
Dynamic Ultrasonographic Measurement of Inferior Joint Capsule Thickness in Patients with Unilateral Frozen Shoulder

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Subjects
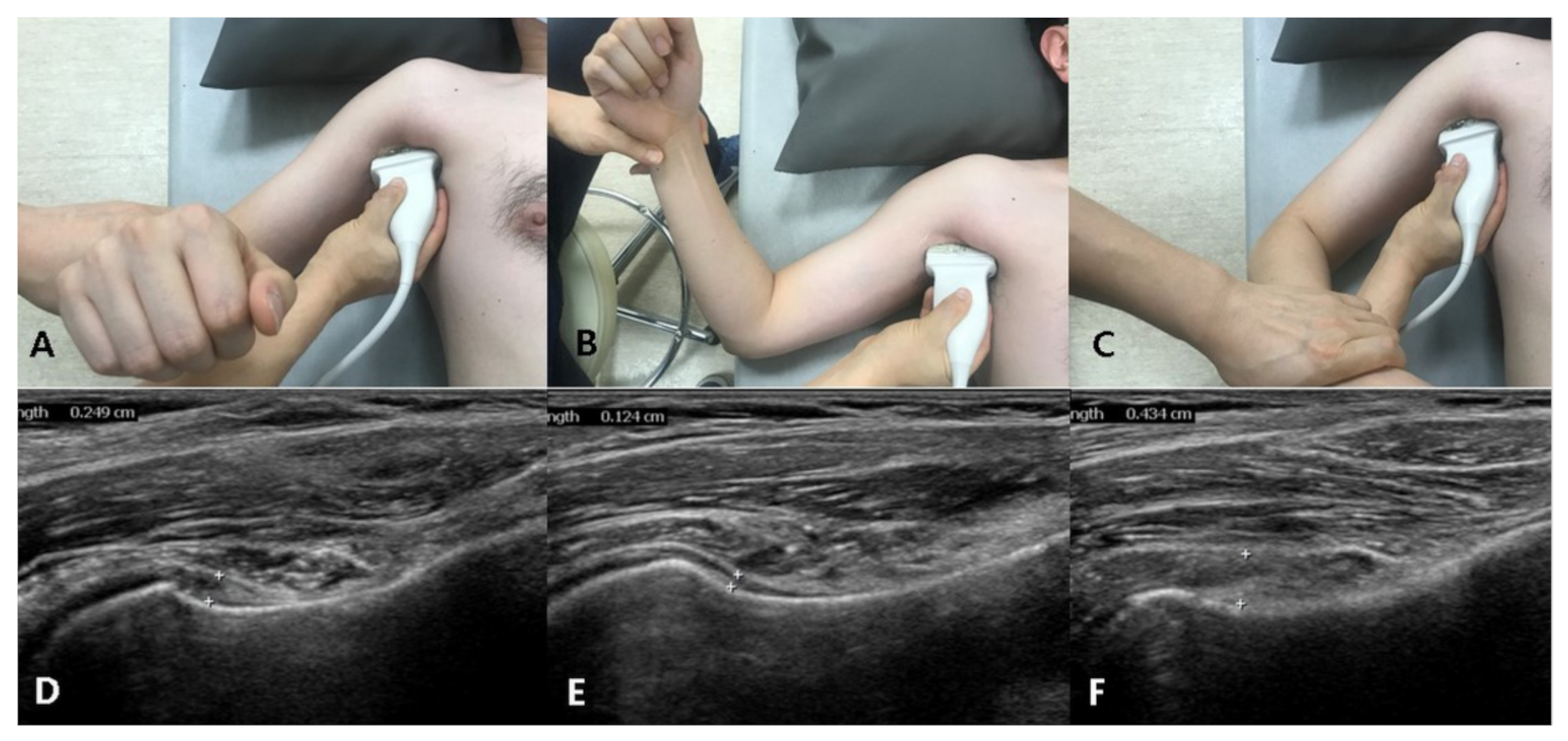
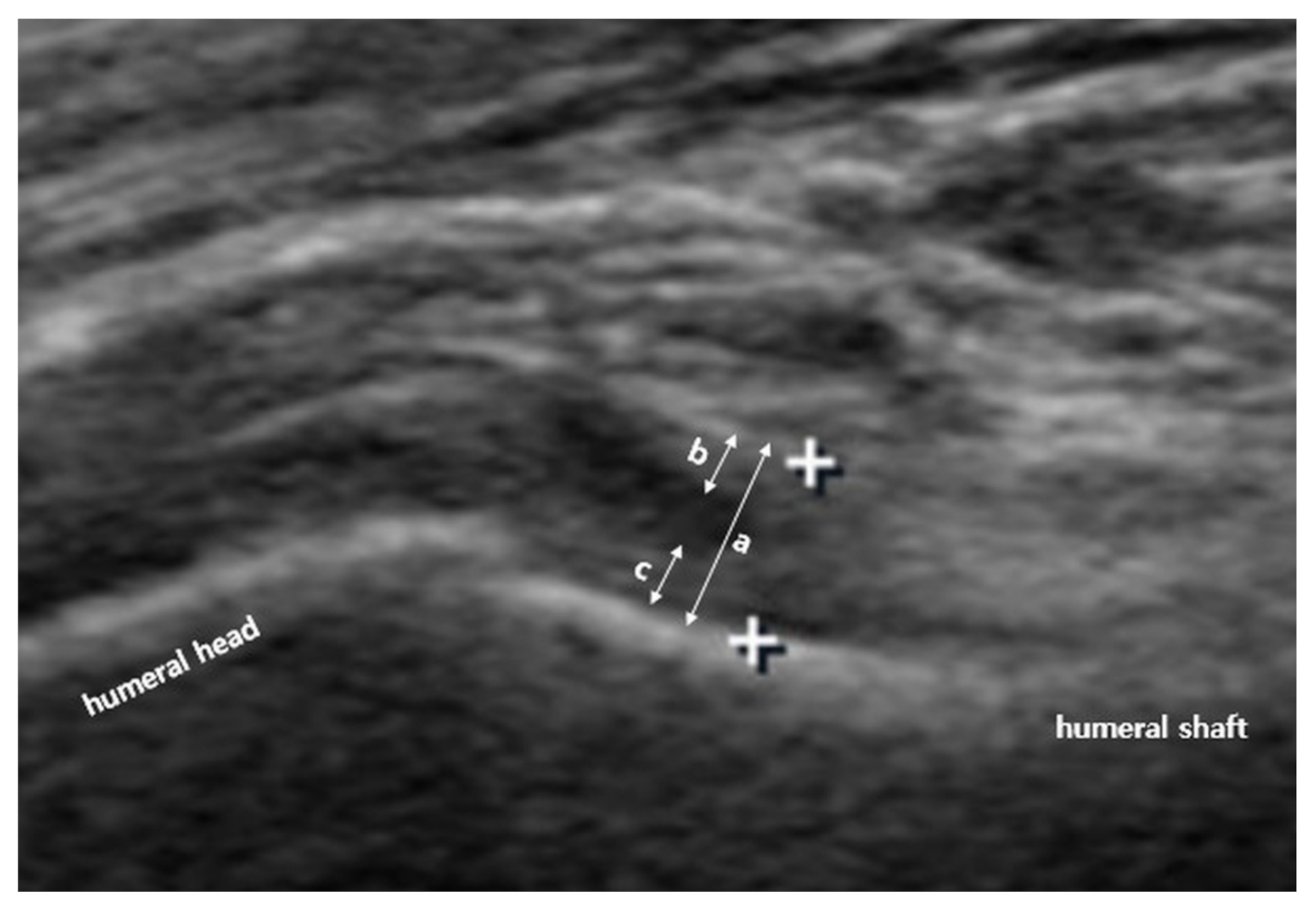
2.2. Us Protocol and Arm Positions
2.3. Range of Motion Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
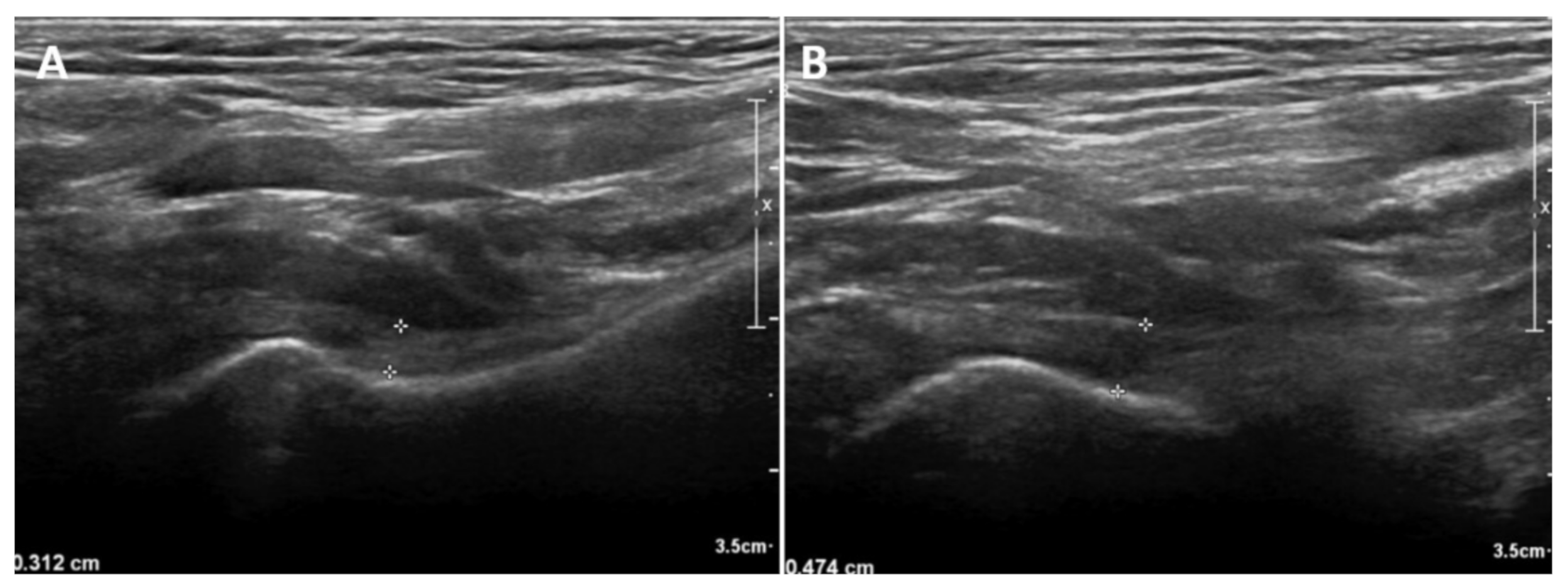
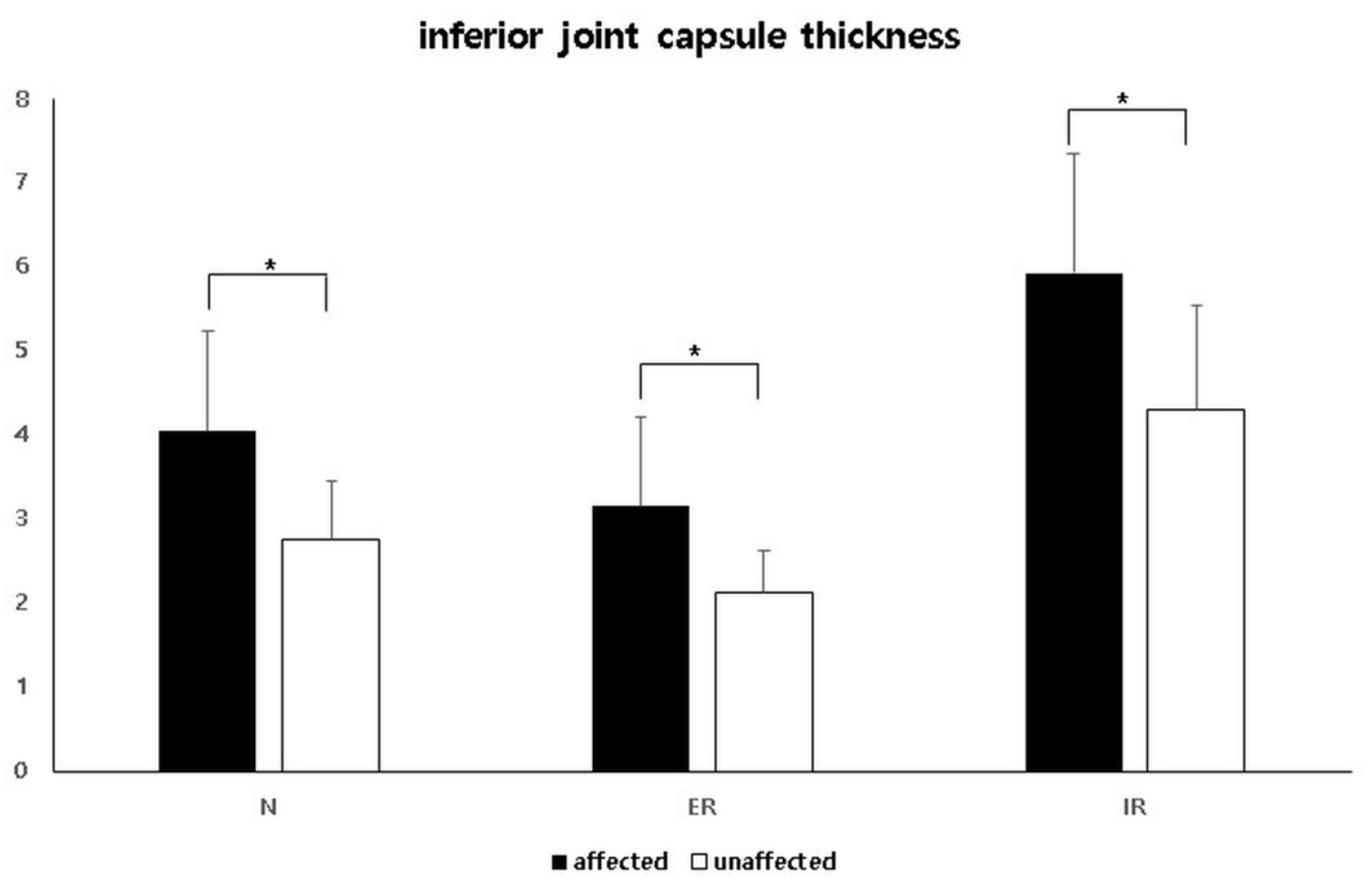
3.2. Comparison of the IJC Thickness on Us between the Affected and Unaffected Shoulders
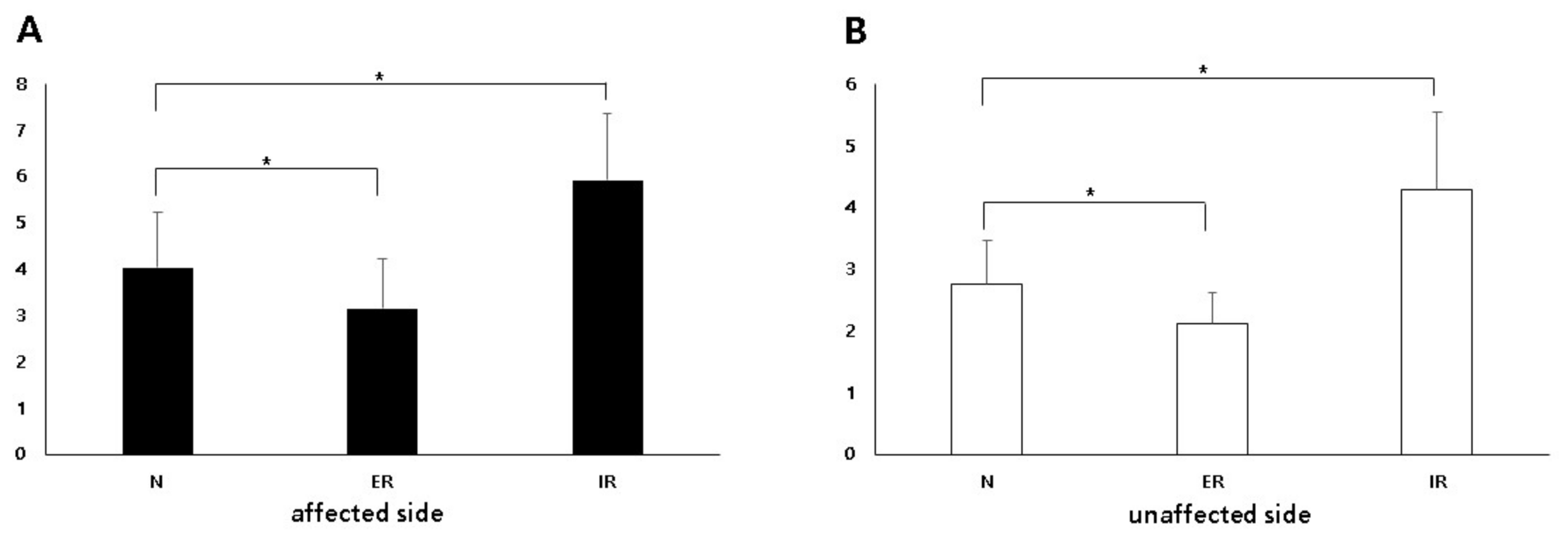
3.3. Comparison of the IJC Thickness on Us Depending on Arm Position
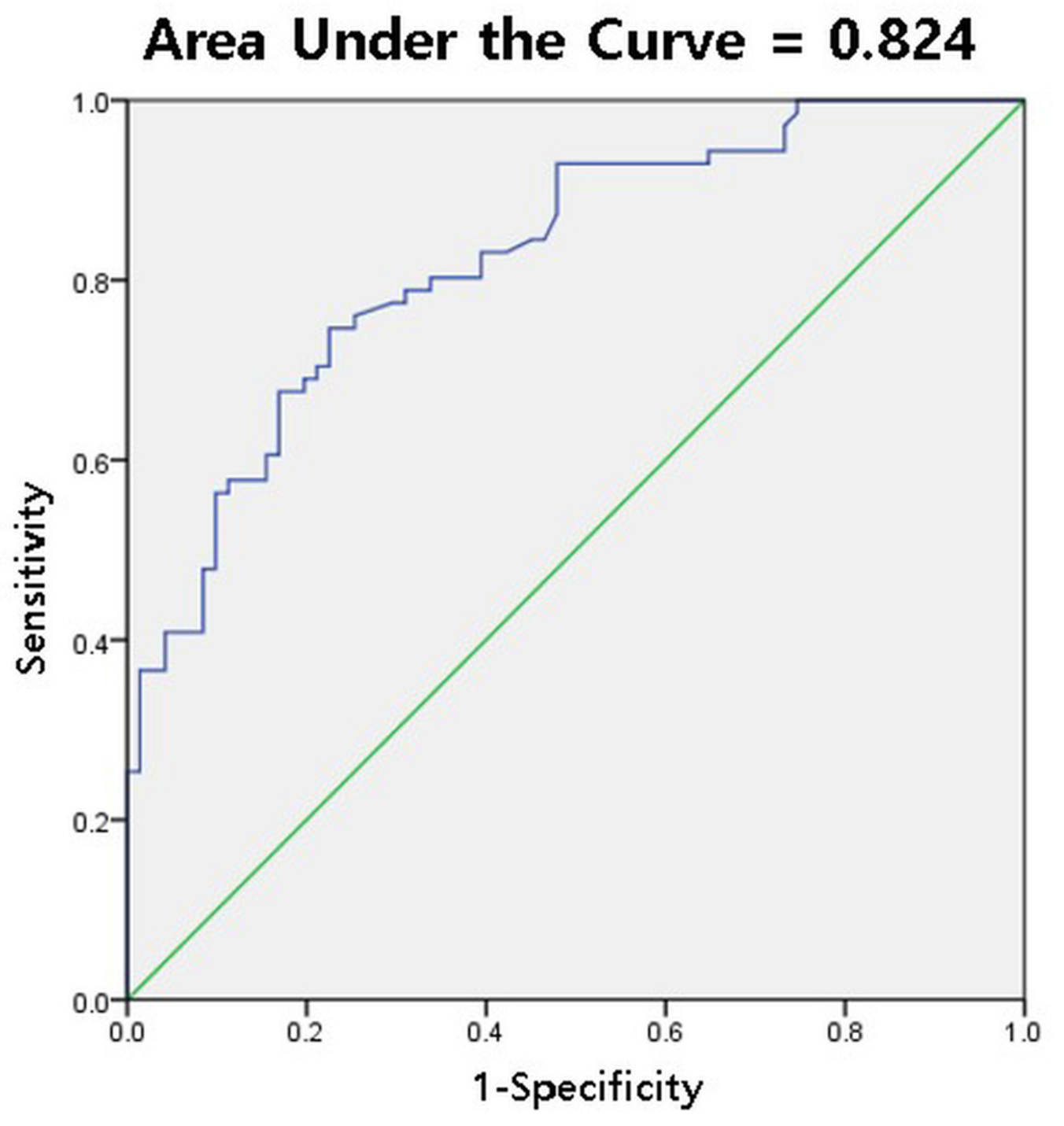
3.4. Diagnostic Cutoff Value for IJC Thickness on Us in the Neutral Position
3.5. Correlation between the Dynamic Change in IJC Thickness US and ROM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neviaser, A.S.; Hannafin, J.A. Adhesive Capsulitis. Am. J. Sports Med. 2010, 38, 2346–2356. [Google Scholar] [CrossRef]
- Brue, S.; Valentin, A.; Forssblad, M.; Werner, S.; Mikkelsen, C.; Cerulli, G. Idiopathic adhesive capsulitis of the shoulder: A review. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 1048–1054. [Google Scholar] [CrossRef]
- Hand, G.C.R.; Athanasou, N.A.; Matthews, T.; Carr, A.J. The pathology of frozen shoulder. J. Bone Jt. Surg. Br. Vol. 2007, 89, 928–932. [Google Scholar] [CrossRef] [Green Version]
- Hsu, J.E.; Anakwenze, O.A.; Warrender, W.J.; Abboud, J.A. Current review of adhesive capsulitis. J. Shoulder Elb. Surg. 2011, 20, 502–514. [Google Scholar] [CrossRef]
- Harris, G.; Bou-Haidar, P.; Harris, C. Adhesive capsulitis: Review of imaging and treatment. J. Med Imaging Radiat. Oncol. 2013, 57, 633–643. [Google Scholar] [CrossRef]
- Tamai, K.; Akutsu, M.; Yano, Y. Primary frozen shoulder: Brief review of pathology and imaging abnormalities. J. Orthop. Sci. 2014, 19, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.C.; Sykes, C.; Saifuddin, A.; Connell, D. Adhesive capsulitis: Sonographic changes in the rotator cuff interval with arthroscopic correlation. Skelet. Radiol. 2005, 34, 522–527. [Google Scholar] [CrossRef]
- Lefevre-Colau, M.-M.; Drapé, J.-L.; Fayad, F.; Rannou, F.; Diche, T.; Minvielle, F.; Demaille-Wlodyka, S.; Mayoux-Benhamou, M.-A.; Fermanian, J.; Poiraudeau, S.; et al. Magnetic resonance imaging of shoulders with idiopathic adhesive capsulitis: Reliability of measures. Eur. Radiol. 2005, 15, 2415–2422. [Google Scholar] [CrossRef]
- Sofka, C.M.; Ciavarra, G.A.; Hannafin, J.A.; Cordasco, F.A.; Potter, H.G. Magnetic Resonance Imaging of Adhesive Capsulitis: Correlation with Clinical Staging. HSS J. 2008, 4, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, K.-S.; Kang, C.H.; Oh, Y.-W.; Jeong, W.-K. Correlation between magnetic resonance imaging and clinical impairment in patients with adhesive capsulitis. Skelet. Radiol. 2012, 41, 1301–1308. [Google Scholar] [CrossRef]
- Ahn, K.-S.; Kang, C.H.; Kim, Y.; Jeong, W.-K. Diagnosis of adhesive capsulitis: Comparison of contrast-enhanced MRI with noncontrast-enhanced MRI. Clin. Imaging 2015, 39, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, D.-H.; Yoon, S.-H.; Lee, H.Y.; Kwack, K.-S. Evaluation of Adhesive Capsulitis of the Shoulder with Fat-Suppressed T2-Weighted MRI: Association Between Clinical Features and MRI Findings. Am. J. Roentgenol. 2016, 207, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mengiardi, B.; Pfirrmann, C.W.A.; Gerber, C.; Hodler, J.; Zanetti, M. Frozen Shoulder: MR Arthrographic Findings. Radiology 2004, 233, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.-Y.; Jee, W.-H.; Chun, H.J.; Kim, Y.-S.; Chung, Y.G.; Kim, J.-M. Adhesive capsulitis of the shoulder: Evaluation with MR arthrography. Eur. Radiol. 2006, 16, 791–796. [Google Scholar] [CrossRef]
- Michelin, P.; Delarue, Y.; Duparc, F.; Dacher, J.N. Thickening of the inferior glenohumeral capsule: An ultrasound sign for shoulder capsular contracture. Eur. Radiol. 2013, 23, 2802–2806. [Google Scholar] [CrossRef]
- Kim, D.H.; Cho, C.-H.; Sung, D.H. Ultrasound measurements of axillary recess capsule thickness in unilateral frozen shoulder: Study of correlation with MRI measurements. Skelet. Radiol. 2018, 47, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Sconfienza, L.M.; Albano, D.; Allen, G.; Bazzocchi, A.; Bignotti, B.; Chianca, V.; De Castro, F.F.; Drakonaki, E.E.; Gallardo, E.; Gielen, J.; et al. Clinical indications for musculoskeletal ultrasound updated in 2017 by European Society of Musculoskeletal Radiology (ESSR) consensus. Eur. Radiol. 2018, 28, 5338–5351. [Google Scholar] [CrossRef]
- Ferrari, D.A. Capsular ligaments of the shoulder. Anatomical and functional study of the anterior superior capsule. Am. J. Sports Med. 1990, 18, 20–24. [Google Scholar] [CrossRef]
- Terry, G.C.; Hammon, D.; France, P.; Norwood, L.A. The stabilizing function of passive shoulder restraints. Am. J. Sports Med. 1991, 19, 26–34. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Kanazawa, K.; Ando, A.; Sekiguchi, T.; Koide, M.; Yabe, Y.; Suzuki, K.; Itoi, E. Effects of joint capsular release on range of motion in patients with frozen shoulder. J. Shoulder Elb. Surg. 2020, 29, 1836–1842. [Google Scholar] [CrossRef]
- Sernik, R.A.; Leão, R.V.; Bizetto, E.L.; Damasceno, R.S.; Horvat, N.; Cerri, G.G. Thickening of the axillary recess capsule on ultrasound correlates with magnetic resonance imaging signs of adhesive capsulitis. Ultrasound 2019, 27, 183–190. [Google Scholar] [CrossRef]
- Cheng, X.; Zhang, Z.; Xuanyan, G.; Li, T.; Li, J.; Yin, L.; Lu, M. Adhesive Capsulitis of the Shoulder: Evaluation With US-Arthrography Using a Sonographic Contrast Agent. Sci. Rep. 2017, 7, 5551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homsi, C.; Bordalo-Rodrigues, M.; Da Silva, J.J.; Stump, X.M.G.R.G. Ultrasound in adhesive capsulitis of the shoulder: Is assessment of the coracohumeral ligament a valuable diagnostic tool? Skelet. Radiol. 2006, 35, 673–678. [Google Scholar] [CrossRef]
- Ryu, K.N.; Lee, S.W.; Rhee, Y.G.; Lim, J.H. Adhesive capsulitis of the shoulder joint: Usefulness of dynamic sonography. J. Ultrasound Med. 1993, 12, 445–449. [Google Scholar] [CrossRef]
- Tandon, A.; Dewan, S.; Bhatt, S.; Jain, A.K.; Kumari, R. Sonography in diagnosis of adhesive capsulitis of the shoulder: A case–control study. J. Ultrasound 2017, 20, 227–236. [Google Scholar] [CrossRef]
- Walmsley, S.; Osmotherly, P.G.; Walker, C.J.; Rivett, D.A. Power Doppler Ultrasonography in the Early Diagnosis of Primary/Idiopathic Adhesive Capsulitis: An Exploratory Study. J. Manip. Physiol. Ther. 2013, 36, 428–435. [Google Scholar] [CrossRef]
- Jung, J.H.; Kim, D.H.; Yi, J.; Cho, C.-H.; Kim, D.-H. Determination of magnetic resonance imaging criteria for diagnosis of adhesive capsulitis. Rheumatol. Int. 2019, 39, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, S.; Li, Y.; Hua, Y.; Li, H. Is the Extended Release of the Inferior Glenohumeral Ligament Necessary for Frozen Shoulder? Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Lee, D.G.; Lee, S.; Kim, D.H. Ultrasonographic Measurement of the Thickness of Axillary Recess Capsule in Healthy Volunteers. Ann. Rehabilit. Med. 2016, 40, 502–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Number of patients | 71 |
| Mean age, years | 58.2 ± 9.9 |
| Sex: male, female | 26, 45 |
| Duration of symptoms, months (range) | 6.7 ± 3.2 (3–14) |
| Number of diabetic patients | 8 |
| Forward flexion (°) | 115.6 ± 18.4 |
| Abduction (°) | 96.8 ± 20.2 |
| External rotation (°) | 40.1 ± 11.3 |
| Internal rotation score | 16.7 ± 2.1 |
| N | ER | IR | p-Value (N vs. ER) | p-Value (N vs. IR) | p-Value (Affected vs. Unaffected) | |
|---|---|---|---|---|---|---|
| Affected side | 4.04 ± 1.19 | 3.15 ± 1.07 | 5.92 ± 1.43 | <0.001 | <0.001 | N: <0.001, ER: <0.001, IR: <0.001 |
| Unaffected side | 2.76 ± 0.70 | 2.12 ± 0.50 | 4.30 ± 1.24 | <0.001 | <0.001 |
| IJC Thickness (mm) | Sensitivity | Specificity | Youden Index |
|---|---|---|---|
| 3.0 | 77.5% | 69.0% | 0.465 |
| 3.2 | 73.2% | 77.5% | 0.507 |
| 3.5 | 66.2% | 83.1% | 0.493 |
| ΔIJCER | ΔIJCIR | |||
|---|---|---|---|---|
| r | p | r | p | |
| Forward flexion | 0.259 | 0.020* | 0.023 | 0.849 |
| Abduction | 0.116 | 0.336 | 0.056 | 0.644 |
| External rotation | 0.165 | 0.168 | 0.150 | 0.212 |
| Internal rotation | −0.114 | 0.346 | 0.135 | 0.262 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-G.; Peo, H.; Cho, J.-H.; Cho, C.-H.; Kim, D.-K.; Kim, D.-H. Dynamic Ultrasonographic Measurement of Inferior Joint Capsule Thickness in Patients with Unilateral Frozen Shoulder. Diagnostics 2021, 11, 898. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050898
Lee J-G, Peo H, Cho J-H, Cho C-H, Kim D-K, Kim D-H. Dynamic Ultrasonographic Measurement of Inferior Joint Capsule Thickness in Patients with Unilateral Frozen Shoulder. Diagnostics. 2021; 11(5):898. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050898
Chicago/Turabian StyleLee, Jun-Gyu, Hyungsun Peo, Jang-Hyuk Cho, Chul-Hyun Cho, Don-Kyu Kim, and Du-Hwan Kim. 2021. "Dynamic Ultrasonographic Measurement of Inferior Joint Capsule Thickness in Patients with Unilateral Frozen Shoulder" Diagnostics 11, no. 5: 898. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050898