
Optical Coherence Tomography Angiography in Type 1 Diabetes Mellitus. Report 4: Glycated Haemoglobin

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design & Study Protocol
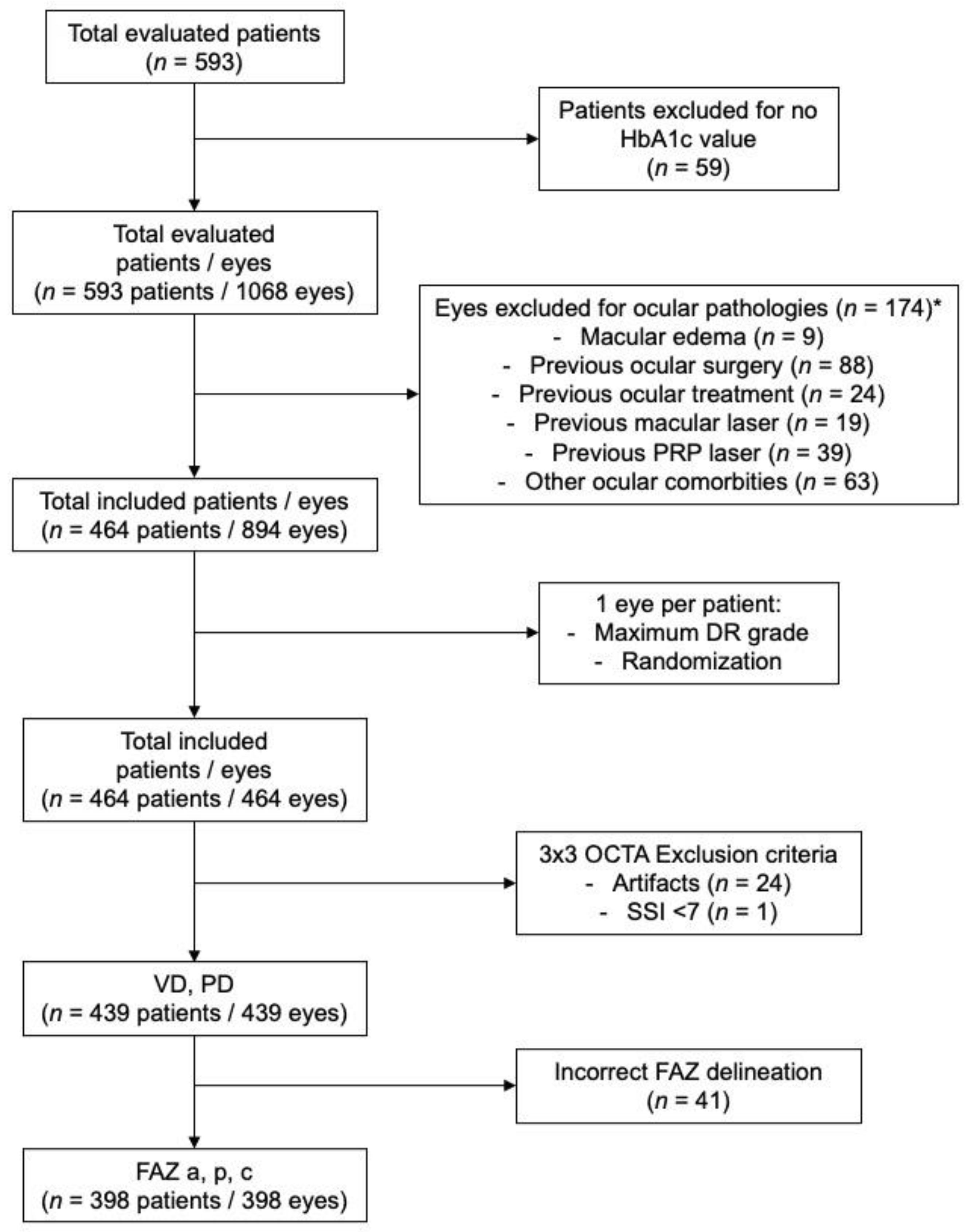
2.2. Inclusion and Exclusion Criteria
2.3. Ocular and Systemic Data
2.4. Glycated Haemoglobin Measurements and Definitions
2.5. Structural OCT and OCTA Imaging Protocols
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Study Groups
3.2. HbA1c Analysis by Study Groups
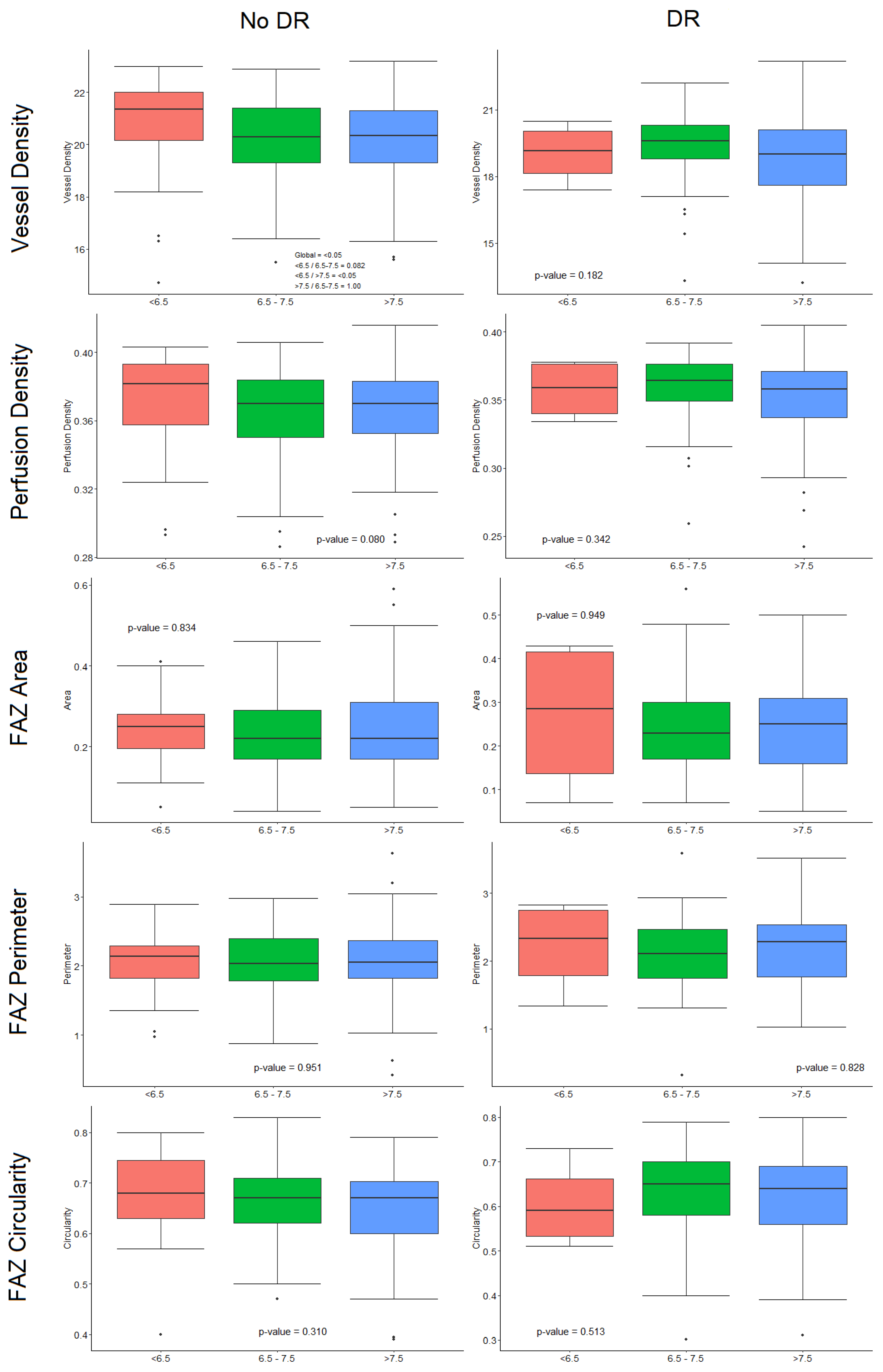
3.3. Differences in OCT and OCTA Parameters by HbA1c Levels
3.4. Influence of 5-Years HbA1c Levels Variability and Progression on OCTA Parameters
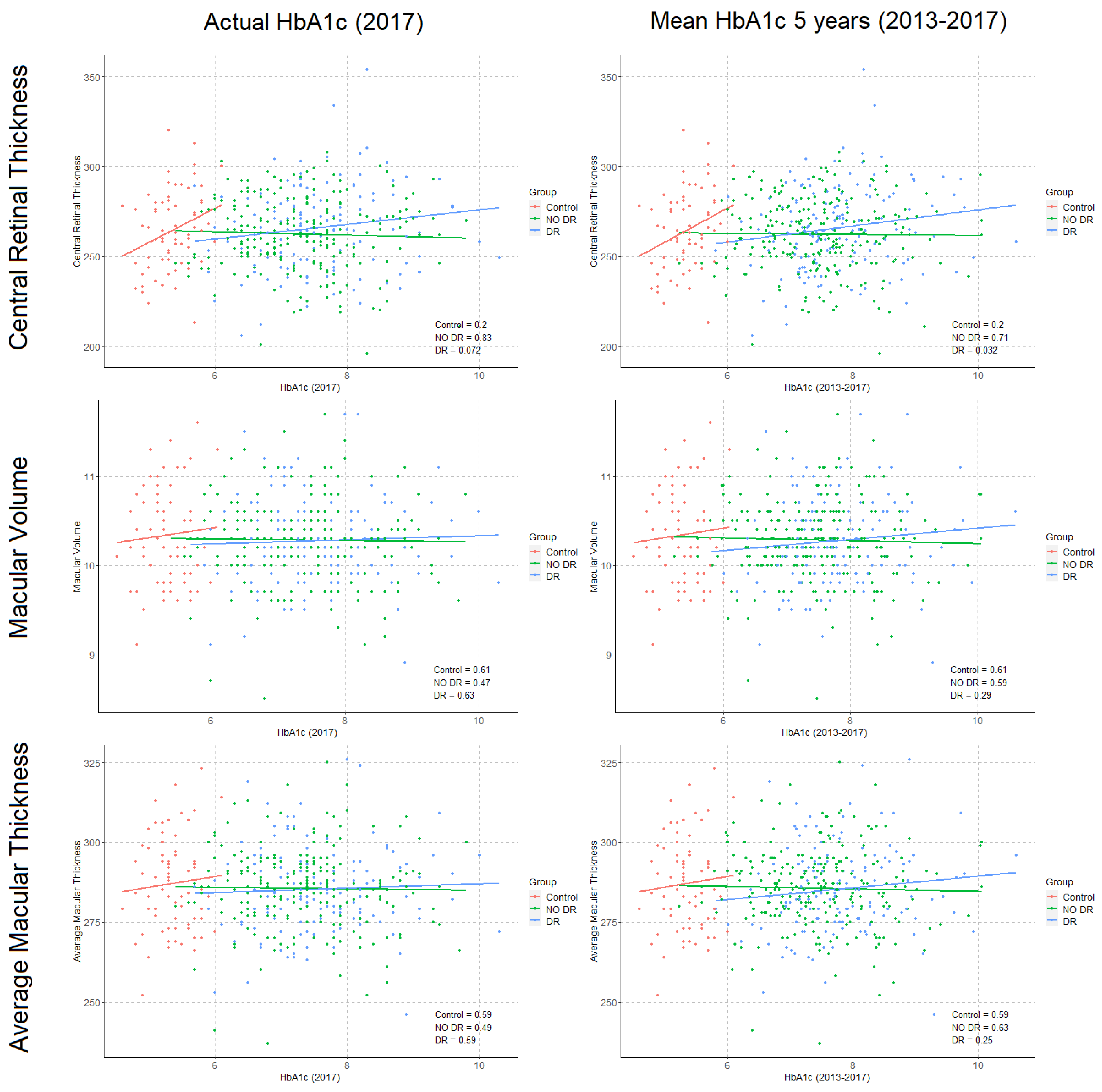
3.5. Correlations between HbA1c Levels and Structural OCT and OCTA Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wagner, S.K.; Fu, D.J.; Faes, L.; Liu, X.; Huemer, J.; Khalid, H.; Ferraz, D.; Korot, E.; Kelly, C.; Balaskas, K.; et al. Insights into Systemic Disease through Retinal Imaging-Based Oculomics. Transl. Vis. Sci. Technol. 2020, 9, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, F.; Muthy, Z.A.; Gallacher, J.; Sudlow, C.; Rees, G.; Yang, Q.; Keane, P.A.; Petzold, A.; Khaw, P.T.; Reisman, C.; et al. Association of Retinal Nerve Fiber Layer Thinning with Current and Future Cognitive Decline: A Study Using Optical Coherence Tomography. JAMA Neurol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Di Renzo, A.; Ziccardi, L.; Martelli, F.; Fadda, A.; Manni, G.; Barboni, P.; Pierelli, F.; Sadun, A.A.; Parisi, V. Optical Coherence Tomography in Alzheimer’s Disease: A Meta-Analysis. PLoS ONE 2015, 10, e0134750. [Google Scholar] [CrossRef]
- Mutlu, U.; Colijn, J.M.; Ikram, M.A.; Bonnemaijer, P.W.M.; Licher, S.; Wolters, F.J.; Tiemeier, H.; Koudstaal, P.J.; Klaver, C.C.W.; Ikram, M.K. Association of Retinal Neurodegeneration on Optical Coherence Tomography with Dementia: A Population-Based Study. JAMA Neurol. 2018, 75, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H. Retinal Microvascular Signs and Disability in the Cardiovascular Health Study. Arch. Ophthalmol. 2012, 130, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Günthner, R.; Hanssen, H.; Hauser, C.; Angermann, S.; Lorenz, G.; Kemmner, S.; Matschkal, J.; Braunisch, M.C.; Küchle, C.; Renders, L.; et al. Impaired Retinal Vessel Dilation Predicts Mortality in End-Stage Renal Disease. Circ. Res. 2019, 124, 1796–1807. [Google Scholar] [CrossRef]
- McGeechan, K.; Liew, G.; Macaskill, P.; Irwig, L.; Klein, R.; Klein, B.E.K.; Wang, J.J.; Mitchell, P.; Vingerling, J.R.; de Jong, P.T.V.M.; et al. Prediction of Incident Stroke Events Based on Retinal Vessel Caliber: A Systematic Review and Individual-Participant Meta-Analysis. Am. J. Epidemiol. 2009, 170, 1323–1332. [Google Scholar] [CrossRef]
- McGeechan, K. Meta-analysis: Retinal Vessel Caliber and Risk for Coronary Heart Disease. Ann. Intern. Med. 2009, 151, 404. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Mitchell, P. Hypertensive Retinopathy. N. Engl. J. Med. 2004, 351, 2310–2317. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Mohamed, Q.; Klein, R.; Couper, D.J. Do retinopathy signs in non-diabetic individuals predict the subsequent risk of diabetes? Br. J. Ophthalmol. 2006, 90, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Ting, D.S.W.; Tan, G.S.W.; Agrawal, R.; Yanagi, Y.; Sie, N.M.; Wong, C.W.; Yeo, I.Y.S.; Lee, S.Y.; Cheung, C.M.G.; Wong, T.Y. Optical coherence tomographic angiography in type 2 diabetes and diabetic retinopathy. JAMA Ophthalmol. 2017, 135, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Barraso, M.; Alé-Chilet, A.; Hernández, T.; Oliva, C.; Vinagre, I.; Ortega, E.; Figueras-Roca, M.; Sala-Puigdollers, A.; Esquinas, C.; Esmatjes, E.; et al. Optical Coherence Tomography Angiography in Type 1 Diabetes Mellitus. Report 1: Diabetic Retinopathy. Transl. Vis. Sci. Technol. 2020, 9, 34. [Google Scholar] [CrossRef]
- Diabetes Control and Complications Trial Research. The Relationship of Glycemic Exposure (HbA1c) to the Risk of Development and Progression of Retinopathy in the Diabetes Control and Complications Trial. Diabetes 1995, 44, 968–983. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Nathan, D.M.; Balkau, B.; Bonora, E.; Borch-Johnsen, K.; Buse, J.B.; Colagiuri, S.; Davidson, M.B.; DeFronzo, R.; Genuth, S.; Holman, R.R.; et al. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. CPD Bull. Clin. Biochem. 2010, 10, 25–33. [Google Scholar]
- American Diabetes Association. Standards of Medical Care in Diabetes—2010. Diabetes Care 2010, 33, S11–S61. [Google Scholar] [CrossRef] [Green Version]
- Sato, K.K.; Hayashi, T.; Harita, N.; Yoneda, T.; Nakamura, Y.; Endo, G.; Kambe, H. Combined measurement of fasting plasma glucose and A1C is effective for the prediction of type 2 diabetes. Diabetes Care 2009, 32, 644–646. [Google Scholar] [CrossRef] [Green Version]
- Edelman, D.; Olsen, M.K.; Dudley, T.K.; Harris, A.C.; Oddone, E.Z. Utility of hemoglobin A1c in predicting diabetes risk. J. Gen. Intern. Med. 2004, 19, 1175–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buse, J.B.; Ginsberg, H.N.; Bakris, G.L.; Clark, N.G.; Costa, F.; Eckel, R.; Fonseca, V.; Gerstein, H.C.; Grundy, S.; Nesto, R.W.; et al. Primary prevention of cardiovascular diseases in people with diabetes mellitus: A scientific statement from the American Heart Association and the American Diabetes Association. Diabetes Care 2007, 30, 162–172. [Google Scholar] [CrossRef] [Green Version]
- Ting, D.S.W.; Peng, L.; Varadarajan, A.V.; Liu, T.Y.A. Novel Retinal Imaging in Assessment of Cardiovascular Risk Factors and Systemic Vascular Diseases. Front. Diabetes 2019, 27, 106–118. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Wong, T.Y. Eyeing cardiovascular risk factors. Nat. Biomed. Eng. 2018, 2, 140–141. [Google Scholar] [CrossRef]
- Subrayan, V.; Menon, S.; Peyman, M.; loo voon pei, A. Correlation between optical coherence tomography-derived macular measurements and glycosylated haemoglobin, age, visual acuity and diabetes duration in patients with type 2 diabetes mellitus. Int. J. Diabetes Dev. Ctries. 2015, 35, 385–388. [Google Scholar] [CrossRef]
- Chou, T.H.; Wu, P.C.; Kuo, J.Z.C.; Lai, C.H.; Kuo, C.N. Relationship of diabetic macular oedema with glycosylated haemoglobin. Eye 2009, 23, 1360–1363. [Google Scholar] [CrossRef] [Green Version]
- Torabi, H.; Isfeedvajani, M.S.; Ramezani, M.; Daryabari, S.H. Choroidal thickness and hemoglobin A1c levels in patients with type 2 diabetes mellitus. J. Ophthalmic Vis. Res. 2019, 14, 285–290. [Google Scholar] [CrossRef] [Green Version]
- Hamed, A.H.; Bayoumi, H.M.; Abdulmonem, A.M. Optical Coherence Tomography Assessment of Macular and Choroidal Thickness in Patients with Proliferative Diabetic Retinopathy in Relation to Hemoglobin A1C. Egypt. J. Hosp. Med. 2019, 77, 5355–5366. [Google Scholar] [CrossRef]
- Gołębiewska, J.; Olechowski, A.; Wysocka-Mincewicz, M.; Odrobina, D.; Baszyńska-Wilk, M.; Groszek, A.; Szalecki, M.; Hautz, W. Optical coherence tomography angiography vessel density in children with type 1 diabetes. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Zarranz-Ventura, J.; Barraso, M.; Alé-Chilet, A.; Hernandez, T.; Oliva, C.; Gascón, J.; Sala-Puigdollers, A.; Figueras-Roca, M.; Vinagre, I.; Ortega, E.; et al. Evaluation of microvascular changes in the perifoveal vascular network using optical coherence tomography angiography (OCTA) in type I diabetes mellitus: A large scale prospective trial. BMC Med. Imaging 2019, 19, 91. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, C.P.; Ferris, F.L.; Klein, R.E.; Lee, P.P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T.; et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef]
- Zeng, Y.; Cao, D.; Yu, H.; Yang, D.; Zhuang, X.; Hu, Y.; Li, J.; Yang, J.; Wu, Q.; Liu, B.; et al. Early retinal neurovascular impairment in patients with diabetes without clinically detectable retinopathy. Br. J. Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Cao, D.; Yang, D.; Huang, Z.; Zeng, Y.; Wang, J.; Hu, Y.; Zhang, L. Optical coherence tomography angiography discerns preclinical diabetic retinopathy in eyes of patients with type 2 diabetes without clinical diabetic retinopathy. Acta Diabetol. 2018, 55, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Ishibazawa, A.; Nagaoka, T.; Takahashi, A.; Omae, T.; Tani, T.; Sogawa, K.; Yokota, H.; Yoshida, A. Optical Coherence Tomography Angiography in Diabetic Retinopathy: A Prospective Pilot Study. Am. J. Ophthalmol. 2015, 160, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.Y.; Chu, Z.; Shahidzadeh, A.; Wang, R.K.; Puliafito, C.A.; Kashani, A.H. Quantifying microvascular density and morphology in diabetic retinopathy using spectral-domain optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT362–OCT370. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, G.; Chihara, E.; Takahashi, H.; Amano, H.; Okazaki, K. Quantitative retinal optical coherence tomography angiography in patients with diabetes without diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 190–196. [Google Scholar] [CrossRef]
- Yeung, L.; Sun, C.C.; Ku, W.C.; Chuang, L.H.; Chen, C.H.; Huang, B.Y.; Ting, M.K.; Yang, K.J. Associations between chronic glycosylated haemoglobin (HbA1c) level and macular volume in diabetes patients without macular oedema. Acta Ophthalmol. 2010, 88, 753–758. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Eyes (C/No DR/DR) | Statistics | Control | No DR | DR | p-Value | p-Value Adjusted |
|---|---|---|---|---|---|---|---|
| General characteristics | |||||||
| Age (years) | (72/247/145) | Mean (SD) | 47.04 (14.03) | 38.34 (12.55) | 41.16 (10.80) | <0.05 | - |
| Median (Q1, Q3) | 48.65 (34.80, 59.65) | 37.10 (27.55, 47.40) | 39.30 (33.70, 48.70) | ||||
| Sex, female | (72/247/145) | n (%) | 47 (65.3%) | 131 (53.0%) | 70 (48.3%) | 0.060 | - |
| Smoking habits | (72/246/145) | ||||||
| Non smoker | n (%) | 52 (72.2%) | 158 (64.2%) | 86 (59.3%) | 0.633 | - | |
| Actual smoker | n (%) | 4 (5.6%) | 53 (21.5%) | 31 (21.4%) | 0.284 | - | |
| Ex-smoker | n (%) | 16 (22.2%) | 35 (14.2%) | 28 (19.3%) | 0.595 | - | |
| Hypertension | (71/247/145) | n (%) | 9 (12.7%) | 20 (8.1%) | 19 (13.1%) | 0.229 | - |
| BMI (kg/m2) | (70/244/145) | Mean (SD) | 23.54 (3.34) | 24.43 (3.72) | 25.35 (3.80) | <0.05 | - |
| Median (Q1, Q3) | 23.48 (21.17, 25.52) | 23.80 (21.66, 26.86) | 24.69 (22.72, 27.40) | ||||
| Diabetes-related characteristics | |||||||
| DM duration (years) | (0/246/143) | Mean (SD) | 0.00 (0.00) | 16.29 (9.65) | 25.97 (8.97) | <0.05 * | - |
| Median (Q1, Q3) | 0.00 (0.00, 0.00) | 15.85 (8.43, 21.85) | 26.00 (20.35, 32.25) | ||||
| Macrovascular complications | (72/246/145) | ||||||
| Cerebrovascular disease | n (%) | 0 (0.0%) | 1 (0.4%) | 3 (2.1%) | 0.158 | - | |
| Ischemic heart disease | n (%) | 1 (1.4%) | 2 (0.8%) | 2 (1.4%) | 0.839 | - | |
| Peripheral vascular disease | n (%) | 0 (0.0%) | 1 (0.4%) | 1 (0.7%) | 0.763 | - | |
| Insulin requirements (UI/kg) | (0/243/145) | Mean (SD) | 0.00 (0.00) | 0.62 (0.24) | 0.65 (0.24) | 0.127 * | - |
| Median (Q1, Q3) | 0.00 (0.00, 0.00) | 0.60 (0.45, 0.78) | 0.64 (0.51, 0.80) | ||||
| HbA1c (2017) | (72/242/141) | Mean (SD) | 5.37 (0.33) | 7.34 (0.86) | 7.54 (0.87) | <0.05 | <0.05 |
| Median (Q1, Q3) | 5.35 (5.18, 5.60) | 7.30 (6.70, 7.80) | 7.40 (7.00, 8.10) | ||||
| Mean HbA1c (2017–2013) | (72/247/145) | Mean (SD) | 5.37 (0.33) | 7.46 (0.87) | 7.79 (0.83) | <0.05 | <0.05 |
| Median (Q1, Q3) | 5.35 (5.18, 5.60) | 7.48 (6.84, 7.97) | 7.72 (7.23, 8.20) | ||||
| Ocular Measurements | |||||||
| Visual Acuity | (72/247/145) | Mean (SD) | 0.97 (0.06) | 0.98 (0.58) | 0.93 (0.11) | <0.05 | - |
| Median (Q1, Q3) | 1.00 (0.99, 1.00) | 0.95 (0.95, 1.00) | 0.95 (0.90, 1.00) | ||||
| Axial Length (mm) | (72/245/144) | Mean (SD) | 23.65 (1.00) | 23.65 (1.14) | 23.33 (1.17) | <0.05 | - |
| Median (Q1, Q3) | 23.48 (22.88, 24.42) | 23.53 (22.84, 24.40) | 23.19 (22.66, 23.90) | ||||
| OCTA—3 × 3 mm | |||||||
| Vessel Density (mm−1) | (67/236/136) | Mean (SD) | 20.65 (1.87) | 20.26 (1.59) | 19.00 (1.86) | <0.05 | <0.05 |
| Median (Q1, Q3) | 21.10 (20.05, 22.00) | 20.50 (19.30, 21.40) | 19.40 (18.05, 20.20) | ||||
| Perfusion Density | (67/236/136) | Mean (SD) | 0.370 (0.031) | 0.366 (0.026) | 0.354 (0.029) | <0.05 | 0.087 |
| Median (Q1, Q3) | 0.377 (0.363, 0.391) | 0.371 (0.352, 0.385) | 0.362 (0.341, 0.375) | ||||
| FAZ Area (mm2) | (62/216/120) | Mean (SD) | 0.230 (0.086) | 0.236 (0.100) | 0.243 (0.106) | 0.810 | 0.691 |
| Median (Q1, Q3) | 0.225 (0.170, 0.290) | 0.225 (0.170, 0.290) | 0.230 (0.160, 0.310) | ||||
| FAZ Perimeter (mm) | (62/216/120) | Mean (SD) | 2.049 (0.409) | 2.046 (0.495) | 2.150 (0.537) | 0.124 | 0.271 |
| Median (Q1, Q3) | 2.085 (1.782, 2.282) | 2.060 (1.788, 2.370) | 2.200 (1.750, 2.532) | ||||
| FAZ Circularity | (62/216/120) | Mean (SD) | 0.665 (0.078) | 0.659 (0.078) | 0.623 (0.097) | <0.05 | 0.151 |
| Median (Q1, Q3) | 0.670 (0.620, 0.720) | 0.670 (0.617, 0.710) | 0.640 (0.570, 0.690) | ||||
| OCT–Macular Cube | |||||||
| Central Macular Thickness (μm) | (69/241/143) | Mean (SD) | 264.61 (21.68) | 262.26 (20.23) | 265.92 (22.92) | 0.252 | 0.489 |
| Median (Q1, Q3) | 264.0 (248.0, 280.0) | 262.0 (250.0, 276.0) | 265.0 (250.0, 281.5) | ||||
| Macular Volume | (69/241/143) | Mean (SD) | 10.34 (0.54) | 10.28 (0.45) | 10.27 (0.49) | 0.706 | 0.454 |
| Median (Q1, Q3) | 10.3 (9.9, 10.7) | 10.3 (10.0, 10.6) | 10.2 (9.9, 10.6) | ||||
| Average Macular Thickness (μm) | (69/241/143) | Mean (SD) | 287.06 (14.83) | 285.52 (12.58) | 285.29 (13.45) | 0.707 | 0.425 |
| Median (Q1, Q3) | 285.0 (276.0, 296.0) | 286.0 (279.0, 293.0) | 284.0 (276.0, 293.5) |
| Diabetic Retinopathy | Statistics | HbA1c Levels (%) | p-Value | |||
|---|---|---|---|---|---|---|
| <6.5 | 6.5–7.5 | >7.5 | ||||
| No DR | OCTA parameter | (Eyes = 32) | (Eyes = 94) | (Eyes = 110) | ||
| Vessel Density (mm-1) | Mean (SD) | 20.71 (1.97) | 20.22 (1.50) | 20.16 (1.53) | <0.05 | |
| Median (Q1, Q3) | 21.35 (20.18, 22.00) | 20.35 (19.30, 21.30) | 20.35 (19.30, 21.30) | |||
| Perfusion Density | Mean (SD) | 0.373 (0.029) | 0.365 (0.025) | 0.366 (0.025) | 0.080 | |
| Median (Q1, Q3) | 0.382 (0.358, 0.393) | 0.370 (0.350, 0.384) | 0.370 (0.353, 0.383) | |||
| (Eyes = 31) | (Eyes = 89) | (Eyes = 96) | ||||
| FAZ Area (mm2) | Mean (SD) | 0.237 (0.081) | 0.233 (0.098) | 0.238 (0.107) | 0.834 | |
| Median (Q1, Q3) | 0.250 (0.195, 0.280) | 0.220 (0.170, 0.290) | 0.220 (0.170, 0.310) | |||
| FAZ Perimeter (mm) | Mean (SD) | 2.041 (0.446) | 2.059 (0.463) | 2.036 (0.541) | 0.951 | |
| Median (Q1, Q3) | 2.140 (1.825, 2.295) | 2.030 (1.780, 2.400) | 2.055 (1.823, 2.363) | |||
| FAZ Circularity | Mean (SD) | 0.677 (0.082) | 0.661 (0.071) | 0.651 (0.083) | 0.310 | |
| Median (Q1, Q3) | 0.680 (0.630, 0.745) | 0.670 (0.620, 0.710) | 0.670 (0.600, 0.703) | |||
| OCT parameter | (Eyes = 33) | (Eyes = 95) | (Eyes = 113) | |||
| Macular Central Thickness (μm) | Mean (SD) | 261.21 (21.70) | 262.68 (17.79) | 262.21 (21.83) | 0.937 | |
| Median (Q1, Q3) | 260.0 (246.0, 276.0) | 263.0 (251.0, 276.0) | 263.0 (248.0, 276.0) | |||
| Macular Volume | Mean (SD) | 10.25 (0.49) | 10.26 (0.41) | 10.31 (0.48) | 0.736 | |
| Median (Q1, Q3) | 10.3 (10.1, 10.5) | 10.3 (10.1, 10.5) | 10.3 (10.0, 10.6) | |||
| Macular Average Thickness (μm) | Mean (SD) | 284.52 (13.87) | 284.96 (11.29) | 286.27 (13.26) | 0.799 | |
| Median (Q1, Q3) | 286.0 (279.0, 292.0) | 285.0 (279.0, 291.5) | 286.0 (278.0, 294.0) | |||
| DR | OCTA parameter | (Eyes = 4) | (Eyes = 51) | (Eyes = 81) | ||
| Vessel Density (mm-1) | Mean (SD) | 19.05 (1.41) | 19.31 (1.68) | 18.80 (1.97) | 0.182 | |
| Median (Q1, Q3) | 19.15 (18.15, 20.05) | 19.60 (18.80, 20.30) | 19.00 (17.60, 20.10) | |||
| Perfusion Density | Mean (SD) | 0.358 (0.023) | 0.359 (0.026) | 0.352 (0.031) | 0.342 | |
| Median (Q1, Q3) | 0.359 (0.340, 0.377) | 0.364 (0.349, 0.377) | 0.358 (0.337, 0.371) | |||
| (Eyes = 4) | (Eyes = 45) | (Eyes = 71) | ||||
| FAZ Area (mm2) | Mean (SD) | 0.268 (0.180) | 0.244 (0.108) | 0.240 (0.102) | 0.949 | |
| Median (Q1, Q3) | 0.285 (0.138, 0.415) | 0.230 (0.170, 0.300) | 0.250 (0.160, 0.310) | |||
| FAZ Perimeter (mm) | Mean (SD) | 2.208 (0.701) | 2.112 (0.559) | 2.171 (0.521) | 0.828 | |
| Median (Q1, Q3) | 2.330 (1.790, 2.748) | 2.110 (1.750, 2.470) | 2.280 (1.770, 2.535) | |||
| FAZ Circularity | Mean (SD) | 0.605 (0.100) | 0.634 (0.098) | 0.617 (0.097) | 0.513 | |
| Median (Q1, Q3) | 0.590 (0.533, 0.663) | 0.650 (0.580, 0.700) | 0.640 (0.560, 0.690) | |||
| OCT parameter | (Eyes = 5) | (Eyes = 56) | (Eyes = 82) | |||
| Macular Central Thickness (μm) | Mean (SD) | 251.20 (29.21) | 260.00 (20.81) | 270.87 (22.85) | <0.05 | |
| Median (Q1, Q3) | 253.0 (245.0, 269.0) | 261.0 (243.8, 273.5) | 270.5 (257.3, 284.8) | |||
| Macular Volume | Mean (SD) | 9.96 (0.22) | 10.28 (0.50) | 10.29 (0.49) | 0.335 | |
| Median (Q1, Q3) | 9.9 (9.9, 10.0) | 10.2 (9.9, 10.6) | 10.3 (10.0, 10.6) | |||
| Macular Average Thickness (μm) | Mean (SD) | 276.20 (6.06) | 285.36 (13.66) | 285.79 (13.54) | 0.303 | |
| Median (Q1, Q3) | 274.0 (274.0, 279.0) | 284.0 (277.5, 293.3) | 285.0 (277.3, 294.0) |
| No DR | DR | ||||||
|---|---|---|---|---|---|---|---|
| OCTA Parameter | Statistics | High Variability | Low Variability | p-Value Adjusted | High Variability | Low Variability | p-Value Adjusted |
| (Eyes = 107) | (Eyes = 109) | (Eyes = 64) | (Eyes = 63) | ||||
| Vessel Density (mm−1) | Mean (SD) | 20.25 (1.57) | 20.35 (1.58) | 0.905 | 18.93 (2.00) | 19.12 (1.76) | 0.635 |
| Median (Q1, Q3) | 20.40 (19.30, 21.40) | 20.50 (19.60, 21.50) | 19.10 (17.80, 20.22) | 19.50 (18.40, 20.20) | |||
| Perfusion Density | Mean (SD) | 0.365 (0.025) | 0.369 (0.026) | 0.699 | 0.353 (0.033) | 0.357 (0.026) | 0.475 |
| Median (Q1, Q3) | 0.370 (0.352, 0.383) | 0.372 (0.354, 0.389) | 0.362 (0.337, 0.376) | 0.362 (0.347, 0.374) | |||
| (Eyes = 96) | (Eyes = 101) | (Eyes = 56) | (Eyes = 57) | ||||
| FAZ Area (mm2) | Mean (SD) | 0.24 (0.11) | 0.24 (0.10) | 0.572 | 0.25 (0.11) | 0.23 (0.10) | 0.466 |
| Median (Q1, Q3) | 0.23 (0.17, 0.30) | 0.23 (0.17, 0.31) | 0.26 (0.17, 0.31) | 0.23 (0.16, 0.29) | |||
| FAZ Perimeter (mm) | Mean (SD) | 2.07 (0.47) | 2.06 (0.54) | 0.861 | 2.17 (0.62) | 2.13 (0.44) | 0.998 |
| Median (Q1, Q3) | 2.06 (1.85, 2.35) | 2.12 (1.77, 2.41) | 2.29 (1.72, 2.55) | 2.11 (1.77, 2.45) | |||
| FAZ Circularity | Mean (SD) | 0.66 (0.08) | 0.66 (0.08) | 0.786 | 0.63 (0.10) | 0.62 (0.09) | 0.934 |
| Median (Q1, Q3) | 0.67 (0.60, 0.71) | 0.67 (0.63, 0.71) | 0.66 (0.58, 0.69) | 0.63 (0.57, 0.69) | |||
| Positive progression | Negative progression | Positive progression | Negative progression | ||||
| (Eyes = 94) | (Eyes = 107) | (Eyes = 36) | (Eyes = 80) | ||||
| Vessel Density (mm−1) | Mean (SD) | 20.31 (1.67) | 20.30 (1.48) | 0.359 | 19.46 (1.93) | 18.80 (1.82) | 0.136 |
| Median (Q1, Q3) | 20.70 (19.22, 21.40) | 20.40 (19.40, 21.40) | 19.70 (18.25, 20.92) | 19.30 (17.88, 20.10) | |||
| Perfusion Density | Mean (SD) | 0.367 (0.027) | 0.367 (0.024) | 0.185 | 0.360 (0.029) | 0.352 (0.029) | 0.146 |
| Median (Q1, Q3) | 0.374 (0.353, 0.388) | 0.371 (0.353, 0.383) | 0.362 (0.347, 0.382) | 0.363 (0.341, 0.369) | |||
| (Eyes = 88) | (Eyes = 95) | (Eyes = 33) | (Eyes = 70) | ||||
| FAZ Area (mm2) | Mean (SD) | 0.24 (0.10) | 0.24 (0.11) | 0.314 | 0.23 (0.09) | 0.25 (0.11) | 0.913 |
| Median (Q1, Q3) | 0.23 (0.18, 0.31) | 0.23 (0.17, 0.29) | 0.23 (0.16, 0.29) | 0.23 (0.17, 0.32) | |||
| FAZ Perimeter (mm) | Mean (SD) | 2.09 (0.51) | 2.03 (0.51) | 0.154 | 2.11 (0.44) | 2.17 (0.58) | 0.977 |
| Median (Q1, Q3) | 2.09 (1.86, 2.42) | 2.11 (1.71, 2.32) | 2.14 (1.67, 2.47) | 2.25 (1.78, 2.58) | |||
| FAZ Circularity | Mean (SD) | 0.65 (0.08) | 0.67 (0.07) | 0.069 | 0.64 (0.08) | 0.62 (0.10) | 0.294 |
| Median (Q1, Q3) | 0.66 (0.60, 0.70) | 0.67 (0.63, 0.71) | 0.63 (0.60, 0.68) | 0.65 (0.55, 0.69) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Morales, C.; Alé-Chilet, A.; Martín-Pinardel, R.; Barraso, M.; Hernández, T.; Oliva, C.; Vinagre, I.; Ortega, E.; Figueras-Roca, M.; Sala-Puigdollers, A.; et al. Optical Coherence Tomography Angiography in Type 1 Diabetes Mellitus. Report 4: Glycated Haemoglobin. Diagnostics 2021, 11, 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091537
Bernal-Morales C, Alé-Chilet A, Martín-Pinardel R, Barraso M, Hernández T, Oliva C, Vinagre I, Ortega E, Figueras-Roca M, Sala-Puigdollers A, et al. Optical Coherence Tomography Angiography in Type 1 Diabetes Mellitus. Report 4: Glycated Haemoglobin. Diagnostics. 2021; 11(9):1537. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091537
Chicago/Turabian StyleBernal-Morales, Carolina, Aníbal Alé-Chilet, Ruben Martín-Pinardel, Marina Barraso, Teresa Hernández, Cristian Oliva, Irene Vinagre, Emilio Ortega, Marc Figueras-Roca, Anna Sala-Puigdollers, and et al. 2021. "Optical Coherence Tomography Angiography in Type 1 Diabetes Mellitus. Report 4: Glycated Haemoglobin" Diagnostics 11, no. 9: 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091537