
Diagnostic Yield and Cost-Effectiveness of “Dynamic” Exome Analysis in Epilepsy with Neurodevelopmental Disorders: A Tertiary-Center Experience in Northern Italy

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Phenotyping
2.2. Genetic Workup
2.3. Costs
2.4. Plan of Analysis
3. Results
3.1. Demographics and Phenotype
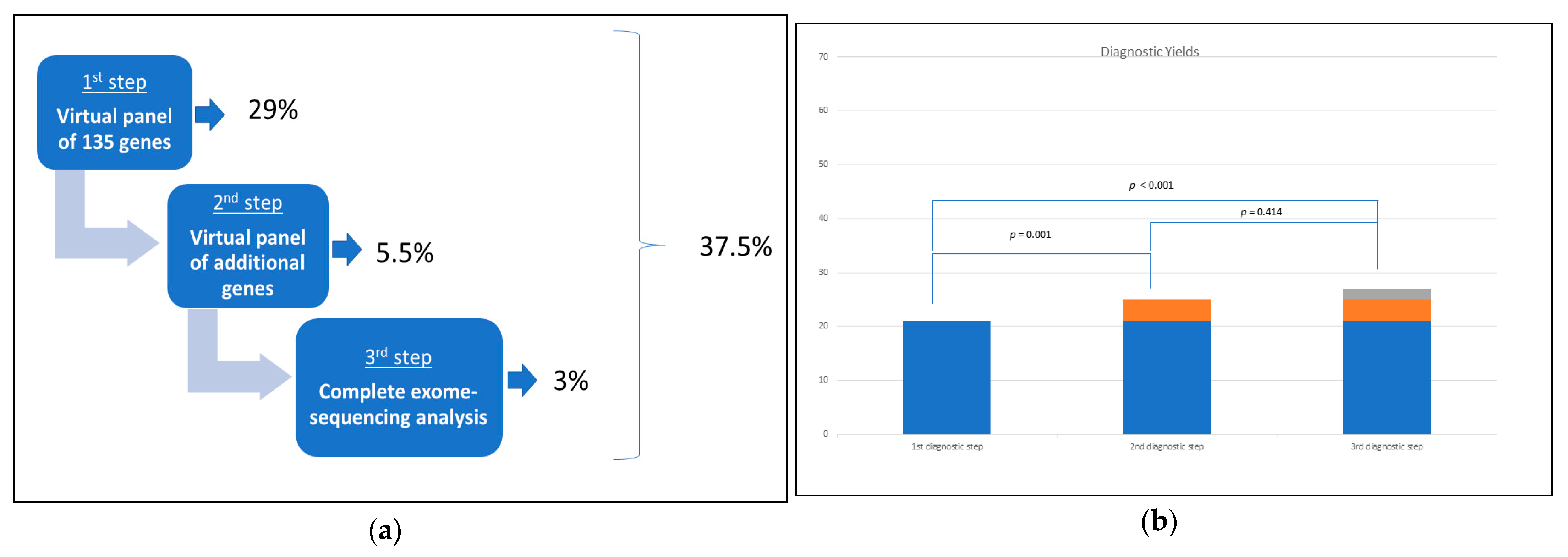
3.2. Molecular Diagnostic Yield of the Cohort
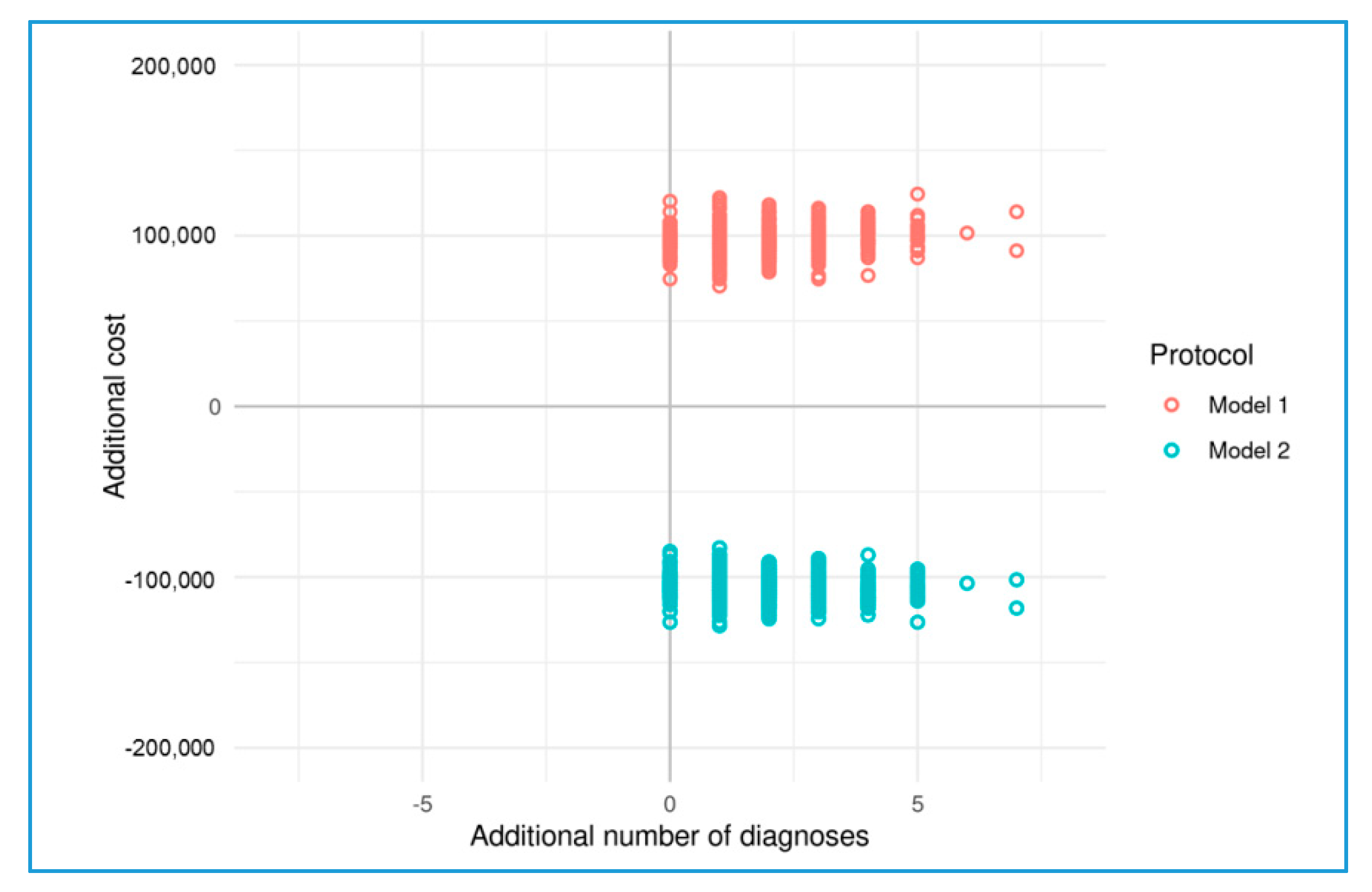
3.3. Cost Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berg, A.T.; Langfitt, J.T.; Testa, F.M.; Levy, S.R.; Di Mario, F.; Westerveld, M.; Kulas, J. Global cognitive function in children with epilepsy: A community-based study. Epilepsia 2008, 49, 608–614. [Google Scholar] [CrossRef]
- Johannesen, K.M.; Nikanorova, N.; Marjanovic, D.; Pavbro, A.; Larsen, L.H.G.; Rubboli, G.; Møller, R.S. Utility of genetic testing for therapeutic decision-making in adults with epilepsy. Epilepsia 2020, 61, 1234–1239. [Google Scholar] [CrossRef]
- Lewis-Smith, D.; Thomas, R.H. The prevalence of genetically diagnosable epilepsies in young adulthood: How many should we be looking for? Epilepsia 2020, 61, 2053–2054. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ari, Y.; Holmes, G.L. Effects of seizures on developmental processes in the immature brain. Lancet Neurol. 2006, 5, 1055–1063. [Google Scholar] [CrossRef]
- Brooks-Kayal, A. Molecular mechanisms of cognitive and behavioral comorbidities of epilepsy in children. Epilepsia 2011, 52 (Suppl. S1), 13–20. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshé, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Specchio, N.; Curatolo, P. Developmental and epileptic encephalopathies: What we do and do not know. Brain 2021, 144, 32–43. [Google Scholar] [CrossRef]
- McTague, A.; Howell, K.B.; Cross, J.H.; Kurian, M.A.; Scheffer, I.E. The genetic landscape of the epileptic encephalopathies of infancy and childhood. Lancet Neurol. 2016, 15, 304–316. [Google Scholar] [CrossRef]
- Weber, Y.G.; Biskup, S.; Helbig, K.L.; Von Spiczak, S.; Lerche, H. The role of genetic testing in epilepsy diagnosis and management. Expert Rev. Mol. Diagn. 2017, 17, 739–750. [Google Scholar] [CrossRef]
- Li, J.; Cai, T.; Jiang, Y.; Chen, H.; He, X.; Chen, C.; Li, X.; Shao, Q.; Ran, X.; Li, Z.; et al. Genes with de novo mutations are shared by four neuropsychiatric disorders discovered from NPdenovo database. Mol. Psychiatry 2016, 21, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochtus, A.; Olson, H.E.; Smith, L.; Keith, L.G.; El Achkar, C.; Taylor, A.; Mahida, S.; Park, M.; Kelly, M.; Shain, C.; et al. Genetic diagnoses in epilepsy: The impact of dynamic exome analysis in a pediatric cohort. Epilepsia 2020, 61, 249–258. [Google Scholar] [CrossRef]
- Pellacani, S.; Dosi, C.; Valvo, G.; Moro, F.; Mero, S.; Sicca, F.; Santorelli, F.M. Customized multigene panels in epilepsy: The best things come in small packages. Neurogenetics 2020, 21, 1–18. [Google Scholar] [CrossRef]
- Neveling, K.; Feenstra, I.; Gilissen, C.; Hoefsloot, L.H.; Kamsteeg, E.J.; Mensenkamp, A.R.; Rodenburg, R.J.; Yntema, H.G.; Spruijt, L.; Vermeer, S.; et al. A post-hoc comparison of the utility of sanger sequencing and exome sequencing for the diagnosis of heterogeneous diseases. Hum. Mutat. 2013, 34, 1721–1726. [Google Scholar] [CrossRef]
- Schwarze, K.; Buchanan, J.; Taylor, J.C.; Wordsworth, S. Are whole-exome and whole-genome sequencing approaches cost-effective? A systematic review of the literature. Genet. Med. 2018, 20, 1122–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Arlington, VA, USA, 2013. [Google Scholar]
- Fisher, R.S. The New Classification of Seizures by the International League Against Epilepsy 2017. Curr. Neurol. Neurosci. Rep. 2017, 17, 48. [Google Scholar] [CrossRef] [PubMed]
- Seaby, E.G.; Pengelly, R.J.; Ennis, S. Exome sequencing explained: A practical guide to its clinical application. Brief Funct. Genom. 2016, 15, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. ACMG Laboratory Quality Assurance Committee. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Snoeijen-Schouwenaars, F.M.; van Ool, J.S.; Verhoeven, J.S.; van Mierlo, P.; Braakman, H.M.H.; Smeets, E.E.; Nicolai, J.; Schoots, J.; Teunissen, M.W.A.; Rouhl, R.P.W.; et al. Diagnostic exome sequencing in 100 consecutive patients with both epilepsy and intellectual disability. Epilepsia 2019, 60, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Stark, Z.; Schofield, D.; Alam, K.; Wilson, W.; Mupfeki, N.; Macciocca, I.; Shrestha, R.; White, S.M.; Gaff, C. Prospective comparison of the cost-effectiveness of clinical whole-exome sequencing with that of usual care overwhelmingly supports early use and reimbursement. Genet. Med. 2017, 19, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Palmer, E.E.; Schofield, D.; Shrestha, R.; Kandula, T.; Macintosh, R.; Lawson, J.A.; Andrews, I.; Sampaio, H.; Johnson, A.M.; Farrar, M.A.; et al. Integrating exome sequencing into a diagnostic pathway for epileptic encephalopathy: Evidence of clinical utility and cost effectiveness. Mol. Genet. Genom. Med. 2018, 6, 186–199. [Google Scholar] [CrossRef]
- Lindy, A.S.; Stosser, M.B.; Butler, E.; Downtain-Pickersgill, C.; Shanmugham, A.; Retterer, K.; Brandt, T.; Richard, G.; McKnight, D.A. Diagnostic outcomes for genetic testing of 70 genes in 8565 patients with epilepsy and neurodevelopmental disorders. Epilepsia 2018, 59, 1062–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, P.; Albury, C.L.; Maksemous, N.; Benton, M.C.; Sutherland, H.G.; Smith, R.A.; Haupt, L.M.; Griffiths, L.R. Next Generation Sequencing Methods for Diagnosis of Epilepsy Syndromes. Front. Genet. 2018, 7, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costain, G.; Cordeiro, D.; Matviychuk, D.; Mercimek-Andrews, S. Clinical Application of Targeted Next-Generation Sequencing Panels and Whole Exome Sequencing in Childhood Epilepsy. Neuroscience 2019, 15, 291–310. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, B.; Lee, J.S.; Kim, H.D.; Choi, J.R.; Lee, S.T.; Kang, H.C. Proband-Only Clinical Exome Sequencing for Neurodevelopmental Disabilities. Pediatr. Neurol. 2019, 99, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.A.; Johnstone, D.L.; Dyment, D.A. Epilepsy genetics: Current knowledge, applications, and future directions. Clin. Genet. 2019, 95, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balciuniene, J.; DeChene, E.T.; Akgumus, G.; Romasko, E.J.; Cao, K.; Dubbs, H.A.; Mulchandani, S.; Spinner, N.B.; Conlin, L.K.; Marsh, E.D.; et al. Use of a Dynamic Genetic Testing Approach for Childhood-Onset Epilepsy. JAMA Netw. Open. 2019, 2, e192129. [Google Scholar] [CrossRef]
- Jiang, Y.L.; Song, C.; Wang, Y.; Zhao, J.; Yang, F.; Gao, Q.; Leng, X.; Man, Y.; Jiang, W. Clinical Utility of Exome Sequencing and Reinterpreting Genetic Test Results in Children and Adults WITH Epilepsy. Front. Genet. 2020, 11, 591434. [Google Scholar] [CrossRef]
- SoRelle, J.A.; Thodeson, D.M.; Arnold, S.; Gotway, G.; Park, J.Y. Clinical Utility of Reinterpreting Previously Reported Genomic Epilepsy Test Results for Pediatric Patients. JAMA Pediatr. 2019, 173, e182302. [Google Scholar] [CrossRef]
- Deignan, J.L.; Chao, E.; Gannon, J.L.; Greely, H.T.; Hagman, K.D.F.; Mao, R.; Topper, S. ACMG Laboratory Quality Assurance Committee. Points to consider when assessing relationships (or suspecting misattributed relationships) during family-based clinical genomic testing: A statement of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 2020, 22, 1285–1287. [Google Scholar]
- Dorschner, M.O.; Amendola, L.M.; Turner, E.H.; Robertson, P.D.; Shirts, B.H.; Gallego, C.J.; Bennett, R.L.; Jones, K.L.; Tokita, M.J.; Bennett, J.T.; et al. Actionable, pathogenic incidental findings in 1000 participants’ exomes. Am. J. Hum. Genet. 2013, 93, 631–640. [Google Scholar] [CrossRef] [Green Version]
- Sánchez Fernández, I.; Loddenkemper, T.; Gaínza-Lein, M.; Sheidley, B.R.; Poduri, A. Diagnostic yield of genetic tests in epilepsy: A meta-analysis and cost-effectiveness study. Neurology 2019, 92, e418–e428. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Proband | Gender | Age | Age at Diagnosis | Gene | Coding Variants | Transcript | Genotype | Protein Variants | Epileptic Diagnosis | NDD Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|
| First Diagnostic Level | ||||||||||
| #1 | M | 17 y | 15y | GRIN2B | c.2444_2446delTTG | NM_000834.5 | Het | p.Ile815_Asp816delinsAsn | DEE | Rett-like phenotype |
| #2 | F | 41 y | 40y | IQSEC2 | c.848delG | NM_001111125.3 | Het | p.Gly283AlafsTer23 | DEE | Severe ID |
| #3 | F | 7 y | 4 y | MECP2 | c.808C>T | NM_004992.4 | Het | p.Arg270Ter | DEE | Rett Syndrome |
| #4 | F | 20 y | 19 y | GNAO1 | c.674G>A | NM_138736.3 | Het | p.Cys225Tyr | DEE | Profound ID |
| #5 | M | 32 y | 29y | CHD2 | c.3951G>T | NM_001271.4 | Het | p.Leu1317Phe | FE | Severe ID, ASD |
| #6 | F | 13 y | 12 y | PURA | c.10C>T | NM_005859.5 | Het | p.Arg4Ter | DEE | Profound ID |
| #7 | M | 6 y | 5 y | KCNQ2 | c.502T>A | NM_172107.4 | Het | p.Phe168Ile | GE | Profound ID |
| #8 | M | 13 y | 9 y | KCNQ2 | c.365C>T | NM_172107.4 | Het | p.Ser122Leu | GE | Profound ID, ASD |
| #9 | F | 14 y | 12 y | IQSEC2 | c.2201_2202delAC | NM_001111125.3 | Het | p.Tyr734SerfsTer7 | FE | ID |
| #10 | M | 4 y | 6 m | CDKL5 | c.601_603delCTT | NM_003159.2 | Hemi | p.Leu201del | DEE | Rett-like phenotype |
| #11 | M | 5 y | 1 y | CDKL5 | c.569delA | NM_003159.2 | Hemi | p.Lys190SerfsTer38 | DEE | Rett-like phenotype |
| #12 | F | 29 y | 28 y | SLC2A1 | c.988C>T | NM_006516.4 | Het | p.Arg330Ter | FE | Moderate ID |
| #13 | M | 32 y | 28 y | ADSL | c.1277G>A | NM_000026.4 | Hom | p.Phe426His | DEE | Profound ID |
| #14 | M | 7 y | 4 y | SCN1A | c.3610T>C | NM_001202435.3 | Het | p.Trp1204Arg | DEE (DS) | Psychomotor delay |
| #15 | F | 9 y | 6 y | KCNT1 | c.2627A>G | NM_020822.3 | Het | p.Tyr876Cys | FE | Moderate ID |
| #16 | F | 7 y | 3 y | SCN8A | c.5630A>G | NM_014191.4 | Het | p.Asn1877Ser | FE | Moderate ID, autistic-like features |
| #17 | F | 12 y | 9 y | SLC2A1 | c.940G>A | NM_006516.4 | Het | p.Gly314Ser | GE | Mild ID |
| #18 | M | 8 y | 7 y | GRIN2A | c.2189A>G | NM_000833.5 | Het | p.Tyr730Cys | DEE (LKS) | Moderate ID |
| #19 | M | 17 y | 16 y | IQSEC2 | c.1075C>T | NM_001111125.3 | Hemi | p.Arg359Cys | GE | Moderate ID |
| #20 | M | 6 y | 3 y | GABRB3 | c.39G>A | NM_021912.5 | Het | p.Trp13Ter | GE | Psychomotor delay |
| #21 | F | 7 y | 6 y | SLC6A1 | c.1229A>C | NM_003042.4 | Het | p.Asp410Ala | GE | Mild ID |
| Second Diagnostic Level | ||||||||||
| #22 | F | 21 y | 20 y | DYNC1H1 | c.12161_12162delATins TGGTTATGATGCCA | NM_001376.5 | Het | p.His4054delinsLeuVal MetMetPro | GE | Mild ID |
| #23 | F | 11 y | 10 y | PIGN | c.1434+5G>A | NM_176787.5 | Hom | - | DEE | Profound ID |
| #24 | F | 4 y | 3 y | PIGN | c.1251+1G>T | NM_176787.5 | Het | - | DEE | Profound ID |
| PIGN | c.2399G>A | NM_176787.5 | Het | p.Gly800Glu | ||||||
| #25 | F | 22 y | 21 y | GNB1 | c.233A>G | NM_002074.5 | Het | p.Lys78Arg | DEE | Profound ID |
| Third Diagnostic Level | ||||||||||
| #26 | M | 16 y | 15 y | PRRT2 | c.649dupC | NM_001256442.2 | Het | p.Arg217ProfsTer8 | Focal epilepsy | Mild ID |
| #27 | F | 6 y | 5 y | PIGC | c.859G>T | NM_153747.2 | Hom | p.Glu287Ter | DEE | Profound ID |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varesio, C.; Gana, S.; Asaro, A.; Ballante, E.; Cabini, R.F.; Tartara, E.; Bagnaschi, M.; Pasca, L.; Valente, M.; Orcesi, S.; et al. Diagnostic Yield and Cost-Effectiveness of “Dynamic” Exome Analysis in Epilepsy with Neurodevelopmental Disorders: A Tertiary-Center Experience in Northern Italy. Diagnostics 2021, 11, 948. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060948
Varesio C, Gana S, Asaro A, Ballante E, Cabini RF, Tartara E, Bagnaschi M, Pasca L, Valente M, Orcesi S, et al. Diagnostic Yield and Cost-Effectiveness of “Dynamic” Exome Analysis in Epilepsy with Neurodevelopmental Disorders: A Tertiary-Center Experience in Northern Italy. Diagnostics. 2021; 11(6):948. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060948
Chicago/Turabian StyleVaresio, Costanza, Simone Gana, Alessia Asaro, Elena Ballante, Raffaella Fiamma Cabini, Elena Tartara, Michela Bagnaschi, Ludovica Pasca, Marialuisa Valente, Simona Orcesi, and et al. 2021. "Diagnostic Yield and Cost-Effectiveness of “Dynamic” Exome Analysis in Epilepsy with Neurodevelopmental Disorders: A Tertiary-Center Experience in Northern Italy" Diagnostics 11, no. 6: 948. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060948