
Serum Anti-Collagen IV IgM and IgG Antibodies as Indicators of Low Vascular Turnover of Collagen IV in Patients with Long-Term Complications of Type 2 Diabetes



Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Population
2.2. Screening of the Patients and Controls
2.3. Immunological and Biochemical Assays
2.3.1. Determination of ACIVAbs IgM and ACIVAbs IgG
2.3.2. Determination of CIV-DP
2.3.3. Determination of CIC-CIV
2.3.4. Determination of Free ACIVAbs
2.3.5. Determination of MMP-2 and MMP-9
2.3.6. Biochemical Analysis
2.4. Clinical Tests and Procedures
2.5. Statistical Analysis
3. Results
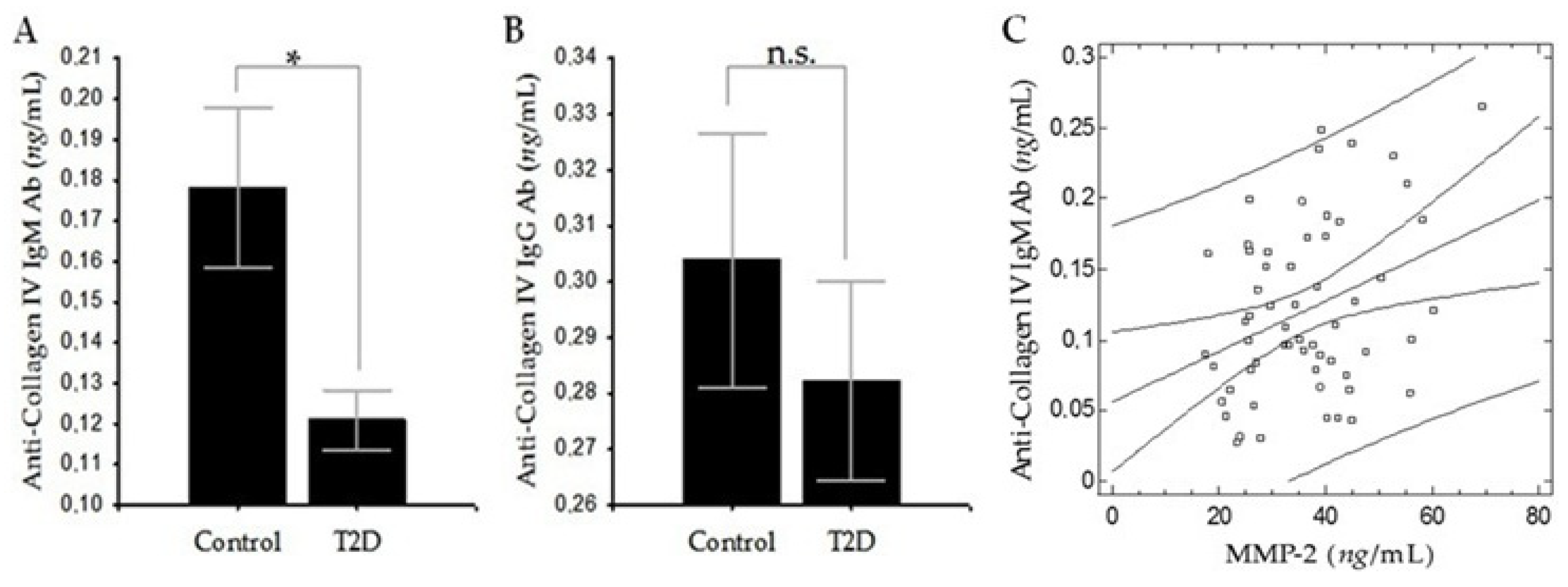
3.1. Comparison of the Levels of ACIVAbs IgM and ACIVAbs IgG between the T2D and Control Groups
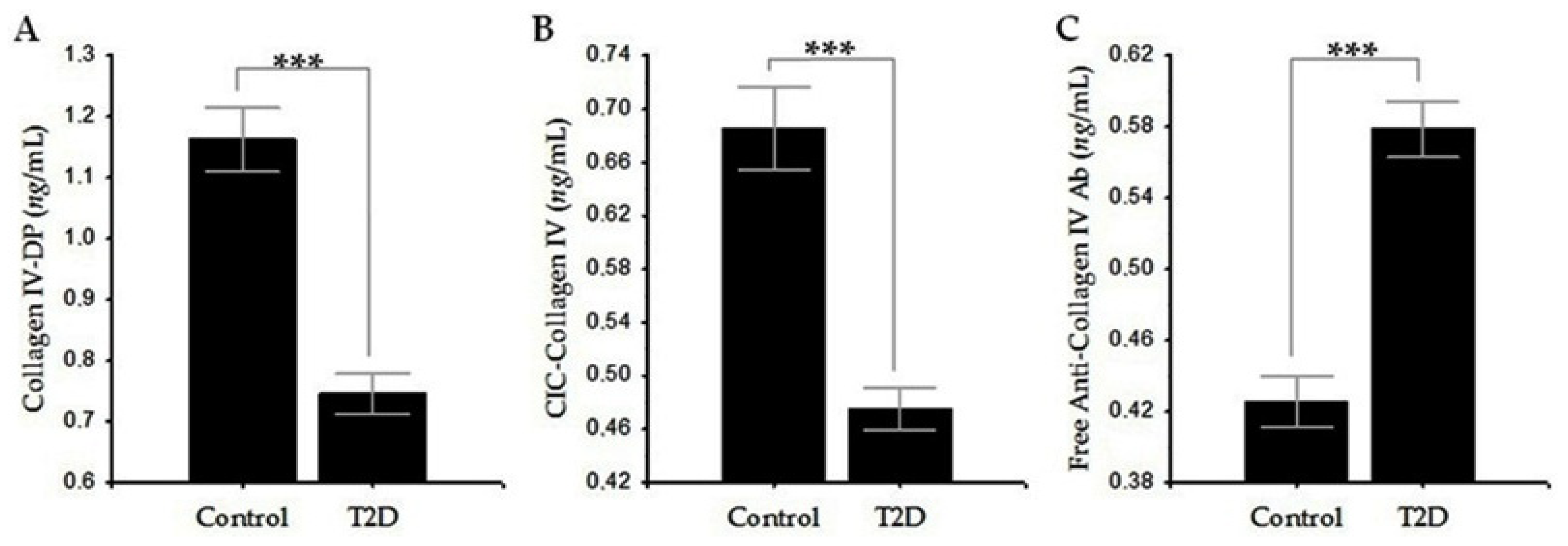
3.2. Comparison of the Levels of CIV-DP, CIC-CIV, and Free ACIVAbs IgG between the T2D and Control Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, N.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF diabetes atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, T.; Heile, M. Type 2 diabetes in the US managed care setting: The burden of disease and rationale for an oral glucagon-like peptide-1 receptor agonist. Am. J. Manag. Care 2020, 26, S325–S334. [Google Scholar] [PubMed]
- Bachmann, K.N.; Wang, T.J. Biomarkers of cardiovascular disease: Contributions to risk prediction in individuals with diabetes. Diabetologia 2018, 61, 987–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzapfel, G.A. Collagen in arterial walls: Biomechanical aspects. In Collagen; Springer: New York, NY, USA, 2008; pp. 285–324. [Google Scholar]
- Wang, Y.; Zeinali-Davarani, S.; Zhang, Y. Arterial mechanics considering the structural and mechanical contributions of ECM constituents. J. Biomech. 2016, 49, 2358–2365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makino, H.; Shikata, K.; Wieslander, J.; Wada, J.; Kashihara, N.; Yoshioka, K.; Ota, Z. Localization of fibril/microfibril and basement membrane collagens in diabetic glomerulosclerosis in type 2 diabetes. Diabet. Med. 1994, 11, 304–311. [Google Scholar] [CrossRef]
- Ljubimov, A.V.; Burgeson, R.E.; Butkowski, R.J.; Couchman, J.R.; Zardi, L.; Ninomiya, Y.; Sado, Y.; Huang, Z.S.; Nesburn, A.B.; Kenney, M.C. Basement membrane abnormalities in human eyes with diabetic retinopathy. J. Histochem. Cytochem. 1996, 44, 1469–1479. [Google Scholar] [CrossRef]
- Roy, S.; Maiello, M.; Lorenzi, M. Increased expression of basement membrane collagen in human diabetic retinopathy. J. Clin. Investig. 1994, 93, 438–442. [Google Scholar] [CrossRef]
- Inukai, T.; Fujiwara, Y.; Tayama, K.; Aso, Y.; Takemura, Y. Serum levels of carboxy-terminal propeptide of human type I procollagen are an indicator for the progression of diabetic nephropathy in patients with Type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2000, 48, 23–28. [Google Scholar] [CrossRef]
- Kotajima, N.; Kimura, T.; Kanda, T.; Obata, K.; Kuwabara, A.; Fukumura, Y.; Kobayashi, I. Type IV collagen as an early marker for diabetic nephropathy in non-insulin-dependent diabetes mellitus. J. Diabetes Complicat. 2000, 14, 13–17. [Google Scholar] [CrossRef]
- Xu, X.; Wu, Z.; Zhou, Q.; Zhang, Y.; Wu, D. The role of determining the levels of serum collagen type IV in diagnosing early diabetic nephropathy. Ren. Fail. 2002, 24, 747–753. [Google Scholar] [CrossRef]
- Yano, Y.; Ura, H.; Sumida, Y.; Gabazza, E.C.; Misaki, M.; Shima, T. Serum 7S domain of type IV collagen levels in essential hypertension and hypertensive type 2 diabetic patients. Diabet. Med. 1997, 14, 466–471. [Google Scholar] [CrossRef]
- Nicoloff, G.; Baydanoff, S.; Petrova, C.; Christova, P. Serum antibodies to collagen type IV and development of diabetic vascular complications in children with type 1 (insulin-dependent) diabetes mellitus: A longitudinal study. Vascul. Pharmacol. 2002, 38, 143–147. [Google Scholar] [CrossRef]
- Nikolov, A.G.; Nicoloff, G.; Tsinlikov, I.; Tsinlikova, I. Anti-collagen type IV antibodies and the development of microvascular complications in diabetic patients with arterial hypertension. J. IMAB 2012, 18, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Kostov, K.; Blazhev, A. Use of glycated hemoglobin (A1c) as a biomarker for vascular risk in type 2 diabetes: Its relationship with matrix metalloproteinases-2,-9 and the metabolism of collagen IV and elastin. Medicina 2020, 56, 231. [Google Scholar] [CrossRef] [PubMed]
- Nicoloff, G.; Blazhev, A.; Petrova, C.; Christova, P. Circulating immune complexes among diabetic children. Clin. Dev. Immunol. 2004, 11, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekiguchi, R.; Yamada, K.M. Basement membranes in development and disease. Curr. Top. Dev. Biol. 2018, 130, 143–191. [Google Scholar] [PubMed]
- Roy, S.; Kim, D. Retinal capillary basement membrane thickening: Role in the pathogenesis of diabetic retinopathy. Prog. Retin. Eye Res. 2020, 9, 100903. [Google Scholar] [CrossRef]
- Halfter, W.; Moes, S.; Asgeirsson, D.O.; Halfter, K.; Oertle, P.; Herraiz, E.M.; Plodinec, M.; Jenoe, P.; Henrich, P.B. Diabetes-related changes in the protein composition and the biomechanical properties of human retinal vascular basement membranes. PLoS ONE 2018, 13, e0195772. [Google Scholar] [CrossRef] [Green Version]
- Marshall, C.B. Rethinking glomerular basement membrane thickening in diabetic nephropathy: Adaptive or pathogenic? Am. J. Physiol. Ren. Physiol. 2016, 311, F831–F843. [Google Scholar] [CrossRef] [Green Version]
- Steffensen, L.B.; Rasmussen, L.M. A role for collagen type IV in cardiovascular disease? Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H610–H625. [Google Scholar] [CrossRef]
- Kalluri, R. Basement membranes: Structure, assembly and role in tumour angiogenesis. Nat. Rev. Cancer 2003, 3, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.R.; Sowers, J.R.; Tyagi, S.C. The central role of vascular extracellular matrix and basement membrane remodeling in metabolic syndrome and type 2 diabetes: The matrix preloaded. Cardiovasc. Diabetol. 2005, 4, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Hudson, B.G.; Reeders, S.T.; Tryggvason, K. Type IV collagen: Structure, gene organization, and role in human diseases: Molecular basis of Goodpasture and Alport syndromes and diffuse leiomyomatosis. J. Biol. Chem. 1993, 268, 26033–26036. [Google Scholar] [CrossRef]
- Khoshnoodi, J.; Pedchenko, V.; Hudson, B.G. Mammalian collagen IV. Microsc. Res. Tech. 2008, 71, 357–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mk, G.; Ra, H. Collagens. Cell Tissue Res. 2010, 339, 247–257. [Google Scholar]
- Thomsen, M.S.; Routhe, L.J.; Moos, T. The vascular basement membrane in the healthy and pathological brain. J. Cereb. Blood Flow Metab. 2017, 37, 3300–3317. [Google Scholar] [CrossRef] [PubMed]
- Borza, D.B.; Chedid, M.F.; Colon, S.; Lager, D.J.; Leung, N.; Fervenza, F.C. Recurrent Goodpasture’s disease secondary to a monoclonal IgA1-κ antibody autoreactive with the α1/α2 chains of type IV collagen. Am. J. Kidney Dis. 2005, 45, 397–406. [Google Scholar] [CrossRef]
- McLeod, O.; Dunér, P.; Samnegård, A.; Tornvall, P.; Nilsson, J.; Hamsten, A.; Bengtsson, E. Autoantibodies against basement membrane collagen type IV are associated with myocardial infarction. Int. J. Cardiol. Heart Vasc. 2015, 6, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Wang, L.; Li, Y.; Liu, S.; Li, J.; Wang, H.; Huang, H. High ambient glucose levels modulates the production of MMP-9 and a5 (IV) collagen by cultured podocytes. Cell Physiol. Biochem. 2006, 17, 57–68. [Google Scholar] [CrossRef]
- Monaco, S.; Sparano, V.; Gioia, M.; Sbardella, D.; di Pierro, D.; Marini, S.; Coletta, M. Enzymatic processing of collagen IV by MMP-2 (gelatinase A) affects neutrophil migration and it is modulated by extracatalytic domains. Protein Sci. 2006, 15, 2805–2815. [Google Scholar] [CrossRef] [Green Version]
- Nikolov, A.; Tsinlikov, I.; Tsinlikova, I.; Nicoloff, G.; Blazhev, A.; Garev, A. Serum anti-collagen type IV IgM antibodies and development of diabetic nephropathy in diabetics with essential hypertension. Cent. Eur. J. Immunol. 2016, 41, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolov, A.; Tzekova, M.; Blazhev, A. Relationship between lipid indices, type IV collagen turnover and the development of microvascular complications in diabetic patients with arterial hypertension. Folia Med. 2019, 61, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Nicoloff, G.; Blazhev, A.; Petrova, C.; Christova, P.; Jordanova-Laleva, P.; Dekov, D.; Dorovski, P. Detection of free antielastin antibodies among diabetic children. J. Investig. Med. 2005, 53, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Ha, J.; Trudeau, K.; Beglova, E. Vascular basement membrane thickening in diabetic retinopathy. Curr. Eye Res. 2010, 35, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Tsilibary, E.C. Microvascular basement membranes in diabetes mellitus. J. Pathol. 2003, 200, 537–546. [Google Scholar] [CrossRef]
- Kuiper, E.J.; van Zijderveld, R.; Roestenberg, P.; Lyons, K.M.; Goldschmeding, R.; Klaassen, I.; van Noorden, C.J.; Schlingemann, R.O. Connective tissue growth factor is necessary for retinal capillary basal lamina thickening in diabetic mice. J. Histochem. Cytochem. 2008, 56, 785–792. [Google Scholar] [CrossRef] [Green Version]
- To, M.; Goz, A.; Camenzind, L.; Oertle, P.; Candiello, J.; Sullivan, M.; Henrich, P.B.; Loparic, M.; Safi, F.; Eller, A.; et al. Diabetes-induced morphological, biomechanical, and compositional changes in ocular basement membranes. Exp. Eye Res. 2013, 116, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Ziyadeh, F.N. Renal tubular basement membrane and collagen type IV in diabetes mellitus. Kidney Int. 1993, 43, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, T.; Giardino, I.; Edelstein, D.; Brownlee, M. Changes in diabetic retinal matrix protein mRNA levels in a common transgenic mouse strain. Curr. Eye Res. 2000, 21, 581–587. [Google Scholar] [CrossRef]
- Liu, D.; Razzaque, M.S.; Cheng, M.; Taguchi, T. The renal expression of heat shock protein 47 and collagens in acute and chronic experimental diabetes in rats. Histochem. J. 2001, 33, 621–628. [Google Scholar] [CrossRef]
- Iglesias-de la Cruz, M.C.; Ziyadeh, F.N.; Isono, M.; Kouahou, M.; Han, D.C.; Kalluri, R.; Mundel, P.; Chen, S. Effects of high glucose and TGF-β1 on the expression of collagen IV and vascular endothelial growth factor in mouse podocytes. Kidney Int. 2002, 62, 901–913. [Google Scholar] [CrossRef] [Green Version]
- Derosa, G.; Avanzini, M.A.; Geroldi, D.; Fogari, R.; Lorini, R.; de Silvestri, A.; Tinelli, C.; d’Annunzio, G. Matrix metalloproteinase 2 may be a marker of microangiopathy in children and adolescents with type 1 diabetes. Diabetes Care 2004, 27, 273–275. [Google Scholar] [CrossRef] [Green Version]
- Uemura, S.; Matsushita, H.; Li, W.; Glassford, A.J.; Asagami, T.; Lee, K.H.; Harrison, D.G.; Tsao, P.S. Diabetes mellitus enhances vascular matrix metalloproteinase activity: Role of oxidative stress. Circ. Res. 2001, 88, 1291–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeters, S.A.; Engelen, L.; Buijs, J.; Chaturvedi, N.; Fuller, J.H.; Schalkwijk, C.G.; Stehouwer, C.D. Plasma levels of matrix metalloproteinase-2,-3,-10, and tissue inhibitor of metalloproteinase-1 are associated with vascular complications in patients with type 1 diabetes: The EURODIAB prospective complications study. Cardiovasc. Diabetol. 2015, 14, 1–10. [Google Scholar]
- Jacqueminet, S.; Abdesselam, O.B.; Chapman, M.J.; Nicolay, N.; Foglietti, M.J.; Grimaldi, A.; Beaudeux, J.L. Elevated circulating levels of matrix metalloproteinase-9 in type 1 diabetic patients with and without retinopathy. Clin. Chim. Acta 2006, 367, 103–107. [Google Scholar] [CrossRef]
- Jayashree, K.; Yasir, M.; Senthilkumar, G.P.; Babu, K.R.; Mehalingam, V.; Mohanraj, P.S. Circulating matrix modulators (MMP-9 and TIMP-1) and their association with severity of diabetic retinopathy. Diabetes Metab. Syndr. 2018, 12, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Thrailkill, K.M.; Bunn, R.C.; Moreau, C.S.; Cockrell, G.E.; Simpson, P.M.; Coleman, H.N.; Frindik, J.P.; Kemp, S.F.; Fowlkes, J.L. Matrix metalloproteinase-2 dysregulation in type 1 diabetes. Diabetes Care 2007, 30, 2321–2326. [Google Scholar] [CrossRef] [Green Version]
- Rogowicz, A.; Zozulinska, D.; Wierusz-Wysocka, B. The role of matrix metalloproteinases in the development of vascular complications of diabetes mellitus-clinical implications. Polskie Archiwum Medycyny Wewnetrznej 2007, 117, 43. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, S.S.; Malaponte, G.; Libra, M.; di Pino, L.; Celotta, G.; Bevelacqua, V.; Petrina, M.; Nicotra, G.S.; Indelicato, M.; Navolanic, P.M.; et al. Plasma levels and zymographic activities of matrix metalloproteinases 2 and 9 in type II diabetics with peripheral arterial disease. Vasc. Med. 2005, 10, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostov, K.; Blazhev, A.; Atanasova, M.; Dimitrova, A. Serum concentrations of endothelin-1 and matrix metalloproteinases-2,-9 in pre-hypertensive and hypertensive patients with type 2 diabetes. Int. J. Mol. Sci. 2016, 17, 1182. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Healthy Control Subjects | Patients with T2D |
|---|---|---|
| (n = 20) | (n = 59) | |
| Men, n (%) | 10 (50.0) | 25 (42.0) |
| Women, n (%) | 10 (50.0) | 34 (58.0) |
| Age, years 1 | 61.5 ± 11.4 | 60.8 ± 14.7 |
| Duration of T2D 1 | N/A 2 | 10.1 ± 7.8 |
| SBP, mmHg 1 | 121.5 ± 8.6 | 149.2 ±16.7 *** |
| DBP, mmHg 1 | 78.2 ± 7.5 | 83.0 ± 10.4 |
| BMI, kg/m2 1 | 24.9 ± 2.4 | 28.4 ± 4.5 *** |
| Smokers, n (%) | 4 (20) | 9 (15) |
| HbA1c (%) 1 | N/A 2 | 7.5 ± 1.8 |
| TC, mmol/L 1 | 4.2 ± 0.7 | 5.2 ± 1.8 * |
| LDL-C, mmol/L 1 | 2.8 ± 0.8 | 3.0 ± 1.1 |
| HDL-C, mmol/L 1 | 1.2 ± 0.2 | 1.0 ± 0.3 *** |
| TG, mmol/L 1 | 1.4 ± 0.4 | 2.7 ± 3.0 |
| CRP, mg/L 1 | 1.1 ± 0.9 | 8.4 ± 7.9 *** |
| MMP-2, ng/mL 1 | 30.68 ± 8.4 | 36.22 ± 11.5 * |
| MMP-9, ng/mL 1 | 25.84 ± 12.7 | 38.48 ± 20.7 ** |
| Neuropathy, n (%) | N/A 2 | 8 (14.0) |
| Microangiopathy, n (%) | N/A 2 | 50 (85.0) |
| Macroangiopathy, n (%) | N/A 2 | 18 (31.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostov, K.; Blazhev, A. Serum Anti-Collagen IV IgM and IgG Antibodies as Indicators of Low Vascular Turnover of Collagen IV in Patients with Long-Term Complications of Type 2 Diabetes. Diagnostics 2021, 11, 900. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050900
Kostov K, Blazhev A. Serum Anti-Collagen IV IgM and IgG Antibodies as Indicators of Low Vascular Turnover of Collagen IV in Patients with Long-Term Complications of Type 2 Diabetes. Diagnostics. 2021; 11(5):900. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050900
Chicago/Turabian StyleKostov, Krasimir, and Alexander Blazhev. 2021. "Serum Anti-Collagen IV IgM and IgG Antibodies as Indicators of Low Vascular Turnover of Collagen IV in Patients with Long-Term Complications of Type 2 Diabetes" Diagnostics 11, no. 5: 900. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050900