
The Assessment of the Usefulness of Prenatal Magnetic Resonance Imaging in the Diagnosis of Central Nervous System Defects

 and
and
Abstract
:1. Introduction
2. Materials and Methods
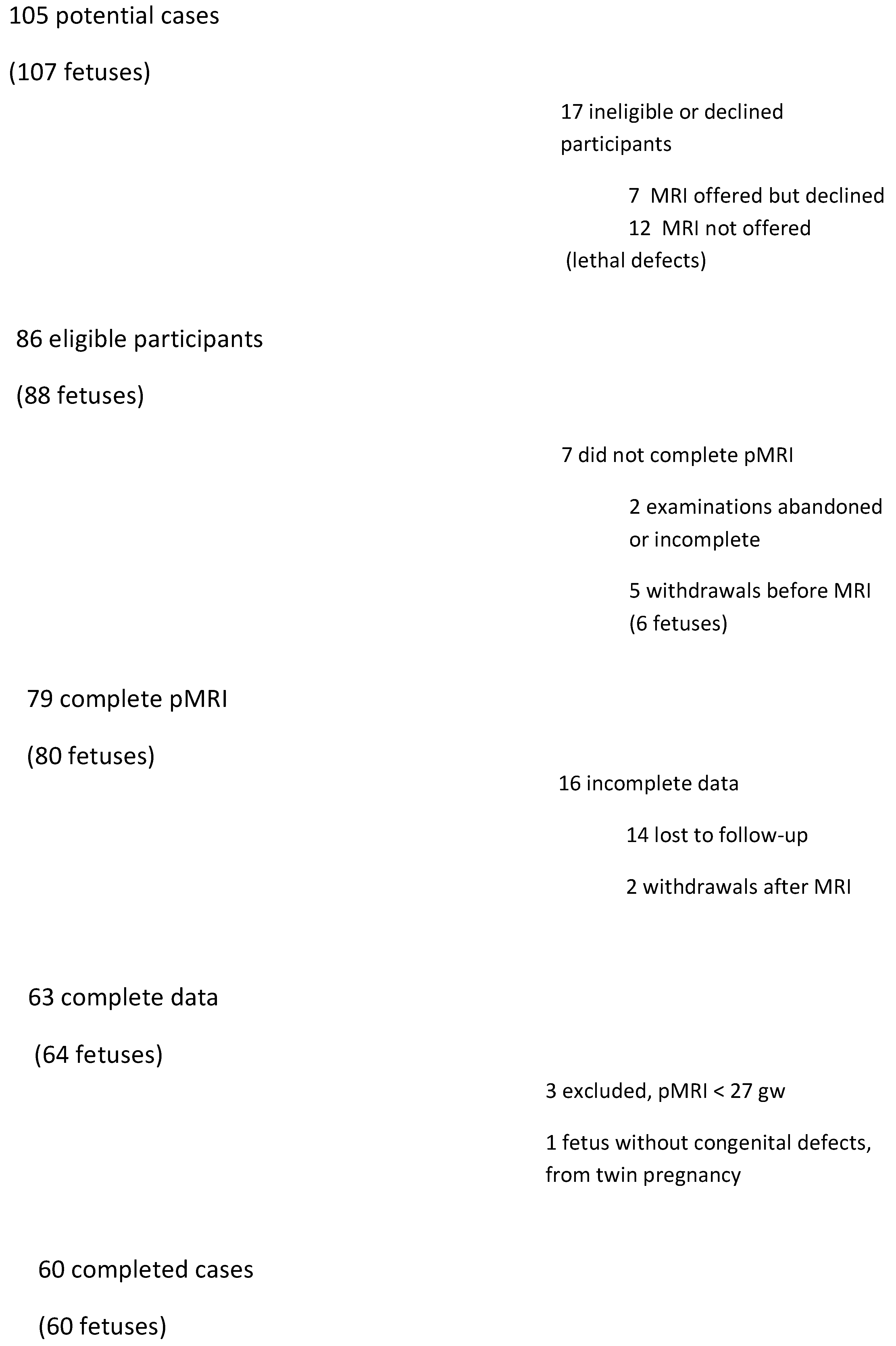
2.1. The Study Group
2.2. Criteria for Inclusion in the Study
2.3. Exclusion Criteria
2.4. Study Protocol
2.5. Prenatal MRI
2.6. Verification of Results
2.7. Statistical Analysis of Results
2.8. Definitions
3. Results
3.1. Study Sample Features
3.2. Consistency of Diagnosis
3.2.1. Ventriculomegaly
3.2.2. Central Line Defects
Agenesis of Corpus Callosum
Holoprosencephaly
Agenesis of the Cavum Septum Pellucidum
3.2.3. Defects of the Posterior Fossa
Defects of the Cerebellum
Dandy-Walker Syndrome
Arnold-Chiari Syndrome
3.2.4. Disorders of Neural Migration and Proliferation
Lysencephaly
Schizencephaly
Microcephaly
3.2.5. Other Irregularities
Abnormalities Related to Peripheral Nervous System Defects
Meningo-Spinal Hernia
Arachnoid Cyst
3.2.6. Additional Irregularities Detected in pMRI
4. Discussion
4.1. Main Findings
- high agreement of diagnoses of ventriculomegaly,
- relatively high agreement of diagnoses of midline defects,
- relatively high agreement of diagnoses of posterior fossa defects,
- fairly high agreement of diagnoses of neuronal angulation and migration defects and of neuronal proliferation defects.
4.2. What Is Known
4.3. Future Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Latos-Bieleńska, A.; Materna-Kiryluk, A. Wrodzone Wady Rozwojowe w Polsce w Latach 2005–2006; Dane z Polskiego Rejestru Wrodzonych Wad Rozwojowych. Ośrodek Wydawnictw Naukowych: Poznań, Poland, 2010. [Google Scholar]
- Herman-Sucharska, I.; Urbanik, A. Badanie MR w obrazowaniu wad ośrodkowego układu nerwowego płodu. Przegl. Lek. 2007, 64, 917–922. [Google Scholar] [PubMed]
- Vergani, P.; Locatelli, A.; Strobelt, N.; Cavallone, M.; Ceruti, P.; Paterlini, G.; Ghidini, A. Clinical outcome of mild fetal ventriculomegaly. Am. J. Obstet. Gynecol. 1998, 178, 218–222. [Google Scholar] [CrossRef]
- Available online: www.eurocat-network.eu (accessed on 16 August 2018).
- Helwich, E.; Bekiesińska-Figatowska, M.; Bokiniec, R. Rekomendacje dotyczące badań obrazowych ośrodkowego układu nerwowego u płodów i noworodków. J. Ultrason. 2014, 14, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.D.; Bradburn, M.; Campbell, M.J.; Cooper, C.L.; Graham, R.; Jarvis, D.; Kilby, M.D.; Mason, G.; Mooney, C.; Robson, S.C.; et al. Use of MRI in the diagnosis of fetal brain abnormalities in utero (MERIDIAN): A multicentre, prospective cohort study. Lancet 2017, 389, 538–546. [Google Scholar] [CrossRef] [Green Version]
- The ENSO Working Group; Di Mascio, D.; Khalil, A.; Thilaganathan, B.; Rizzo, G.; Buca, D.; Liberati, M.; Celentano, C.; Melchiorre, K.; Caulo, M.; et al. Role of prenatal magnetic resonance imaging in fetuses with isolated mild or moderate ventriculomegaly in the era of neurosonography: International multicenter study. Ultrasound Obstet. Gynecol. 2020, 56, 340–347. [Google Scholar] [CrossRef]
- The ENSO Working Group; Sileo, F.G.; Pilu, G.; Prayer, D.; Rizzo, G.; Khalil, A.; Managanaro, L.; Volpe, P.; Van Mieghem, T.; Bertucci, E.; et al. Role of prenatal magnetic resonance imaging in fetuses with isolated anomalies of corpus callosum: Multinational study. Ultrasound Obstet. Gynecol. 2021, 58, 26–33. [Google Scholar] [CrossRef]
- Rossi, A.C.; Prefumo, F. Additional value of fetal magnetic resonance imaging in the prenatal diagnosis of central nervous sys-tem anomalies: A systematic review of the literature. Ultrasound Obstet Gynecol. 2014, 44, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Herman-Sucharska, I. Rola Badania Płodu Techniką Rezonansu Magnetycznego w Nowoczesnej Diagnostyce i Poranictwie Prenatalnym u Dzieci z Wadami Rozszczepowymi Kręgosłupa: Rozprawa Habilitacyjna ZamKor P; Sagnowski i Wspólnicy: Krakow, Poland, 2010. [Google Scholar]
- Blaicher, W.; Bernaschek, G.; Deutinger, J.; Messerschmidt, A.; Schindler, E.; Prayer, D. Fetal and early postnatal magnetic resonance imaging—Is there a difference? J. Périnat. Med. 2004, 32, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Herman-Sucharska, I.; Jelińska, A.; Urbanik, A.; Tomaszczyk, J.; Zamłyński, J.; Pawlik, D.; Stawska, H. Wpływ prenatalnego badania MR na poradnictwo prenatalne i zmianę decyzji terapeutycznych u dzieci z wadami wrodzonymi ośrodkowego układu nerwowego. Przegl Lek. 2010, 67, 262–267. [Google Scholar] [PubMed]
- Whitby, E.H.; Paley, M.N.J.; Sprigg, A.; Rutter, S.; Davies, N.P.; Wilkinson, I.D.; Griffiths, P.D. Comparison of ultrasound and magnetic resonance imaging in 100 singleton preg-nancies with suspected brain abnormalities. BJOG 2004, 111, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Kul, S.; Korkmaz, H.A.A.; Cansu, A.; Dinc, H.; Ahmetoglu, A.; Guven, S.; Imamoglu, M. Contribution of MRI to ultrasound in the diagnosis of fetal anomalies. J. Magn. Reson. Imaging 2012, 35, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Bekiesińska-Figatowska, M.; Szkudlińska-Pawlak, S.; Romaniuk-Doroszewska, A.; Duczkowski, M.; Iwanowska, B.; Duczkowska, A.; Mądzik, J.; Brągoszewska, H. First experience with neonatal examinations with the use of MR-compatible incubator. Pol. J. Radiol. 2014, 79, 268–274. [Google Scholar] [PubMed] [Green Version]
- Bekiesinska-Figatowska, M.; Jurkiewicz, E.; Duczkowski, M.; Duczkowska, A.; Romaniuk-Doroszewska, A.; Bragoszewska, H.; Ceran, A. Congenital CNS Tumors Diagnosed on Prenatal MRI. Neuroradiol. J. 2011, 24, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Ben-Sira, L.; Constantini, S.; Beni-Adani, L. Impact of prenatal magnetic resonance imaging on postnatal neurosurgical treat-ment. J. Neurosurg. 2006, 105, 203–209. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| McNemara’s Test: χ2 (p) | Cohen’s Kappa Coefficient: κ (95% CI) | Newborn | |||
|---|---|---|---|---|---|
| CNS Defect | Fetus | 0 | 1 | ||
| Ventriculomegaly | 0 | 29 | 1 | ||
| 0.25 (0.62) | 0.87 (0.74–0.99) | 1 | 3 | 27 | |
| Central line defects | 0 | 29 | 6 | ||
| 0 (1) | 0.55 (0.34–0.77) | 1 | 7 | 18 | |
| Defects of the posteriori fossa | 0 | 46 | 2 | ||
| 0.57 (0.45) | 0.6 (0.33–0.86) | 1 | 5 | 7 | |
| Disorders of neural migration and proliferation | 0 | 48 | 6 | ||
| 2.29 (0.13) | 0.53 (0.23–0.83) | 1 | 1 | 5 | |
| Others | 0 | 41 | 4 | ||
| 0.13 (0.72) | 0.64 (0.42–0.87) | 1 | 4 | 11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kołak, M.; Herman-Sucharska, I.; Radoń-Pokracka, M.; Stolarek, M.; Horbaczewska, A.; Huras, H. The Assessment of the Usefulness of Prenatal Magnetic Resonance Imaging in the Diagnosis of Central Nervous System Defects. Diagnostics 2021, 11, 1723. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091723
Kołak M, Herman-Sucharska I, Radoń-Pokracka M, Stolarek M, Horbaczewska A, Huras H. The Assessment of the Usefulness of Prenatal Magnetic Resonance Imaging in the Diagnosis of Central Nervous System Defects. Diagnostics. 2021; 11(9):1723. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091723
Chicago/Turabian StyleKołak, Magdalena, Izabela Herman-Sucharska, Małgorzata Radoń-Pokracka, Małgorzata Stolarek, Anna Horbaczewska, and Hubert Huras. 2021. "The Assessment of the Usefulness of Prenatal Magnetic Resonance Imaging in the Diagnosis of Central Nervous System Defects" Diagnostics 11, no. 9: 1723. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091723