
Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Detection and Definition of BM Involvement
2.3. Statistical Analysis
3. Results
3.1. Patients
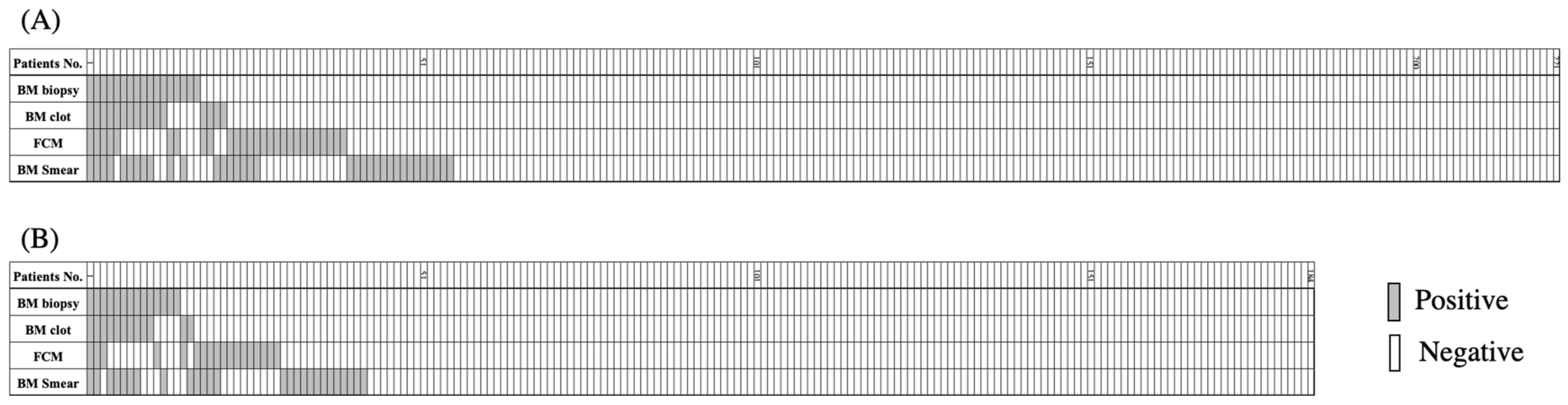
3.2. BM Lymphoma Invasion Detected by Four Different Modalities
3.3. Prognostic Significance of the Detection of BM Involvement by Different Modalities
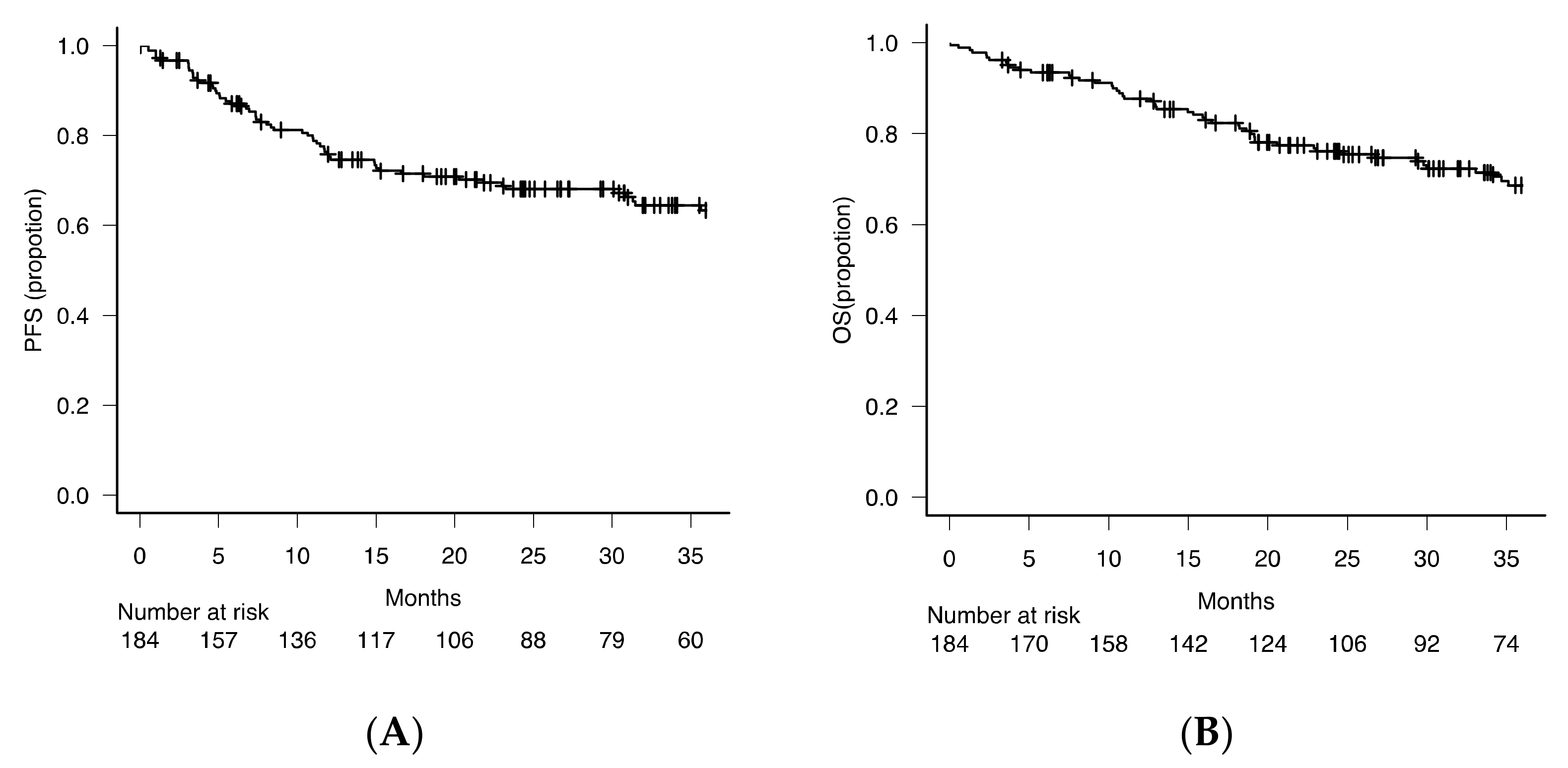
3.3.1. Patients
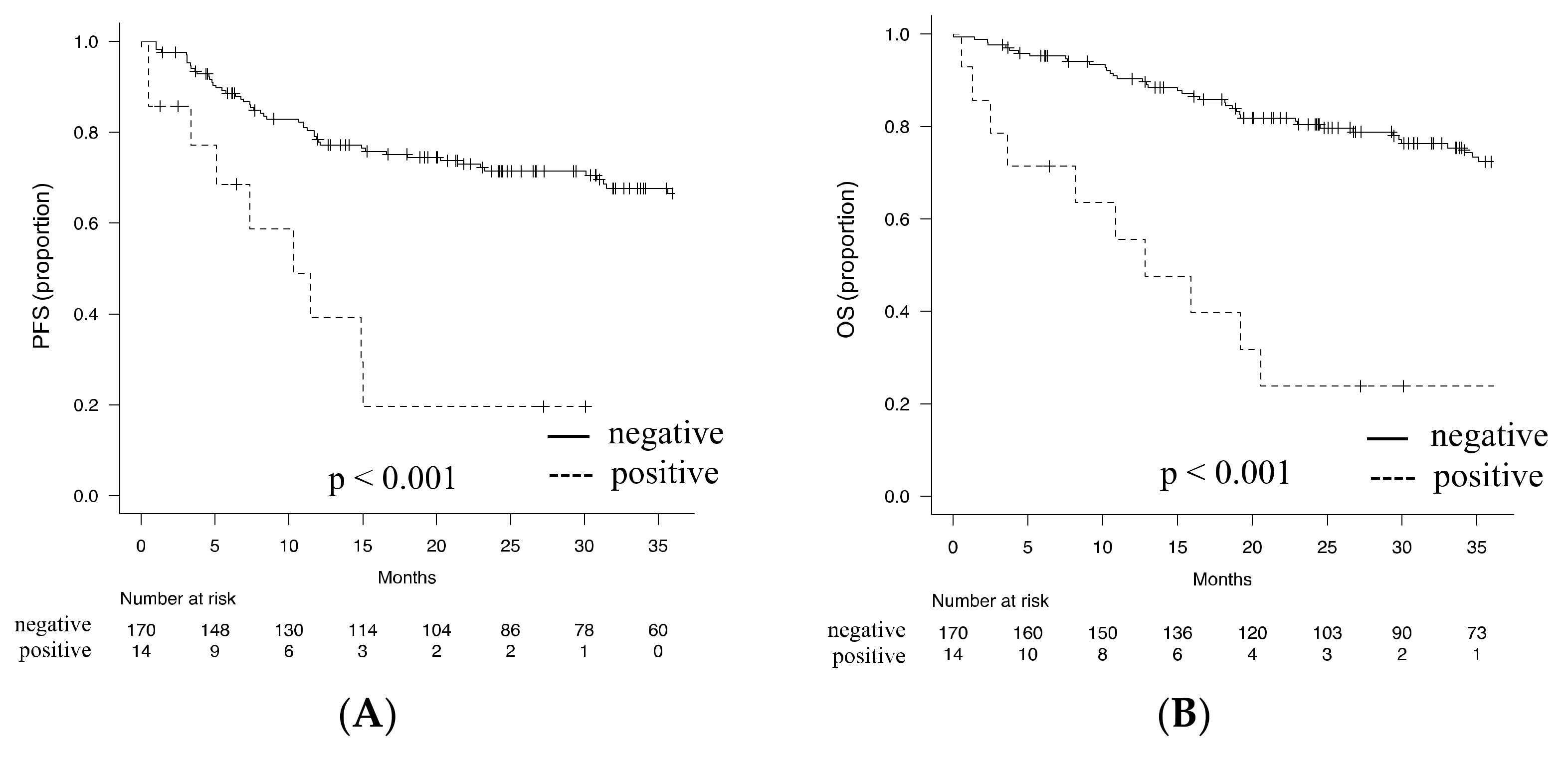
3.3.2. Prognostic Impact of the Detection of BM Involvement by BM Biopsy
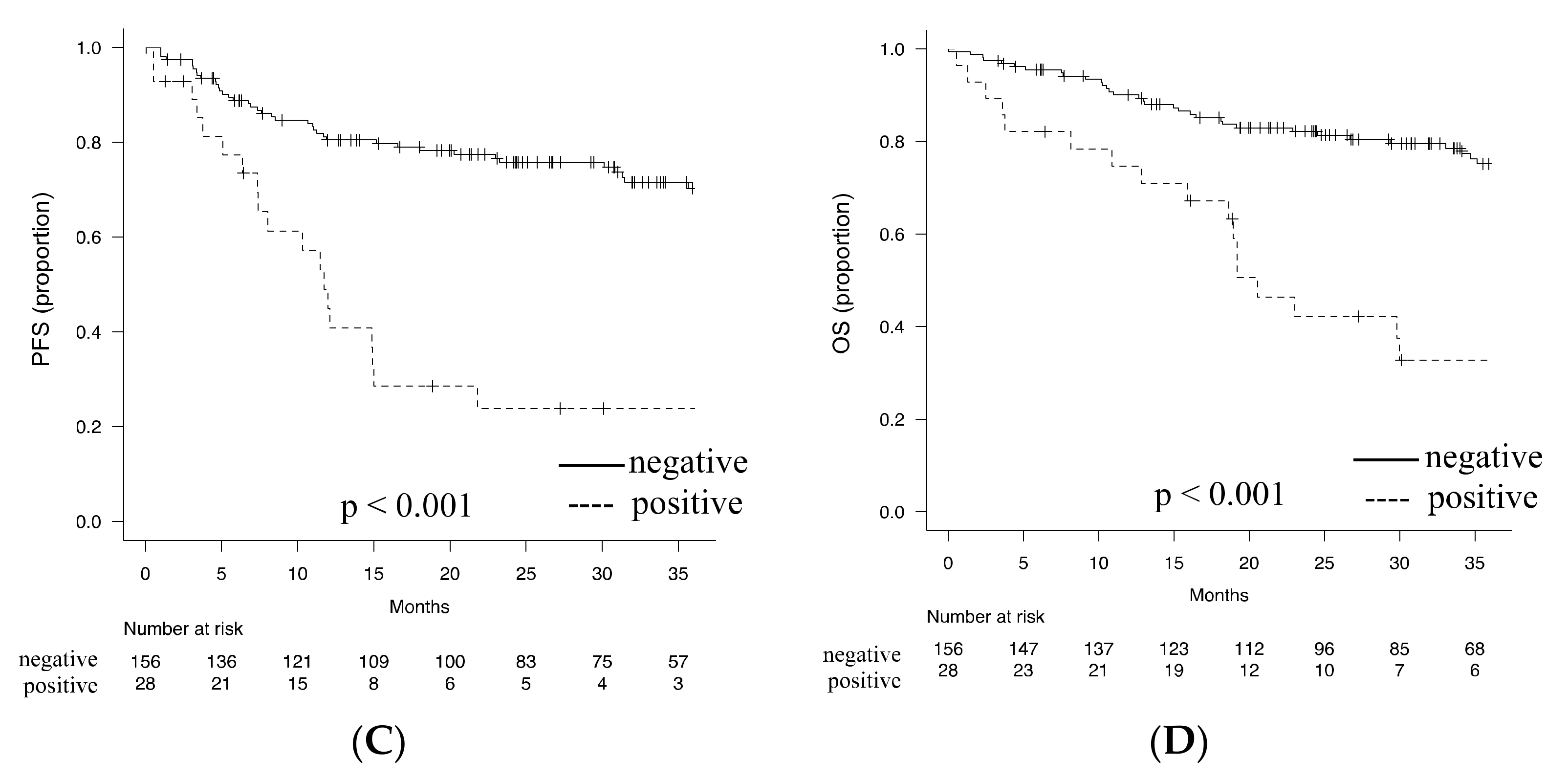
3.3.3. Optimal Detection Method of BM Involvement for Prediction of Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alizadeh, A.A.; Eisen, M.B.; Davis, R.E.; Ma, C.; Lossos, I.S.; Rosenwald, A.; Boldrick, J.C.; Sabet, H.; Tran, T.; Yu, X.; et al. Distinct Types of Diffuse Large B-Cell Lymphoma Identified by Gene Expression Profiling. Nature 2000, 403, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Chapuy, B.; Stewart, C.; Dunford, A.J.; Kim, J.; Kamburov, A.; Redd, R.A.; Lawrence, M.S.; Roemer, M.G.M.; Li, A.J.; Ziepert, M.; et al. Molecular Subtypes of Diffuse Large B Cell Lymphoma Are Associated with Distinct Pathogenic Mechanisms and Outcomes. Nat. Med. 2018, 24, 679–690. [Google Scholar] [CrossRef]
- Schmitz, R.; Wright, G.W.; Huang, D.W.; Johnson, C.A.; Phelan, J.D.; Wang, J.Q.; Roulland, S.; Kasbekar, M.; Young, R.M.; Shaffer, A.L.; et al. Genetics and Pathogenesis of Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2018, 378, 1396–1407. [Google Scholar] [CrossRef]
- Sehn, L.H.; Berry, B.; Chhanabhai, M.; Fitzgerald, C.; Gill, K.; Hoskins, P.; Klasa, R.; Savage, K.J.; Shenkier, T.; Sutherland, J.; et al. The Revised International Prognostic Index (R-IPI) Is a Better Predictor of Outcome than the Standard IPI for Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Blood 2007, 109, 1857–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipp, M.A. International Non-Hodgkin’s Lymphoma Prognostic Factors Project A Predictive Model for Aggressive Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 1993, 329, 987–994. [Google Scholar] [CrossRef]
- Kobayashi, T.; Kuroda, J.; Yokota, I.; Tanba, K.; Fujino, T.; Kuwahara, S.; Isa, R.; Yamaguchi, J.; Kawata, E.; Akaogi, T.; et al. The Kyoto Prognostic Index for Patients with Diffuse Large B-Cell Lymphoma in the Rituximab Era. Blood Cancer J. 2016, 6, e383. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Sehn, L.H.; Rademaker, A.W.; Gordon, L.I.; Lacasce, A.S.; Crosby-Thompson, A.; Vanderplas, A.; Zelenetz, A.D.; Abel, G.A.; Rodriguez, M.A.; et al. An Enhanced International Prognostic Index (NCCN-IPI) for Patients with Diffuse Large B-Cell Lymphoma Treated in the Rituximab Era. Blood 2014, 123, 837–842. [Google Scholar] [CrossRef]
- Ohmachi, K.; Kinoshita, T.; Tobinai, K.; Ogawa, G.; Mizutani, T.; Yamauchi, N.; Fukuhara, N.; Uchida, T.; Yamamoto, K.; Miyazaki, K.; et al. A Randomized Phase 2/3 Study of R-CHOP vs CHOP Combined with Dose-Dense Rituximab for DLBCL: The JCOG0601 Trial. Blood Adv. 2021, 5, 984–993. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Viardot, A.; Goebeler, M.-E.; Hess, G.; Neumann, S.; Pfreundschuh, M.; Adrian, N.; Zettl, F.; Libicher, M.; Sayehli, C.; Stieglmaier, J.; et al. Phase 2 Study of the Bispecific T-Cell Engager (BiTE) Antibody Blinatumomab in Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Blood 2016, 127, 1410–1416. [Google Scholar] [CrossRef]
- Sehn, L.H.; Herrera, A.F.; Flowers, C.R.; Kamdar, M.K.; McMillan, A.; Hertzberg, M.; Assouline, S.; Kim, T.M.; Kim, W.S.; Ozcan, M.; et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 155–165. [Google Scholar] [CrossRef]
- Yan, Y.; Chan, W.C.; Weisenburger, D.D.; Anderson, J.R.; Bast, M.A.; Vose, J.M.; Bierman, P.J.; Armitage, J.O. Clinical and Prognostic Significance of Bone Marrow Involvement in Patients with Diffuse Aggressive B-Cell Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1995, 13, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.W.; Moon, J.H.; Chae, Y.S.; Lee, S.J.; Kim, J.G.; Kim, Y.-K.; Lee, J.-J.; Yang, D.-H.; Kim, H.-J.; Kim, J.Y.; et al. Clinical Outcome of Rituximab-Based Therapy (RCHOP) in Diffuse Large B-Cell Lymphoma Patients with Bone Marrow Involvement. Cancer Res. Treat. 2013, 45, 112–117. [Google Scholar] [CrossRef]
- Cho, M.-C.; Chung, Y.; Jang, S.; Park, C.-J.; Chi, H.-S.; Huh, J.; Suh, C.; Shim, H. Prognostic Impact of Germinal Center B-Cell-like and Non-Germinal Center B-Cell-like Subtypes of Bone Marrow Involvement in Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Medicine 2018, 97, e13046. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.A.; Kurtin, P.J.; Katzmann, J.A.; Hoyer, J.D.; Li, C.Y.; Hodnefield, J.M.; Meyers, C.H.; Habermann, T.M.; Witzig, T.E. Immunophenotypic Analysis of Peripheral Blood and Bone Marrow in the Staging of B-Cell Malignant Lymphoma. Blood 1999, 94, 3889–3896. [Google Scholar] [CrossRef] [PubMed]
- Gomyo, H.; Shimoyama, M.; Minagawa, K.; Yakushijin, K.; Urahama, N.; Okamura, A.; Yamamoto, K.; Ito, M.; Chihara, K.; Hayashi, Y.; et al. Morphologic, Flow Cytometric and Cytogenetic Evaluation of Bone Marrow Involvement in B-Cell Lymphoma. Haematologica 2003, 88, 1358–1365. [Google Scholar]
- Kawano-Yamamoto, C.; Muroi, K.; Izumi, T.; Saito, K.; Ozawa, K. Two-Color Flow Cytometry with a CD19 Gate for the Evaluation of Bone Marrow Involvement of B-Cell Lymphoma. Leuk. Lymphoma 2002, 43, 2133–2137. [Google Scholar] [CrossRef]
- Martín-Moro, F.; Piris-Villaespesa, M.; Marquet-Palomanes, J.; García-Cosío, M.; Villarrubia, J.; Lario, A.; García, I.; Michael, B.; Roldán, E.; García-Vela, J.A.; et al. Bone Marrow Infiltration by Flow Cytometry at Diffuse Large B-Cell Lymphoma NOS Diagnosis Implies Worse Prognosis without Considering Bone Marrow Histology. Cytom. Prat B Clin. Cytom. 2020, 98, 525–528. [Google Scholar] [CrossRef]
- Greenbaum, U.; Levi, I.; Madmoni, O.; Lior, Y.; Al-Athamen, K.; Perry, Z.H.; Hatzkelzon, L.; Shubinsky, G. The Prognostic Significance of Bone Marrow Involvement in Diffuse Large B Cell Lymphoma According to the Flow Cytometry. Leuk. Lymphoma 2019, 60, 2477–2482. [Google Scholar] [CrossRef]
- Wolach, O.; Fraser, A.; Luchiansky, M.; Shapiro, C.; Radnay, J.; Shpilberg, O.; Lishner, M.; Lahav, M. Can Flow Cytometry of Bone Marrow Aspirate Predict Outcome of Patients with Diffuse Large B Cell Lymphoma? A Retrospective Single Centre Study. Hematol. Oncol. 2015, 33, 42–47. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, R.N.; Mark, H.F.; Medeiros, L.J. Fluorescent in situ hybridization in routinely processed bone marrow aspirate clot and core biopsy sections. Am. J. Pathol. 1994, 145, 1309–1314. [Google Scholar] [PubMed]
- Ong, M.G.; Lowery-Nordberg, M.; Pillarisetti, S.; Veillon, D.; Cotelingam, J. Maximizing the diagnostic yield from bone marrow aspirate material using the cell block technique on clot sections. Lab. Med. 2015, 46, e24–e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bain, B.J. Bone Marrow Biopsy Morbidity: Review of 2003. J. Clin. Pathol. 2005, 58, 406–408. [Google Scholar] [CrossRef] [PubMed]
- Bain, B.J. Bone Marrow Biopsy Morbidity and Mortality. Br. J. Haematol. 2003, 121, 949–951. [Google Scholar] [CrossRef] [Green Version]
- Gladden, K.; Spill, G.R. Iliac Fracture after a Bone Marrow Biopsy. PMR 2011, 3, 1150–1152. [Google Scholar] [CrossRef]
- Arima, H.; Maruoka, H.; Nasu, K.; Tabata, S.; Kurata, M.; Matsushita, A.; Imai, Y.; Takahashi, T.; Ishikawa, T. Impact of Occult Bone Marrow Involvement on the Outcome of Rituximab plus Cyclophosphamide, Doxorubicin, Vincristine and Prednisone Therapy for Diffuse Large B-Cell Lymphoma. Leuk. Lymphoma 2013, 54, 2645–2653. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; et al. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2021, 384, 842–858. [Google Scholar] [CrossRef]
- Lim, C.H.; Hyun, S.H.; Cho, Y.S.; Choi, J.Y.; Lee, K.-H. Prognostic Significance of Bone Marrow 2-[18F]-Fluoro-2-Deoxy-d-Glucose Uptake in Diffuse Large B-Cell Lymphoma: Relation to Iliac Crest Biopsy Results. Clin. Radiol. 2021, 76, 550.e19–550.e28. [Google Scholar] [CrossRef]
- Göçer, M.; Kurtoğlu, E. Comparison of Bone Marrow Involvement with Bone Marrow Biopsy and PET-CT and Evaluation of Any Effects on Survival in Patients Diagnosed with Hodgkin and Non-Hodgkin Lymphoma. Indian J. Hematol. Blood Transfus. Off. J. Indian Soc. Hematol. Blood Transfus. 2021, 37, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Saiki, Y.; Tomita, N.; Uchida, A.; Uemura, Y.; Suzuki, Y.; Hirakawa, T.; Kato, M.; Hoshikawa, M.; Kawano, T.; Nakamura, N.; et al. Biopsy Remains Indispensable for Evaluating Bone Marrow Involvement in DLBCL Patients despite the Use of Positron Emission Tomography. Int. J. Hematol. 2021, 113, 675–681. [Google Scholar] [CrossRef]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT Staging of DLBCL Accurately Identifies and Provides New Insight into the Clinical Significance of Bone Marrow Involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Nievelstein, R.A.J.; de Klerk, J.M.H. Bone Marrow 18F-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography Cannot Replace Bone Marrow Biopsy in Diffuse Large B-Cell Lymphoma. Am. J. Hematol. 2014, 89, 726–731. [Google Scholar] [CrossRef]
- Chen-Liang, T.-H.; Martín-Santos, T.; Jerez, A.; Rodríguez-García, G.; Senent, L.; Martínez-Millán, C.; Muiña, B.; Orero, M.; Teruel, A.; Martín, A.; et al. Bone Marrow Biopsy Superiority over PET/CT in Predicting Progression-Free Survival in a Homogeneously-Treated Cohort of Diffuse Large B-Cell Lymphoma. Cancer Med. 2017, 6, 2507–2514. [Google Scholar] [CrossRef]
- Alonso-Álvarez, S.; Alcoceba, M.; García-Álvarez, M.; Blanco, O.; Rodríguez, M.; Baile, M.; Caballero, J.C.; Dávila, J.; Vidriales, M.B.; Esteban, C.; et al. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-Cell Lymphoma. Cancers 2020, 12, 474. [Google Scholar] [CrossRef] [Green Version]
- Yao, Z.; Deng, L.; Xu-Monette, Z.Y.; Manyam, G.C.; Jain, P.; Tzankov, A.; Visco, C.; Bhagat, G.; Wang, J.; Dybkaer, K.; et al. Concordant Bone Marrow Involvement of Diffuse Large B-Cell Lymphoma Represents a Distinct Clinical and Biological Entity in the Era of Immunotherapy. Leukemia 2018, 32, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sehn, L.H.; Scott, D.W.; Chhanabhai, M.; Berry, B.; Ruskova, A.; Berkahn, L.; Connors, J.M.; Gascoyne, R.D. Impact of Concordant and Discordant Bone Marrow Involvement on Outcome in Diffuse Large B-Cell Lymphoma Treated with R-CHOP. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1452–1457. [Google Scholar] [CrossRef]
- Morton, L.M.; Wang, S.S.; Devesa, S.S.; Hartge, P.; Weisenburger, D.D.; Linet, M.S. Lymphoma Incidence Patterns by WHO Subtype in the United States, 1992–2001. Blood 2006, 107, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-M.; Li, J.-Y.; Gale, R.P.; Huang, X.-J. The Mystery of Chronic Lymphocytic Leukemia (CLL): Why Is It Absent in Asians and What Does This Tell Us about Etiology, Pathogenesis and Biology? Blood Rev. 2015, 29, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Yoo, I.Y.; Bang, S.H.; Lim, D.J.; Kim, S.J.; Kim, K.; Kim, H.J.; Kim, S.H.; Cho, D. Prevalence and Immunophenotypic Characteristics of Monoclonal B-Cell Lymphocytosis in Healthy Korean Individuals With Lymphocytosis. Ann. Lab. Med. 2020, 40, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Gelvez, J.C.; Salama, M.E.; Perkins, S.L.; Leavitt, M.; Inamdar, K.V. Prognostic Impact of Tumor Microenvironment in Diffuse Large B-Cell Lymphoma Uniformly Treated With R-CHOP Chemotherapy. Am. J. Clin. Pathol. 2016, 145, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Spatially Resolved Dark- versus Light-Zone Microenvironment Signature Subdivides Germinal Center-Related Aggressive B Cell Lymphomas-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33083730/ (accessed on 25 August 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Total Number of Patients, n | 221 |
| Age, median (range) | 72 (26–97) |
| Gender, Male, n (%) | 135 (61.1) |
| ECOG PS 2–4, n (%) | 68 (31.2) |
| LDH > ULN, n (%) | 131 (59.3) |
| Ann Arbor Stage III/IV, n (%) | 127 (57.5) |
| Extranodal site 2 or more, n (%) | 63 (28.5) |
| R-IPI, n (%) | |
| Very good | 12 (5.4) |
| Good | 92 (41.6) |
| Poor | 117 (52.9) |
| Treatment regimen, n (%) | |
| R-CHOP (-like) regimen | 184 (83.3) |
| Intensive chemotherapy other than R-CHOP | 17 (7.7) |
| Upfront autologous stem cell transplantation | 13 (5.9) |
| Palliative care | 7 (3.2) |
| A. All Patients (n = 221) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Modality | BM Biopsy | BM Clot | FCM | ||||||||
| Result/n (%) | − | + | κ | − | + | κ | − | + | κ | ||
| 204 (92.3) | 17 (7.7) | 205 (92.7) | 16 (7.3) | 194 (87.8) | 27 (12.2) | ||||||
| BM smear | − | 187 (84.6) | 181 (81.9) | 6 (2.7) | 0.366 | 182 (82.4) | 5 (2.3) | 0.379 | 170 (76.9) | 17 (7.7) | 0.222 |
| + | 34 (15.4) | 23 (10.4) | 11 (5) | 23 (10.4) | 11 (5) | 24 (10.9) | 10 (4.5) | ||||
| FCM | − | 194 (87.8) | 184 (83.3) | 10 (4.5) | 0.247 | 185 (83.7) | 9 (4.1) | 0.258 | |||
| + | 27 (12.2) | 20 (9.0) | 7 (3.2) | 20 (9.0) | 7 (3.2) | ||||||
| BM clot | − | 205 (92.7) | 200 (90.5) | 5 (2.3) | 0.705 | ||||||
| + | 16 (7.3) | 4 (1.8) | 12 (5.4) | ||||||||
| B. Patients Initially Treated with R-CHOP or R-CHOP-Like Regimen (n = 184) | |||||||||||
| Modality | BM Biopsy | BM Clot | FCM | ||||||||
| Result/n (%) | − | + | κ | − | + | κ | − | + | κ | ||
| 170 (92.4) | 14 (7.6) | 172 (93.5) | 12 (6.5) | 166 (90.2) | 18 (9.8) | ||||||
| BM smear | − | 158 (85.9) | 152 (82.6) | 6 (3.3) | 0.334 | 154 (83.7) | 4 (2.2) | 0.364 | 146 (79.3) | 12 (6.5) | 0.178 |
| + | 26 (14.1) | 18 (9.8) | 8 (4.3) | 18 (9.8) | 8 (4.3) | 20 (10.9) | 6 (3.3) | ||||
| FCM | − | 166 (90.2) | 156 (84.8) | 10 (5.4) | 0.180 | 158 (85.9) | 8 (4.3) | 0.204 | |||
| + | 18 (9.8) | 14 (7.6) | 4 (2.2) | 14 (7.6) | 4 (2.2) | ||||||
| BM clot | − | 172 (93.5) | 168 (91.3) | 4 (2.2) | 0.752 | ||||||
| + | 12 (6.5) | 2 (1.1) | 10 (5.4) | ||||||||
| Clinical Characteristics | BM Involvement Diagnosed by BM Biopsy | ||
|---|---|---|---|
| Negative | Positive | p Value | |
| Number of patients, n | 170 | 14 | - |
| Age, median (range) | 73 (28–89) | 76 (43–89) | 0.393 |
| Gender, Male, n (%) | 105 (61.8) | 7 (50.0) | 0.405 |
| ECOG PS 2–4, n (%) | 40 (23.8) | 11 (78.6) | <0.001 |
| LDH > ULN, n (%) | 90 (52.9) | 13 (92.4) | 0.004 |
| Disease stage III, IV, n (%) | 84 (49.4) | 14 (100.0) | <0.001 |
| Extranodal site 2 or more, n (%) | 40 (23.5) | 4 (28.6) | 0.745 |
| Leukocyte count, median (×109/L) (range) | 6.14 (1.80–5.87) | 5.50 (1.10–2.48) | 0.497 |
| Hemoglobin level, median (g/dL) (range) | 12.4 (5.2–16.2) | 9.9 (6.7–14.5) | 0.011 |
| Platelet, median (×109/L) (range) | 217.0 (180.0–763.0) | 105.0 (80.0–215.0) | <0.001 |
| R-IPI, n (%) | 0.003 | ||
| Very good | 12 (7.1) | 0 (0.0) | |
| Good | 80 (47.1) | 1 (7.1) | |
| Poor | 78 (45.9) | 13 (92.9) | |
| Univariate Analysis | Multivariate Analysis * | |||||||
|---|---|---|---|---|---|---|---|---|
| Modality | Result (n) | HR | 95% CI | p | HR | 95% CI | p | c-Index |
| BM biopsy | − (170) | 1 | − | − | 1 | − | − | 0.684 |
| + (14) | 4.29 | 2.08–8.83 | <0.001 | 2.87 | 1.27–6.50 | 0.011 | ||
| BM clot | − (172) | 1 | − | − | 1 | − | − | 0.688 |
| + (12) | 4.37 | 2.14–8.92 | <0.001 | 2.69 | 1.24–5.83 | 0.012 | ||
| FCM | − (166) | 1 | − | − | 1 | − | − | 0.703 |
| + (18) | 3.06 | 1.63–5.78 | <0.001 | 2.75 | 1.44–5.24 | 0.002 | ||
| BM smear | − (158) | 1 | − | − | 1 | − | − | 0.702 |
| + (26) | 3.50 | 2.02–6.08 | <0.001 | 2.46 | 1.36–4.44 | 0.003 | ||
| BM biopsy and/or clot | − (186) | 1 | − | − | 1 | − | − | 0.69 |
| + (16) | 3.75 | 1.89–7.43 | <0.001 | 2.42 | 1.16–5.07 | 0.019 | ||
| BM biopsy and/or FCM | − (156) | 1 | − | − | 1 | − | − | 0.712 |
| + (28) | 3.94 | 2.27–6.82 | <0.001 | 3.33 | 1.85–6.00 | <0.001 | ||
| BM biopsy and/or BM smear | − (152) | 1 | − | − | 1 | − | − | 0.695 |
| + (32) | 3.08 | 1.79–5.31 | <0.001 | 2.13 | 1.19–3.83 | 0.011 | ||
| BM clot and/or FCM | − (158) | 1 | − | − | 1 | − | − | 0.705 |
| + (26) | 3.66 | 2.10–6.36 | <0.001 | 2.89 | 1.62–5.17 | <0.001 | ||
| BM clot and/or BM smear | − (154) | 1 | − | − | 1 | − | − | 0.707 |
| + (30) | 3.60 | 2.11–6.14 | <0.001 | 2.54 | 1.42–4.55 | 0.002 | ||
| FCM and/or BM smear | − (146) | 1 | − | − | 1 | − | − | 0.708 |
| + (38) | 3.29 | 1.97– 5.50 | <0.001 | 2.50 | 1.45–4.30 | <0.001 | ||
| BM biopsy, clot, and/or FCM | − (155) | 1 | − | − | 1 | − | − | 0.705 |
| + (29) | 3.52 | 2.04–6.09 | <0.001 | 2.82 | 1.58–5.01 | <0.001 | ||
| BM biopsy, clot, and/or BM smear | − (151) | 1 | − | − | 1 | − | − | 0.704 |
| + (33) | 3.31 | 1.94– 5.66 | <0.001 | 2.32 | 1.30–4.14 | <0.001 | ||
| BM biopsy, FCM, and/or BM smear | − (142) | 1 | − | − | 1 | − | − | 0.706 |
| + (42) | 3.19 | 1.92–5.31 | <0.001 | 2.37 | 1.37–4.08 | 0.002 | ||
| BM clot, FCM, and/or BM smear | − (144) | 1 | − | − | 1 | − | − | 0.707 |
| + (40) | 3.39 | 2.03–5.64 | <0.001 | 2.52 | 1.47–4.34 | <0.001 | ||
| BM biopsy, clot, FCM, and/or BM smear | − (142) | 1 | − | − | 1 | − | − | 0.706 |
| + (42) | 3.19 | 1.92–5.31 | <0.001 | 2.37 | 1.37–4.08 | 0.002 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, H.; Uoshima, N.; Muramatsu, A.; Isa, R.; Fujino, T.; Matsumura-Kimoto, Y.; Tsukamoto, T.; Mizutani, S.; Shimura, Y.; Kobayashi, T.; et al. Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma. Diagnostics 2021, 11, 1724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091724
Okamoto H, Uoshima N, Muramatsu A, Isa R, Fujino T, Matsumura-Kimoto Y, Tsukamoto T, Mizutani S, Shimura Y, Kobayashi T, et al. Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma. Diagnostics. 2021; 11(9):1724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091724
Chicago/Turabian StyleOkamoto, Haruya, Nobuhiko Uoshima, Ayako Muramatsu, Reiko Isa, Takahiro Fujino, Yayoi Matsumura-Kimoto, Taku Tsukamoto, Shinsuke Mizutani, Yuji Shimura, Tsutomu Kobayashi, and et al. 2021. "Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma" Diagnostics 11, no. 9: 1724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091724