
Vessel Wall Inflammatory Activity as Determined by F-18 Fluorodeoxyglucose PET in Large Vessel Vasculitis Is Attenuated by Immunomodulatory Drugs


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. PET/CT Image Analysis
2.3. Statistical Analysis
3. Results
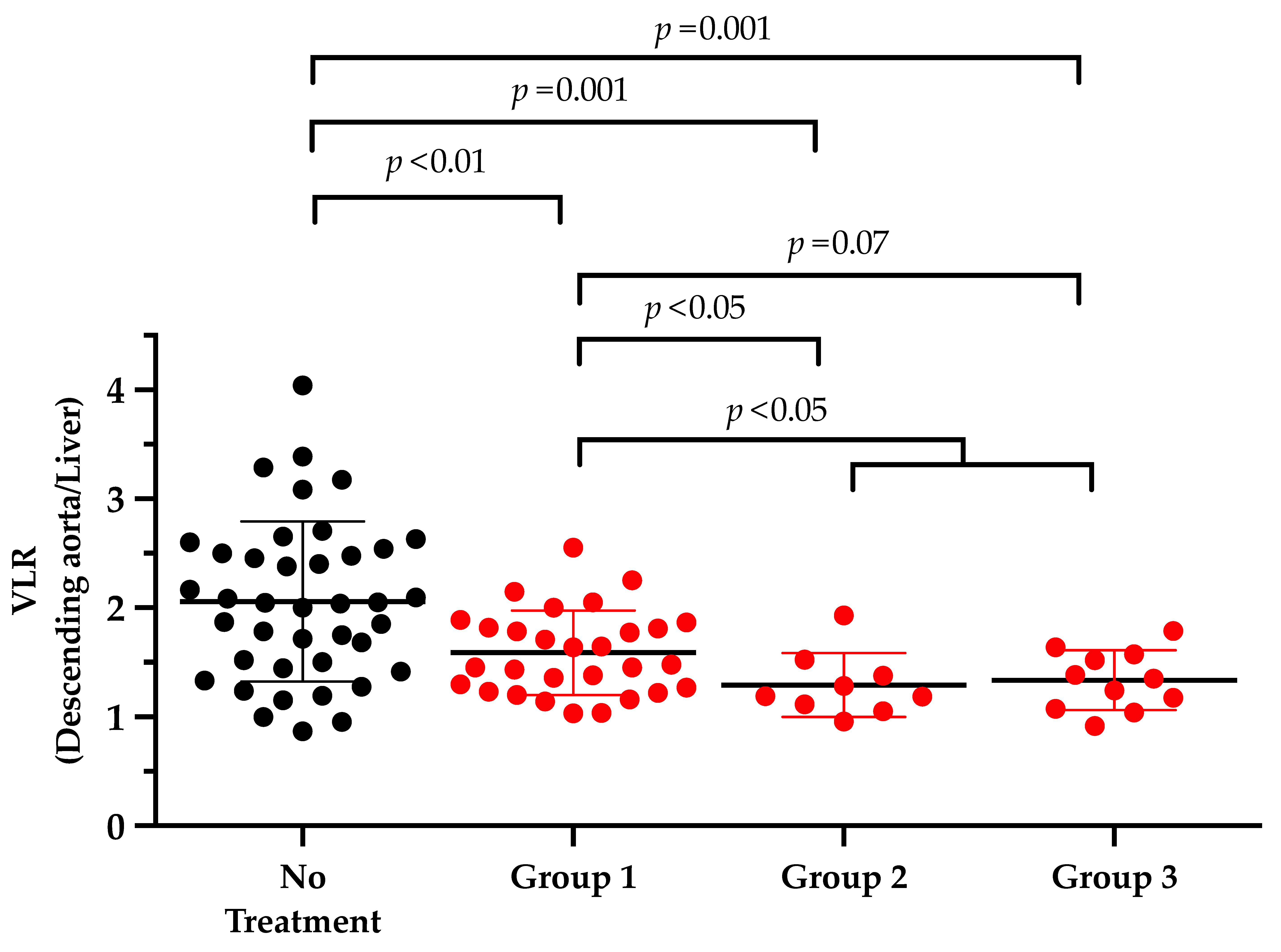
3.1. Impact of Immunomodulatory Drugs on Vessel Wall Uptake
Vessel Wall Uptake Decreases with the Additional Intake of Immunomodulatory Drugs
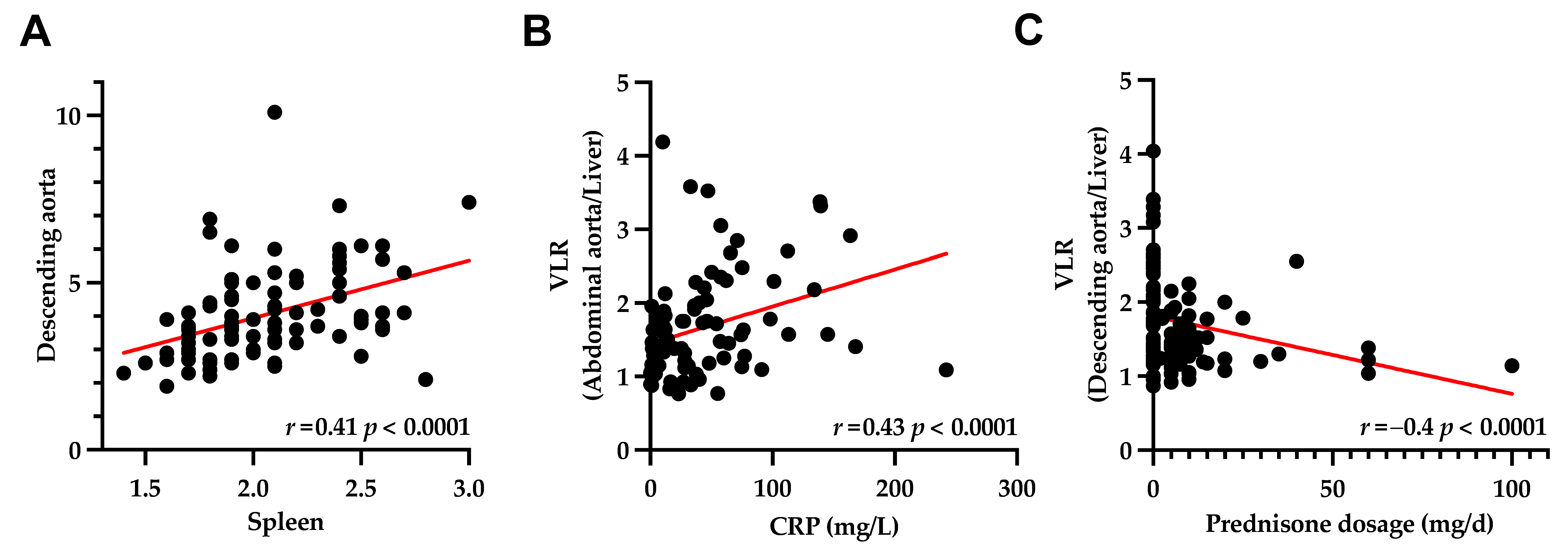
3.2. Hematopoietic Organs
3.3. Systemic Inflammatory Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dejaco, C.; Ramiro, S.; Duftner, C.; Besson, F.L.; Bley, T.A.; Blockmans, D.; Brouwer, E.; Cimmino, M.A.; Clark, E.; Dasgupta, B.; et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann. Rheum. Dis. 2018, 77, 636–643. [Google Scholar] [CrossRef]
- Lariviere, D.; Benali, K.; Coustet, B.; Pasi, N.; Hyafil, F.; Klein, I.; Chauchard, M.; Alexandra, J.F.; Goulenok, T.; Dossier, A.; et al. Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: A real-life prospective study. Medicine 2016, 95, e4146. [Google Scholar] [CrossRef]
- Buttgereit, F.; Brabant, T.; Dinges, H.; Hiemer, I.; Kaplani, M.; Kiltz, U.; Kyburz, D.; Reißhauer, A.; Schneider, M.; Weseloh, C.; et al. S3-Leitlinie zur Behandlung der Polymyalgia rheumatica. Z. Rheumatologie. 2018, 77, 429–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; de Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, G.S.; Merkel, P.A.; Brasington, R.D.; Lenschow, D.J.; Liang, P. Anti-tumor necrosis factor therapy in patients with difficult to treat Takayasu arteritis. Arthritis Rheum. 2004, 50, 2296–2304. [Google Scholar] [CrossRef] [PubMed]
- Shinjo, S.K.; Pereira, R.M.R.; Tizziani, V.A.P.; Radu, A.S.; Levy-Neto, M. Mycophenolate mofetil reduces disease activity and steroid dosage in Takayasu arteritis. Clin. Rheumatol. 2007, 26, 1871–1875. [Google Scholar] [CrossRef]
- de Souza, A.W.; de Almeida Agustinelli, R.; de Cinque Almeida, H.; Oliveira, P.B.; Pinheiro, F.A.; Oliveira, A.C.; Sato, E.I. Leflunomide in Takayasu arteritis -A long term observational study. Rev. Bras Reumatol. Engl. Ed. 2016, 56, 371–375. [Google Scholar] [CrossRef] [Green Version]
- Stone, J.H.; Klearman, M.; Collinson, N. Trial of Tocilizumab in Giant-Cell Arteritis. N. Engl. J. Med. 2017, 377, 1494–1495. [Google Scholar] [CrossRef]
- Taimen, K.; Salomäki, S.P.; Hohenthal, U.; Mali, M.; Kajander, S.; Seppänen, M.; Nuutila, P.; Palomäki, A.; Roivainen, A.; Pirilä, L.; et al. The Clinical Impact of Using 18F-FDG-PET/CT in the Diagnosis of Suspected Vasculitis: The Effect of Dose and Timing of Glucocorticoid Treatment. Contrast Media Mol. Imaging 2019, 2019, 9157637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhtyar, C.; Guillevin, L.; Cid, M.C.; Dasgupta, B.; De Groot, K.; Gross, W.L.; Hauser, T.; Hellmich, B.; Jayne, D.; Kallenberg, C.G.M.; et al. EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2008, 68, 318–323. [Google Scholar] [CrossRef] [Green Version]
- Slart, R.; Writing Group; Reviewer Group; Members of EANM Cardiovascular; Members of EANM Infection & Inflammation; Members of Committees, SNMMI Cardiovascular; Members of Council, PET Interest Group; Members of ASNC; EANM Committee Coordinator. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: Joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derlin, T.; Sedding, D.G.; Dutzmann, J.; Haghikia, A.; Konig, T.; Napp, L.C.; Schutze, C.; Owsianski-Hille, N.; Wester, H.J.; Kropf, S.; et al. Imaging of chemokine receptor CXCR4 expression in culprit and nonculprit coronary atherosclerotic plaque using motion-corrected [68Ga]pentixafor PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1934–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, M.; Briel, M.; Daikeler, T.; Walker, U.A.; Rasch, H.; Berg, S.; Ng, Q.K.; Raatz, H.; Jayne, D.; Kotter, I.; et al. The impact of 18F-FDG PET on the management of patients with suspected large vessel vasculitis. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Prieto-Gonzalez, S.; Depetris, M.; Garcia-Martinez, A.; Espigol-Frigole, G.; Tavera-Bahillo, I.; Corbera-Bellata, M.; Planas-Rigol, E.; Alba, M.A.; Hernandez-Rodriguez, J.; Grau, J.M.; et al. Positron emission tomography assessment of large vessel inflammation in patients with newly diagnosed, biopsy-proven giant cell arteritis: A prospective, case-control study. Ann. Rheum. Dis. 2014, 73, 1388–1392. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Bengel, F.M.; Derlin, T. Emerging molecular targets for imaging of atherosclerotic plaque using positron emission tomography. Curr. Radiopharm. 2020. [Google Scholar] [CrossRef]
- Werner, R.A.; Thackeray, J.T.; Diekmann, J.; Weiberg, D.; Bauersachs, J.; Bengel, F.M. The Changing Face of Nuclear Cardiology: Guiding Cardiovascular Care Toward Molecular Medicine. J. Nucl. Med. 2020, 61, 951–961. [Google Scholar] [CrossRef]
- Weiberg, D.; Thackeray, J.T.; Daum, G.; Sohns, J.M.; Kropf, S.; Wester, H.J.; Ross, T.L.; Bengel, F.M.; Derlin, T. Clinical Molecular Imaging of Chemokine Receptor CXCR4 Expression in Atherosclerotic Plaque Using (68)Ga-Pentixafor PET: Correlation with Cardiovascular Risk Factors and Calcified Plaque Burden. J. Nucl. Med. 2018, 59, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Borchert, T.; Beitar, L.; Langer, L.B.N.; Polyak, A.; Wester, H.-J.; Ross, T.L.; Hilfiker-Kleiner, D.; Bengel, F.M.; Thackeray, J.T. Dissecting the target leukocyte subpopulations of clinically relevant inflammation radiopharmaceuticals. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef]
- Kircher, M.; Tran-Gia, J.; Kemmer, L.; Zhang, X.; Schirbel, A.; Werner, R.A.; Buck, A.K.; Wester, H.J.; Hacker, M.; Lapa, C.; et al. Imaging Inflammation in Atherosclerosis with CXCR4-Directed 68Ga-Pentixafor PET/CT: Correlation with 18F-FDG PET/CT. J. Nucl. Med. 2020, 61, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Lensen, K.D.F.; Comans, E.F.I.; Voskuyl, A.E.; Van Der Laken, C.J.; Brouwer, E.; Zwijnenburg, A.T.; Arias-Bouda, L.M.P.; Glaudemans, A.W.J.M.; Slart, R.H.J.A.; Smulders, Y.M. Large-Vessel Vasculitis: Interobserver Agreement and Diagnostic Accuracy of 18F-FDG-PET/CT. BioMed Res. Int. 2015, 2015, 914692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Mean ± SD |
|---|---|---|
| Clinical parameters | ||
| Female | 72/94 (76.6) | - |
| Age | 63 ± 13 | |
| >50 years | 82 (87.2) | - |
| ≤50 years | 12 (12.8) | - |
| C-reactive protein (mg/L) | 87/94 (92.6) | 42.8 ± 46.5 |
| Diabetes 1 | 6/87 (6.9) | - |
| Hypertension 2 | 44/88 (50.0) | - |
| Medication | ||
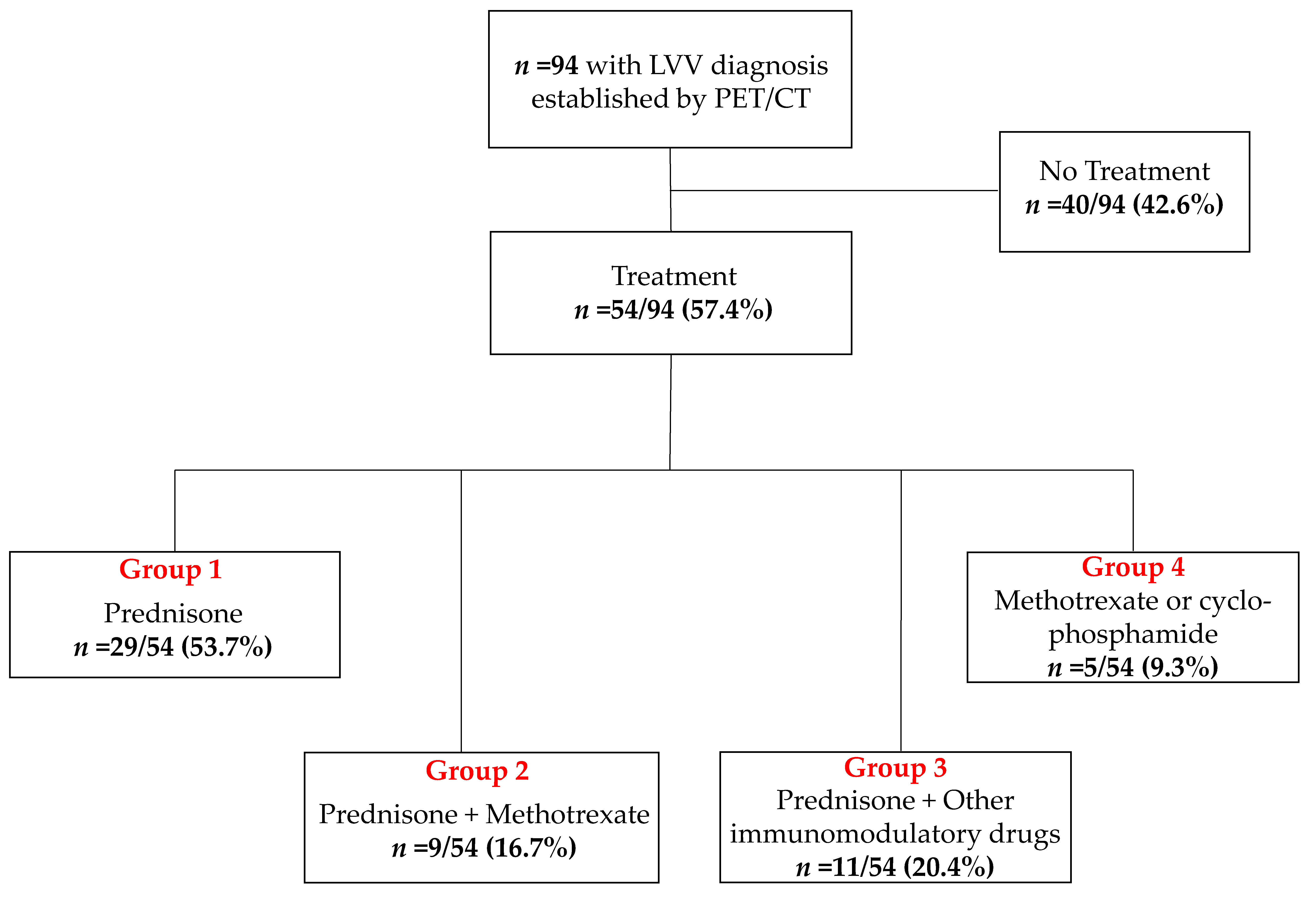
| No treatment | 40/94 (42.6) | - |
| Treatment | 54/94 (57.4) | - |
| Group 1: Prednisone | 29/54 (53.7) | - |
| Group 2: Methotrexate with prednisone | 9/54 (16.7) | - |
| Group 3: Other immunomodulatory drugs 3 with prednisone | 11/54 (20.4) | - |
| Group 4: Methotrexate or Cyclophosphamide 4 | 5/54 (9.3) | - |
| SUV | VLR | |
|---|---|---|
| Hematopoietic organs | ||
| Bone marrow | 1.82 ± 0.48 | - |
| Spleen | 2.06 ± 0.33 | - |
| Arterial segments | ||
| Vertebral artery | 2.79 ± 1.47 | 1.18 ± 0.63 |
| Subclavian artery | 3.41 ± 1.61 | 1.46 ± 0.74 |
| Carotid artery | 3.52 ± 1.40 | 1.50 ± 0.62 |
| Ascending aorta | 3.87 ± 1.24 | 1.65 ± 0.54 |
| Aortic arch | 3.99 ± 1.17 | 1.70 ± 0.52 |
| Descending aorta | 4.04 ± 1.39 | 1.73 ± 0.62 |
| Abdominal aorta | 3.92 ± 1.64 | 1.68 ± 0.75 |
| Femoral artery | 3.19 ± 1.57 | 1.35 ± 0.65 |
| Arterial Segment | No Treatment | Group 1 Prednisone | Group 2 Methotrexate + Prednisone | Group 3 Other Immunomodulatory Drugs 1 + Prednisone | |||
|---|---|---|---|---|---|---|---|
| VLR | VLR | p-Value | VLR | p-Value | VLR | p-Value | |
| Vertebral artery | 1.35 ± 0.72 | 1.18 ± 0.67 | 0.28 | 0.98 ± 0.35 | 0.06 | 0.91 ± 0.24 | 0.006 |
| Subclavian artery | 1.84 ± 0.83 | 1.33 ± 0.54 | 0.007 | 0.90 ± 0.30 | 0.0005 | 1.00 ± 0.53 | 0.001 |
| Carotid artery | 1.76 ± 0.73 | 1.47 ± 0.49 | 0.06 | 1.13 ± 0.38 | 0.006 | 1.14 ± 0.27 | 0.004 |
| Ascending aorta | 1.90 ± 0.62 | 1.51 ± 0.42 | 0.004 | 1.31 ± 0.22 | 0.003 | 1.51 ± 0.29 | 0.07 |
| Aortic arch | 1.96 ± 0.58 | 1.63 ± 0.41 | 0.018 | 1.32 ± 0.26 | 0.001 | 1.35 ± 0.23 | 0.0003 |
| Descending aorta | 2.06 ± 0.73 | 1.59 ± 0.39 | 0.005 | 1.29 ± 0.29 | 0.001 | 1.34 ± 0.27 | 0.001 |
| Abdominal aorta | 2.08 ± 0.92 | 1.48 ± 0.43 | 0.006 | 1.21 ± 0.32 | 0.002 | 1.33 ± 0.46 | 0.007 |
| Femoral artery | 1.56 ± 0.78 | 1.26 ± 0.54 | 0.12 | 1.27 ± 0.45 | 0.42 | 1.02 ± 0.34 | 0.049 |
| Arterial Segment | Spleen | Bone Marrow | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| Vertebral artery | 0.41 | <0.0001 | 0.18 | 0.08 |
| Subclavian artery | 0.34 | 0.0007 | 0.12 | 0.27 |
| Carotid artery | 0.54 | <0.0001 | 0.25 | 0.014 |
| Ascending aorta | 0.41 | <0.0001 | 0.26 | 0.0013 |
| Aortic arch | 0.48 | <0.0001 | 0.20 | 0.05 |
| Descending aorta | 0.41 | <0.0001 | 0.08 | 0.44 |
| Abdominal aorta | 0.38 | 0.0002 | 0.22 | 0.031 |
| Femoral artery | 0.47 | <0.0001 | 0.20 | 0.05 |
| Arterial Segment | r | p-Value |
|---|---|---|
| Vertebral artery | 0.32 | 0.003 |
| Subclavian artery | 0.33 | 0.002 |
| Carotid artery | 0.38 | 0.0003 |
| Ascending aorta | 0.25 | 0.018 |
| Aortic arch | 0.38 | 0.0004 |
| Descending aorta | 0.29 | 0.007 |
| Abdominal aorta | 0.43 | <0.001 |
| Femoral artery | 0.35 | 0.0008 |
| Arterial Segment | r | p-Value |
|---|---|---|
| Vertebral artery | −0.15 | 0.15 |
| Subclavian artery | −0.38 | 0.0002 |
| Carotid artery | −0.24 | 0.02 |
| Ascending aorta | −0.26 | 0.01 |
| Aortic arch | −0.4 | <0.0001 |
| Descending aorta | −0.4 | <0.0001 |
| Abdominal aorta | −0.36 | 0.0004 |
| Femoral artery | −0.15 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sherzay, R.; Witte, T.; Derlin, T.; Hoepfner, M.; Bengel, F.M. Vessel Wall Inflammatory Activity as Determined by F-18 Fluorodeoxyglucose PET in Large Vessel Vasculitis Is Attenuated by Immunomodulatory Drugs. Diagnostics 2021, 11, 1132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071132
Sherzay R, Witte T, Derlin T, Hoepfner M, Bengel FM. Vessel Wall Inflammatory Activity as Determined by F-18 Fluorodeoxyglucose PET in Large Vessel Vasculitis Is Attenuated by Immunomodulatory Drugs. Diagnostics. 2021; 11(7):1132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071132
Chicago/Turabian StyleSherzay, Romilda, Torsten Witte, Thorsten Derlin, Marius Hoepfner, and Frank M. Bengel. 2021. "Vessel Wall Inflammatory Activity as Determined by F-18 Fluorodeoxyglucose PET in Large Vessel Vasculitis Is Attenuated by Immunomodulatory Drugs" Diagnostics 11, no. 7: 1132. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071132