
The Role in Teledermoscopy of an Inexpensive and Easy-to-Use Smartphone Device for the Classification of Three Types of Skin Lesions Using Convolutional Neural Networks

 , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
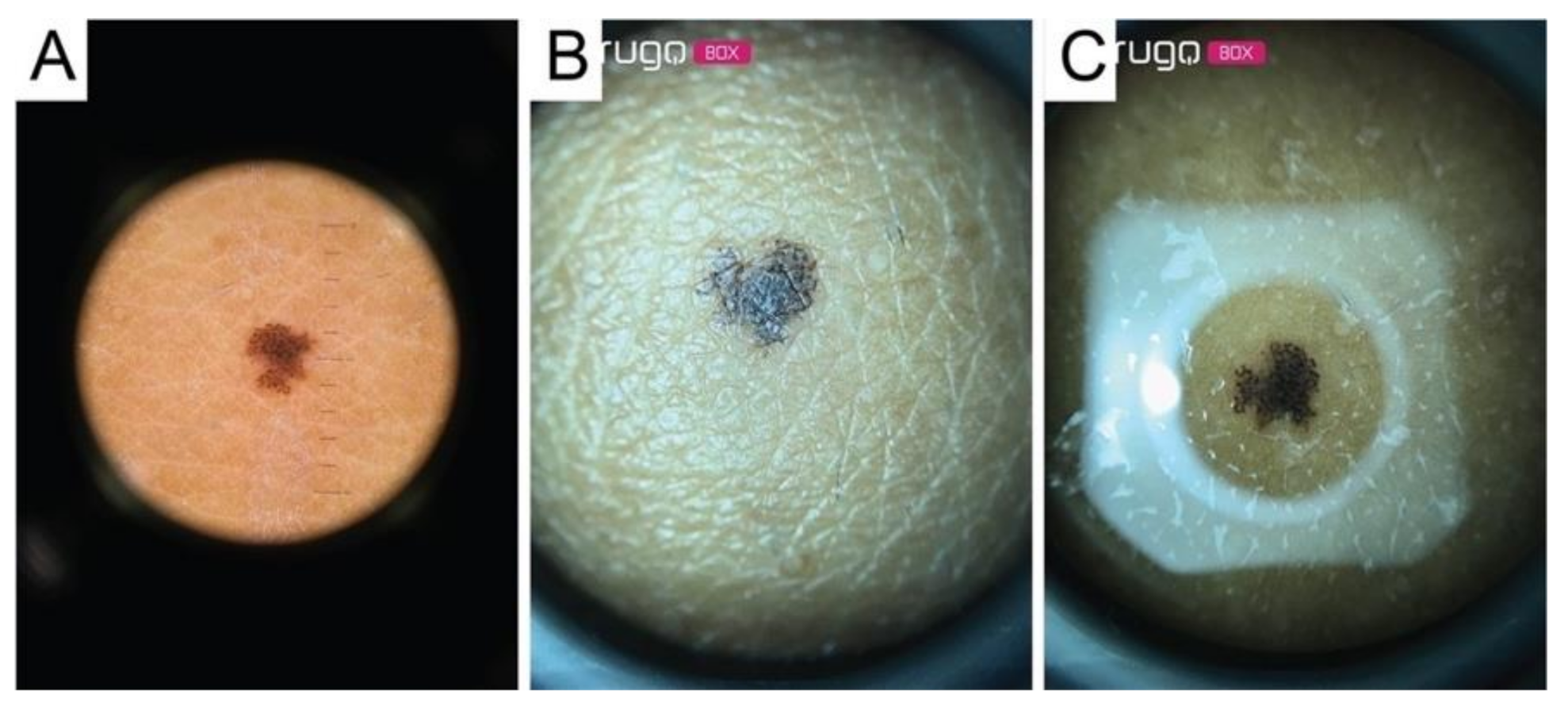
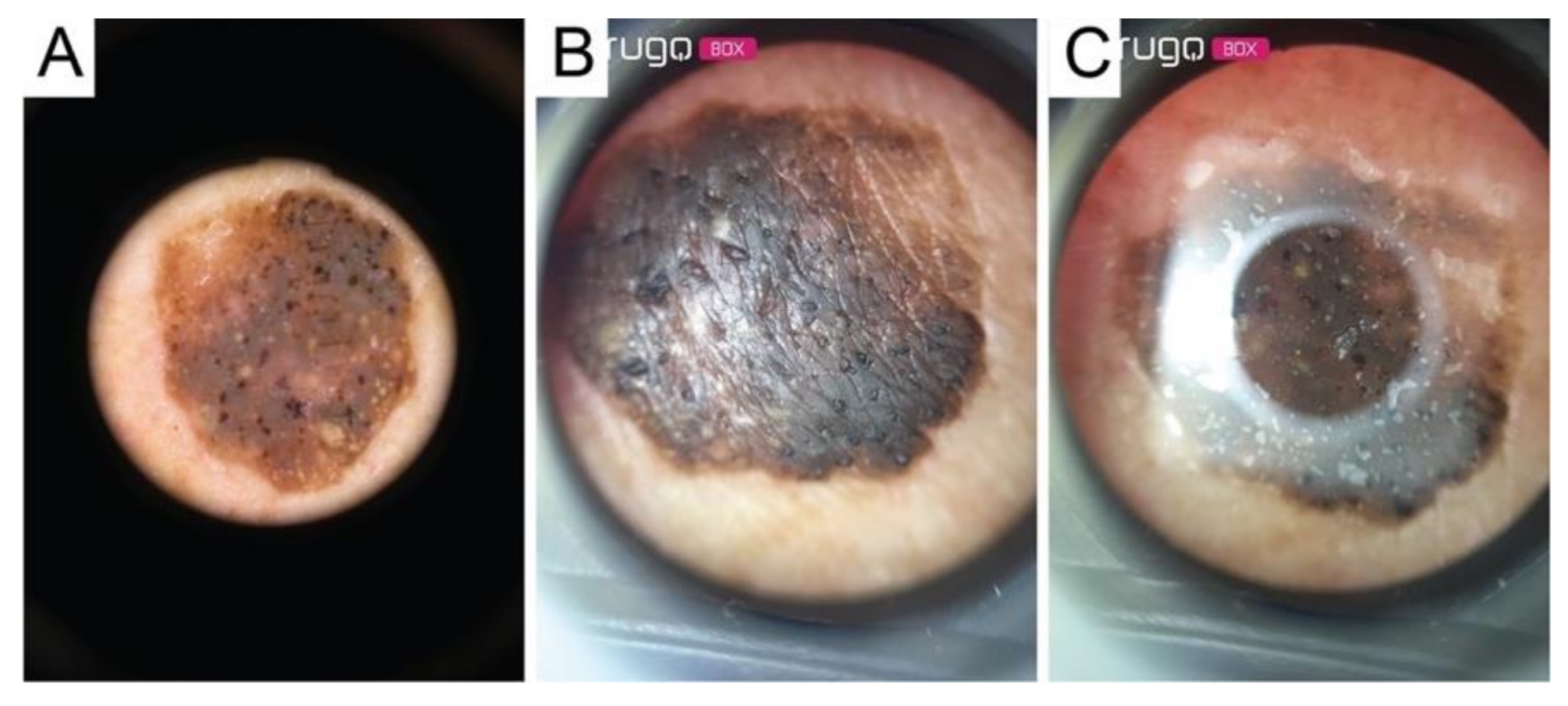
2.1. Devices’ and Images’ Acquisition
- (1)
- Shadow effect: due to not being able to compress the lesions directly using the Nurugo microscope (Figure 3A);
- (2)
- Glare effect: due to the light of the smartphone flash reflected off of the skin (Figure 3B);
- (3)
- The inability to acquire epiluminescence images (the flash of common smartphones does not produce polarized light and, therefore, does not allow the visualization of the structures under the epidermis); and
- (4)
- Impossibility of applying immersion oil to cancel the reflection of light (the device has no support downstream of the lens).
2.2. Processing
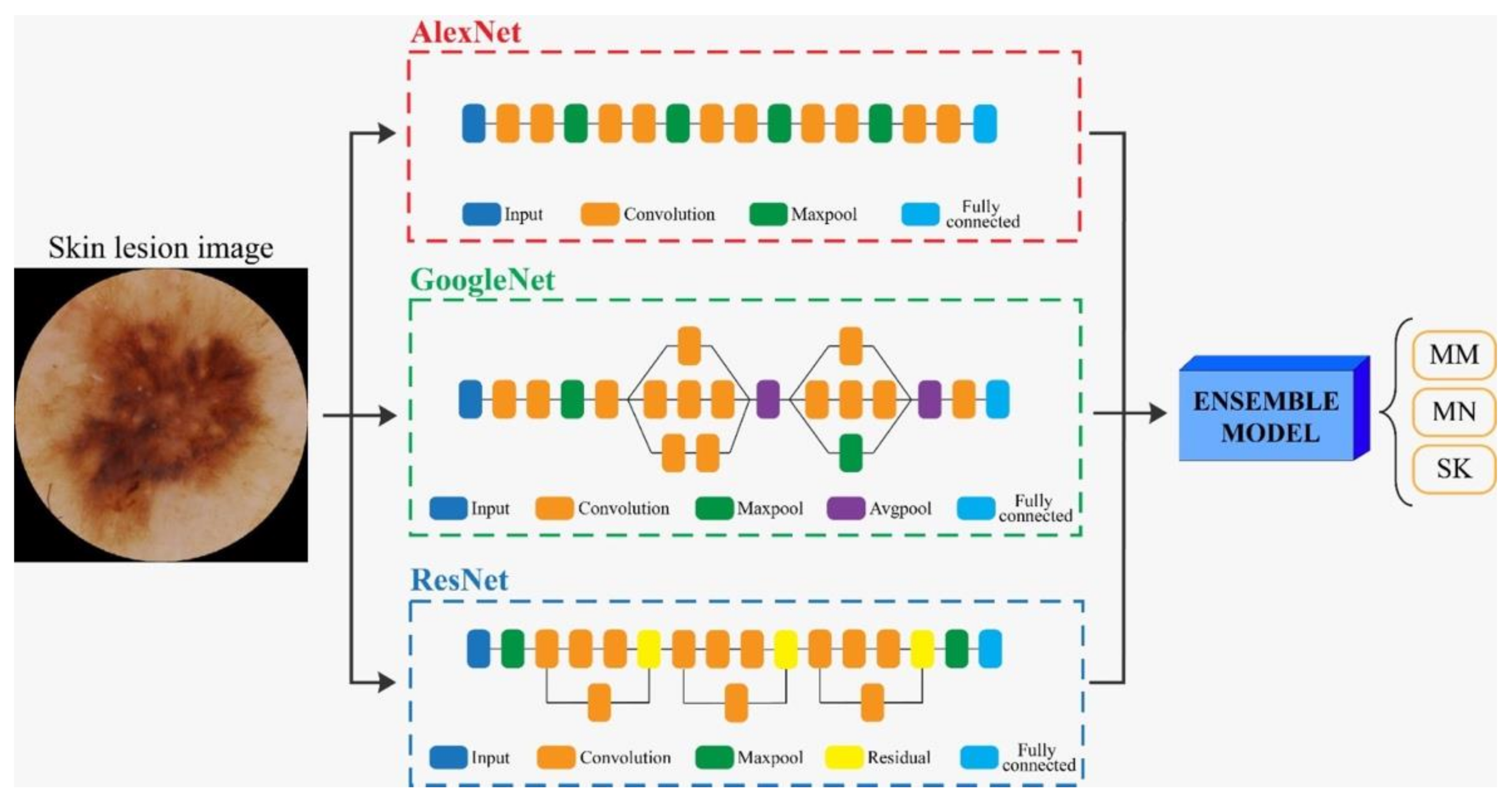
2.3. CNN Classification Algorithm
- (1)
- Training phase in which networks learn from the examples provided (training-set images for learning and validation-set images to test the learning level).
- (2)
- Evaluation of the final performances on the test set images to understand the model’s ability to classify new images, not used during training.
- (3)
- In our study, transfer learning was applied using three different CNN architectures: AlexNet, GoogleNet, and ResNet [14]. The AlexNet [15] employed a series of convolutional layers to extract a higher-level representation of the image content. The GoogleNet [16] was organized to concatenate convolutional layers having different kernel sizes. The ResNet [17] adopted skip connections and batch normalization to perform the classification task.
- (4)
- Finally, we created an ensemble model that combined the predictions of the three deep networks (AlexNet, GoogleNet, and ResNet). Specifically, the probability of the ensemble model was obtained as the average of the three output probabilities from each single CNN. Then, the final, predicted label was equal to the predicted label with maximum probability over all classes (MM, MN, SK).
3. Results
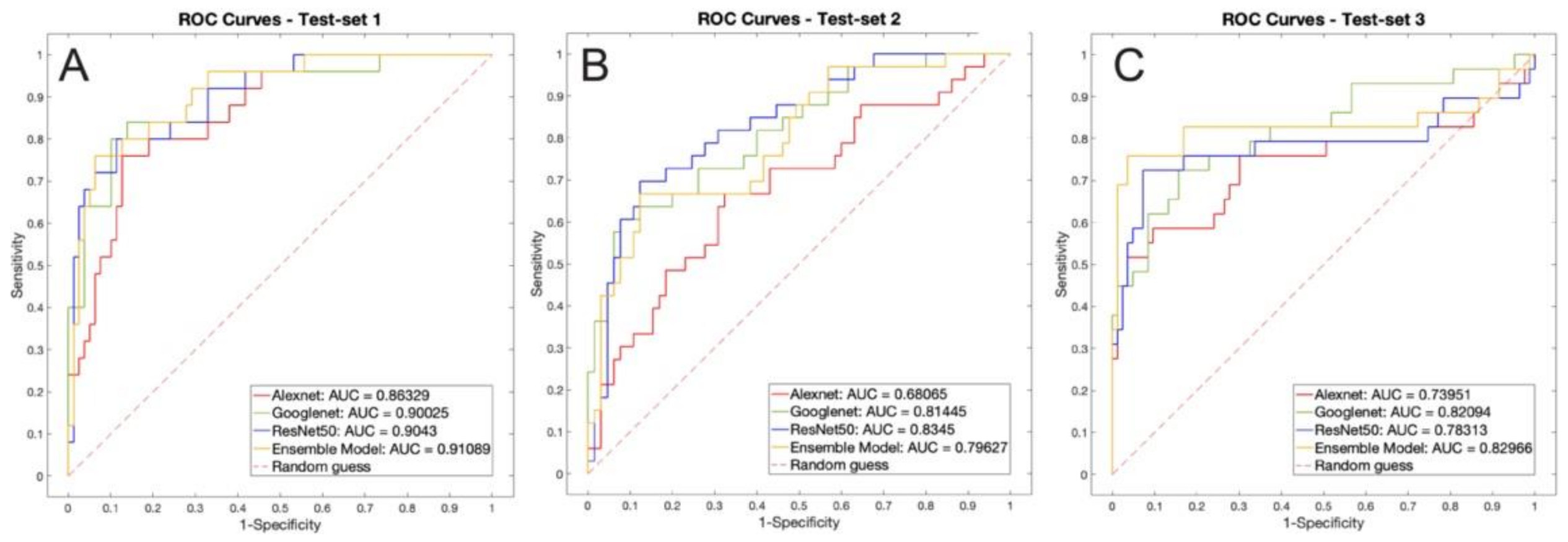
3.1. Performance on ISIC Images (Test Set 1)
3.2. Performance on Dermatoscope Images (Test Set 2)
3.3. Performance on NurugoTM Derma Images (Test Set 3)
4. Discussion
- (1)
- The FOV of the image was excessively restricted by the artifact caused by the glass.
- (2)
- The bubbles created by the interface liquid interfered with the image interpretation.
- (3)
- The use of the slide itself complicated image acquisition, rendering it more time consuming.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaliyadan, F.; Ramsey, M.L. Teledermatology. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Lee, J.J.; English, J.C., 3rd. Teledermatology: A Review and Update. Am. J. Clin. Dermatol. 2018, 19, 253–260. [Google Scholar] [CrossRef]
- Lipoff, J.B.; Cobos, G.; Kaddu, S.; Kovarik, C.L. The Africa Teledermatology Project: A retrospective case review of 1229 consultations from sub-Saharan Africa. J. Am. Acad. Dermatol. 2015, 72, 1084–1085. [Google Scholar] [CrossRef]
- Coates, S.J.; Kvedar, J.; Granstein, R.D. Teledermatology: From historical perspective to emerging techniques of the modern era: Part II: Emerging technologies in teledermatology, limitations and future directions. J. Am. Acad. Dermatol. 2015, 72, 577–586. [Google Scholar] [CrossRef]
- Börve, A.; Terstappen, K.; Sandberg, C.; Paoli, J. Mobile teledermoscopy-there’s an app for that! Dermatol. Pract. Concept 2013, 3, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Scalvenzi, M.; Fabbrocini, G. Teledermatology: A useful tool to fight COVID-19. J. Dermatol. Treat. 2020, 31, 325. [Google Scholar] [CrossRef] [Green Version]
- Lafolla, T. History of Telemedicine Infographic. Available online: https://blog.evisit.com/history-telemedicine-infographic (accessed on 10 May 2019).
- Tensen, E.; Van der Heijden, J.P.; Jaspers, M.W.; Witkamp, L. Two Decades of Teledermatology: Current Status and Integration in National Healthcare Systems. Curr. Dermatol. Rep. 2016, 5, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnane, A.; Dallest, K.; Janda, M.; Soyer, H.P. Teledermatology for the Diagnosis and Management of Skin Cancer. JAMA Dermatol. 2017, 153, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Romero, G.; Sanchez, P.; Garcia, M.; Cortina, P.; Vera, E.; Garrido, J.A. Randomized controlled trial comparing store-and-forward teledermatology alone and in combination with web-camera videoconferencing. Clin. Exp. Dermatol. 2010, 35, 311–377. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancerwith deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Hough, P. Method and Means for Recognizing Complex Patterns. U.S. Patent 3,069,654, 18 December 1962. [Google Scholar]
- Yilmaz, E.; Trocan, M. Benign and Malignant Skin Lesion Classification Comparison for Three Deep-Learning Architectures. In Intelligent Information and Database Systems; Springer International Switzerland Publishing: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Archivio ISIC. 2020. Available online: https://www.isic-archive.com/#!/topWithHeader/onlyHeaderTop/gallery (accessed on 15 March 2020).
- Glowacz, A.; Glowacz, Z. Recognition of images of finger skin with application of histogram, image filtration and K-NN classifier. Biocybern. Biomed. Eng. 2016, 36, 95–101. [Google Scholar] [CrossRef]
- Meiburger, K.M.; Savoia, P.; Molinari, F.; Veronese, F.; Tarantino, V.; Salvi, M.; Fadda, M.; Seoni, S.; Zavattaro, E.; De Santi, B.; et al. Automatic Extraction of Dermatological Parameters from Nevi Using an Inexpensive Smartphone Microscope: A Proof of Concept. In Proceedings of the 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 399–402. [Google Scholar] [CrossRef]
- Muñoz-López, C.; Ramírez-Cornejo, C.; Marchetti, M.A.; Han, S.S.; Del Barrio-Díaz, P.; Jaque, A.; Uribe, P.; Majerson, D.; Curi, M.; Del Puerto, C.; et al. Performance of a deep neural network in teledermatology: A single-centre prospective diagnostic study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 546–553. [Google Scholar] [CrossRef]
- Han, S.S.; Park, I.; Chang, S.E.; Lim, W.; Kim, M.S.; Park, G.H.; Chae, J.B.; Huh, C.H.; Na, J.-I. Augmented Intelligence Dermatology: Deep Neural Networks Empower Medical Professionals in Diagnosing Skin Cancer and Predicting Treatment Options for 134 Skin Disorders. J. Investig. Dermatol. 2020, 140, 1753–1761. [Google Scholar] [CrossRef]
- Navarrete-Dechent, C.; Dusza, S.W.; Liopyris, K.; Marghoob, A.A.; Halpern, A.C.; Marchetti, M.A. Automated Dermatological Diagnosis: Hype or Reality? J. Investig. Dermatol. 2018, 138, 2277–2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamel, S.A.; Haldeman, K.M.; Ely, H.; Kovarik, C.L.; Pak, H.; Armstrong, A.W. Application of mobile teledermatology for skin cancer screening. J. Am. Acad. Dermatol. 2012, 67, 576–581. [Google Scholar] [CrossRef]
- Houwink, E.J.F. Teledermatology in Norway using a mobile phone app. PLoS ONE 2020, 15, e0232131. [Google Scholar]
- Wolf, J.; Moreau, J.; Akilov, O.; Patton, T.; English, J.C.; Ho, J.; Ferris, L.K. Diagnostic Inaccuracy of Smart Phone Applications for Melanoma Detection. JAMA Dermatol. 2013, 149, 422–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walocko, F.M.; Tejasvi, T. Teledermatology Applications in Skin Cancer Diagnosis. Dermatol. Clin. 2017, 35, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Pathipati, A.S.; Ko, J.M. Implementation and evaluation of Stanford Health Care direct-care teledermatology program. SAGE Open Med. 2016, 4, 2050312116659089. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set Images | MN (Images) | MM (Images) | SK (Images) |
|---|---|---|---|
| Training-set | 200 | 200 | 200 |
| Test set 1 * | 35 | 25 | 37 |
| Test set 2 ° | 39 | 18 | 21 |
| Test set 3 § | 39 | 18 | 21 |
| Method | Accuracy | Sensitivity | Specificity | PV+ | PV− | F1 |
|---|---|---|---|---|---|---|
| D1 | 68.0% | 36.0% | 74.7% | 51.3% | 93.3% | 63.5% |
| D2 | 70.1% | 32.0% | 97.0% | 80.0% | 78.0% | 46.0% |
| D3 | 75.3% | 44.0% | 94.0% | 73.3% | 81.6% | 55.0% |
| Texture analysis | 48.5% | 44.0% | 66.7% | 37.9% | 72.0% | 40.7% |
| AlexNet | 76.0% | 80.0% | 77.6% | 54.1% | 92.2% | 64.5% |
| GoogleNet | 74.0% | 88.0% | 76.4% | 56.4% | 94.8% | 68.8% |
| ResNet | 74.0% | 80.0% | 77.3% | 54.1% | 92.0% | 64.5% |
| Ensemble model | 79.8% | 84.0% | 81.6% | 60.0% | 93.9% | 70.0% |
| Method | Accuracy | Sensitivity | Specificity | PV+ | PV− | F1 |
|---|---|---|---|---|---|---|
| D1 | 94.9% | 83.3% | 79.7% | 93.8% | 95.2% | 88.2% |
| D2 | 93.6% | 88.9% | 78.1% | 84.2% | 96.6% | 86.5% |
| D3 | 92.3% | 83.3% | 79.2% | 83.3% | 95.0% | 83.3% |
| Texture analysis | 31.6% | 21.1% | 53.3% | 25.0% | 48.0% | 22.9% |
| AlexNet | 56.1% | 69.7% | 52.5% | 44.2% | 76.2% | 54.1% |
| GoogleNet | 55.1% | 81.8% | 49.1% | 49.1% | 81.8% | 61.4% |
| ResNet | 70.4% | 72.7% | 79.0% | 66.7% | 83.3% | 69.6% |
| Ensemble model | 57.1% | 75.8% | 53.5% | 48.1% | 79.5% | 58.8% |
| Method | Accuracy | Sensitivity | Specificity | PV+ | PV− | F1 |
|---|---|---|---|---|---|---|
| D1 | 92.3% | 77.8% | 80.6% | 87.5% | 93.5% | 82.4% |
| D2 | 88.5% | 66.7% | 82.6% | 80.0% | 90.5% | 72.7% |
| D3 | 87.2% | 72.2% | 80.9% | 72.2% | 91.7% | 72.2% |
| Texture analysis | 48.4% | 48.3% | 50.7% | 27.4% | 71.7% | 35.0% |
| AlexNet | 67.9% | 58.6% | 85.5% | 63.0% | 83.1% | 60.7% |
| GoogleNet | 70.5% | 65.5% | 84.5% | 63.3% | 85.7% | 64.4% |
| ResNet | 75.9% | 69.0% | 90.3% | 74.1% | 87.8% | 71.4% |
| Ensemble model | 83.9% | 72.4% | 97.3% | 91.3% | 90.1% | 80.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veronese, F.; Branciforti, F.; Zavattaro, E.; Tarantino, V.; Romano, V.; Meiburger, K.M.; Salvi, M.; Seoni, S.; Savoia, P. The Role in Teledermoscopy of an Inexpensive and Easy-to-Use Smartphone Device for the Classification of Three Types of Skin Lesions Using Convolutional Neural Networks. Diagnostics 2021, 11, 451. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030451
Veronese F, Branciforti F, Zavattaro E, Tarantino V, Romano V, Meiburger KM, Salvi M, Seoni S, Savoia P. The Role in Teledermoscopy of an Inexpensive and Easy-to-Use Smartphone Device for the Classification of Three Types of Skin Lesions Using Convolutional Neural Networks. Diagnostics. 2021; 11(3):451. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030451
Chicago/Turabian StyleVeronese, Federica, Francesco Branciforti, Elisa Zavattaro, Vanessa Tarantino, Valentina Romano, Kristen M. Meiburger, Massimo Salvi, Silvia Seoni, and Paola Savoia. 2021. "The Role in Teledermoscopy of an Inexpensive and Easy-to-Use Smartphone Device for the Classification of Three Types of Skin Lesions Using Convolutional Neural Networks" Diagnostics 11, no. 3: 451. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11030451