
The Assessment of Nipple Areola Complex Sensation with Semmes-Weinstein Monofilaments—Normative Values and Its Covariates


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. Study I
2.1.2. Study II
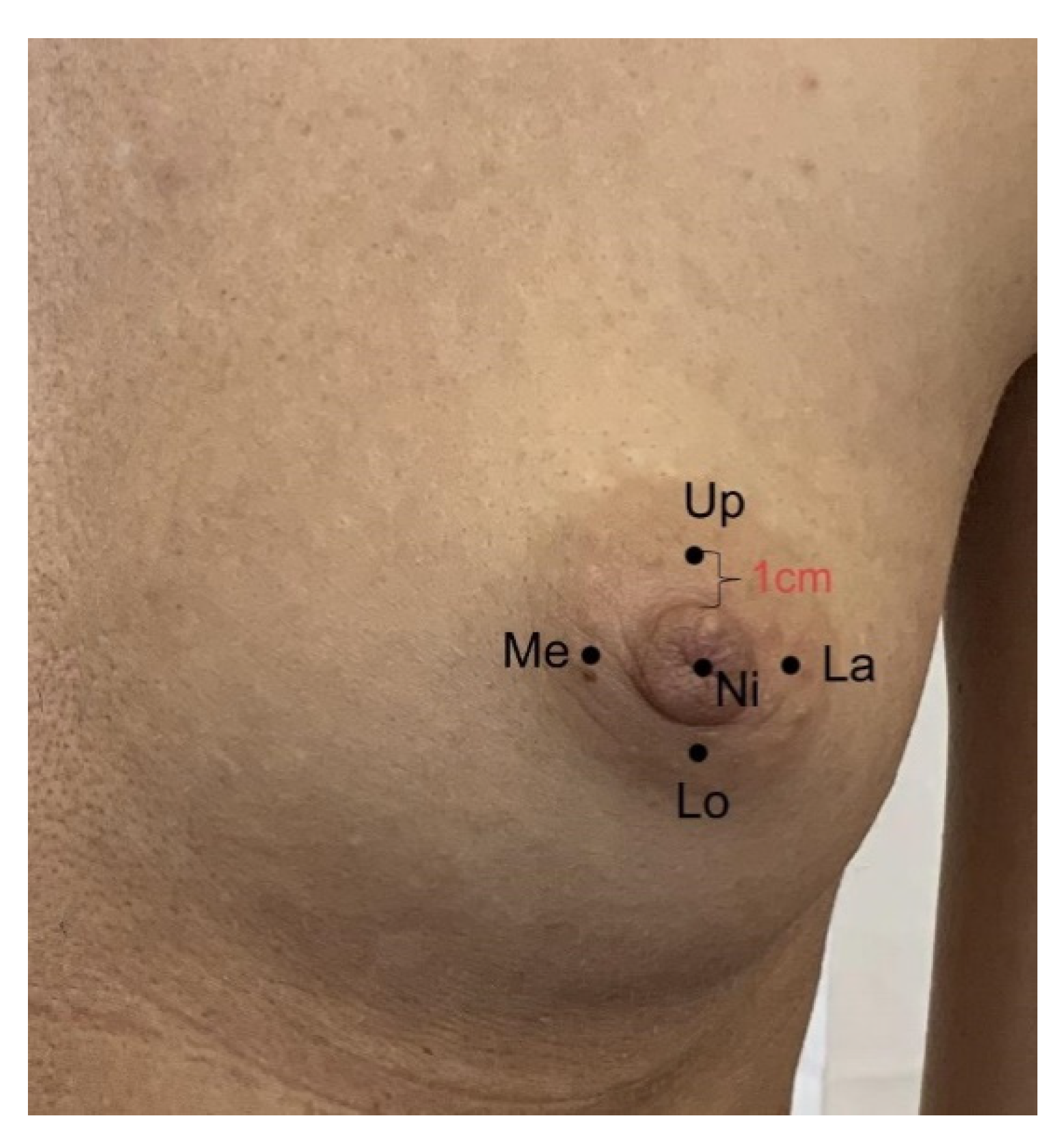
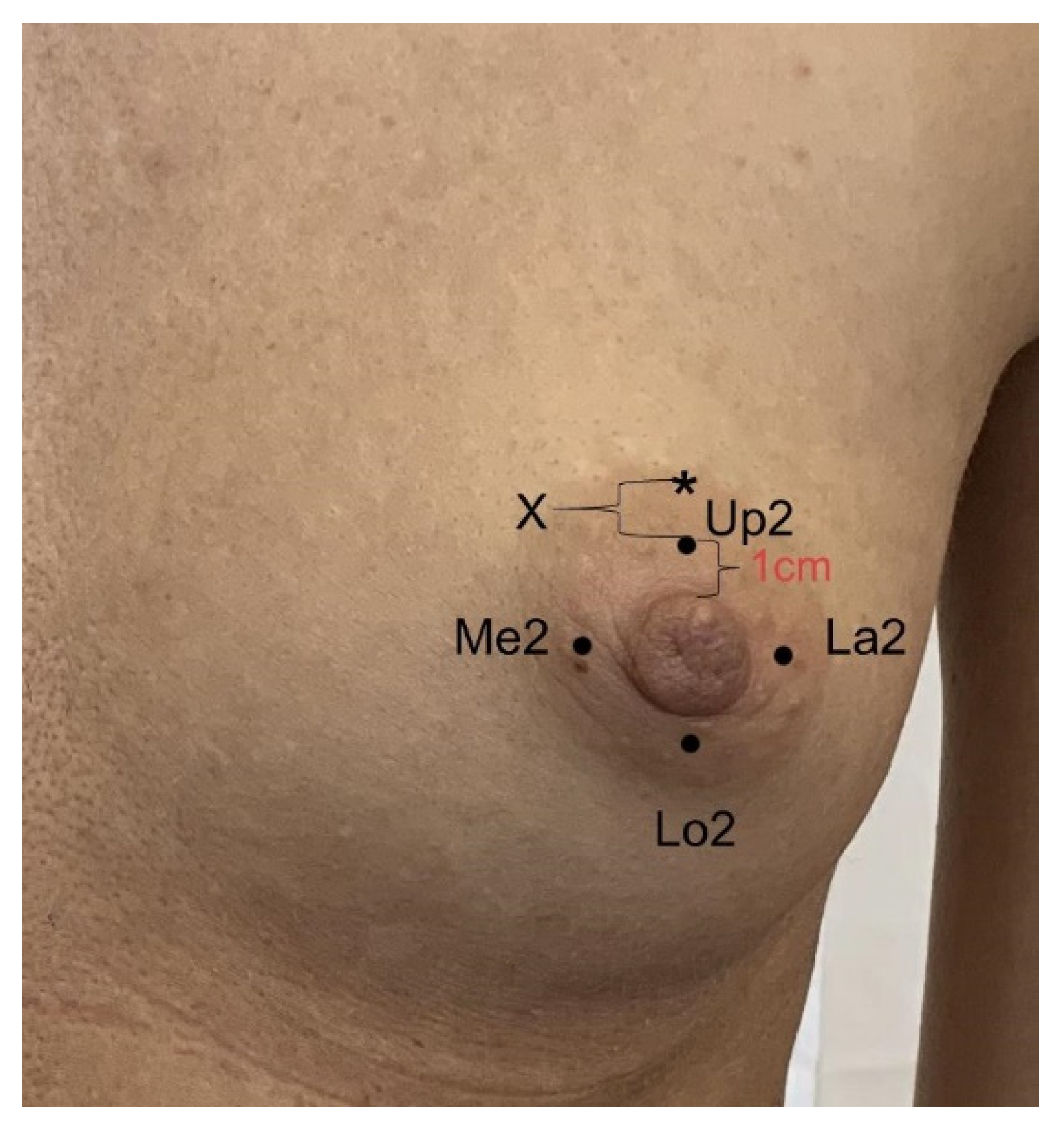
2.2. Anthropometric and Sensory Measurements with SWM and Weber TPD
2.3. Statistical Analysis
3. Results
3.1. Study I
3.1.1. Factors Affecting NAC Sensation
3.1.2. Multifactorial Model (Stepwise Logistic Regression Analysis) Identifying Risk Factors of Impaired Sensation (SWM Test ≥ 3.84)
3.2. Study II
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rochlin, D.; Brazio, P.; Wapnir, I.; Nguyen, D. Immediate Targeted Nipple–Areolar Complex Reinnervation. Plast. Reconstr. Surg. Glob. Open 2020, 8, 2719. [Google Scholar] [CrossRef] [PubMed]
- Chirappapha, P.; Srichan, P.; Lertsithichai, P.; Thaweepworadej, P.; Sukarayothin, T.; Leesombatpaiboon, M.; Kongdan, Y. Nipple-Areola Complex Sensation after Nipple-Sparing Mastectomy. Past. Reconstr. Surg. Glob. Open 2018, 6, 1716. [Google Scholar] [CrossRef] [PubMed]
- Temple, C.; Hurst, L. Reduction Mammaplasty Improves Breast Sensibility. Plast. Reconstr. Surg. 1999, 104, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, F.; Brown, F.; Gold, M.; Walton, R.; Shafer, B. Preoperative and Postoperative Nipple-Areola Sensibility in Patients Undergoing Reduction Mammaplasty. Plast. Reconstr. Surg. 1993, 92, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Slezak, S.; Dellon, A. Quantitation of Sensibility in Gigantomastia and Alteration Following Reduction Mammaplasty. Plast. Reconstr. Surg. 1993, 91, 1265–1269. [Google Scholar] [CrossRef]
- Wright, E.; Lee, G.; Boneti, C.; Vasconez, L.; De La Torre, J. Breast Reconstruction and Oncoplastic Surgery. In The Breast, 5th ed.; Elsevier: Oxford, UK, 2018; pp. 477–491. [Google Scholar]
- Tairych, G.; Kuzbari, R.; Rigel, S.; Todoroff, B.; Schneider, B.; Deutinger, M. Normal Cutaneous Sensibility of the Breast. Plast. Reconstr. Surg. 1998, 102, 701–704. [Google Scholar] [CrossRef]
- Zucca-Matthes, G.; Urban, C.; Vallejo, A. Anatomy of the nipple and breast ducts. Gland. Surg. 2016, 5, 32–36. [Google Scholar]
- Cornelissen, A.; Beugels, J.; van Kuijk, S.; Heuts, E.; Rozen, S.; Spiegel, A.; van der Hulst, R.; Tuinder, S. Sensation of the autologous reconstructed breast improves quality of life: A pilot study. Breast Cancer Res. Treat. 2017, 167, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Araco, A.; Araco, F.; Sorge, R.; Gravante, G. Sensitivity of the Nipple-Areola Complex and Areolar Pain Following Aesthetic Breast Augmentation in a Retrospective Series of 1200 Patients. Plast. Reconstr. Surg. 2011, 128, 984–989. [Google Scholar] [CrossRef]
- Mofid, M.; Klatsky, S.; Singh, N.; Nahabedian, M. Nipple-Areola Complex Sensitivity after Primary Breast Augmentation: A Comparison of Periareolar and Inframammary Incision Approaches. Plast. Reconstr. Surg. 2006, 117, 1694–1698. [Google Scholar] [CrossRef]
- Mofid, M.; Dellon, L.; Elias, J.; Nahabedian, M. Quantitation of Breast Sensibility Following Reduction Mammaplasty: A Comparison of Inferior and Medial Pedicle Techniques. Plast. Reconstr. Surg. 2002, 109, 2283–2288. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, O.A.; Kolhe, P.S. Comparison of nipple and areolar sensation after breast reduction by free nipple graft and inferior pedicle techniques. Br. J. Plast. Surg. 2000, 53, 126–129. [Google Scholar] [CrossRef]
- Hamdi, M.; Greuse, M.; DeMey, A.; Webster, M. A prospective quantitative comparison of breast sensation after superior and inferior pedicle mammaplasty. Br. J. Plast. Surg. 2001, 54, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.; Kania, K.; Spiegel, A. Post-mastectomy sensory recovery and restoration. Gland. Surg. 2021, 10, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Godwin, Y.; Valassiadou, K.; Lewis, S.; Denley, H. Investigation into the Possible Cause of Subjective Decreased Sensory Perception in the Nipple-Areola Complex of Women with Macromastia. Plast. Reconstr. Surg. 2004, 113, 1598–1606. [Google Scholar] [CrossRef]
- Garcia, E.; Veiga, D.; Sabino-Neto, M.; Beraldo Cardoso, F.; Batista, I.; Leme, R.; Cabral, I.; Novo, N.; Ferreira, L. Sensitivity of the Nipple-Areola Complex and Sexual Function Following Reduction Mammaplasty. Aesthetic Surg. J. 2015, 35, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlenz, I.; Rigel, S.; Schemper, M.; Kuzbari, R. Alteration of Nipple and Areola Sensitivity by Reduction Mammaplasty: A Prospective Comparison of Five Techniques. Plast. Reconstr. Surg. 2005, 115, 743–751. [Google Scholar] [CrossRef]
- Chiummariello, S.; Angelisanti, M.; Arleo, S.; Alfano, C. Evaluation of the sensitivity after reduction mammoplasty. Our experience and review of the literature. Ann. Ital. Di Chir. 2013, 84, 385–388. [Google Scholar]
- Shridharani, S.; Magarakis, M.; Stapleton, S.; Basdag, B.; Seal, S.; Rosson, G. Breast Sensation after Breast Reconstruction: A Systematic Review. J. Reconstr. Microsurg. 2010, 26, 303–310. [Google Scholar] [CrossRef]
- Robinson, J.; Short, R. Changes in breast sensitivity at puberty, during the menstrual cycle, and at parturition. BMJ 1977, 1, 1188–1191. [Google Scholar] [CrossRef] [Green Version]
- Critchley, H.; Maybin, J.; Armstrong, G.; Williams, A. Physiology of the Endometrium and Regulation of Menstruation. Physiol. Rev. 2020, 100, 1149–1179. [Google Scholar] [CrossRef]
- Ader, D.; Shriver, C.; Browne, M. Cyclical Mastalgia: Premenstrual Syndrome or Recurrent Pain Disorder? J. Psychosom. Obstet. Gynecol. 1999, 20, 198–202. [Google Scholar] [CrossRef]
- Boyle, C.; Berkowitz, G.; Kelsey, J. Epidemiology of premenstrual symptoms. Am. J. Public Health 1987, 77, 349–350. [Google Scholar] [CrossRef]
- Suda, M.; Kawakami, M.; Okuyama, K.; Ishii, R.; Oshima, O.; Hijikata, N.; Nakamura, T.; Oka, A.; Kondo, K.; Liu, M. Validity and Reliability of the Semmes-Weinstein Monofilament Test and the Thumb Localizing Test in Patients with Stroke. Front. Neurol. 2021, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.; Lavery, D.; Lavery, D.; LaFontaine, J.; Bharara, M.; Najafi, B. Accuracy and Durability of Semmes-Weinstein Monofilaments: What is the Useful Service Life? Diabetes Res. Clin. Pract. 2012, 97, 399–404. [Google Scholar] [CrossRef]
- Yong, R.; Karas, T.; Smith, K.; Petrov, O. The Durability of the Semmes-Weinstein 5.07 Monofilament. J. Foot Ankle Surg. 2000, 39, 34–38. [Google Scholar] [CrossRef]
- Longo, B.; Timmermans, F.W.; Farcomeni, A.; Frattaroli, J.M.; D’orsi, G.; Atzeni, M.; Sorotos, M.; Laporta, R.; Santanelli di Pompeo, F. Septum-Based Mammaplasties: Surgical Techniques and Evaluation of Nipple-Areola Sensibility. Aesthetic Plast. Surg. 2020, 44, 689–697. [Google Scholar] [CrossRef]
- Jerosch-Herold, C. Assessment of Sensibility after Nerve Injury and Repair: A Systematic Review of Evidence for Validity, Reliability and Responsiveness of Tests. J. Hand Surg. 2005, 30, 252–264. [Google Scholar] [CrossRef]
- Mayfield, J.; Sugarman, J. The use of the Semmes-Weinstein monofilament and other threshold tests for preventing foot ulceration and amputation in persons with diabetes. J. Fam. Pract. 2000, 49, 17–29. [Google Scholar]
- Kuzbari, R.; Schlenz, I. Reduction Mammaplasty and Sensitivity of the Nipple-Areola Complex. Ann. Plast. Surg. 2007, 58, 3–11. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Normal-Sized Breasts n = 270 | Hypertrophic Breasts n = 50 | Normal vs. Hypertrophic | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | Quartiles | Mean | SD | Chi/p | Median | Quartiles | Mean | SD | Chi/p | p ** | |
| SWMT | 79.96 p < 0.0001 | SWMT | 47.81 p < 0.0001 | ||||||||
| nipple | 3.22 | 2.83; 3.61 | 3.03 | 0.59 | 3.22 | 2.83; 3.61 | 3.24 | 0.42 | 0.013 | ||
| upper | 3.61 | 2.83; 3.84 | 3.23 | 0.77 | 3.61 | 3.22; 4.08 | 3.55 | 0.46 | 0.027 | ||
| medial | 3.22 | 2.83; 3.84 | 3.26 | 0.74 | 3.61 | 3.22; 4.08 | 3.55 | 0.45 | 0.038 | ||
| lower | 3.22 | 2.44; 3.84 | 3.21 | 0.82 | 3.61 | 3.22; 4.08 | 3.67 | 0.47 | 0.001 | ||
| lateral | 3.22 | 2.44; 3.84 | 3.19 | 0.82 | 3.61 | 3.22; 4.08 | 3.61 | 0.47 | 0.003 | ||
| Mean * | 3.22 | 2.75; 3.69 | 3.18 | 0.60 | 3.56 | 3.3; 3.77 | 3.52 | 0.36 | 0.0003 | ||
| 2PDT | 4.95 p = 0.176 | 2PDT | 1.20 p = 0.753 | ||||||||
| upper | 15 | 13; 15 | 13.66 | 2.39 | 15 | 12; 15 | 13.32 | 2.54 | 0.357 | ||
| medial | 15 | 13; 15 | 13.67 | 2.42 | 15 | 12; 15 | 13.32 | 2.83 | 0.931 | ||
| lower | 15 | 14; 15 | 13.80 | 2.20 | 15 | 12; 15 | 13.26 | 2.82 | 0.39 | ||
| lateral | 15 | 13; 15 | 13.71 | 2.30 | 15 | 12; 15 | 13.26 | 2.98 | 0.829 | ||
| Mean * | 14.75 | 13.75; 15 | 13.71 | 2.14 | 14.75 | 12.75; 15 | 13.29 | 2.62 | 0.441 | ||
| Normal-Sized Breasts n = 270 | Nipple | Upper | Medial | Lower | Lateral | Mean * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R ** | p | R | p | R | p | R | p | R | p | R | p | |
| age | 0.30 | <0.0001 | 0.25 | <0.0001 | 0.22 | 0.0003 | 0.16 | 0.008 | 0.24 | <0.0001 | 0.28 | <0.0001 |
| BMI | 0.22 | 0.0002 | 0.32 | <0.0001 | 0.35 | <0.0001 | 0.30 | <0.0001 | 0.39 | <0.0001 | 0.39 | <0.0001 |
| births | 0.25 | <0.0001 | 0.18 | 0.003 | 0.14 | 0.0182 | 0.06 | 0.306 | 0.13 | 0.03 | 0.18 | 0.003 |
| breastfeeding | 0.24 | <0.0001 | 0.16 | 0.009 | 0.10 | 0.091 | 0.03 | 0.655 | 0.11 | 0.083 | 0.14 | 0.02 |
| cup size | 0.23 | 0.0001 | 0.34 | <0.0001 | 0.42 | <0.0001 | 0.37 | <0.0001 | 0.41 | <0.0001 | 0.45 | <0.0001 |
| sn-n | 0.25 | <0.0001 | 0.43 | <0.0001 | 0.47 | <0.0001 | 0.42 | <0.0001 | 0.44 | <0.0001 | 0.49 | <0.0001 |
| areola diameter | 0.09 | 0.153 | 0.40 | <0.0001 | 0.41 | <0.0001 | 0.37 | <0.0001 | 0.34 | <0.0001 | 0.39 | <0.0001 |
| Normal-Sized Breasts n = 270 | Oral Contraception = 36 | No Oral Contraception n = 234 | p ** | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | Quartiles | Mean | SD | Median | Quartiles | Mean | SD | ||
| nipple | 2.83 | 2.44; 3.22 | 2.92 | 0.64 | 3.22 | 2.83; 3.61 | 3.05 | 0.59 | 0.176 |
| upper | 3.22 | 2.635; 3.84 | 3.13 | 0.80 | 3.61 | 2.83; 3.84 | 3.25 | 0.77 | 0.401 |
| medial | 3.22 | 2.635; 3.725 | 3.17 | 0.77 | 3.22 | 2.83; 3.84 | 3.27 | 0.74 | 0.482 |
| lower | 3.22 | 2.44; 3.61 | 3.01 | 0.83 | 3.61 | 2.44; 3.84 | 3.24 | 0.82 | 0.109 |
| lateral | 2.44 | 2.36; 3.61 | 2.92 | 0.88 | 3.61 | 2.44; 3.84 | 3.23 | 0.80 | 0.047 |
| mean * | 3.04 | 2.594; 3.478 | 3.03 | 0.56 | 3.29 | 2.814; 3.702 | 3.21 | 0.61 | 0.069 |
| Normal-Sized Breasts n = 270 | R * | t | p |
|---|---|---|---|
| age | 0.29 | 5.02 | <0.0001 |
| BMI | 0.24 | 3.96 | <0.0001 |
| births | 0.30 | 5.21 | <0.0001 |
| breastfeeding | 0.32 | 5.55 | <0.0001 |
| cup size | 0.05 | 0.77 | 0.443 |
| sn-n | 0.23 | 3.87 | 0.0001 |
| areola diameter | 0.28 | 4.82 | <0.0001 |
| Cycle phase | Mean (SD) | H | p ** |
| follicular | 13.59 (2.26) | 10.66 | 0.014 |
| ovulation | 13.83 (2.35) | ||
| luteal | 13.64 (2.12) | ||
| menopause | 14.82 (0.60) |
| n = 270 | OR | 95% CI | Wald Chi-Square | p |
|---|---|---|---|---|
| age | 1.05 | 1.02; 1.09 | 8.03 | 0.005 |
| size | 1.78 | 1.21; 2.62 | 8.56 | 0.003 |
| sn-n | 1.2 | 1.06; 1.36 | 8.81 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasielska-Trojan, A.; Szulia, A.; Zawadzki, T.; Antoszewski, B. The Assessment of Nipple Areola Complex Sensation with Semmes-Weinstein Monofilaments—Normative Values and Its Covariates. Diagnostics 2021, 11, 2145. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112145
Kasielska-Trojan A, Szulia A, Zawadzki T, Antoszewski B. The Assessment of Nipple Areola Complex Sensation with Semmes-Weinstein Monofilaments—Normative Values and Its Covariates. Diagnostics. 2021; 11(11):2145. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112145
Chicago/Turabian StyleKasielska-Trojan, Anna, Agata Szulia, Tomasz Zawadzki, and Bogusław Antoszewski. 2021. "The Assessment of Nipple Areola Complex Sensation with Semmes-Weinstein Monofilaments—Normative Values and Its Covariates" Diagnostics 11, no. 11: 2145. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112145