
Interpretation According to Clone-Specific PD-L1 Cutoffs Reveals Better Concordance in Muscle-Invasive Urothelial Carcinoma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Microarray Construction and PD-L1 IHC Staining
2.2. Interpretation of PD-L1 Expression
2.3. Statistical Analysis
3. Results
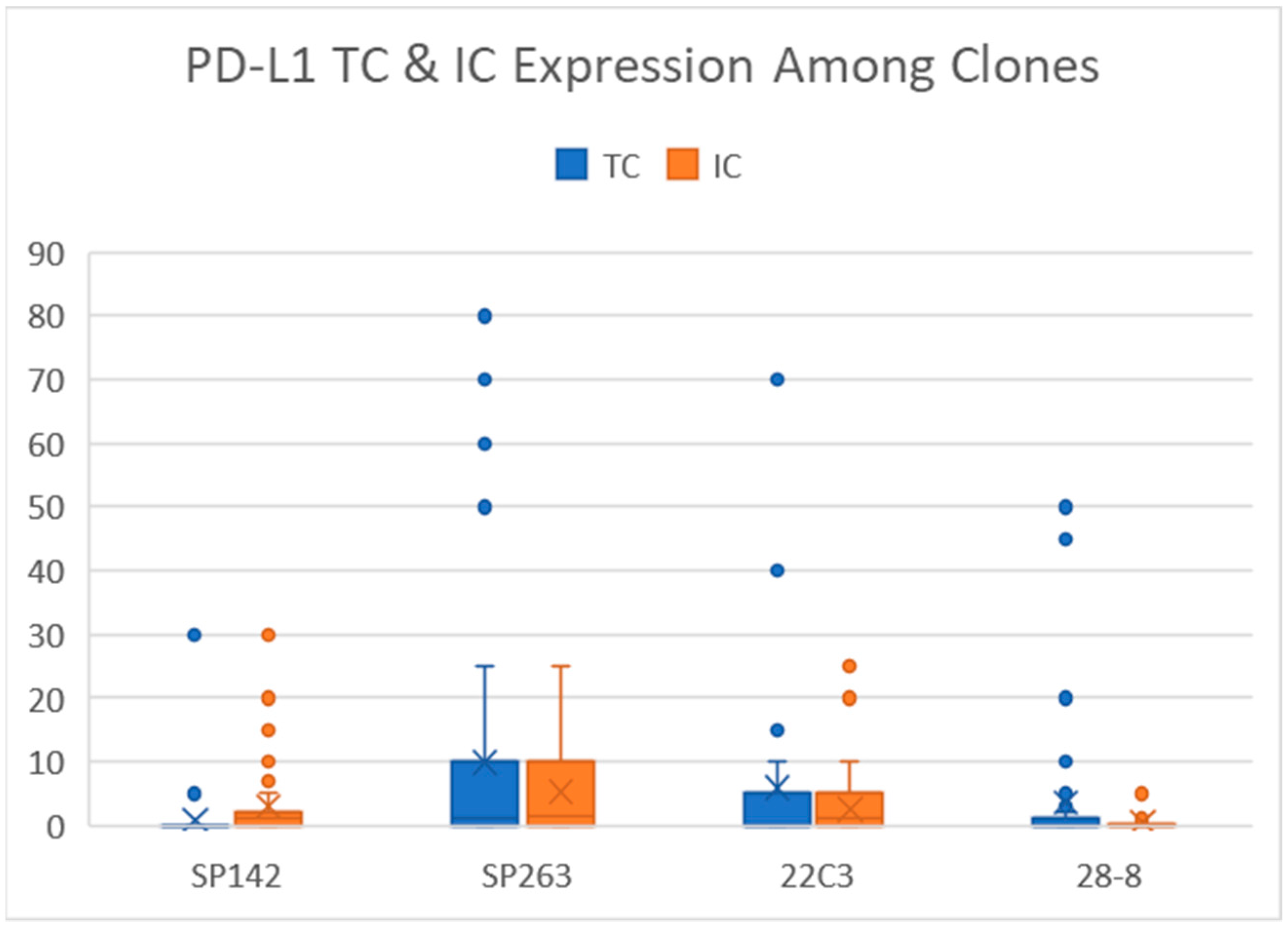
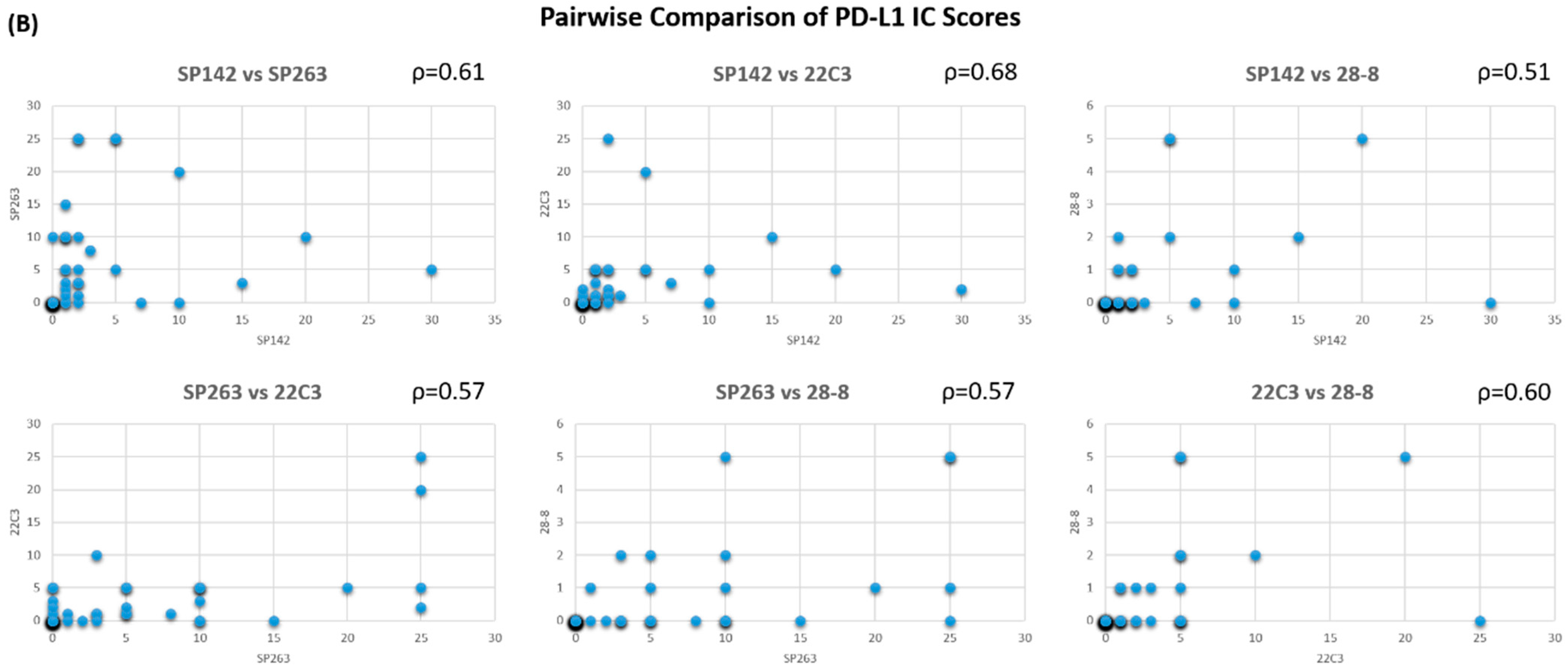
3.1. Correlation of TC and IC Expression between Clones
3.2. Concordance of PD-L1 Expression between Clones
3.3. Association of High PD-L1 Expression between Phenotypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aggen, D.H.; Drake, C.G. Biomarkers for immunotherapy in bladder cancer: A moving target. J. Immunother. Cancer 2017, 5, 94. [Google Scholar] [CrossRef]
- Zhu, J.; Armstrong, A.J.; Friedlander, T.W.; Kim, W.; Pal, S.K.; George, D.J.; Zhang, T. Biomarkers of immunotherapy in urothelial and renal cell carcinoma: PD-L1, tumor mutational burden, and beyond. J. Immunother. Cancer 2018, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Arriola, A.G.P.; Farahani, S.J.; Bhargava, H.K.; Guzzo, T.J.; Brooks, J.S.J.; Lal, P. PD-L1 Expression Reveals Significant Association With Squamous Differentiation in Upper Tract Urothelial Carcinoma. Am. J. Clin. Pathol. 2019, 151, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Lee, C.; Kim, Y.A.; Moon, K.C. PD-L1 Expression in Muscle-Invasive Urinary Bladder Urothelial Carcinoma According to Basal/Squamous-Like Phenotype. Front. Oncol. 2020, 10, 527385. [Google Scholar] [CrossRef] [PubMed]
- Reis, H.; Serrette, R.; Posada, J.; Lu, V.; Chen, Y.-B.; Gopalan, A.; Fine, S.W.; Tickoo, S.K.; Sirintrapun, S.J.; Iyer, G.; et al. PD-L1 Expression in Urothelial Carcinoma With Predominant or Pure Variant Histology. Am. J. Surg. Pathol. 2019, 43, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, A.; Liu, S.K.; Vesprini, D.; Xu, B.; Downes, M.R. Basal-subtype bladder tumours show a ‘hot’ immunophenotype. Histopathology 2018, 73, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [Green Version]
- Ning, Y.; Suzman, D.; Maher, V.E.; Zhang, L.; Tang, S.; Ricks, T.; Palmby, T.; Fu, W.; Liu, Q.; Goldberg, K.B.; et al. FDA Approval Summary: Atezolizumab for the Treatment of Patients with Progressive Advanced Urothelial Carcinoma after Platinum-Containing Chemotherapy. Oncology 2017, 22, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Hirsch, F.R.; McElhinny, A.; Stanforth, D.; Ranger-Moore, J.; Jansson, M.; Kulangara, K.; Richardson, W.; Towne, P.; Hanks, D.; Vennapusa, B.; et al. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J. Thorac. Oncol. 2017, 12, 208–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.-B.; Borczuk, A.C.; Botling, J.; Bubendorf, L.; Chirieac, L.; Chen, G.; Chou, T.-Y.; et al. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roach, C.; Zhang, N.; Corigliano, E.; Jansson, M.; Toland, G.; Ponto, G.; Dolled-Filhart, M.; Emancipator, K.; Stanforth, D.; Kulangara, K. Development of a Companion Diagnostic PD-L1 Immunohistochemistry Assay for Pembrolizumab Therapy in Non–Small-cell Lung Cancer. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstock, C.; Khozin, S.; Suzman, D.; Zhang, L.; Tang, S.; Wahby, S.; Goldberg, K.B.; Kim, G.; Pazdur, R. U.S. Food and Drug Administration Approval Summary: Atezolizumab for Metastatic Non–Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 4534–4539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckstein, M.; Cimadamore, A.; Hartmann, A.; Lopez-Beltran, A.; Cheng, L.; Scarpelli, M.; Montironi, R.; Gevaert, T. PD-L1 assessment in urothelial carcinoma: A practical approach. Ann. Transl. Med. 2019, 7, 690. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.C.; Bondaruk, J.; Yao, H.; Wang, Z.; Zhang, L.; Lee, S.; Lee, J.-G.; Cogdell, D.; Zhang, M.; Yang, G.; et al. Assessment of Luminal and Basal Phenotypes in Bladder Cancer. Sci. Rep. 2020, 10, 9743. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Scheel, A.H.; Dietel, M.; Heukamp, L.C.; Jöhrens, K.; Kirchner, T.; Reu, S.; Rüschoff, J.; Schildhaus, H.-U.; Schirmacher, P.; Tiemann, M.; et al. Harmonized PD-L1 immunohistochemistry for pulmonary squamous-cell and adenocarcinomas. Mod. Pathol. 2016, 29, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Hahn, E.; Slodkowska, E.; Eskander, A.; Enepekides, D.; Higgins, K.; Vesprini, D.; Liu, S.K.; Downes, M.R.; Xu, B. Reproducibility of PD-L1 immunohistochemistry interpretation across various types of genitourinary and head/neck carcinomas, antibody clones, and tissue types. Hum. Pathol. 2018, 82, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Zajac, M.; Scott, M.; Ratcliffe, M.; Scorer, P.; Barker, C.; Al-Masri, H.; Rebelatto, M.C.; Walker, J. Concordance among four commercially available, validated programmed cell death ligand-1 assays in urothelial carcinoma. Diagn. Pathol. 2019, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, A.; Slodkowska, E.; Jungbluth, A.; Liu, S.K.; Vesprini, D.; Enepekides, D.; Higgins, K.; Katabi, N.; Xu, B.; Downes, M.R. PD-L1 Immunohistochemistry Assay Concordance in Urothelial Carcinoma of the Bladder and Hypopharyngeal Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2018, 42, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Tretiakova, M.; Fulton, R.; Kocherginsky, M.; Long, T.; Ussakli, C.; Antic, T.; Gown, A. Concordance study of PD-L1 expression in primary and metastatic bladder carcinomas: Comparison of four commonly used antibodies and RNA expression. Mod. Pathol. 2018, 31, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clone | Scoring Algorithm | Definition of IC Included for Scoring | Cut-Offs |
|---|---|---|---|
| SP142 | All immune cells in the intratumoral and contiguous peritumoral stroma. | IC ≥ 5% | |
| SP263 | or | All immune cells within the tumor reactive stroma, between the tumor islands and those invading the tumor proper. | TC ≥ 25% or IC ≥ 25% |
| 22C3 | Only mononuclear inflammatory cells, including lymphocytes, macrophages/ histiocytes. | CPS ≥ 10 | |
| 28-8 | NA | TC ≥ 5% |
| PD-L1 Clones | SP142 | SP263 | 22C3 | 28-8 |
|---|---|---|---|---|
| SP142 | 1 | TC: 0.41 (−0.1–0.67) IC: 0.29 (−0.24–0.60) | TC: 0.53 (0.17–0.74) IC: 0.36 (−0.17–0.65) | TC: 0.68 (0.48–0.82) IC: 0.25 (−0.24–0.57) |
| SP263 | 0.72 (0.47–0.98) | 1 | TC: 0.92 (0.83–0.96) IC: 0.69 (0.41–0.83) | TC: 0.84 (0.59–0.92) IC: 0.25 (−0.19–0.55) |
| 22C3 | 0.69 (0.45–0.94) | 0.69 (0.45–0.94) | 1 | TC: 0.93 (0.87–0.97) IC: 0.34 (−0.12–0.62) |
| 28-8 | 0.76 (0.51–1.01) | 0.61 (0.30–91) | 0.60 (0.32–0.87) | 1 |
| Clone | SP142 (p = 0.05) | SP263 (p = 0.05) | 22C3 (p = 0.07) | 28-8 (p = 0.01) | ||||
|---|---|---|---|---|---|---|---|---|
| Expression | Low | High | Low | High | Low | High | Low | High |
| Luminal type | 31 | 5 | 31 | 5 | 29 | 7 | 34 | 2 |
| Basal type | 2 | 3 | 2 | 3 | 2 | 3 | 2 | 3 |
| Undetermined | 4 | 1 | 4 | 1 | 3 | 2 | 4 | 1 |
| Total | 37 | 9 | 37 | 9 | 34 | 12 | 40 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, T.-H.; Cheng, W.; Wang, Y.-H. Interpretation According to Clone-Specific PD-L1 Cutoffs Reveals Better Concordance in Muscle-Invasive Urothelial Carcinoma. Diagnostics 2021, 11, 448. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030448
Huang T-H, Cheng W, Wang Y-H. Interpretation According to Clone-Specific PD-L1 Cutoffs Reveals Better Concordance in Muscle-Invasive Urothelial Carcinoma. Diagnostics. 2021; 11(3):448. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030448
Chicago/Turabian StyleHuang, Tzu-Hao, Wei Cheng, and Yeh-Han Wang. 2021. "Interpretation According to Clone-Specific PD-L1 Cutoffs Reveals Better Concordance in Muscle-Invasive Urothelial Carcinoma" Diagnostics 11, no. 3: 448. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030448