
Primary Psychosis: Risk and Protective Factors and Early Detection of the Onset

 ,
,
Abstract
:1. Introduction
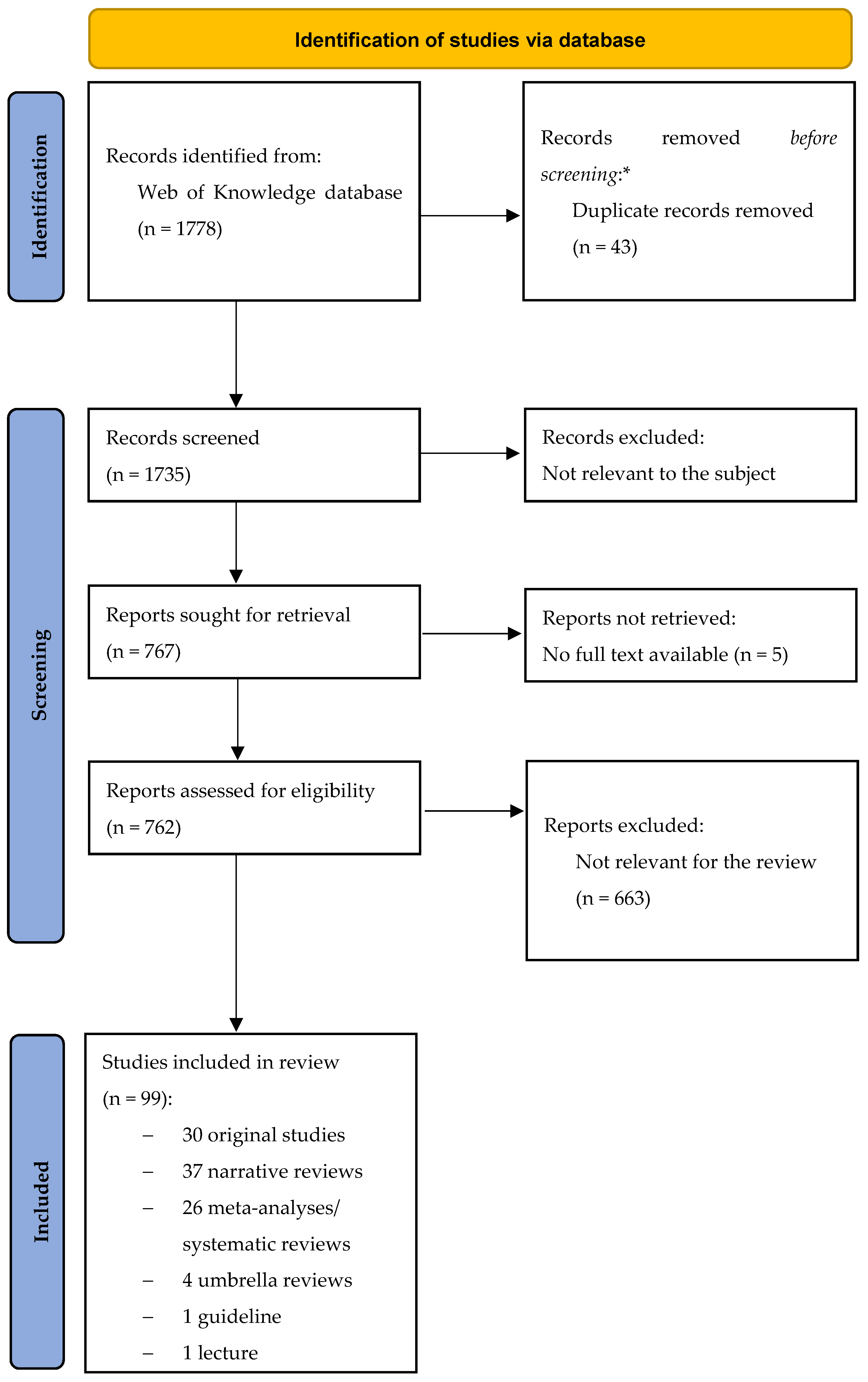
2. Methods
- (i)
- they were very recent and were not cited in second literature publications;
- (ii)
- They discussed topics never included into second literature works, mainly regarding protective factors or preventive programs that have a less wide literature.
3. Results
3.1. Risk Factors for Primary Psychosis
3.1.1. Individual Risk Factors
Familiar and Parental Risk Factors
Sociodemographic Risk Factors
Personal Pre-Morbid Characteristics Associated with a Higher Risk of Developing Primary Psychosis
Comorbidities Associated with a Higher Risk of Developing Primary Psychosis
Genetic Factors Associated with a Higher Risk of Developing Primary Psychosis
3.1.2. Environmental Risk Factors
Prenatal and Perinatal Risk Factors
Childhood-Related Environmental Risk Factors
Adolescence-Related Environmental Risk Factors
Continuous Risk Factors and Factors That Can Play a Role at Any Time in Life
3.2. Protective Factors for Primary Psychosis
3.2.1. Individual Protective Factors
Parental, Socio-Demographic, and Personal Protective Factors
Autoimmune Comorbidities Associated with a Reduced Risk of Developing Primary Psychosis
3.2.2. Environmental Protective Factors
Prenatal Protective Factors
Childhood and Adolescence-Related Environmental Protective Factors
3.3. Early Detection of the Onset
3.3.1. Help Seekers and Populations at Risk of Developing Primary Psychosis
3.3.2. Screening Tools for Stratification of the Risk of Developing Primary Psychosis
3.3.3. Models and Levels of Preventive Interventions and their Limitation
3.3.4. Integrated Model of Prevention and Early Detection of the Onset in Primary Psychosis
- (i)
- a first part, the ERIraos-Check List, which is used for screening purposes, contains questions on generic and psychotic psychiatric symptoms, on global functioning, with importance given to self-perception of functioning, and on the evaluation of some well-known risk factors for primary psychosis such as obstetric complications, neurodevelopment delays or alterations, family history, and substance abuse;
- (ii)
- a second part, the ERIraos-Symptom List, which is administered to people evaluated at least at modest risk of transition to psychosis in the ERIraos-Check List. This second-level evaluation is carried out in specialized centers and aims to carefully detect imminent transition [115]. Thereafter, the ERIraos has been successfully employed as a tool for the early recognition of psychosis risk in several further German studies [116,117,118] and subsequently translated and validated into different languages and populations [115,119]. This instrument proved to be suitable for routine use as a scale for the identification of the at-risk subjects.
- (i)
- subjects at early (pre-psychotic) prodromal stage and
- (ii)
- subjects at late (early psychotic) prodromal stage.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Maj, M.; van Os, J.; De Hert, M.; Gaebel, W.; Galderisi, S.; Green, M.F.; Guloksuz, S.; Harvey, P.D.; Jones, P.B.; Malaspina, D.; et al. The clinical characterization of the patient with primary psychosis aimed at personalization of management. World Psychiatry 2021, 20, 4–33. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Psychiatric Organization: Geneva, Switzerland, 2019; Available online: https://icd.who.int/ (accessed on 26 August 2021).
- Perälä, J.; Suvisaari, J.; Saarni, S.I.; Kuoppasalmi, K.; Isometsä, E.; Pirkola, S.; Partonen, T.; Tuulio-Henriksson, A.; Hintikka, J.; Kieseppä, T.; et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch. Gen. Psychiatry 2007, 64, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease 2017, Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- van Os, J.; Reininghaus, U. The clinical epidemiology of schizophrenia. In Kaplan & Sadock’s Comprehensive Textbook of Psychiatry, 10th ed.; Kaplan, B., Sadock, B.J., Sadock, V.A., Ruiz, P., Eds.; Lippincott Williams & Wilkins: London, UK, 2017. [Google Scholar]
- Sartorius, N.; Shapiro, R.; Kimura, M.; Barrett, K. WHO International Pilot Study of Schizophrenia. Psychol. Med. 1972, 2, 422–425. [Google Scholar] [CrossRef] [Green Version]
- Howes, O.D.; Whitehurst, T.; Shatalina, E.; Townsend, L.; Onwordi, E.C.; Mak, T.L.A.; Arumuham, A.; O’Brien, O.; Lobo, M.; Vano, L.; et al. The clinical significance of duration of untreated psychosis: An umbrella review and random-effects meta-analysis. World Psychiatry 2021, 20, 75–95. [Google Scholar] [CrossRef]
- Marshall, M.; Lewis, S.; Lockwood, A.; Drake, R.; Jones, P.; Croudace, T. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: A systematic review. Arch. Gen. Psychiatry 2005, 62, 975–983. [Google Scholar] [CrossRef] [Green Version]
- Perkins, D.O.; Gu, H.; Boteva, K.; Lieberman, J.A. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: A critical review and meta-analysis. Am. J. Psychiatry 2005, 162, 1785–1804. [Google Scholar] [CrossRef]
- Altamura, A.C.; Serati, M.; Buoli, M. Is duration of illness really influencing outcome in major psychoses? Nord. J. Psychiatry 2015, 69, 1685–1699. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, A.; Denovan-Wright, E.M.; Uher, R. Gene–environment interplay in the etiology of psychosis. Psychol. Med. 2018, 48, 1925–1936. [Google Scholar] [CrossRef]
- Porta, M. A Dictionary of Epidemiology; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Radua, J.; Ramella-Cravaro, V.; Ioannidis, J.P.A.; Reichenberg, A.; Phiphopthatsanee, N.; Amir, T.; Yenn Thoo, H.; Oliver, D.; Davies, C.; Morgan, C.; et al. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry 2018, 17, 49–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althwanay, A.; Alzamil, N.A.; Almukhadhib, O.Y.; Alkhunaizi, S.; Althwanay, R. Risks and Protective Factors of the Prodromal Stage of Psychosis: A Literature Review. Cureus 2020, 12, e8639. [Google Scholar] [CrossRef]
- Zamanpoor, M. Schizophrenia in a genomic era: A review from the pathogenesis, genetic and environmental etiology to diagnosis and treatment insights. Psychiatr. Genet. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- DeRosse, P.; Malhotra, A.K.; Lencz, T. Molecular genetics of the psychosis phenotype. Can. J. Psychiatry 2012, 57, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, M.G.; Nordgaard, J.; Jansson, L.B. Genetics of schizophrenia: Overview of methods, findings and limitations. Front. Hum. Neurosci. 2017, 11, 322. [Google Scholar] [CrossRef] [Green Version]
- Tandon, R.; Keshavan, M.S.; Nasrallah, H.A. Schizophrenia, “just the facts” what we know in 2008. 2. Epidemiology and etiology. Schizophr. Res. 2008, 102, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Rasic, D.; Hajek, T.; Alda, M.; Uher, R. Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: A meta-analysis of family high-risk studies. Schizophr. Bull. 2014, 40, 28–38. [Google Scholar] [CrossRef] [Green Version]
- Giegling, I.; Hosak, L.; Mössner, R.; Serretti, A.; Bellivier, F.; Claes, S.; Collier, D.A.; Corrales, A.; DeLisi, L.E.; Gallo, C.; et al. Genetics of schizophrenia: A consensus paper of the WFSBP task force on genetics. World J. Biol. Psychiatry 2017, 18, 492–505. [Google Scholar] [CrossRef]
- Davies, C.; Segre, G.; Estradé, A.; Radua, J.; De Micheli, A.; Provenzani, U.; Oliver, D.; Salazar de Pablo, G.; Ramella-Cravaro, V.; Besozzi, M.; et al. Prenatal and perinatal risk and protective factors for psychosis: A systematic review and meta-analysis. Lancet Psychiatry 2020, 7, 399–410. [Google Scholar] [CrossRef]
- Arango, C.; Dragioti, E.; Solmi, M.; Cortese, S.; Domschke, K.; Murray, R.M.; Jones, P.B.; Uher, R.; Carvalho, A.F.; Reichenberg, A.; et al. Risk and protective factors for mental disorders beyond genetics: An evidence-based atlas. World Psychiatry 2021, 20, 417–436. [Google Scholar] [CrossRef]
- Cantor-Graae, E.; Selten, J.P. Schizophrenia and migration: A meta-analysis and review. Am. J. Psychiatry 2005, 162, 12–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fett, A.J.; Lemmers-Jansen, I.L.J.; Krabbendam, L. Psychosis and urbanicity: A review of the recent literature from epidemiology to neurourbanism. Curr. Opin. Psychiatry 2019, 32, 232–241. [Google Scholar] [CrossRef]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.J.; Hayes, J.F. Air Pollution (Particulate Matter) Exposure and Associations with Depression, Anxiety, Bipolar, Psychosis and Suicide Risk: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandaker, G.M.; Barnett, J.H.; White, I.R.; Jones, P.B. A quantitative meta-analysis of population-based studies of premorbid intelligence and schizophrenia. Schizophr. Res. 2011, 132, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeppesen, R.; Benros, M.E. Autoimmune Diseases and Psychotic Disorders. Front. Psychiatry 2019, 10, 131. [Google Scholar] [CrossRef] [Green Version]
- Cullen, A.E.; Holmes, S.; Pollak, T.A.; Blackman, G.; Joyce, D.W.; Kempton, M.J.; Murray, R.M.; McGuire, P.; Mondelli, V. Associations Between Non-neurological Autoimmune Disorders and Psychosis: A Meta-analysis. Biol. Psychiatry 2019, 85, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Giannitelli, M.; Consoli, A.; Raffin, M.; Jardri, R.; Levinson, D.F.; Cohen, D.; Laurent-Levinson, C. An overview of medical risk factors for childhood psychosis: Implications for research and treatment. Schizophr. Res. 2018, 192, 39–49. [Google Scholar] [CrossRef]
- Malaspina, D.; Walsh-Messinger, J.; Brunner, A.; Rahman, N.; Corcoran, C.; Kimhy, D.; Goetz, R.R.; Goldman, S.B. Features of schizophrenia following premorbid eating disorders. Psychiatry Res. 2019, 278, 275–280. [Google Scholar] [CrossRef]
- Sharma, L.P.; Reddy, Y.C.J. Obsessive-compulsive disorder comorbid with schizophrenia and bipolar disorder. Indian J. Psychiatry 2019, 61 (Suppl. 1), S140–S148. [Google Scholar] [CrossRef]
- Balaratnasingam, S.; Janca, A. Normal personality, personality disorder and psychosis: Current views and future perspectives. Curr. Opin. Psychiatry 2015, 28, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Tarbox, S.I.; Pogue-Geile, M.F. A multivariate perspective on schizotypy and familial association with schizophrenia: A review. Clin. Psychol. Rev. 2011, 31, 1169–1182. [Google Scholar] [CrossRef] [Green Version]
- Nelson, M.T.; Seal, M.L.; Pantelis, C.; Phillips, L.J. Evidence of a dimensional relationship between schizotypy and schizophrenia: A systematic review. Neurosci. Biobehav. Rev. 2013, 37, 317–327. [Google Scholar] [CrossRef]
- Barrantes-Vidal, N.; Grant, P.; Kwapil, T.R. The role of schizotypy in the study of the etiology of schizophrenia spectrum disorders. Schizophr. Bull. 2015, 41 (Suppl. 2), S408–S416. [Google Scholar] [CrossRef]
- Schizophrenia Working Group of the Psychiatric Genomics Consortium. Biological insights from 108 schizophrenia-associated genetic loci. Nature 2014, 511, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergen, S.E.; Ploner, A.; Howrigan, D.; O’Donovan, M.C.; Smoller, J.W.; Sullivan, P.F.; Sebat, J.; Neale, B.; Kendler, K.S. Joint contributions of rare copy number variants and common SNPs to risk for schizophrenia. Am. J. Psychiatry 2018, 176, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Sønderby, I.E.; Ching, C.R.K.; Thomopoulo, S.I.; van der Meer, D.; Sun, D.; Villalon-Reina, J.E.; Agartz, I.; Amunts, K.; Arango, C.; Armstrong, N.J.; et al. Effects of copy number variations on brain structure and risk for psychiatric illness: Large-scale studies from the ENIGMA working groups on CNVs. Hum. Brain Mapp. 2021. [Google Scholar] [CrossRef]
- Jalbrzikowski, M. Neuroimaging Phenotypes Associated With Risk and Resilience for Psychosis and Autism Spectrum Disorders in 22q11.2 Microdeletion Syndrome. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 211–224. [Google Scholar] [CrossRef]
- Fernandez, A.; Drozd, M.M.; Thümmler, S.; Dor, E.; Capovilla, M.; Askenazy, F.; Bardoni, B. Childhood-Onset Schizophrenia: A Systematic Overview of Its Genetic Heterogeneity From Classical Studies to the Genomic Era. Front. Genet. 2019, 10, 1137. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, M.L.; Herrera, L.; Gaspar, P.A.; Nieto, R.; Maturana, A.; Villar, M.J.; Salinas, V.; Silva, H. Shifting the focus toward rare variants in schizophrenia to close the gap from genotype to phenotype. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2017, 174, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S. Beyond the dopamine hypothesis of schizophrenia to three neural networks of psychosis: Dopamine, serotonin, and glutamate. CNS Spectr. 2018, 23, 187–191. [Google Scholar] [CrossRef]
- Xu, F.L.; Ding, M.; Wu, X.; Liu, Y.P.; Xia, X.; Yao, J.; Wang, B.J. A Meta-analysis of the Association Between SLC6A3 Gene Polymorphisms and Schizophrenia. J. Mol. Neurosci. 2020, 70, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Howell, K.R.; Law, A.J. Neurodevelopmental concepts of schizophrenia in the genome-wide association era: AKT/mTOR signaling as a pathological mediator of genetic and environmental programming during development. Schizophr. Res. 2020, 217, 95–104. [Google Scholar] [CrossRef]
- GeneCards®. Available online: https://www.genecards.org/ (accessed on 14 September 2021).
- Saatci, D.; van Nieuwenhuizen, A.; Handunnetthi, L. Maternal infection in gestation increases the risk of non-affective psychosis in offspring: A meta-analysis. J. Psychiatr. Res. 2021, 139, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Ursini, G.; Punzi, G.; Chen, Q.; Marenco, S.; Robinson, J.F.; Porcelli, A.; Hamilton, E.G.; Mitjans, M.; Maddalena, G.; Begemann, M.; et al. Convergence of placenta biology and genetic risk for schizophrenia. Nat. Med. 2018, 24, 792–801. [Google Scholar] [CrossRef]
- Barron, H.; Hafizi, S.; Andreazza, A.C.; Mizrahi, R. Neuroinflammation and Oxidative Stress in Psychosis and Psychosis Risk. Int. J. Mol. Sci. 2017, 18, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setién-Suero, E.; Suárez-Pinilla, P.; Ferro, A.; Tabarés-Seisdedos, R.; Crespo-Facorro, B.; Ayesa-Arriola, R. Childhood trauma and substance use underlying psychosis: A systematic review. Eur. J. Psychotraumatol. 2020, 11, 1748342. [Google Scholar] [CrossRef]
- Varese, F.; Smeets, F.; Drukker, M.; Lieverse, R.; Lataster, T.; Viechtbauer, W.; Read, J.; van Os, J.; Bentall, R.P. Childhood adversities increase the risk of psychosis: A meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr. Bull. 2012, 38, 661–671. [Google Scholar] [CrossRef]
- Pastore, A.; de Girolamo, G.; Tafuri, S.; Tomasicchio, A.; Margari, F. Traumatic experiences in childhood and adolescence: A meta-analysis of prospective studies assessing risk for psychosis. Eur. Child. Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Hailes, H.P.; Yu, R.; Danese, A.; Fazel, S. Long-term outcomes of childhood sexual abuse: An umbrella review. Lancet Psychiatry 2019, 6, 830–839. [Google Scholar] [CrossRef] [Green Version]
- Ayerbe, L.; Pérez-Piñar, M.; Foguet-Boreu, Q.; Ayis, S. Psychosis in children of separated parents: A systematic review and meta-analysis. Eur. Psychiatry 2020, 63, e3. [Google Scholar] [CrossRef] [Green Version]
- Sideli, L.; Murray, R.M.; Schimmenti, A.; Corso, M.; La Barbera, D.; Trotta, A.; Fisher, H.L. Childhood adversity and psychosis: A systematic review of bio-psycho-social mediators and moderators. Psychol. Med. 2020, 50, 1761–1782. [Google Scholar] [CrossRef]
- Tomassi, S.; Tosato, S. Epigenetics and gene expression profile in first-episode psychosis: The role of childhood trauma. Neurosci. Biobehav. Rev. 2017, 83, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.Y.; Zhang, X.; Pan, L.Y.; Ma, Y.C. Childhood infection and subsequent risk of psychotic disorders in adults: A systematic review and meta-analysis. Asian J. Psychiatr 2020, 54, 102275. [Google Scholar] [CrossRef] [PubMed]
- van Winkel, R.; Kuepper, R. Epidemiological, neurobiological, and genetic clues to the mechanisms linking cannabis use to risk for nonaffective psychosis. Annu. Rev. Clin. Psychol. 2014, 10, 767–791. [Google Scholar] [CrossRef]
- Marconi, A.; Di Forti, M.; Lewis, C.M.; Murray, R.M.; Vassos, E. Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. Schizophr. Bull. 2016, 42, 1262–1269. [Google Scholar] [CrossRef]
- Ortiz-Medina, M.B.; Perea, M.; Torales, J.; Ventriglio, A.; Vitrani, G.; Aguilar, L.; Roncero, C. Cannabis consumption and psychosis or schizophrenia development. Int. J. Soc. Psychiatry 2018, 64, 690–704. [Google Scholar] [CrossRef]
- King, M.; Jones, R.; Petersen, I.; Hamilton, F.; Nazareth, I. Cigarette smoking as a risk factor for schizophrenia or all non-affective psychoses. Psychol. Med. 2021, 51, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.G.; Matuschka, L.; Niemelä, S.; Miettunen, J.; Emmerson, B.; Mustonen, A. Evidence of a Causal Relationship Between Smoking Tobacco and Schizophrenia Spectrum Disorders. Front. Psychiatry 2018, 9, 607. [Google Scholar] [CrossRef]
- Masood, B.; Lepping, P.; Romanov, D.; Poole, R. Treatment of Alcohol-Induced Psychotic Disorder (Alcoholic Hallucinosis)—A Systematic Review. Alcohol Alcohol. 2018, 53, 259–267. [Google Scholar] [CrossRef]
- Regier, D.A.; Farmer, M.E.; Rae, D.S.; Locke, B.Z.; Keith, S.J.; Judd, L.L.; Goodwin, F.K. Comorbidity of mental disorders with alcohol and other drug abuse. JAMA 1990, 264, 2511–2518. [Google Scholar] [CrossRef]
- Hartz, S.M.; Pato, C.N.; Medeiros, H.; Cavazos-Rehg, P.; Sobell, J.J.; Knowles, J.A.; Bierut, L.J.; Pato, M.T. Comorbidity of Severe Psychotic Disorders With Measures of Substance Use. JAMA Psychiatry 2014, 71, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartz, S.M.; Horton, A.C.; Oehlert, M.; Carey, C.E.; Agrawal, A.; Bogdan, R.; ShiunChen, L.; Hancock, D.B.; Johnson, E.O.; Pato, C.N.; et al. Association between substance use disorder and polygenic liability to schizophrenia. Biol. Psychiatry 2017, 82, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Addington, J.; Case, N.; Saleem, M.M.; Auther, A.M.; Cornblatt, B.A.; Cadenhead, K.S. Substance use in clinical high risk for psychosis: A review of the literature. Early Interv. Psychiatry 2014, 8, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huizink, A.C.; Mulder, E.J. Maternal smoking, drinking or cannabis use during pregnancy and neurobehavioral and cognitive functioning in human offspring. Neurosci. Biobehav. Rev. 2006, 30, 24–41. [Google Scholar] [CrossRef]
- Zammit, S.; Thomas, K.; Thompson, A.; Horwood, J.; Menezes, P.; Gunnell, D.; Hollis, C.; Wolke, D.; Lewis, G.; Harrison, G. Maternal tobacco, cannabis and alcohol use during pregnancy and risk of adolescent psychotic symptoms in offspring. Br. J. Psychiatry 2009, 195, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Attademo, L.; Bernardini, F.; Garinella, R.; Compton, M.T. Environmental pollution and risk of psychotic disorders: A review of the science to date. Schizophr. Res. 2017, 181, 55–59. [Google Scholar] [CrossRef]
- David, A.S.; Prince, M. Psychosis following head injury: A critical review. J. Neurol. Neurosurg. Psychiatry 2005, 76 (Suppl. 1), i53–i60. [Google Scholar] [CrossRef]
- Watson, C.J.; Thomas, R.H.; Solomon, T.; Michael, B.D.; Nicholson, T.R.; Pollak, T.A. COVID-19 and psychosis risk: Real or delusional concern? Neurosci. Lett. 2021, 741, 135491. [Google Scholar] [CrossRef]
- Rutter, M. Resilience in the face of adversity: Protective factors and resistence to psychiatric disorder. Br. J. Psychiatry 1985, 147, 598–611. [Google Scholar] [CrossRef]
- Institute of Medicine. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research; The National Academies Press: Washington, DC, USA, 1994. [Google Scholar] [CrossRef]
- Moberg, P.J.; Kamath, V.; Marchetto, D.M.; Calkins, M.E.; Doty, R.L.; Hahn, C.G.; Borgmann-Winter, K.E.; Kohler, C.G.; Gur, R.E.; Turetsky, B.I. Meta-analysis of olfactory function in schizophrenia, first-degree family members, and youths at-risk for psychosis. Schizophr. Bull. 2014, 40, 50–59. [Google Scholar] [CrossRef]
- Riches, S.; Arseneault, L.; Bagher-Niakan, R.; Alsultan, M.; Crush, E.; Fisher, H.L. Protective Factors for Early Psychotic Phenomena Among Children of Mothers with Psychosis. Front. Psychiatry 2019, 9, 750. [Google Scholar] [CrossRef] [Green Version]
- Mizuno, Y.; Wartelsteiner, F.; Frajo-Apor, B. Resilience research in schizophrenia: A review of recent developments. Curr. Opin. Psychiatry 2016, 29, 218–223. [Google Scholar] [CrossRef]
- Euesden, J.; Breen, G.; Farmer, A.; McGuffin, P.; Lewis, C.M. The Relationship Between Schizophrenia and Rheumatoid Arthritis Revisited: Genetic and Epidemiological Analyses. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2015, 168B, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, J.; Brown, A.; St Clair, D. Prevention and schizophrenia--the role of dietary factors. Schizophr. Bull. 2011, 37, 272–283. [Google Scholar] [CrossRef] [Green Version]
- Freedman, R.; Ross, R.G. Prenatal choline and the development of schizophrenia. Shanghai Arch. Psychiatry 2015, 27, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Allswede, D.M.; Buka, S.L.; Yolken, R.H.; Torrey, E.F.; Cannon, T.D. Elevated maternal cytokine levels at birth and risk for psychosis in adult offspring. Schizophr. Res. 2016, 172, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Crush, E.; Arseneault, L.; Jaffee, S.R.; Danese, A.; Fisher, H.L. Protective Factors for Psychotic Symptoms Among Poly-victimized Children. Schizophr. Bull. 2018, 44, 691–700. [Google Scholar] [CrossRef] [Green Version]
- González-Pinto, A.; Ruiz de Azúa, S.; Ibáñez, B.; Otero-Cuesta, S.; Castro-Fornieles, J.; Graell-Berna, M.; Ugarte, A.; Parellada, M.; Moreno, D.; Soutullo, C.; et al. Can positive family factors be protective against the development of psychosis? Psychiatry Res. 2011, 186, 28–33. [Google Scholar] [CrossRef]
- Tienari, P.; Wynne, L.C.; Sorri, A.; Lahti, I.; Läksy, K.; Moring, J.; Naarala, M.; Nieminen, P.; Wahlberg, K.E. Genotype-environment interaction in schizophrenia-spectrum disorder. Long-term follow-up study of Finnish adoptees. Br. J. Psychiatry 2004, 184, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Wahlberg, K.E.; Wynne, L.C.; Hakko, H.; Läksy, K.; Moring, J.; Miettunen, J.; Tienari, P. Interaction of genetic risk and adoptive parent communication deviance: Longitudinal prediction of adoptee psychiatric disorders. Psychol. Med. 2004, 34, 1531–1541. [Google Scholar] [CrossRef]
- Brokmeier, L.L.; Firth, J.; Vancampfort, D.; Smith, L.; Deenik, J.; Rosenbaum, S.; Stubbs, B.; Schuch, F.B. Does physical activity reduce the risk of psychosis? A systematic review and meta-analysis of prospective studies. Psychiatry Res. 2020, 284, 112675. [Google Scholar] [CrossRef]
- Olds, D.L.; Eckenrode, J.; Henderson, C.R., Jr.; Kitzman, H.; Powers, J.; Cole, R.; Sidora, K.; Morris, P.; Pettitt, L.M.; Luckey, D. Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial. JAMA 1997, 278, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Schweinhart, L. Long-term follow-up of a preschool experiment. J. Exp. Criminol. 2013, 9, 389–409. [Google Scholar] [CrossRef] [Green Version]
- Colizzi, M.; Lasalvia, A.; Ruggeri, M. Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? Int. J. Ment. Health Syst. 2020, 14, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Bipolar Disorder, Psychosis and Schizophrenia in Children and Young People. 2015. Available online: https://www.nice.org.uk/guidance/qs102 (accessed on 16 September 2021).
- Fusar-Poli, P.; Davies, C.; Solmi, M.; Brondino, N.; De Micheli, A.; Kotlicka-Antczak, M.; Shin, J.I.; Radua, J. Preventive Treatments for Psychosis: Umbrella Review (Just the Evidence). Front. Psychiatry 2019, 10, 764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGorry, P.D.; Hartmann, J.A.; Spooner, R.; Nelson, B. Beyond the “at risk mental state” concept: Transitioning to transdiagnostic psychiatry. World Psychiatry 2018, 17, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGorry, P.D.; Yung, A.R.; Phillips, L.J. The “close-in” or ultra high-risk model: A safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr. Bull. 2003, 29, 771–790. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, P.; Bonoldi, I.; Yung, A.R.; Borgwardt, S.; Kempton, M.J.; Valmaggia, L.; Barale, F.; Caverzasi, E.; McGuire, P. Predicting psychosis: Meta-analysis of transition outcomes in individuals at high clinical risk. Arch. Gen. Psychiatry 2012, 69, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savill, M.; D’Ambrosio, J.; Cannon, T.D.; Loewy, R.L. Psychosis risk screening in different populations using the Prodromal Questionnaire: A systematic review. Early Interv. Psychiatry 2018, 12, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Cannon, T.D.; Yu, C.; Addington, J.; Bearden, C.E.; Cadenhead, K.S.; Cornblatt, B.A.; Heinssen, R.; Jeffries, C.D.; Mathalon, D.H.; McGlashan, T.H.; et al. An Individualized Risk Calculator for Research in Prodromal Psychosis. Am. J. Psychiatry 2016, 173, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Rutigliano, G.; Stahl, D.; Davies, C.; Bonoldi, I.; Reilly, T.; McGuire, P. Development and Validation of a Clinically Based Risk Calculator for the Transdiagnostic Prediction of Psychosis. JAMA Psychiatry 2017, 74, 493–500. [Google Scholar] [CrossRef]
- Clark, S.R.; Baune, B.T.; Schubert, K.O.; Lavoie, S.; Smesny, S.; Rice, S.M.; Schäfer, M.R.; Benninger, F.; Feucht, M.; Klier, C.M.; et al. Prediction of transition from ultra-high risk to first-episode psychosis using a probabilistic model combining history, clinical assessment and fatty-acid biomarkers. Transl. Psychiatry 2016, 6, e897. [Google Scholar] [CrossRef] [Green Version]
- Yuen, H.P.; Mackinnon, A. Performance of joint modelling of time-to-event data with time-dependent predictors: An assessment based on transition to psychosis data. PeerJ 2016, 4, e2582. [Google Scholar] [CrossRef] [PubMed]
- Rus-Calafell, M.; Schneider, S. Are we there yet?!—A literature review of recent digital technology advances for the treatment of early psychosis. mHealth 2020, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Gupta, T.; Mittal, V.A. Advances in clinical staging, early intervention, and the prevention of psychosis [version 1; peer review: 3 approved]. F1000Research 2019, 8, 2027. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Sullivan, S.A.; Shah, J.L.; Uhlhaas, P.J. Improving the Detection of Individuals at Clinical Risk for Psychosis in the Community, Primary and Secondary Care: An Integrated Evidence-Based Approach. Front. Psychiatry 2019, 10, 774. [Google Scholar] [CrossRef] [Green Version]
- Salazar de Pablo, G.; Estradé, A.; Cutroni, M.; Andlauer, O.; Fusar-Poli, P. Establishing a clinical service to prevent psychosis: What, how and when? Systematic review. Transl. Psychiatry 2021, 11, 43. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Salazar de Pablo, G.; Correll, C.U.; Meyer-Lindenberg, A.; Millan, M.J.; Borgwardt, S.; Galderisi, S.; Bechdolf, A.; Pfennig, A.; Kessing, L.V.; et al. Prevention of Psychosis: Advances in Detection, Prognosis, and Intervention. JAMA Psychiatry 2020, 77, 755–765. [Google Scholar] [CrossRef]
- Bosnjak Kuharic, D.; Kekin, I.; Hew, J.; Rojnic Kuzman, M.; Puljak, L. Interventions for prodromal stage of psychosis. Cochrane Database Syst. Rev. 2019, CD012236. [Google Scholar] [CrossRef]
- Devoe, D.J.; Farris, M.S.; Townes, P.; Addington, J. Interventions and Transition in Youth at Risk of Psychosis: A Systematic Review and Meta-Analyses. J. Clin. Psychiatry 2020, 81, 17r12053. [Google Scholar] [CrossRef]
- Häfner, H.; Maurer, K.; Ruhrmann, S.; Bechdolf, A.; Klosterkötter, J.; Wagner, M.; Maier, W.; Bottlender, R.; Möller, H.J.; Gaebel, W.; et al. Early detection and secondary prevention of psychosis: Facts and visions. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Klosterkötter, J.; Hellmich, M.; Steinmayer, E.M.; Schultze-Lutter, F. Diagnosing schizophrenia in the initial prodromal phase. Arch. Gen. Psychiatry 2001, 58, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Yung, A.R.; Yuen, H.P.; McGorry, P.D.; Phillips, L.J.; Kelly, D.; Dell’Olio, M.; Francey, S.M.; Cosgrave, E.M.; Killackey, E.; Stanford, C.; et al. Mapping the onset of psychosis: The Comprehensive Assessment of At-Risk Mental States. Aust. N. Z. J. Psychiatry 2005, 39, 964–971. [Google Scholar] [CrossRef]
- Miller, T.J.; McGlashan, T.H.; Rosen, J.L.; Cadenhead, K.; Cannon, T.; Ventura, J.; McFarlane, W.; Perkins, D.O.; Pearlson, G.D.; Woods, S.W. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: Predictive validity, interrater reliability, and training to reliability. Schizophr. Bull. 2003, 29, 703–715, Erratum in Schizophr Bull. 2004, 30, 217. [Google Scholar] [CrossRef] [Green Version]
- Häfner, H.; Riecher, A.; Maurer, K.; Meissner, S. Ein Instrument zurretrospektiven Einschätzung des Erkrankungsbeginns beiSchizophrenie (Instrument for the retrospective assessmentof the onset of schizophrenia—‘IRAOS’)—Entwicklung undErgebnisse. Z Klin. Psychol. 1990, 19, 230–255. [Google Scholar]
- Häfner, H.; Riecher-Rössler, A.; Hambrecht, M.; Maurer, K.; Meissner, S.; Schmidtke, A.; Fätkenheuer, B.; Löffler, W.; van der Heiden, W. IRAOS: An instrument for the assessment of onset and early course of schizophrenia. Schizophr. Res. 1992, 6, 209–223. [Google Scholar] [CrossRef]
- Häfner, H.; Löffler, W.; Maurer, K.; Riecher-Rössler, A.; Stein, A. IRAOS—Interview for the Retrospective Assessment of the Onset and Course of Schizophrenia and Other Psychoses; Hogrefe & Huber: Göttingen, Germany, 2003. [Google Scholar]
- Maurer, K.; Zink, M.; Rausch, F.; Häfner, H. The early recognition inventory ERIraos assesses the entire spectrum of symptoms through the course of an at-risk mental state. Early Interv. Psychiatry 2018, 12, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Rausch, F.; Eifler, S.; Esser, A.; Esslinger, C.; Schirmbeck, F.; Meyer-Lindenberg, A.; Zink, M. The Early Recognition Inventory ERIraos detects at risk mental states of psychosis with high sensitivity. Compr. Psychiatry 2013, 54, 1068–1076. [Google Scholar] [CrossRef]
- Maurer, K.; Hörrmann, F.; Trendler, G.; Schmidt, M.; Häfner, H. Früherkennung des Psychoserisikos mit dem Early Recognition Inventory (ERIraos). Identification of psychosis risk by the Early Recognition Inventory (ERIraos)—description of the schedules and preliminary results on reliability and validity of the checklist. Nervenheilkunde 2006, 25, 11–16. [Google Scholar]
- Maurer, K.; Häfner, H. Rasch scaling of a screening instrument: Assessing proximity to psychosis onset by the ERIraos Checklist. Sage Open 2014, 4. [Google Scholar] [CrossRef]
- Meneghelli, A.; Alpi, A.; Cascio, M.T.; Häfner, H.; Maurer, K.; Preti, A.; Raballo, A.; Cocchi, A. Versione Italiana dell’Early Recognition Inventory for the retrospective assessment of the onset of schizophrenia Checklist: Affidabilità, validità e istruzioni per l’uso. J. Psychopathol. 2014, 20, 186–198. [Google Scholar]
- Melle, I.; Larsen, T.K.; Haahr, U.; Friis, S.; Johannessen, J.O.; Opjordsmoen, S.; Simonsen, E.; Rund, B.R.; Vaglum, P.; McGlashan, T. Reducing the duration of untreated first-episode psychosis: Effects on clinical presentation. Arch. Gen. Psychiatry 2004, 61, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wölwer, W.; Buchkremer, G.; Häfner, H.; Klosterkötter, J.; Maier, W.; Möller, H.J.; Gaebel, W. German research network on schizophrenia-bridging the gap between research and care. Eur. Arch. Psychiatry Clin. Neurosci. 2003, 253, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, J.O.; Larsen, T.K.; Joa, I.; Melle, I.; Friis, S.; Opjordsmoen, S.; Rund, B.R.; Simonsen, E.; Vaglum, P.; McGlashan, T.H. Pathways to care for first-episode psychosis in an early detection healthcare sector: Part of the Scandinavian TIPS study. Br. J. Psychiatry Suppl. 2005, 48, s24–s28. [Google Scholar] [CrossRef] [Green Version]
- Maurer, K.; Häfner, H. Checkliste fürr die Hausarztpraxis in Arbeit. Erste Signale einer Psychose richtig deuten [Early diagnosis of schizophrenia]. MMW Fortschr. Med. 2007, 149, 36–38. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gene Loci | Corresponding Transcript/Protein and Localization | Principal Known Functions | ||||
|---|---|---|---|---|---|---|
| General Description of the Function(s) | Central Nervous System (CNS) Development | Neuronal Morphology Regulation | Signal Transmission | |||
| NEUROTRANSMITTER RECEPTORS | DRD2 (Dopamine Receptor D2) | G protein-coupled membrane receptor | Dopamine signaling | Dopaminergic system | ||
| DRD1, 3, 4 (Dopamine Receptors D1, D3, D4) | G protein-coupled membrane receptor | Dopamine signaling | Dopaminergic system | |||
| HTR2A (5-Hydroxytryptamine -5-HT- Receptor 2A) [44] | G protein-coupled membrane receptor | Regulation of dopamine and glutamate release in the mesolimbic and mesocortical systems | Serotoninergic system Dopaminergic system Glutamatergic system | |||
| GRM3 (Glutamate Metabotropic Receptor 3) | G protein-coupled membrane receptor | Glutamate signaling | Glutamatergic system | |||
| GRIN2B (Glutamate Ionotropic Receptor N-methyl-D-aspartate—NMDA—Type Subunit 2B) | Subunit of the NMDA membrane receptor—ion channel (NMDAR) | Neurodevelopment, circuit formation, synaptic plasticity, and cellular migration and differentiation | Neurogenesis Differentiation of neural progenitors | Glutamatergic system | ||
| GABRB2 (Gamma-Aminobutyric Acid -GABA- Type A Receptor Subunit Beta2) | Subunit of the GABA-A membrane receptor—ion channel | Balance in excitatory/inhibitory signaling in the CNS | GABAergic system | |||
| NEUROTRASMITTER METABOLISM AND SIGNAL REGULATION | PDE4B (Phosphodiesterase 4B) | Intracellular enzyme | Cyclic AMP (cAMP)-specific phosphodiesterase (PDE), family IV. It modulates cAMP second messenger concentration in the transduction of the signal process | Signal transmission in different systems | ||
| COMT (Catechol-O-Methyl-transferase) | Intracellular enzyme | Dopamine and noradrenaline metabolism | Dopaminergic system Noradrenergic system | |||
| RGS-4 (Regulator of G Protein Signaling 4) [45] | Intracellular enzyme activator | Activate GTPase activity of G alpha subunits of heterotrimeric G proteins, thus deactivating them | Differentiation of neural progenitors—Axonogenesis in embryogenesis | Glutamatergic system (signal transduction) | ||
| SLC18A2 (Solute Carrier Family 18 Member A2) | ATP-dependent transmembrane transporter | ATP-dependent transporter of monoamines | Dopaminergic system Serotoninergic system Noradrenergic system | |||
| DAOA (D-Amino Acid Oxidase Activator) and DAOA-AS1 (Antisense RNA 1) | Intracellular enzyme activator and corresponding long non-coding RNA | Metabolism of glial D-serine that regulates neuronal NDMAR signaling, mitochondrial function, dendritic arborization | Dendritic regulation | Glia-neuron communication Glutamatergic system | ||
| DTNBP1 (Dystrobrevin Binding Protein 1) and CMYA5 (Cardiomyopathy Associated 5) | Intracellular proteins that participate in the formation of the lysosome-related organelles complex 1 (BLOC-1) | Synaptic vesicle trafficking and neurotransmitter release, in particular regulation of cell surface exposure of DRD2 and glutamatergic release. Actin cytoskeleton reorganization and neurite outgrowth. | Neurite regulation | Dopaminergic system Glutamatergic system Synaptic regulation | ||
| CELL-CELL CONTACT AND NEURODEVELOPMENT | DISC1 (Disrupted In Schizophrenia 1) | Scaffold intracellular protein | Involved in neurogenesis (neural progenitor proliferation, neuron positioning), dendritic development, and synapse formation | Neurogenesis | Dendritic regulation | Synaptic regulation |
| NRXN1 (Neurexin 1) | Membrane receptor | Binds neuroligins to form Ca(2+)-dependent neurexin/neuroligin complexes at synapses in the CNS | Synaptic regulation | |||
| ERBB4 (Erb-B2 Receptor Tyrosine Kinase 4) | Membrane receptor tyrosine kinases, epidermal growth factor subfamily. | Binds neuroregulins NMDAR pathway | Regulation of CNS development | Glutamatergic system | ||
| NRG1 (Neuregulin 1) | Membrane glycoprotein | Mediates cell–cell signaling. Binds to ERBB receptors NMDAR pathway | Neurogenesis Gliogenesis Differentiation of neural progenitors | Glutamatergic system | ||
| AKT1 (AKT-8 retrovirus Serine/Threonine Kinase 1) [46] | Intracellular Serine/Threonine kinase | Known oncogene involved PI3K and mTOR signaling pathways Placentar and CNS development and functioning | Neurogenesis | Dendritic regulation | Synaptic regulation | |
| RELN (Reelin) | Large extracellular matrix serine protease | Enzymatic activity modulates cell adhesion | CNS development (cellular migration) | Neuronal morphology regulation (microtubule functioning) | ||
| IMMUNE SYSTEM | IL1B (Interleukin 1 Beta) | Cytokine (extracellular messenger) | Potent proinflammatory cytokine, involved in neuroinflammation during neurodevelopment and adult life | Altered by neuroinflammation | ||
| Factors Associated with the Development of Primary Psychosis | Prenatal | Perinatal | Childhood | Adolescence | Strength of Evidence of the Association | References | Modifiable Factor | Level(s) of Preventive Intervention | |
|---|---|---|---|---|---|---|---|---|---|
| RISK | Family history of primary psychosis | ● | +++ | [13,16,17,19,20,21] | No | - | |||
| Paternal characteristics (e.g., age <20 or >45, low socio-economic status) | ● | +++ | [13,15,23,24] | No | - | ||||
| Maternal characteristics (e.g., age <20 or >35, any severe psychiatric condition, pre-pregnancy obesity) | ● | +++ | [15,23] | Only obesity | Primary | ||||
| Diabetes and hypertension during pregnancy | ● | ++ | [15] | Yes | Primary | ||||
| Maternal infections during pregnancy | ● | +++ | [13,23,48] | Yes | Primary | ||||
| Suboptimal number of antenatal care visits | ● | ++ | [23] | Yes | Primary | ||||
| Maternal stress during pregnancy | ● | +++ | [13,23] | Yes | Primordial a | ||||
| Maternal nutritional deficits during pregnancy | ● | +++ | [13,23] | Yes | Primary | ||||
| Obstetric complications (e.g., maternal or fetal hypoxia during delivery, preterm ruptured membranes) | ● | +++ | [15,23] | No | - | ||||
| Neonatal factors (e.g., premature birth, incubator or resuscitation) | ● | +++ | [13,15,23] | No | - | ||||
| Minor physical anomalies | ● | ++++ | [15,16,24,28] | No | - | ||||
| Genetic factors (cf. Table 2) | ● | ● | ● | +++ | [17,18,22,42,43] | No | - | ||
| Socio-demographic (e.g., male gender, ethnic minority, birth in winter, disadvantaged groups) | ● | ● | ● | ● | ++++ | [13,15,20,23,24] | Only social part | Primordial b | |
| Childhood adversities and traumas (e.g., physical, psychological, and sexual abuse, bullying) | ● | +++ | [13,15,24,51,52,53,55] | Yes | Primordial b | ||||
| Difficult parental relationship (e.g., parental communication deviance, separation or death, neglect) | ● | +++ | [15,52,53,55] | Only some | Primordial c | ||||
| Childhood infections (mostly CNS infections) | ● | +++ | [15,24,28,31,58] | Yes | Primary | ||||
| Traumatic brain injury | ● | ● | ++ | [13,15] | Yes | Primary | |||
| Exposure to traffic | ● | ● | ++ | [15] | Yes | Primordial | |||
| Exposure to benzene | ● | ● | ++ | [15] | Yes | Primary | |||
| Tobacco use | ● | ++ | [13,15,24,62] | Yes | Primary/Secondary | ||||
| Cannabis use | ● | +++ | [13,20,24,56,59,60] | Yes | Primary/Secondary | ||||
| Psychostimulants use | ● | ++ | [13,20] | Yes | Primary/Secondary | ||||
| Autoimmune diseases (e.g., celiac disease, pernicious anemia) | ● | ● | ++ | [29,30] | No | - | |||
| Psychological characteristics (e.g., trait anhedonia; premorbid low IQ) | ● | ● | ++++ | [15,24] | No | - | |||
| Other psychiatric disorders (e.g., obsessive compulsive disorder, schizotypal personality) | ● | ++ | [32,33,34,35,36,37] | Yes | Primary | ||||
| Urbanicity * | ● | ● | +++ | [13,15,20,24,26] | No | - | |||
| Ethnicity (migration and specific ethnic minorities) * | ● | ● | ++++ | [15,24] | No | - | |||
| PROTECTIVE | Prenatal dietary supplementation (vitamin D, iron, folates, phosphatidyl-choline) | ● | ++ | [80,81] | Yes | Primary d | |||
| Socio-demographic (e.g., elevated socio-economic status and an economic well-being) | ● | ● | ● | ● | +++ | [15] | Yes | Primordial | |
| Physical characteristics (e.g.,: olfactory identification abilities) | ● | ● | ++ | [15,24] | No | - | |||
| Psychological characteristics (e.g., extraversion, openness; high premorbid IQ; resilience) | ● | ● | ++ | [16,24,28] | No | - | |||
| Positive family environment (e.g., good parental system, healthy relationships with relatives) | ● | ● | ++ | [16,83,84] | Yes | Primordial | |||
| Autoimmune diseases (e.g., ankylosing spondylitis) | ● | + | [29,30,79] | No | - | ||||
| Physical activity | ● | + | [87] | Yes | Primordial/Primary | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brasso, C.; Giordano, B.; Badino, C.; Bellino, S.; Bozzatello, P.; Montemagni, C.; Rocca, P. Primary Psychosis: Risk and Protective Factors and Early Detection of the Onset. Diagnostics 2021, 11, 2146. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112146
Brasso C, Giordano B, Badino C, Bellino S, Bozzatello P, Montemagni C, Rocca P. Primary Psychosis: Risk and Protective Factors and Early Detection of the Onset. Diagnostics. 2021; 11(11):2146. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112146
Chicago/Turabian StyleBrasso, Claudio, Benedetta Giordano, Cristina Badino, Silvio Bellino, Paola Bozzatello, Cristiana Montemagni, and Paola Rocca. 2021. "Primary Psychosis: Risk and Protective Factors and Early Detection of the Onset" Diagnostics 11, no. 11: 2146. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112146