1. Introduction
Taenia solium is a neglected zoonotic parasite ranked first on the global scale of foodborne parasites [
1]. Humans are the final host, carrying the tapeworm in their intestines (taeniosis, T), but can also act as an accidental dead-end intermediate host, in which the metacestode larval stage can develop in the muscles, the subcutaneous tissue (cysticercosis, CC) or the central nervous system (neurocysticercosis, NCC).
T. solium is endemic in sub-Saharan Africa, Latin America, and south-east Asia [
2], particularly affecting poor communities with free-range pigs and low levels of sanitation, hygiene, and education. In rural communities of Zambia, high prevalence rates of
T. solium have been reported and NCC is considered the main cause of acquired epilepsy in these areas [
3,
4,
5]. Apart from the significant public health impact, NCC also has a strong economic and social impact on people suffering from or affected by this disease, as they are often stigmatized and marginalized in their communities.
The diagnosis of NCC in such settings is problematic, particularly because it requires access to neuroimaging and trained neurologists, which are scarce in resource-poor areas. Also, for the diagnosis of CC and T, the existing tests are not suitable to use in these communities because an accurate detection is either expensive, time consuming, and/or requires expensive equipment, infrastructure, and/or skilled personnel [
6], all of which are scarce in resource-limited settings. Therefore, field applicable, affordable, and accurate point-of-care (POC) tests for T and (N)CC are urgently needed in order to control the pathogen. Such tests are not only required for diagnosis and treatment, but also for surveillance and monitoring of control programs [
7]. Although several rapid diagnostic tests have been developed, many still require proper evaluation in the population in which they are intended to be used [
8]. Therefore, the SOLID project “Evaluation of an antibody detecting point-of-care test for the diagnosis of
Taenia solium taeniosis and (neuro)cysticercosis in Tanzania and Zambia” was launched in 2016. Within the project, the performance of a newly developed POC test was assessed in two different settings to represent the intended use and role where the test may be used in practice: community-based (in Zambia) and hospital-based (in Tanzania).
The conduct of a diagnostic accuracy study in low-resource community settings was anticipated to be challenging. Besides the difficulties of conducting a clinical trial in developing countries (such as the limited research and neuroimaging infrastructure mentioned above), peculiarities specifically related to the disease led to additional concerns for the design and planning of this study. The low prevalence of taeniosis and the lack of a gold standard for taeniosis and cysticercosis were important factors to consider when designing the trial. Therefore, the aim of this paper is to describe the design, the challenges, and rationale for the design of the diagnostic accuracy study in low-resource community settings in Zambia. The materials and methods section presents the TS POC test (index test under evaluation), gives an overview of the planning of the study and describes the design that was finally used for the trial (based on protocol version 1.3; 29 August 2017), which takes all the challenges into account. In the discussion, we detail the rationale behind different design aspects that were chosen for this trial, aiming to reduce bias and increase the generalizability of the study results.
2. Materials and Methods
2.1. TS POC Test
An antibody-detecting prototype test (TS POC) has been developed by a team of researchers from the Centers for Disease Control and Prevention (CDC), Atlanta, USA, in collaboration with the Department of Neurology, Klinikum rechts der Isar, Technical University of Munich (TUM), Germany. The TS POC test combines two well-validated and extensively used recombinant proteins in one multi-strip test kit: rT24H for the detection of CC antibodies (TS POC CC), and rES33 for the detection of T antibodies (TS POC T) [
9,
10]. Recombinant antigens were chosen for the present TS POC prototype to facilitate a future standardized low-cost production of this test for resource-poor settings. The preliminary laboratory performance of the TS POC was estimated at a sensitivity of 88–93% (for one cyst or multiple cysts, respectively) and specificity of 99% for cysticercosis, and a sensitivity of 82% and specificity of 99% for taeniosis (CDC, TUM, 2017 unpublished data). Before the potential commercialization and implementation of the test, a large-scale field evaluation of its performance and applicability as a rapid test is required. Therefore, a diagnostic accuracy study was conducted, aiming to assess the sensitivity and specificity of the multistrip TS POC test in
T. solium endemic communities.
2.2. Study Planning
The SOLID project had a multidisciplinary team with a very intense North/South collaboration. The project was funded for a period of four years. The entire first year served to elaborate on the study protocols, prepare the SOPs and treatment protocols, electronic case report forms (eCRFs), train project staff, and obtain the necessary ethical clearances and approvals. The trial was registered on 21 November 2017, at the Pan African Clinical Trials Registry (identifier: PACTR201712002788898). The SOLID study project was granted ethical clearance for the Zambian part of the study by the University of Zambia Biomedical Research Ethics Committee [UNZABREC 005-07-17], the Institute of Tropical Medicine [IRB/AB/ac/112 Ref 1177/17] through the ethics committee of the University of Antwerp [EC UZA 17/31/352], and by TUM through the Ethical committee of Klinikum rechts der Isar, Munich [299/18S]. Authorization to conduct research was also granted by the National Health Research Authority at the Ministry of Health in Zambia.
Participant recruitment was done in year two and three. Enrolment started in December 2017 and the last patient was recruited in July 2019. The fourth and final year was used for data cleaning, analyses, and result dissemination and communication to a large span of stakeholders ranging from study participants to ministries in Zambia and international organizations such as the WHO.
2.3. Study Objectives and Outcomes
The primary objective of the study was to assess the sensitivity and specificity of the TS POC T and TS POC CC strips for T and CC/NCC, respectively (
Table 1).
Since there is no gold standard test for the detection of T nor of CC, three different reference tests were performed (
Table 1), and a Bayesian approach was used to determine the accuracy of the TS POC test for T and CC [
11]. For NCC, a composite case definition was used as reference standard according to predefined criteria [
12].
A secondary outcome of the study was to assess the accuracy measures of the TS POC T test relative to results after the treatment and purging of participants who tested positive using the TS POC T and/or any of the T reference tests. The exploratory outcomes of the study included the assessment of observer agreement and ease of use of the test. The follow-up of patients diagnosed with active NCC (over a period of six months), the effect of anthelmintic treatment of symptomatic patients with active NCC, and the community prevalence and clinical/radiological characteristics of NCC were also evaluated.
Laboratory personnel performing the analyses of the reference tests for T and CC were blinded to the TS POC test result. CT scans were read in detail by two independent readers (blinded to the results of the other reader, clinical results, and the TS POC result). Details regarding the assessment of the primary outcome measures can be found in
Appendix A.1.
2.4. Study Design
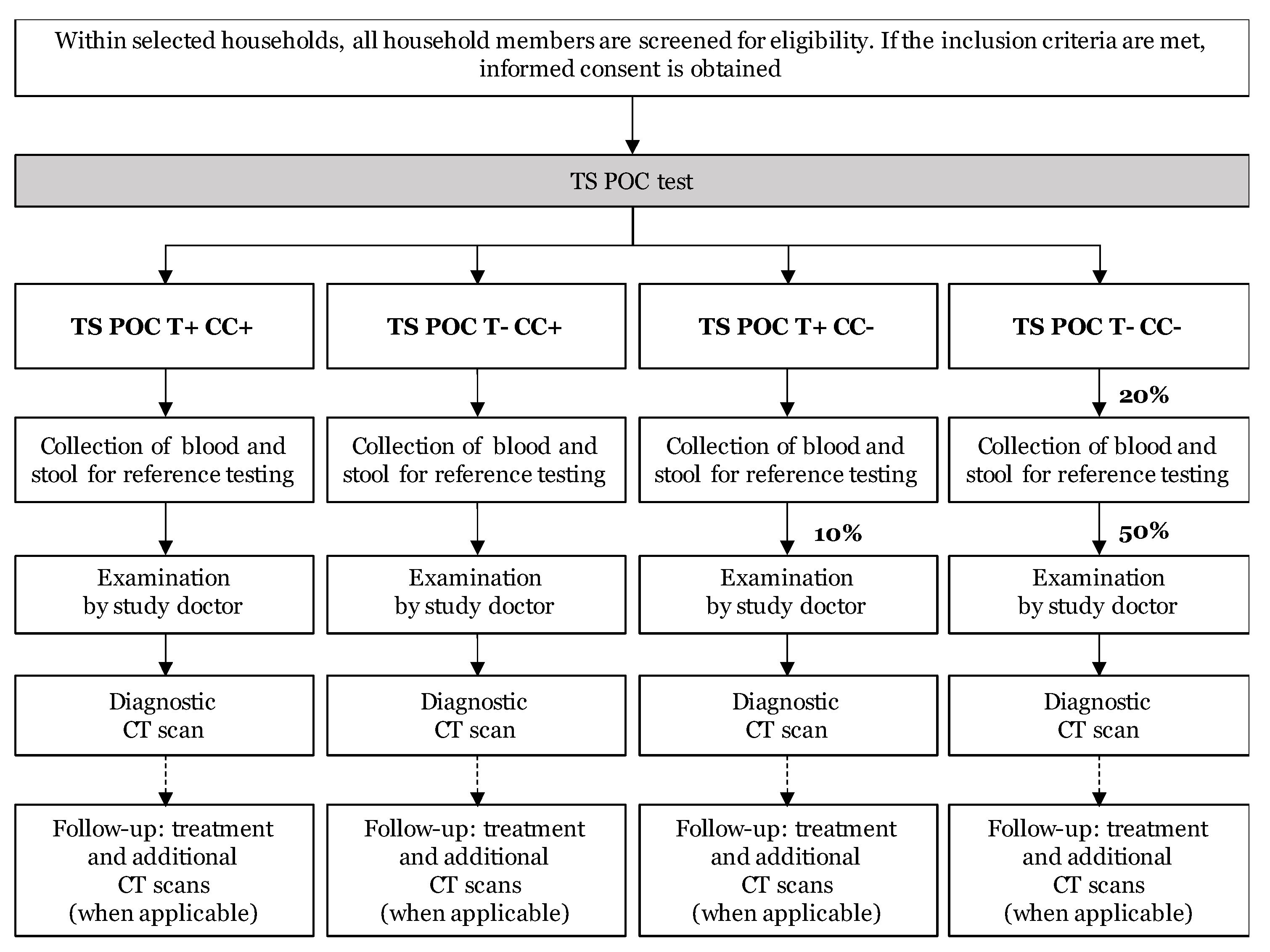
The study was a diagnostic accuracy study with prospective data collection, using a two-stage design. All tests were applied to the same study subject (within-subject or paired design). The flow of the study is visualized in
Figure 1. After obtaining written informed consent, all participants were subjected to the TS POC test (index test; stage 1). All participants with a TS POC positive result and a subset of participants with a TS POC negative result were subjected to several reference tests, clinical examination, and computed tomography (CT) scanning of the brain (stage 2).
The TS POC test was interpreted by two independent readers (two-factorial design) and provided results for both T and CC, resulting in four different TS POC test result combinations: T+CC+, T-CC+, T+CC-, and T-CC-. A blood sample was collected, and a stool sample was requested from all participants who tested positive for at least one test and a 20% subset of participants who tested negative for both outcomes. The 20% subset was obtained by selecting every 5th T-CC- participant for sampling, using a tally system.
All TS POC CC positive and a subset of the TS POC CC negative study subjects were invited for further (clinical) examinations (
Figure 1). In the T+CC- group, a tally system was used, and every 10th participant was selected. From the T-CC- group that was selected for reference sampling, half was invited for further examination by tossing a coin, resulting in a final 10% of the T-CC- group that was selected for further (clinical) examinations. After a clinical neurological examination and a detailed questionnaire at the rural health center by a study doctor, the participants were invited for a diagnostic CT scan of the brain.
All participants who tested positive using the TS POC T test and TS POC T negative participants who tested positive using any of the reference tests for T, were treated with niclosamide and purged. For symptomatic patients with active NCC (based on the diagnostic CT scan), additional CT scans were performed at later time points to evaluate the treatment effect. More information regarding the treatment and follow-up of patients is given in
Appendix A.2.
2.5. Study Area and Population
The study area was Sinda district in the Eastern province of Zambia (
Figure 2). The area was selected as it was well known by the research team and recognized for its high
T. solium endemicity, the presence of free-roaming pigs and low sanitation levels [
13]. The prevalence in the Eastern province of Zambia of human cysticercosis is reported to be 33.5–38.5% (based on antibody detection), and of taeniosis of 6.3–11.9% (copro antigen ELISA) [
4].
Communities were selected based on their willingness to participate, proximity to a Rural Health Centre (RHC), willingness of the staff to cooperate, and year-round accessibility. Four Neighborhood Health Communities (NHC; Mtore, Butao, Chinzure, and Ndaula) in the catchment of Mtandaza RHC were selected. These four communities comprised of 40 different villages in total.
2.6. Study Participants: Eligibility and Recruitment
The exclusion criteria were minimized as much as possible to obtain a representative sample of the target population, but certain groups were excluded due to ethical reasons (particularly related to the CT scan). The inclusion criteria were living in the area and being 10 years of age or older, while the exclusion criteria were pregnancy, and suffering from self-reported severe health conditions hampering daily activities.
Based on an informal pre-study census, the total population within the participating communities was 4331 inhabitants, belonging to 862 households. To obtain the targeted sample size of 1200 participants, 27.7% of our target population had to be tested. The number of participants in each village was thus determined proportionately (27.7%) to the total number of inhabitants within that village.
All households within a village were randomized by generating a random number. Starting with the household with the lowest random number, all household members within the selected household were screened for eligibility, and every consenting eligible household member was recruited. Each participant was given a unique study code at enrolment. The number of household members who were not available and who were not willing to participate, were also documented. The recruitment of the next households continued until the target number for the village was met.
Registration (including written informed consent/assent), the TS POC test, and blood and stool sampling was conducted through door-to-door visits to the selected households by a qualified and trained researcher and (community) health worker. Written informed consent (assent and parent/guardian informed consent for minors) to take part in the study was sought from each participating individual prior to commencing the study procedures. For illiterate participants, a thumbprint was used, and a witness was consulted to sign on their behalf. An additional consent provision was included to store samples after completion of the study and future scientific research.
The study communities were sensitized, starting with the area Chief and village headmen to obtain permission to recruit people in their villages. Sensitizations for all villages in each of the four NHCs were held to explain the study. The sensitization was repeated a day before recruitment in the village commences, and comprised the explanation of the life cycle of the parasite, the purpose and methods of the study, and potential harms and benefits. This sensitization was repeated at the household level during recruitment.
2.7. Training
To ensure high quality data collection, everyone involved in participant recruitment and performing the TS POC test was trained on the biology of the parasite, diagnosis, treatment, prevention, and control of the parasite in endemic areas. Training on project procedures, Good Clinical (Laboratory) Practices and sample collection for nurses and community health workers and refresher trainings of all field teams were set up prior to each field mission to assure the proper handling and troubleshooting of the TS POC test prior to each sampling time point. The compliance on good storage and distribution practices along the supply chain was also documented, following a detailed Standard Operating Procedure (SOP) regarding TS POC test receipt, handling, storage, distribution, and retrieval of unused tests prior to implementation. GZ, who performed the clinical examinations and administered the questionnaires, was trained in neurological examination prior to the study and was supported throughout the study by the neurology team at TUM (ASW, DS) and ITM (EB).
2.8. Data Management
Specific eCRFs were created using EpiCollect5 (
https://five.epicollect.net, accessed on 21 June 2021) to capture the participants’ data. Laboratory test results were recorded in Microsoft Excel files, using a separate database per reference test. Databases with results of the TS POC test, laboratory analyses, clinical examinations, and CT scans were cleaned separately, so personnel involved in data cleaning were blinded to the other test results. Databases were only merged prior to data analysis, after a sufficient level of cleaning of each of the databases. More information on data validation, monitoring, and adverse events can be found in
Appendix A.3.
2.9. Sample Size and Statistical Analysis
The sample size of 1200 study subjects was calculated to obtain a desired precision of the sensitivity and specificity of minimum 10% [
14,
15].
The primary analysis question of this study was to determine the sensitivity and specificity of the TS POC test for the detection of, respectively T, CC, and NCC, each using (a set of) different reference tests. Due to the lack of a gold standard for T and CC, the diagnostic sensitivity and specificity of the TS POC test was estimated using a Bayesian approach [
11]. The sampling scheme was accounted for in the analysis by expanding the original approach by altering the multinomial probabilities according to the observed sampling frequencies. For the diagnosis of NCC, the sensitivity and specificity were computed using the final NCC diagnosis as gold standard, also correcting for verification bias. More details on sample size calculation and statistical analyses can be found in
Appendix A.4.
3. Discussion
The study was designed to minimize potential sources of bias and maximize generalizability, while accounting for the challenges of working in resource-poor community settings and limitations related to the disease, such as the low prevalence of taeniosis and the lack of gold standard for taeniosis and cysticercosis.
To increase the efficiency of the study, a two-phase design was used. All participants received the index test (TS POC), after which all TS POC positive participants and a sample of the TS POC negative participants were selected for reference tests. Consequently, the total number of reference tests, clinical examinations, and CT scans was reduced compared to a conventional cohort design. When the prevalence is low and the reference standard is expensive or invasive, a two-phase design is the design of choice [
16]. The number of various reference tests, which were more time consuming and expensive than the index test, could thus be lowered. This reduction was particularly worthwhile for CT scanning, as it is expensive, logistically difficult to organize, and the inclusion of a disproportionate number of (unnecessary) brain CT scans in healthy participants would be unethical. Besides the benefits of increased efficiency, a drawback of a two-stage design is the risk of bias if there is a differential dropout, which is a potential problem in any study. Nevertheless, withdrawals can be higher in this type of designs, particularly if the reference tests are more time consuming or invasive than the index test and due to the potentially longer time period between performing the index test and reference tests [
16]. The latter was avoided by requesting samples immediately after the TS POC test, which was feasible since the results of the TS POC test are available within 20 min [
17], thus reducing loss to follow-up due to a time gap.
The study initially envisioned more complex flows for sampling and clinical follow-up. As an example, for TS POC T-CC+ participants, only blood samples are needed as only serum is necessary for the CC reference tests. An additional stool sample for T reference testing would only be requested for a negative subset in this group. Nevertheless, a more uniform and simpler flow was finally adopted by requesting both blood and stool samples from all selected participants to avoid errors of incorrect sampling. Additional subsets were also planned for CT scanning, based on the combination of the TS POC test result and clinical examination results. Nevertheless, complex constructs are more difficult to implement under field settings, not only because of difficulties in identification, but also due to the lack of continuous internet access and technical resources, which hampers instant simple randomization and a complex follow-up system. The tally system that was finally used in this study to select subsets of participants for sampling, allowed immediate action, thus providing more clarity for the participants about the following steps in the study and avoiding a discontinuity between testing and sampling. Additionally, the simplified flow for clinical follow-ups also allowed participants to be informed without delay, which was preferred over an off-site randomization of participants. The latter would have resulted in a time lag and difficulties in seeking out selected participants, which may have resulted in more loss to follow-up. Several other measures were also taken to minimize attrition bias for the evaluation of NCC, such as regular visits to selected participants, organizing free transport to Chipata Central Hospital and providing incentives (food and drinks during CT scan appointments), and medical follow-up/treatment free of charge.
The project aimed to determine the accuracy measures of the TS POC test in communities that are highly endemic for T. solium. Therefore, all eligible household members within randomly selected households were recruited, to get a good representation of people with and without the disease in the target population. Nevertheless, pregnant women and children below the age of 10 years were not included for ethical and practical reasons such as the risk of radiation in case a CT scan would be needed, and the difficulties associated with sample collection, CT scanning and purging of young children. Although NCC is often associated with late onset epilepsy, the impact of NCC in children is not extensively studied, resulting in a research gap that needs urgent attention. Thus, future project proposals are encouraged to include also children. Also, people who were absent at the time of sampling or refused participation were not included in the trial, potentially leading to a bias in the results and limiting generalizability of the study results.
To avoid review bias, laboratory analyses were performed by personnel that was blinded to the TS POC results (and other reference test results). Reading of the CT scans was done by two independent readers, who were also blinded to the TS POC result. A two-factorial design was used, during which the TS POC was interpreted by two readers. While the training was necessary to ensure high quality data collection and correct recruitment, challenges for independent reading of the TS POC test appeared. Given the rural and door-to-door setting, it was difficult to ensure complete blindness by the second reader, which might lead to a bias in the results. Solutions, such as a window cover, were implemented.
This community-based study was expected to define the accuracy measures for the TS POC test for the detection of T, CC, and NCC, for its use in the community. Besides the aforementioned benefits of increased efficiency, the two-phase design was thus also particularly useful as the index test was evaluated at a point in the diagnostic pathway where it is meant to be used in practice [
16]. If the TS POC test for T proves to have a good sensitivity, the test can be used to screen people in the community. The early detection of tapeworm carriers is crucial to stop disease transmission as it ensures a rapid halt to environmental contamination with infective eggs, reducing not only the risk of new (N)CC cases, but also of porcine cysticercosis, and thus breaking the life cycle. A rapid test with high sensitivity is thus particularly useful for control programs against
T. solium, allowing selective chemotherapy of people who test T positive during screening. Besides its usefulness in control programs, the simultaneous detection of T and CC also makes the TS POC test a valuable tool for epidemiological research, and to monitor the effectiveness of interventions of control or elimination programs [
18].
The study also evaluated if the TS POC test has good predictive values for the detection of NCC, symptomatic or not, which could contribute to an improved diagnosis and referral of test positive people to district hospitals, where further diagnosis and follow-up can be made. Additionally, in areas with ongoing mass drug administration programs with praziquantel and/or albendazole, the test could potentially identify people that may be at risk for the presence of viable cysticerci in the central nervous system. Nevertheless, before the implementation of the tool as a screening device for NCC cases, additional studies must be performed to evaluate the cost-effectiveness of such strategies and whether screening with the TS POC test is also associated with improved patient outcomes [
19]. An assessment of the clinical importance of the TS POC test should then preferably be done using a diagnostic randomized controlled trial [
20].


 ,
, 


{kind=link}
{kind=link}