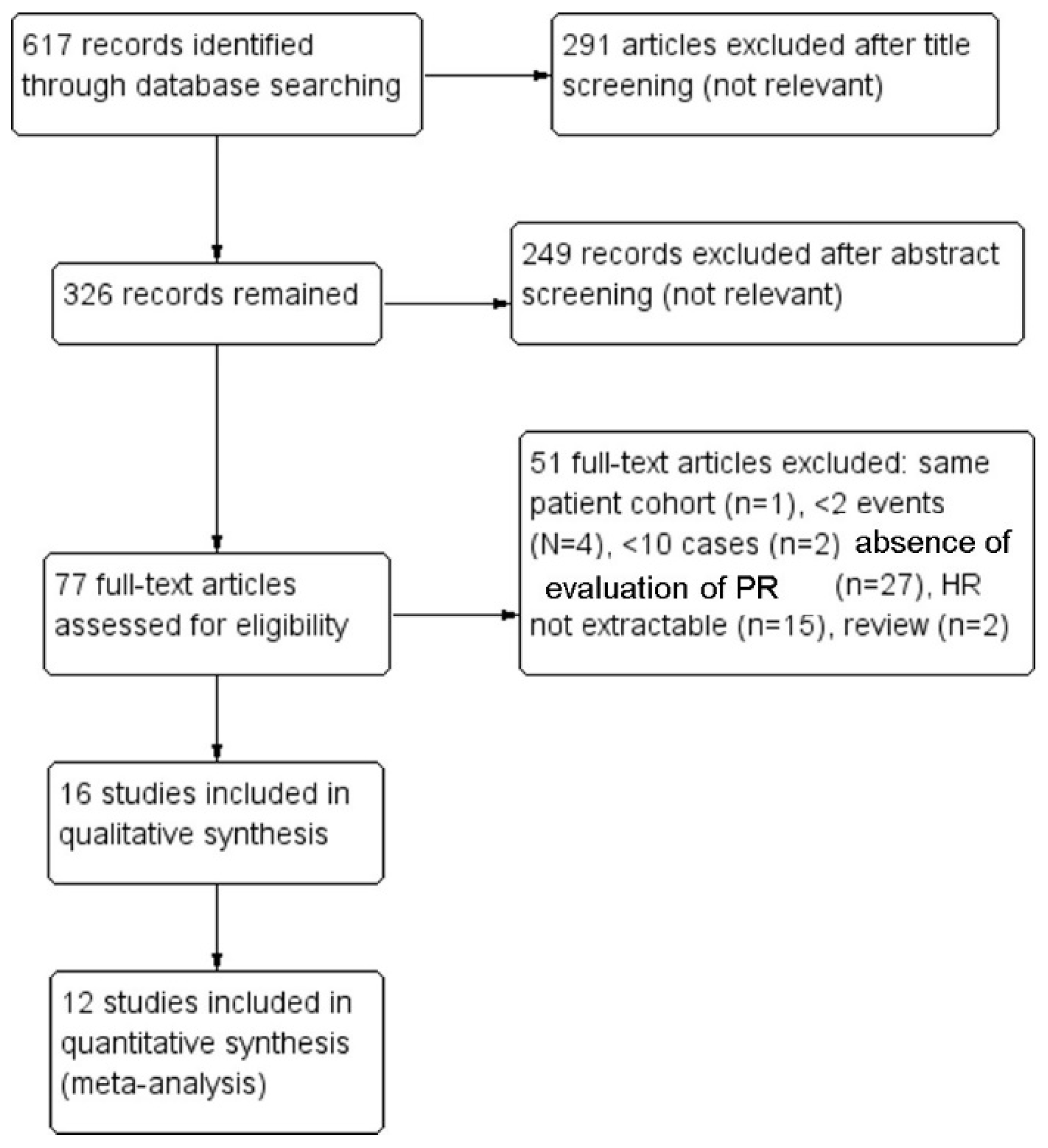
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- McCluggage, W.G.; Judge, M.J.; Alvarado-Cabrero, I.; Duggan, M.A.; Horn, L.C.; Hui, P.; Ordi, J.; Otis, C.N.; Park, K.J.; Plante, M.; et al. Data Set for the Reporting of Carcinomas of the Cervix: Recommendations From the International Collaboration on Cancer Reporting (ICCR). Int. J. Gynecol. Pathol. 2018, 37, 205–228. [Google Scholar] [CrossRef]
- Santoro, A.; Angelico, G.; Inzani, F.; Arciuolo, D.; Spadola, S.; Valente, M.; D’Alessandris, N.; Piermattei, A.; Fiorentino, V.; CIanfrini, F.; et al. Standard ultrastaging compared to one-step nucleic acid amplification (OSNA) for the detection of sentinel lymph node metastases in early stage cervical cancer. Int. J. Gynecol. Cancer. 2020, 30, 1871–1877. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynecol. Obstet. 2018, 143, 22–36. [Google Scholar]
- Santoro, A.; Angelico, G.; Piermattei, A.; Inzani, F.; Valente, M.; Arciuolo, D.; Spadola, S.; Mulè, A.; Zorzato, P.; Fagotti, A.; et al. Pathological Chemotherapy Response Score in Patients Affected by High Grade Serous Ovarian Carcinoma: The Prognostic Role of Omental and Ovarian Residual Disease. Front. Oncol. 2019, 9, 778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannoni, G.F.; Vellone, V.G.; Carbone, A. Morpphological effects of radiochemotherapy on cervical carcinoma: A morphological study of 50 cases of hysterectomy specimens after neoadjuvant treatment. Int. J. Gynecol. Pathol. 2008, 27, 274–281. [Google Scholar]
- Travaglino, A.; Raffone, A.; Mascolo, M.; Guida, M.; Insabato, L.; Zannoni, G.F.; Zullo, F. Clear cell endometrial carcinoma and the TCGA classification. Histopathology 2020, 76, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Raffone, A.; Travaglino, A.; Santoro, A.; Esposito, I.; Angelico, G.; Spadola, S.; Zannoni, G.F. Accuracy of One-Step Nucleic Acid Amplification in Detecting Lymph Node Metastases in Endometrial Cancer. Pathol. Oncol. Res. 2020, 26, 2049–2056. [Google Scholar] [PubMed]
- Travaglino, A.; Raffone, A.; Santoro, A.; Gencarelli, A.; Angelico, G.; Spadola, S.; Marzullo, L.; Zullo, F.; Insabato, L.; Zannoni, G.F. Prognostic significance of atypical mitotic figures in smooth muscle tumors of uncertain malignant potential (STUMP) of the uterus and uterine adnexa. APMIS 2021, 129, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travaglino, A.; Raffone, A.; Mollo, A.; Borrelli, G.; Alfano, P.; Zannoni, G.F.; Insabato, L.; Zullo, F. TCGA molecular subgroups and FIGO grade in endometrial endometrioid carcinoma. Arch. Gynecol. Obstet. 2020, 301, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Travaglino, A.; Raffone, A.; Gencarelli, A.; Mollo, A.; Guida, M.; Insabato, L.; Santoro, A.; Zannoni, G.F.; Zullo, F. TCGA Classification of Endometrial Cancer: The Place of Carcinosarcoma. Pathol. Oncol. Res. 2020, 26, 2067–2073. [Google Scholar] [CrossRef] [PubMed]
- Travaglino, A.; Raffone, A.; Mascolo, M.; Guida, M.; Insabato, L.; Zannoni, G.F.; Zullo, F. TCGA Molecular Subgroups in Endometrial Undifferentiated/Dedifferentiated Carcinoma. Pathol. Oncol. Res. 2020, 26, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Sato, T.; Watanabe, M.; Sasaki, M.; Tsuneki, I.; Tanaka, K. Neoadjuvant chemotherapy using low-dose consecutive intraarterial infusions of cisplatin combined with 5-fluorouracil for locally advanced cervical adenocarcinoma. Gynecol. Oncol. 2001, 81, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Obata, H.; Tabata, T.; Tanaka, K.; Toyoda, N.; Nishiura, K.; Yanoh, K.; Okugawa, T. A pilot study of neoadjuvant chemotherapy with mitomycin C, etoposide, cisplatin, and epirubicin for adenocarcinoma of the cervix. Int. J. Clin. Oncol. 2004, 9, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Buda, A.; Fossati, R.; Colombo, N.; Fei, F.; Floriani, I.; Alletti, D.G.; Katsaros, D.; Landoni, F.; Lissoni, A.; Malzoni, C.; et al. Randomized trial of neoadjuvant chemotherapy comparing paclitaxel, ifosfamide, and cisplatin with ifosfamide and cisplatin followed by radical surgery in patients with locally advanced squamous cell cervical carcinoma: The SNAP01 (Studio Neo-Adjuvante Portio) Italian Collaborative Study. J. Clin. Oncol. 2005, 23, 4137–4145. [Google Scholar] [PubMed]
- Candelaria, M.; Chanona-Vilchis, J.; Cetina, L.; Flores-Estrada, D.; López-Graniel, C.; González-Enciso, A.; Cantú, D.; Poitevin, A.; Rivera, L.; Hinojosa, J.; et al. Prognostic significance of pathological response after neoadjuvant chemotherapy or chemoradiation for locally advanced cervical carcinoma. Int. Semin. Surg. Oncol. 2006, 3, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadducci, A.; Sartori, E.; Maggino, T.; Zola, P.; Cosio, S.; Zizioli, V.; Lapresa, M.; Piovano, E.; Landoni, F. Pathological response on surgical samples is an independent prognostic variable for patients with Stage Ib2-IIb cervical cancer treated with neoadjuvant chemotherapy and radical hysterectomy: An Italian multicenter retrospective study (CTF Study). Gynecol. Oncol. 2013, 131, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Takatori, E.; Shoji, T.; Omi, H.; Kagabu, M.; Miura, F.; Takeuchi, S.; Kumagai, S.; Yoshizaki, A.; Sato, A.; Sugiyama, T. Analysis of prognostic factors for patients with bulky squamous cell carcinoma of the uterine cervix who underwent neoadjuvant chemotherapy followed by radical hysterectomy. Int. J. Clin. Oncol. 2015, 20, 345–350. [Google Scholar] [CrossRef]
- Buda, A.; Lissoni, A.A.; Floriani, I.; Biagioli, E.; Gerardi, C.; Bonazzi, C.; Chiari, S.; Locatelli, L.; Dell’Anna, T.; Signorelli, M.; et al. Long-Term Clinical Benefits of Neoadjuvant Chemotherapy in Women With Locally Advanced Cervical Cancer: Validity of Pathological Response as Surrogate Endpoint of Survival. Int. J. Gynecol. Cancer. 2015, 25, 1468–1475. [Google Scholar] [CrossRef]
- Liang, Y.; Lü, B.; Chen, X.; Qin, J.; Cheng, X.; Xie, X.; Lü, W. Prognostic value of pathological response to neoadjuvant chemotherapy in bulky stage Ib2 and IIa cervical squamous cell cancer patients. Virchows Arch. 2016, 468, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Sun, H.; Chen, Z.; Li, X.; Wang, S.; Zhao, X.; Tang, F.; Jia, Y.; Hu, T.; Du, X.; et al. Optimal pathological response indicated better long-term outcome among patients with stage IB2 to IIB cervical cancer submitted to neoadjuvant chemotherapy. Sci. Rep. 2016, 6, 28278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Wu, M.F.; Lu, H.W.; Zhang, B.Z.; Wang, L.J.; Lin, Z.Q. Impact of Hyperglycemia on Outcomes among Patients Receiving Neoadjuvant Chemotherapy for Bulky Early Stage Cervical Cancer. PLoS ONE 2016, 11, e0166612. [Google Scholar] [CrossRef]
- Siesto, G.; Romano, F.; Accardi, A.; Bulletti, C.; Iedà, N.P.; Vitobello, D. Robotic Surgery in Patients With Locally Advanced Cervical Cancer After Neoadjuvant Chemotherapy: Survival Outcomes. Int. J. Gynecol. Cancer. 2016, 26, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Ditto, A.; Martinelli, F.; Signorelli, M.; Chiappa, V.; Lopez, C.; Indini, A.; Maggiore, U.L.R.; Sabatucci, I.; Lorusso, D.; et al. Impact of Blood Transfusions on Survival of Locally Advanced Cervical Cancer Patients Undergoing Neoadjuvant Chemotherapy Plus Radical Surgery. Int. J. Gynecol. Cancer. 2017, 27, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Landoni, F.; Cosio, S.; Zizioli, V.; Zola, P.; Ferrero, A.; Lapresa, M.T.; Maggino, T.; Sartori, E. Neoadjuvant Platinum-based Chemotherapy Followed by Radical Hysterectomy for Stage Ib2-IIb Adenocarcinoma of the Uterine Cervix—An Italian Multicenter Retrospective Study. Anticancer Res. 2018, 38, 3627–3634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Lü, W.; Zhang, X.; Lü, B. Tumor-infiltrating CD8+ and FOXP3+ lymphocytes before and after neoadjuvant chemotherapy in cervical cancer. Diagn. Pathol. 2018, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Huang, K.; Tang, F.; Li, X.; Wang, X.; Long, S.; Zhou, S.; Zhang, J.; Ning, R.; Li, S.; et al. Adjuvant chemotherapy after surgery can improve clinical outcomes for patients with IB2-IIB cervical cancer with neoadjuvant chemotherapy followed by radical surgery. Sci. Rep. 2018, 8, 6443. [Google Scholar] [CrossRef] [Green Version]
- Wei, L.-C.; Li, X.; Zhang, Y.; Dang, Y.-Z.; Li, W.-W.; Li, J.-P.; Zhao, L.-N.; Liu, S.-J.; Li, X.; Shi, M. Individualized pelvic lymphadenectomy should follow neoadjuvant concurrent chemoradiotherapy for locally advanced cervical cancer. Medicine 2018, 97, e0331. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother Oncol. 2018, 127, 404–416. [Google Scholar] [CrossRef]
- de Maria, S.; Santoro, A.; Fuggetta, M.P.; Rocchetti, R.; Cottarelli, A.; Lanzilli, G.; Stiuso, P.; Angelico, G.; Spadola, S.; Franco Zannoni, G.; et al. A possible interplay between HR-HPV and stemness in tumor development: An in vivo investigation of CD133 as a putative marker of cancer stem cell in HPV18-infected KB cell line. APMIS 2020, 128, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Al-Mansour, Z.; Verschraegen, C. Locally advanced cervical cancer: What is the standard of care? Curr. Opin. Oncol. 2010, 22, 503–512. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Zhao, Q.; Geng, Y.N.; Yang, S.L.; Li, X.M.; Finas, D.; Yin, C.H.; Wu, Y.M. Analysis of short-term efficacy as defined by RECIST and pathological response of neoadjuvant chemotherapy comprised paclitaxel and cisplatin followed by radical surgery in patients with locally advanced cervical cancer: A prospective observational study. Medicine 2018, 97, e10913. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Wang, N.; Liu, Y.; Li, X.; Fan, L.; Li, M.; Wang, L.; Yu, Z.; Yan, Q.; Guo, Y.; et al. Tumor invasion depth is a useful pathologic assessment for predicting outcomes in cervical squamous cell carcinoma after neoadjuvant radiotherapy. Diagn. Pathol. 2015, 10, 200. [Google Scholar] [CrossRef] [Green Version]
- Khokher, S.; Qureshi, M.U.; Chaudhry, N.A. Comparison of WHO and RECIST criteria for evaluation of clinical response to chemotherapy in patients with advanced breast cancer. Asian Pac. J. Cancer Prev. 2012, 13, 3213–3218. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, H.; Okada, M.; Kaji, Y.; Satouchi, M.; Sato, Y.; Yamabe, Y.; Onaya, H.; Endo, M.; Sone, M.; Arai, Y. New response evaluation criteria in solid tumours-revised RECIST guideline (version 1.1). Gan Kagaku Ryoho. Cancer Chemother. 2009, 36, 2495–2501. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Institution | Period of Enrollment | Sample Size | Histotype | Stage | Evaluation of Pathological Response | Oncologic Outcome Assessed | Follow-up Duration, Mean/Median (Range) |
|---|---|---|---|---|---|---|---|---|---|
| Aoki 2001 [14] | Japan | Niigata University Hospital | 1993–1998 | 11 | AC | IB-III | proportion of viable cells (no vs. <1/3 vs. 1–2/3 vs. >2/3) | OS | 30 (1–65) m |
| Tabata 2004 [15] | Japan | Mie University | 1997–2002 | 14 | AC | IB-IIB | residual lesion size (no vs. <5 mm vs. >5 mm) * | OS | 47 (14–83) m |
| Buda 2005 [16] | Italy | 21 Italian centers | 1997–2000 | 219 | SCC | IB2-IVA | residual stromal invasion depth (<3 mm vs. >3 mm) | OS | 43 (31–56) m ** |
| Candelaria 2006 [17] | Mexico | Instituto Nacional de Cancerología | unclear | 178 | AC, SCC | IB2-IIIB | residual lesion size (no vs. <1 mm vs. >1 mm) * | OS | 30 (3–66) m |
| Gadducci 2013 [18] | Italy |
| 2002–2011 2009–2011 | 333 | AC, SCC | IB2-IIB | residual stromal invasion depth (<3 mm vs. >3 mm) | OS, PFS | 66 (8–212) m |
| Takatori 2015 [19] | Japan |
| 2002–2012 | 33 | SCC | IB2-IIB | proportion of viable cells (no vs. <1/3 vs. 1–2/3 vs. >2/3) * | OS | 34 (6–112) m |
| Buda 2015 [20] | Italy | San Gerardo Hospital of Monza | 1992–2011 | 446 | AC, SCC | IIB-IVA | residual stromal invasion depth (<3 mm vs. >3 mm) | OS | 152 (98–193)** |
| Liang 2015 [21] | China | Women’s Hospital, Zhejiang University | 2003–2012 | 204 | SCC | IB2-IIA | -proportion of viable cells -residual stromal invasion depth -residual lesion size | OS, PFS | 64 (26–128) m |
| Huang 2016 [22] | China | 8 Chinese centers | unclear | 853 (retrospective) 603 (prospective) | Any | IB2-IIB | residual stromal invasion depth (<3 mm vs. >3 mm) | PFS | unclear |
| Li 2016 [23] | China | Sun Yat-sen Memorial Hospital | 2005–2010 | 347 | AC, SCC | IB2-IIA | any residual lesion (no vs. yes) | OS, PFS | 37 (4–65) m |
| Siesto 2016 [24] | Italy | Humanitas Clinical and Research Center, Milan | 2009–2015 | 32 | AC, SCC | IB2-IIB | residual stromal invasion depth (<3 mm vs. >3 mm) | OS, PFS | 36 (5–71) m |
| Bogani 2017 [25] | Italy | National Cancer Institute, Milan | 1990–2011 | 275 | Any | IB2-IIB | residual stromal invasion depth (<3 mm vs. >3 mm) | OS, PFS | 48 (not reported) m |
| Gadducci 2018 [26] | Italy |
| 1992–2014 | 82 | AC | IB2-IIB | residual disease extent (intracervical vs. extracervical) | OS, PFS | 89 (5–208) m |
| Liang 2018 [27] | China | Women’s Hospital, Zhejiang University | 2007–2014 | 137 | SCC | IB2-IIA | residual stromal invasion depth (<3 mm vs. >3 mm) | OS, PFS | 51 (22–117) m |
| Sun 2018 [28] | China | Huazhong University of Science and Technology, Wuhan | 1999–2008 | 393 | SCC | IB2-IIB | residual stromal invasion depth (<3 mm vs. >3 mm) | OS, PFS | unclear |
| Wei 2018 [29] | China | The Fourth Military Medical University | 2009–2014 | 410 | AC, SCC | IB2-III | any residual lesion (no vs. yes) | OS | 51 (4–97) m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zannoni, G.F.; Travaglino, A.; Raffone, A.; Arciuolo, D.; D’Alessandris, N.; Scaglione, G.; Tralongo, P.; Inzani, F.; Angelico, G.; Santoro, A. Depth of Stromal Invasion as the Most Prognostically Relevant Regression System in Locally Advanced Cervical Cancer after Neoadjuvant Treatment: A Systematic Review and Meta-Analysis Grading. Diagnostics 2021, 11, 1772. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101772
Zannoni GF, Travaglino A, Raffone A, Arciuolo D, D’Alessandris N, Scaglione G, Tralongo P, Inzani F, Angelico G, Santoro A. Depth of Stromal Invasion as the Most Prognostically Relevant Regression System in Locally Advanced Cervical Cancer after Neoadjuvant Treatment: A Systematic Review and Meta-Analysis Grading. Diagnostics. 2021; 11(10):1772. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101772
Chicago/Turabian StyleZannoni, Gian Franco, Antonio Travaglino, Antonio Raffone, Damiano Arciuolo, Nicoletta D’Alessandris, Giulia Scaglione, Pietro Tralongo, Frediano Inzani, Giuseppe Angelico, and Angela Santoro. 2021. "Depth of Stromal Invasion as the Most Prognostically Relevant Regression System in Locally Advanced Cervical Cancer after Neoadjuvant Treatment: A Systematic Review and Meta-Analysis Grading" Diagnostics 11, no. 10: 1772. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101772